

Abstract
Background
Helicobacter pylori (H.pylori) infections are prevalent and recognized as major cause of gastrointestinal diseases in Ethiopia. However, Studies conducted on the prevalence, risk factors and other clinical forms of H.pylori on different population and geographical areas are reporting conflicting results. Therefore, this review was conducted to estimate the pooled prevalence of H.pylori infections and associated factors in Ethiopia.
Methods
PubMed, Embase, Google scholar, and Ethiopian Universities’ repositories were searched following the Preferred Items for Systematic review and Meta-analysis (PRISMA) guideline. The quality of included studies was assessed using the Newcastle-Ottawa Scale in meta-analysis. Heterogeneity between studies was assessed using Cochrane Q test and I2 test statistics based on the random effects model. Comprehensive meta-analysis (CMA 2.0) and Review Manager (RevMan 5.3) were employed to compute the pooled prevalence and summary odds ratios of factors associated with of H.pylori infection.
Results
Thirty seven studies with a total of 18,890 participants were eligible and included in the analysis. The overall pooled prevalence of H.pylori infection was 52.2% (95% CI: 45.8–58.6). In the subgroup analysis by region, the highest prevalence was found in Somalia (71%; 95% CI: 32.5–92.6) and the lowest prevalence was reported in Oromia (39.9%; 95% CI: 17.3–67.7). Absence of hand washing after toilet (OR = 1.8, 95% CI; 1.19–2.72), alcohol consumption (OR = 1.34, 95% CI; 1.03–1.74) and gastrointestinal (GI) symptoms (OR = 2.23, 95% CI; 1.59–3.14) were associated with H.pylori infection. The trend of H.pylori infection showed a decreasing pattern overtime from 1990 to 2017 in the meta-regression analysis.
Conclusion
The prevalence of H.pylori infection remains high; more than half of Ethiopians were infected. Although the trend of infection showed a decreasing pattern; appropriate use of eradication therapy, health education primarily to improve knowledge and awareness on the transmission dynamics of the bacteria, behavioral changes, adequate sanitation, population screening and diagnosis using multiple tests are required to reduce H.pylori infections. Recognizing the bacteria as a priority issue and designing gastric cancer screening policies are also recommended.
Electronic supplementary material
The online version of this article (10.1186/s12876-018-0927-3) contains supplementary material, which is available to authorized users.
Keywords: Helicobacter pylori, Systematic review, Meta-analysis, Ethiopia
Background
Helicobacter pylori have been found to infect about half of the world’s population [1–5]. The prevalence of H.pylori infection varies globally with a greater prevalence generally reported from developing countries. The global estimate of H.pylori infection was reported at 48.5% while continental reports were 69.4% in South America, 37.1% in North America, 24.4% in Oceania, 54.6% in Asia, 47.0% in Europe and 79.1% in Africa [2, 6]. This difference has been related to geography, age, ethnicity, socioeconomic factors, and methods of diagnosis and eradication therapy [1, 6, 7]. Diseases associated with H.pylori infections are commonly occur at earlier ages in developing countries [1–3, 8–10].
The burden of H.pylori infections goes beyond the gastrointestinal tract and associated with different complications including hyperemesis gravidarum [11], coronary heart disease [12, 13], anemia [14–17], diabetes mellitus [18–22], cholecystitis [23, 24], HIV [25–27], growth trajectories [28], autoimmune and Parkinson’s disease [29]. Failure to H.pylori eradication therapy is also linked to bacterial resistance and poor patient compliance [30–34].
In 2017, World Health Organization (WHO) has published lists of 16 bacteria that pose the greatest risk for human health. H.pylori was thus categorized as a high priority pathogen for research and development of new and effective treatments [35]. In addition, recommendations are emerging to change approaches to management of H.pylori due to increased drug resistance [30, 31, 36–38]. The success of these developments needs knowledge of prevalence of H.pylori.
In Ethiopia, the prevalence of H.pylori infection ranged from 7.7% [39] to 91% [40]. It is highly prevalent and recognized as major cause of gastrointestinal diseases. Studies conducted on the prevalence, risk factors and other clinical forms of H.pylori on different population and geographical areas are reporting conflicting results. Socioeconomic factors, sanitation, crowded living conditions, unsafe food and water, ethnicity as well as poverty can contribute to H.pylori infections [41]. Studies published on the prevalence of H.pylori in Ethiopia dated back to the 1990’s [42]. However, comprehensive review has not been done on its prevalence and associated factors in Ethiopia. Therefore; this study was done to estimate the pooled prevalence of H.pylori infection and associated factors in Ethiopia.
Methods
Data bases and search strategy
PubMed, Embase, and Google scholar were searched to identify potential articles on H.pylori infections in Ethiopia. To include unpublished studies, Ethiopian University repositories were searched and reference lists of eligible studies were searched to maximize inclusion of relevant studies. The search was conducted following the PRISMA guideline and checklists ( [43], Fig. 1). The following terms with MeSH (Medical Subject Headings) and Boolean operators were used to search PubMed; Helicobacter pylori OR H.pylori OR Campylobacter pylori OR C.pylori OR gastritis OR gastric cancer OR gastric carcinoma OR peptic ulcer disease OR PUD OR duodenal ulcer OR dyspepsia OR mucosa associated lymphoid tissue OR MALT AND Ethiopia. The search was limited to English language publications and done independently by each reviewer to minimize bias and the missing of studies. Search results were combined in to EndNote X6 file (Clarivate Analytics USA) and duplicates were removed. All articles published up to June 30, 2018 were included in the review if fulfilled the eligibility criteria (Table 1).
Fig. 1.
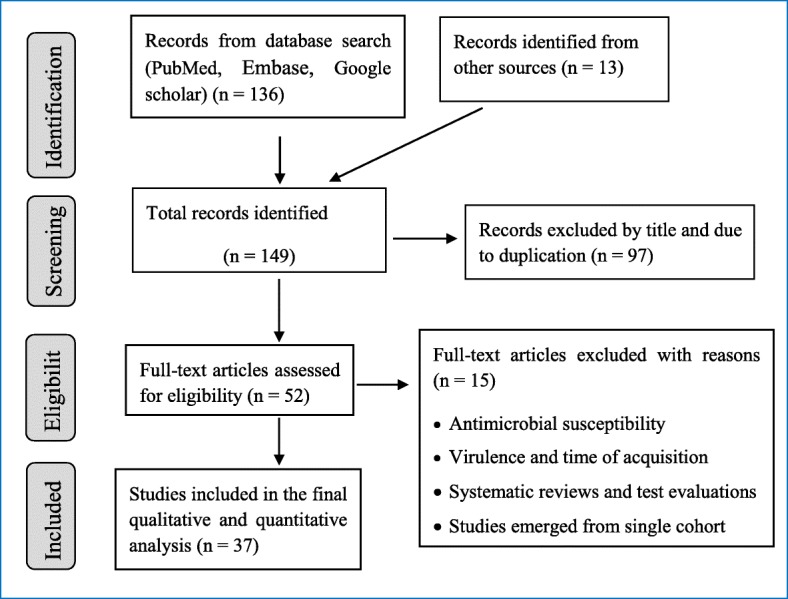
PRISMA flow chart of article selection
Table 1.
Eligibility criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
| • Country and setting: Ethiopia and any setting • Study design: any study design • Outcome: reported the prevalence or number of H.pylori cases and sample size • Type of articles: full text and peer-reviewed; published in English language • Publication year: up to June 30, 2018 • Types of diagnosis: reported any laboratory tests |
• Evaluation of diagnostic tests and antimicrobial sensitivity • Systematic reviews and meta-analysis • Studies on virulence factor genes • Studies on age at acquisition of H.pylori infection and its effect • Studies emerged from single cohort study with similar prevalence report |
Quality assessment
The quality of included studies was assessed by using the Newcastle-Ottawa Scale (NOS) (Additional file 1). Two authors independently assessed the quality of each study. Disagreements between authors was resolved by discussion and articles were included if agreement was reached between the authors.
Data extraction
Data were extracted into customized Microsoft Excel. Data extracted from each included study include; author, publication year, study area, study period, study design, study population, sample size, laboratory tests used, prevalence and/or number of H.pylori cases. We have also contacted corresponding authors of the included studies for missing data though no one responded.
Data analysis
Studies providing data on crude prevalence of H.pylori or numbers of cases and study participants were included in the meta-analysis. Prevalence for individual studies was determined by multiplying the ratio of cases to sample size by 100. The estimation of pooled prevalence and summary odds ratios of H.pylori infection was done using CMA 2.0 and RevMan 5.3 softwares. Subgroup analyses were done by study period, study region, study design, laboratory tests used (types and numbers) and publication history. With the assumption that true effect sizes exists between eligible studies, the random effects model was used to determine the pooled prevalence, summary odds ratios and 95% CIs. Significant association between H.pylori infections and potential factors was declared at p-value < 0.05. Heterogeneity was evaluated using the Cochran’s Q test and I2 statistics. Significant heterogeneity was declared at I2 > 50% and Q-test (P < 0.10).
Publication bias and sensitivity analysis
Funnel plots were drawn to assess the possibility of publication bias. We plotted the studies’ logit event rate and the standard error to detect asymmetry in the distribution. A gap in the funnel plot indicates potential for publication bias. In addition, Begg’s adjusted rank correlation and Egger’s regression asymmetry tests were used to assess publication bias, with P < 0.05 considered to indicate potential publication bias. Sensitivity analysis, leave-one-out analysis was done to assess the prime determinant of the pooled prevalence of H.pylori infection and to detect the possible causes of heterogeneity between studies.
Results
Characteristics of included studies
Thirty seven studies with a total population of 18,890 met the inclusion criteria and included in the analysis. The detail characteristics of included studies are shown in (Table 2). The included studies were conducted between 1990 and 2017; of which 29 were published and 8 were unpublished. Thirteen studies were conducted in the Southern Nations, Nationalities and Peoples Region (SNNPR) of Ethiopia. Eleven studies were conducted in Addis Ababa; nine studies in Amhara region, two studies in Oromia, one study in Somalia and one study in Benishangul Gumuz region. Nineteen studies were reported among adults [15, 39, 40, 42, 44–58], eight of the studies were reported on children [14, 59–65] while nine studies were conducted on both adults and children [25, 26, 58, 66–72]. One study did not describe the study population [73]. Among the include studies, 20 were cross-sectional, eight were case control, six were cohort, and two were retrospective studies. Ten studies used multiple tests in detecting H.pylori while 27 studies employed a single test to declare H.pylori infection. The prevalence of H.pylori from eligible individual studies ranged from 7.7 to 91.0%.
Table 2.
Lists and characteristics of the included 37 studies
| Author, year | Study period | Study region | Study design | Study subjects | Lab test used | Sample size | Cases | Prevalence (%) | Publication history |
|---|---|---|---|---|---|---|---|---|---|
| Ababu, 2016 | 2016 | Addis Ababa | Cross-sectional | HIV patients on ART | Stool antigen | 388 | 213 | 54.9 | Unpublished |
| Abebaw, 2014 | 2013 | Amhara | Cross-sectional | Dyspeptic patients | Serology (IgG) | 209 | 151 | 72.2 | Published |
| Alebie, 2016 | 2016 | Somalia | Cross-sectional | University students with gastritis | Serology (IgG, IgM, IgA) | 145 | 103 | 71.0 | Published |
| Alemayehu, 2011 | 2010–2011 | South | Case control | Dyspeptic and non-dyspeptic patients | Serology (IgG) | 106 | 66 | 62.3 | Unpublished |
| Amberebir, 2011 | 2008–2009 | South | Cohort | Children at age three | Stool antigen | 616 | 253 | 41.1 | Published |
| Amberebir, 2014 | 2008–2009 | South | Cohort | Children at age five | Stool antigen | 857 | 377 | 44.0 | Published |
| Asrat, 2004 | 2000–2002 | Addis Ababa | Cross-sectional | Dyspeptic patients | PCR, culture, Rapid Urease,, Histology, Silver stain, stool antigen, serology (EIA, immunoblot – IgG), | 300 | 273 | 91.0 | Published |
| Assefa, 2017 | 2016 | Addis Ababa | Case control | Pregnant women | Stool antigen | 150 | 37 | 24.7 | Unpublished |
| Ayele, 2017 | 2016 | South | Case control | Dyspeptic and non-dyspeptic patients | Stool antigen | 168 | 13 | 7.7 | Published |
| Berhaneselassie, 2017 | 2010 | South | Case control | Dyspeptic and non-dyspeptic patients | Serology (IgG) | 195 | 175 | 89.7 | Published |
| Desta, 2002 | 2001 | Addis Ababa | Cross-sectional | Blood donors | Serology (IgG) | 150 | 133 | 88.7 | Published |
| Dilnessa, 2017 | 2015 | Gumuz | Cross-sectional | Dyspeptic and non-dyspeptic patients | Stool antigen | 230 | 112 | 48.7 | Published |
| Hailu. 2016 | 2012–2013 | South | Cross-sectional | Upper GI symptoms | Stool antigen | 349 | 177 | 50.7 | Published |
| Henriksen, 1999 | 1992–1995 | South | Cohort | PUD and non-PUD patients | Rapid urease, Loffler stain | 290 | 234 | 80.7 | Published |
| Kassew, 2017 | 2016 | Amhara | Cross-sectional | Dyspeptic patients | Stool antigen | 354 | 133 | 37.6 | Published |
| Kebede, 2015 | 2014 | Oromia | Cross-sectional | TB and non-TB patients | Stool antigen | 108 | 20 | 18.5 | Published |
| Kemal, 2014 | 2014 | Addis Ababa | Cross-sectional | Upper GI symptoms | Stool antigen | 221 | 57 | 25.8 | Unpublished |
| Kibru, 2014 | 2013 | South | Cross-sectional | Dyspeptic patients | Stool antigen | 401 | 210 | 52.4 | Published |
| Lindkvist, 1998 | 1995 | South | Case control | Rural and 2–4 years old children | Serology(EIA, immunoblot - IgG) | 242 | 116 | 47.9 | Published |
| Lindkvist, 1999 | 1995 | South | Cohort | Seronegative children | Serology(EIA, immunoblot - IgG) | 77 | 44 | 57.1 | Published |
| Mathewos, 2013 | 2009–2011 | Amhara | Retrospective | H.pylori suspects | Serology (IgG, IgM, IgA) | 1388 | 912 | 65.7 | Published |
| Moges, 2006 | 2003 | Amhara | Cross-sectional | Dyspeptic patients | Serology (IgG) | 215 | 184 | 85.7 | Published |
| Seid, 2017 | 2017 | Addis Ababa | Case control | Dyspeptic and non-dyspeptic HIV patients | Stool antigen | 370 | 117 | 31.6 | Unpublished |
| Seid, 2018 | 2015 | Amhara | Cross-sectional | Upper GI symptoms | Stool antigen | 318 | 99 | 31.1 | Published |
| Seid, 2018a | 2015–2016 | Amhara | Cross-sectional | Upper GI symptoms | Serology (IgG) | 363 | 255 | 70.2 | Published |
| Seid, 2018b | 2016 | Amhara | Cross-sectional | Upper GI symptoms | Stool antigen, serology (IgG) | 342 | 104 | 30.4 | Published |
| Tadege, 2005 | 2002–2003 | Amhara | Case control | Dyspeptic and non-dyspeptic patients | Serology (EIA, imunoblot - IgG) | 200 | 124 | 62.0 | Published |
| Tadesse, 2011 | 2009 | Addis Ababa | Case control | Dyspeptic and non-dyspeptic patients | Stool antigen, serology (IgG, IgM, IgA) | 238 | 109 | 45.8 | Published |
| Tadesse, 2014 | 2012–2013 | South | Cross-sectional | Upper GI symptoms | Serology (double ELISA -IgG) | 408 | 340 | 83.3 | Published |
| Taye, 2015 | 2008–2009 | South | Cohort | Children at age 6.5 | Stool antigen | 848 | 88 | 10.4 | Published |
| Tedla, 1992 | 1990 | South | Cohort | Upper GI symptoms | Rapid urease, Loeffler, Methylene blue stain | 444 | 324 | 73.0 | Published |
| Teka, 2016 | 2010–2011 | Addis Ababa | Cross-sectional | HIV positive and negative patients | Serology (IgG) | 212 | 120 | 56.6 | Published |
| Terfa, 2015 | 2015 | Addis Ababa | Cross-sectional | Women of child bearing age | Stool antigen | 332 | 96 | 28.9 | Unpublished |
| Tesfaye, 2017 | 2016–2017 | Oromia | Cross-sectional | Health facility and school children | Serology (IgM, IgG, IgA), stool antigen | 461 | 296 | 64.2 | Unpublished |
| Tsega, 1996 | 1994 | Addis Ababa | Case control | NUD and asymptomatic patients | Gram, giemsa, gemineze stain | 207 | 120 | 58.0 | Published |
| Workineh, 2016 | 2009–2013 | Amhara | Retrospective | Dyspeptic patients | Serology (IgG, IgM, IgA) | 6566 | 2733 | 41.6 | Published |
| Worku, 2017 | 2017 | Addis Ababa | Cross-sectional | School children | Stool antigen | 422 | 61 | 14.5 | Unpublished |
Pooled prevalence of H.pylori
A total of 18,890 Ethiopians were participated in the study; out of which 8979 were infected with H.pylori in the period under review giving an overall pooled prevalence of 52.2% (95% CI: 45.8–58.6; I2 = 51.05%, p = 0.503) (Fig. 2). Sensitivity analysis revealed no significant difference both in the pooled prevalence and heterogeneity. When one study was excluded from the analysis step-by-step, the pooled prevalence was between 50.5 and 53.5% while heterogeneity was similar (I2 = 53.5%). Drawing of funnel plot supported with Egger’s regression (p = 0.172) and Begg’s correlation (p = 0.367) tests showed no evidence of significant publication bias (Fig. 3).
Fig. 2.

Forest plot of the pooled prevalence of helicobacter pylori infection in Ethiopia from 37 studies
Fig. 3.

Publication bias assessment funnel plot; Egger’s regression test (p = 0.172) and Begg’s rank correlation (p = 0.367)
Subgroup prevalence of H.pylori
Prevalence of H.pylori for subgroups was analyzed for study region, study period, sample size, study design, type and number of diagnostic tests used and publication history. The prevalence of H.pylori when studies were categorized by region ranged from 39.9% (95% CI: 17.3–67.7%; I2 = 67.6%, P = 0.486) in Oromia to 71% (95% CI: 32.5–92.6.2; I2 = 0.0%, P = 0.280) in Somalia. Other regional prevalence rates were 48.1% in Addis Ababa, 54.6% in Amhara, 48.7% in Benishangul Gumuz and 53.6% in SNNPR. Subgroup analysis by publication history showed a prevalence of 56.5% from published and 36.8% from unpublished studies. Subgroup analysis was also computed by the study period when the studies were conducted to see the trend of H.pylori infection. Hence, the prevalence of H.pylori was 64.4% in the period 1990–2000, 62.2% in the period 2001–2011 and 42.9% in the period 2012–2017, showing a decreasing trend. The pooled prevalence was also higher in studies which used multiple tests than studies employed a single test to detect H.pylori infection (62.9 and 48.1%, respectively) (Table 3).
Table 3.
Pooled prevalence of H.pylori infections in Ethiopia stratified according to sub-groups
| Variables | No of included studies | Pooled prevalence estimate | Heterogeneity | |||
|---|---|---|---|---|---|---|
| Sample size | Cases | Prevalence, 95% CI | I2 (%) | Q (P-value) | ||
| Region | ||||||
| Addis Ababa | 11 | 2990 | 1336 | 48.1 (36.3–60.2) | 50.4 | 0.790 |
| Amhara | 9 | 9955 | 4695 | 54.6 (42.0–66.7) | 1.7 | 0.412 |
| Benishangul gumuz | 1 | 230 | 112 | 48.7 (16.0–82.6) | 0.0 | 0.954 |
| Oromia | 2 | 569 | 316 | 39.9 (17.3–67.7) | 61.4 | 0.517 |
| Somalia | 1 | 145 | 103 | 71.0 (32.5–92.6) | – | – |
| SNNPR | 13 | 5001 | 2417 | 53.6 (42.4–64.4) | 53.1 | 0.569 |
| Study period a | ||||||
| 1990–2000 | 5 | 1260 | 838 | 64.4 (47.3–78.5) | 0.0 | 0.097 |
| 2001–2011 | 12 | 8724 | 4118 | 62.2 (51.1–72.1) | 64.3 | 0.031 |
| 2012–2017 | 21 | 8906 | 4.023 | 42.9 (34.8–51.4) | 37.0 | 0.102 |
| Sample size | ||||||
| < 150 | 6 | 736 | 403 | 54.7 (36.8–71.4) | 51.3 | 0.614 |
| 151–500 | 26 | 7879 | 4213 | 54.5 (45.9–62.8 | 39.5 | 0.306 |
| 501–1000 | 3 | 2321 | 718 | 28.6 (12.8–52.2) | 31.2 | 0.074 |
| > 1000 | 2 | 7954 | 3645 | 53.9 (25.5–79.9) | 0.0 | 0.804 |
| Study design | ||||||
| Cross-sectional | 20 | 5928 | 3137 | 55.1 (44.9–64.9) | 39.9 | 0.324 |
| Case control | 9 | 1876 | 877 | 47.0 (32.5–62.1) | 44.7 | 0.704 |
| Cohort | 6 | 3132 | 1320 | 49.7 (39.6–67.5) | 45.7 | 0.972 |
| Retrospective | 2 | 7954 | 3645 | 53.9 (24.5–80.5) | 0.0 | 0.812 |
| Lab tests used | ||||||
| Stool antigen | 18 | 6712 | 2276 | 31.4 (24.6–39.1) | 8.5 | < 0.001 |
| Serology (IgM, IgG, IgA) | 15 | 10,937 | 5752 | 69.7 (61.2–76.9) | 2.3 | < 0.001 |
| Others b | 4 | 1241 | 951 | 77.8 (63.0–87.8) | 21 | 0.001 |
| Number of tests used | ||||||
| Single | 27 | 7235 | 16,099 | 48.1 (40.8–55.5) | 57.22 | 0.662 |
| Multiple | 10 | 1744 | 2801 | 62.9 (51.0–73.4) | 19.7 | 0.034 |
| Publication history | ||||||
| Published | 29 | 16,440 | 8036 | 56.6 (49.2–63.6) | 51.5 | 0.081 |
| Unpublished | 8 | 2450 | 943 | 36.8 (24.9–50.5) | 11.2 | 0.059 |
SNNPR South nations, nationalities and peoples region
a One study is divided in to two datasets by study period making the total dataset 38
b Includes (PCR, culture, rapid urease, methylyne blue stain, giemsa stain, loefler stain, histopatholgy, silver stain, gemnieze stain, gram stain,….)
Factors associated with H.pylori infection
Factors associated with H.pylori infections were grouped in to; sociodemographic, environmental, behavioral and clinical factors. Summary odds ratios (ORs) and their respective 95% confidence intervals (CIs) were computed based on the random effects model. Whenever there was data from the studies, we have tried to summarize the ORs and 95% CIs to identify the factors associated with H.pylori infections.
Socio-demographic risk factors
Available sociodemographic data (by age, sex, residency and level of education) were extracted and analyzed to determine their possible association with H.pylori infection but none of these variables had significant association. Even though not significant; male participants (OR = 1.07; 95% CI: 0.93–1.23; p = 0.33) and urban residents (OR = 1.04; 95% CI: 0.74–1.74; p = 0.83) were more likely to be infected with H.pylori than their counter parts (Fig. 4).
Fig. 4.

Sociodemographic factors associated with H.pylori infection by sex (a); by age group (b); by educational level (c) and by residency (d)
Environmental factors
Sources of drinking water, hand washing before meal and after toilet were the environmental factors assessed for their possible association with H.pylori infection. Participants who were not washing their hands after toilet were more likely to be infected with H.pylori (OR = 1.8; 95% CI: 1.19–2.72; p = 0.005). Other variables had no significant association (Fig. 5).
Fig. 5.

Environmental factors associated with H.pylori infection by type of water source for drinking (a); and by hand washing habit after toilet (b)
Behavioral factors
Chat chewing, cigarette smoking and drinking alcohol were analyzed for any association with H.pylori infection. Even though not significant, chat chewing had a preventive effect (OR = 0.94; 95% CI: 0.58–1.53; p = 0.80) for H.pylori infection while smoking increases the risks of infection (OR = 1.25; 95% CI: 0.67–2.30; p = 0.48). Participants who were taking alcohol had a significant association with H.pylori infection (OR = 1.34; 95% CI: 1.03–1.74; p = 0.03) (Fig. 6).
Fig. 6.

Behavioral factors associated with H.pylori infection chat chewing (a); by cigarette smoking (b) and by alcohol consumption (c)
Clinical factors
Gastrointestinal (GI) symptoms, allergic reactions, hyperemesis gravidarum, HIV and TB infections were some of the clinical factors reported with H.pylori infection by included studies. Because studies on allergic reactions, hyperemesis gravidarum, HIV and TB infections are small enough to compute pooled summary of odds ratios, we analyzed only the association between GI symptoms and H.pylori infection. Hence; participants who had GI symptoms (including dyspepsia, gastritis, peptic ulcer and related) were more likely to be infected with H.pylori (OR = 2.23; 95% CI: 1.59–3.14; p < 0.00001) (Fig. 7).
Fig. 7.

Clinical factors associated with H.pylori infection by gastrointestinal (GI) symptoms
Meta-regression
Meta-regression was done to explore the trend of prevalence of H.pylori by year of study and sample size of the included studies. A significant downward trend of H.pylori infection was observed from 1990 to 2017 (B = − 0.067, p = 0.00004). However; there was no significant association between prevalence of H.pylori and sample size of the studies even though there was a slight decrease of prevalence of H.pylori with increased sample size (B = − 0.00079; p = 0.193) (Fig. 8).
Fig. 8.

Meta-regression of the prevalence H.pylori infection by year of study (B = −0.067, p = 0.00004) (a); and sample size of studies (B = −0.00079, p = 0.193) (b)
Discussion
The global prevalence of H.pylori infection was estimated at 48.5% in 2017 [6]. The World Gastroenterology Organization (WGO) in its 2011 global guideline reported prevalence of > 95% among adults, 48% among 2–4 age groups and 80% among children aged at six in Ethiopia [1] but there was no national pooled prevalence reported yet. Estimating the national and regional prevalence, trends of infection and associated factors is crucial to establish appropriate strategies for the diagnosis, prevention and control of H.pylori infection. Estimates of H.pylori infection is usually challenging since some factors have profound effect than others and some studies look in to distinct population or samples, method of isolation, geographical distribution, socioeconomic, behavioral, environmental and clinical factors.
The 37 studies included in our analysis determined the prevalence of antigens and/or antibodies (either IgM, IgA or IgG) of H.pylori and ranged from 7.7 to 91.0% among different study populations, geographical areas and study period. However, the overall pooled prevalence of H.pylori in Ethiopia was estimated to be 52.2% (95% CI: 45.8–58.6). This overall prevalence estimate is lower than reports from Nigeria (87.7%), South Africa (77.6%), Portugal (86.4%), Tunisia (72.8%), Brazil (71.2%) and Estonia (82.5%) [6]. Some reasons may explain the lower prevalence in Ethiopia. Firstly; the number of studies and participants included; pooled from 37 studies and 18,890 participants in our analysis compared to fewer number of studies and participants. Second, our analysis included recent reports which showed a decreasing trend to recent times. Third, most of the laboratory tests used by studies included in our review were based on stool antigen for detection of H.pylori; which has low isolation rate.
However, our estimate is higher than other countries; 22.1% in Denmark, 43.6% in Thailand, 46.8% in Democratic republic of Congo (DRC) and 40.9% in Egypt [6]. These differences might be attributable to differences in time trend of studies, poor personal and environmental hygiene, low socioeconomic status and behavioral factors; and sensitivity/specificity of laboratory tests employed in detecting H.pylori. Stool antigen and serological tests were the most widely used methods used in detecting H.pylori infection.
The trend of H.pylori infection showed a decreasing pattern in the last three decades from 1990 to 2017; 64.4% in the first decade (1990–2000), 62.2% in the second decade (2001–2011) and 42.9% in the third decade (2012–2017). This decrement might be related with relative improvements in sanitation, water access, life style and behavioral changes, quality of life and socioeconomic status, and increased awareness on the transmission, diagnosis, eradication therapy, prevention and control of H.pylori infection.
Regional estimates of H.pylori infection in the subgroup analysis showed a lower prevalence of 39.9% in Oromia and higher prevalence of 71.0% in Somalia region. This regional difference can be attributable that in Somalia, study participants were University students with known gastritis which is a known risk factor for H.pylori infection. Other explanations could be related with sociodemographic, socioeconomic, environmental, clinical, behavioral factors and number of studies included in each category.
The prevalence of H.pylori infection differs on the bases of laboratory tests used. Higher prevalence was observed when detection is supplemented with sensitive tests including PCR, culture, rapid urease test and histopathology as shown in (Table 3). This is supported by studies comparing diagnostic tests for H.pylori that sensitive tests improve the detection rate of H.pylori infections from clinical samples [74–77]. In addition, combination of at least two diagnostic methods is recommended to increase the validity of results [16, 20, 28, 48, 63, 78–82], but only ten studies used multiple tests to make a definitive diagnosis of H.pylori in our analysis. Our subgroup analysis confirms that the pooled prevalence of H.pylori infection when multiple tests are used is higher than the pooled prevalence when a single test is used to detect H.pylori infection (62.9% Vs 48.1%).
Several risk factors for H.pylori infection were identified and reported usually with conflicting result. These factors are to be analyzed and pooled to have a summary of effect sizes. The results of this meta-analysis showed that participants with gastrointestinal (GI) symptoms were more likely to be infected with H.pylori (OR = 2.23; 95% CI: 1.59–3.14). This could be due to the effect of GI symptoms providing a growing medium (changing pH, thinning of gastric wall, gastric ulceration, change in gut microbiota) for the bacteria.
Although the type and level of alcohol, amount and frequency of consumption were not described, individuals taking alcohol were more likely to be infected with H.pylori infection than those who did not consume alcohol. This result is inconsistent with previous studies [83–86] reporting that alcohol consumption has either a protective effect or has no any relation with H.pylori infection. Other study [87] reported alcohol as a risk factor for H.pylori supporting our analysis. As alcohol is known to directly damage the gastric mucosal layer, it is theoretically possible that alcohol can provide ways for H.pylori infection. In addition, heavy drinking can possibly predispose consumers to social contacts that favor transmission of H.pylori infection. Other mechanism may be involved in the synergistic effect of alcohol including bacterial adherence and host factors in facilitating infection among drinkers. Further longitudinal and epidemiological studies are needed to test these explanations.
Previous studies [1, 86, 88] have reported that the prevalence of H.pylori infection seems to increase with age but the increment with age is assumed most likely due to cohort effect. As most infections are acquired early in life; the bacteria usually persists indefinitely unless treated with specific antibiotic. In our analysis, consistent with the assumption, participants in the age of <20 years were less likely to be infected when compared to above 20 years of age but the association is not significant (OR = 0.85; 95% CI: 0.70–1.03).
Poor sanitation and unsafe food and water were repeatedly reported as risk factors contributing for H.pylori infection. In our analysis, individuals who were not washing their hands after toiled were more likely to be infected with H.pylori. This is in agreement with previous studies [1, 41] and can be explained that H.pylori is largely transmitted through feco-oral or oral-oral routes. Lack of proper sanitation and basic hygiene after toilet, therefore; can be source of infection and increase the chance of acquiring H.pylori. World Health Organization (WHO) has also identified it as one of the greatest risks for human health and categorized it as a high priority pathogen for research and development of new and effective treatments [35].
In the meta-regression analysis, the prevalence of H.pylori infection showed a significant downward trend from 1990 to 2017 (B = − 0.067, p = 0.00004). This can be due to relative improvements in sanitation, water access, lifestyle and behavioral changes, quality of life and socioeconomic status, increased awareness on the transmission, diagnosis, eradication therapy, preventive and control of H.pylori infection. On the other hand; a slight decrement of prevalence of H.pylori was observed with increased sample size (B = − 0.00079; p = 0.193) but the association was not significant. This might be related with the numbers of studies done on large sample sizes in that only few studies were done when compared to numbers of studies done on small sample sizes.
Strengths and limitations
The strength of this study is that it included relatively larger numbers of published and unpublished studies without time limit of publication year. It has provided the national pooled prevalence, trends of infection and identified factors associated with H.pylori infection. The study included sub-group analysis and meta-regression of differences of study area, laboratory tests, study period, sample size and study designs. In few regions of Ethiopia, no study was found from and most identified studies were hospital based which could affect the generalisability of our findings. Moreover, there was lack of data sets to investigate the association between H.pylori infection and possible risk factors and the outcome variables may be affected by other cofounders.
Conclusion
The prevalence of H.pylori infection remains high; more than half of Ethiopians were infected and significant association was observed between H.pylori infection and absence of hand washing after toilet, alcohol drinking and presence of gastrointestinal (GI) symptoms. These findings strengthen the action to implement the control and prevention of H.pylori infection more effectively to prevent gastric cancer and other related complications in Ethiopia. Although the trend of infection showed a decreasing pattern; appropriate use of eradication therapy, health education primarily to improve knowledge and awareness on the transmission dynamics of the bacteria, behavioral changes, adequate sanitation, population screening and diagnosis using multiple tests are required to reduce H.pylori infections.. Recognizing the bacteria as a priority issue and designing gastric cancer screening policies are also recommended.
Additional file
Newcastle-Ottawa Scale for cross sectional studies. (DOC 34 kb)
Acknowledgements
Not applicable.
Funding
The authors declare that they did not receive funding for this research from any source.
Availability of data and materials
All data generated or analyzed are included in the results of the manuscript and its supplementary files.
Abbreviations
- EIA
Enzyme immune assay
- ELISA
Enzyme linked immunosorbent assay
- GI
Gastrointestinal
- H.pylori
Helicobacter pylori
- MALT
Mucosal-associated lymphoid tissue
- NUD
Non-ulcer dyspepsia
- PCR
Polymerase chain reaction
- RUT
Rapid urease test
- UBT
Urea breath test
- WGO
World Gastroenterology organization
- WHO
World health organization
Authors’ contributions
AM: Conceived and designed the study; analyzed data, and drafted the manuscript. AM, CG, BZ, and TA select and assess quality of studies, extract data, interpret result, and review the manuscript. All authors read and approved the manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Addisu Melese, Email: addisum22@gmail.com.
Chalachew Genet, Email: chaliegenet@gmail.com.
Balew Zeleke, Email: balew2006@gmail.com.
Tesfaye Andualem, Email: tesfayeandu@gmail.com.
References
- 1.Hunt RH, Xiao SD, Megraud F, et al. Helicobacter pylori in developing countries, world gastroenterology organisation global guideline. J Gastrointestin Liver Dis. 2011;20(3):299–304. [PubMed] [Google Scholar]
- 2.GO MF. Review article: natural history and epidemiology of helicobacter pyloriinfection. Aliment Pharmacol Ther. 2002;16(Suppl. 1):3–15. doi: 10.1046/j.1365-2036.2002.0160s1003.x. [DOI] [PubMed] [Google Scholar]
- 3.Zabala Torrres B, Lucero Y, Lagomarcino AJ, et al. Prevalence and dynamics of Helicobacter pylori infection during childhood. Helicobacter. 2017;22:e12399. doi: 10.1111/hel.12399. [DOI] [PubMed] [Google Scholar]
- 4.O’Connor A, O’Morain CA, Ford AC. Population screening and treatment of Helicobacter pylori infection. Nat Rev Gastroenterol Hepatol. 2017;14:230–240. doi: 10.1038/nrgastro.2016.195. [DOI] [PubMed] [Google Scholar]
- 5.Jemilohun AC, Otegbayo JA, Ola SO, et al. Prevalence of helicobacter pylori among Nigerian patients with dyspepsia in Ibadan. Pan Afr Med J. 2011;6:18. doi: 10.4314/pamj.v6i1.69090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.James KY, WYL H, Ng WK, et al. Global prevalence of helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. 2017;153:420–429. doi: 10.1053/j.gastro.2017.04.022. [DOI] [PubMed] [Google Scholar]
- 7.Salih BA. Helicobacter pylori infection in developing countries: the burden for how long? Saudi J Gastroenterol. 2009;15(3):201–207. doi: 10.4103/1319-3767.54743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lindkvist PA, D. Nilsson, et al. age at acquisition of helicobacter pylori infection: comparison of a high and a low prevalence country. Scand J Infect Dis. 1996;28(2):181–184. doi: 10.3109/00365549609049072. [DOI] [PubMed] [Google Scholar]
- 9.Miele ERE. Helicobacter pylori Infection in Pediatrics. Helicobacter. 2015;20(Suppl. S1):47–53. doi: 10.1111/hel.12257. [DOI] [PubMed] [Google Scholar]
- 10.Matjazˇ Homan IH, Kolacˇek S. Helicobacter pylori in pediatrics. Helicobacter. 2012;17(Suppl.1):43–48. doi: 10.1111/j.1523-5378.2012.00982.x. [DOI] [PubMed] [Google Scholar]
- 11.Ng QX, Venkatanarayanan N, De Deyn MLZQ, et al. A meta-analysis of the association between Helicobacter pylori (H. pylori) infection and hyperemesis gravidarum. Helicobacter. 2017;23:e12455. doi: 10.1111/hel.12455. [DOI] [PubMed] [Google Scholar]
- 12.Iraj Nabipour KV, Jafari SM, et al. The association of metabolic syndrome and Chlamydia pneumoniae, Helicobacter pylori, cytomegalovirus, and herpes simplex virus type 1: The Persian Gulf Healthy Heart Study. Cardiovasc Diabetol. 2006;5:25. doi: 10.1186/1475-2840-5-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Michael A, Mendall PMG, Molineaux N, et al. Relation of Helicobacter pyloi infection and coronary heart disease. Br Heart J. 1994;71:437–439. doi: 10.1136/hrt.71.5.437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Taye B, Enquselassie F, Tsegaye A, et al. Effect of early and current helicobacter pylori infection on the risk of anaemia in 6.5-year-old Ethiopian children. BMC Infect Dis. 2015;15:270. doi: 10.1186/s12879-015-1012-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kibru D, Gelaw B, Alemu A, et al. Helicobacter pylori infection and its association with anemia among adult dyspeptic patients attending Butajira Hospital, Ethiopia. BMC Infect Dis. 2014;14:656. doi: 10.1186/s12879-014-0656-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ali MAH, Muhammad EM, Hameed BH, et al. The impact of Helicobacter pylori infection on iron deficiency anemia in pregnancy. Iraqi J Hematol. 2017;6(2):60. doi: 10.4103/ijh.ijh_19_17. [DOI] [Google Scholar]
- 17.Lauren Hudak AJ, Haj S, et al. An updated systematic review and meta- analysis on the association between Helicobacter pyloriinfection and iron deficiency anemia. Helicobacter. 2017;22:e12330. doi: 10.1111/hel.12330. [DOI] [PubMed] [Google Scholar]
- 18.Alshareef SA, Rayis DA, Adam I, et al. Helicobacter pyloriinfection, gestational diabetes mellitus and insulin resistance among pregnant Sudanese women. BMC Res Notes. 2018;11:517. doi: 10.1186/s13104-018-3642-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jeon CY, Haan MN, Cheng C, et al. Helicobacter pylori infection is associated with an increased rate of diabetes. Diabetes Care. 2012;35:520–5. [DOI] [PMC free article] [PubMed]
- 20.Tseng C-H. Diabetes, insulin use and Helicobacter pylori eradication: a retrospective cohort study. BMC Gastroenterol. 2012;12:46. doi: 10.1186/1471-230X-12-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Abdulbari Bener RM, Afifi M, et al. Association between type 2 diabetes mellitus and helicobacter pylori infection. Turk J Gastroenterol. 2017;18(4):225–229. [PubMed] [Google Scholar]
- 22.Mengge Zhou JL, Qi Y, et al. Association between Helicobacter pylori infection and risk of new-onset diabetes: a community-based, prospective cohort study. Lancet Endocrinol. 2016;14. www.thelancet.com/diabetes-endocrinology.
- 23.Mohammadreza Motie AR, Abbasi H, et al. The Relationship Between Cholecystitis and Presence of Helicobacter pylori in the Gallbladder. Zahedan J Res Med Sci. 2017;19(7):e9621. [Google Scholar]
- 24.Li Cen JP, Zhou B, et al. Helicobacter Pyloriinfection of the gallbladder and the risk of chronic cholecystitis and cholelithiasis: A systematic review and meta- analysis. Helicobacter. 2018;23:e12457. doi: 10.1111/hel.12457. [DOI] [PubMed] [Google Scholar]
- 25.Moges F, Kassu A, Mengistu G, et al. Seroprevalence of helicobacter pylori in dyspeptic patients and its relationship with HIV infection, ABO blood groups and life style in a university hospital, Northwest Ethiopia. World J Gastroenterol. 2006;12(12):1957–1961. doi: 10.3748/wjg.v12.i12.1957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Getachew Seid KD, Tsegaye A. Helicobacter pylori infection among dyspeptic and non-dyspeptic HIV patients at YekaHealth center, Addis Ababa, Ethiopia. 2017. [Google Scholar]
- 27.Sarfo FS, Eberhardt KA, Dompreh A, et al. Helicobacter pylori Infection is associated with higher CD4 T cell counts and lower HIV-1 viral loads in ART-Naïve HIV-positive patients in Ghana. PLoS One. 2015;10:e0143388. doi: 10.1371/journal.pone.0143388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Taye B, Enquselassie F, Tsegaye A, et al. Effect of helicobacter pylori infection on growth trajectories in young Ethiopian children: a longitudinal study. Int J Infect Dis. 2016;50:57–66. doi: 10.1016/j.ijid.2016.08.005. [DOI] [PubMed] [Google Scholar]
- 29.Shen X, Yang H, Wu Y, Zhang D, Jiang H. Meta-analysis: Association of Helicobacter pylori infection with Parkinson’s diseases. Helicobacter. 2017;22:e12398. doi: 10.1111/hel.12398. [DOI] [PubMed] [Google Scholar]
- 30.Mégraud F. Time to change approaches to helicobacter pylori management. Lancet Gastroenterol Hepatol. 2017;2:692–693. doi: 10.1016/S2468-1253(17)30245-5. [DOI] [PubMed] [Google Scholar]
- 31.Seck A, Burucoa C, Dia D, et al. Primary antibiotic resistance and associated mechanisms in Helicobacter pylori isolates from Senegalese patients. Annals of Clinical Microbiology and Antimicrobials. 2013;12:3. doi: 10.1186/1476-0711-12-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Vakil N, Vaira D. Treatment for H. pylori infection: new challenges with antimicrobial resistance. J Clin Gastroenterol. 2013;47(5):383–388. doi: 10.1097/MCG.0b013e318277577b. [DOI] [PubMed] [Google Scholar]
- 33.Jaka H, Rhee JA, Östlundh L, et al. The magnitude of antibiotic resistance to Helicobacter pylori in Africa and identified mutations which confer resistance to antibiotics: systematic review and meta-analysis. BMC Infectious Diseases. 2018;18:193. doi: 10.1186/s12879-018-3099-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ferenc S, Gnus J, Kościelna M, et al. High antibiotic resistance of Helicobacter pylori and its effect on tailored and empiric eradication of the organism in Lower Silesia, Poland. Helicobacter. 2017;22:e12365. [DOI] [PubMed]
- 35.Dang BN, Graham DY. Helicobacter pylori infection and antibiotic resistance: a WHO high priority. Nat Rev Gastroenterol Hepatol. 2017;14(1):383–384. doi: 10.1038/nrgastro.2017.57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Asrat D, Kassa E, Mengistu Y, et al. Antimicrobial susceptibility pattern of helicobacter pylori strains isolated from adult dyspeptic patients in Tikur Anbassa University Hospital, Addis Ababa, Ethiopia. Ethiop Med J. 2004;42(2):79–85. [PubMed] [Google Scholar]
- 37.Ben Mansour K, Burucoa C, Zribi M, et al. Primary resistance to clarithromycin, metronidazole and amoxicillin of Helicobacter pylori isolated from Tunisian patients with peptic ulcers and gastritis: a prospective multicentre study. Ann Clin Microbiol Antimicrob. 2010;9:22. doi: 10.1186/1476-0711-9-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kuo Y-T, Liou JM, El-Omar EM, et al. Primary antibiotic resistance in Helicobacter pylori in the Asia-Pacific region: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2017;2:707–715. doi: 10.1016/S2468-1253(17)30219-4. [DOI] [PubMed] [Google Scholar]
- 39.Ayele B, Molla E. Dyspepsia and Associated Risk Factors at Yirga Cheffe Primary Hospital, Southern Ethiopia. Clin Microbiol. 2017;6:3. doi: 10.4172/2327-5073.1000282. [DOI] [Google Scholar]
- 40.Asrat D, Nilsson I, Mengistu Y, et al. Prevalence of helicobacter pylori infection among adult dyspeptic patients in Ethiopia. Ann Trop Med Parasitol. 2004;98(2):181–189. doi: 10.1179/000349804225003190. [DOI] [PubMed] [Google Scholar]
- 41.Natuzzi E. Neglected tropical diseases: is it time to add helicobacter pylorito the list? Glob Health Promot. 2013;20(3):47–48. doi: 10.1177/1757975913499037. [DOI] [PubMed] [Google Scholar]
- 42.Tedla Z. Helicobacter pylori infection in patients with upper gastrointestinal symptoms in Arba Minch hospital: southwestern Ethiopia. Ethiop Med J. 1992;30(1):43–49. [PubMed] [Google Scholar]
- 43.LA Moher D, Tetzlaff J, Altman DG, The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009;6(6):e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Yilikal Assefa KD. Association of Helicobacter pylori infection and hyperemesis gravidarum women: a case control study in selected Hospital and two health centers in Kirkos Sub-city, Addis Ababa, Ethiopia. 2017. [Google Scholar]
- 45.Kebede W, Mathewos B, Abebe G. H. PyloriPrevalence and its effect on CD4+Lymphocyte count in active pulmonary tuberculosis patients at hospitals in Jimma, Southwest Ethiopia. Int J Immunol. 2015;3(1):7–13. doi: 10.11648/j.iji.20150301.12. [DOI] [Google Scholar]
- 46.Tadege T, Mengistu Y, Desta K, Asrat D. Serioprevalence of Helicobacter pylori Infection in and its Relationship with ABO Blood Groups. Ethiop J Health Dev. 2015;9(1):55–59. [Google Scholar]
- 47.Tebelay Dilnessa MA. Prevalence of helicobacter pylori and risk factors among dyspepsia and non-dyspepsia adults at Assosa general hospital, West Ethiopia: a comparative study. Ethiop J Health Dev. 2017;31(1):4–12. [Google Scholar]
- 48.Tadesse E, Daka D, Yemane D, Shimelis T. Seroprevalence of helicobacter pylori infection and its related risk factors in symptomatic patients in southern Ethiopia. BMC Res Notes. 2014;7:834. doi: 10.1186/1756-0500-7-834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Taddesse G, Habteselassie A, Desta K, et al. Association of dyspepsia symptoms and helicobacter pylori infections in private higher clinic, Addis Ababa, Ethiopia. Ethiop Med J. 2011;49(2):109–116. [PubMed] [Google Scholar]
- 50.Seid A, Tamir Z, Kasanew B, Senbetay M. Co-infection of intestinal parasites and helicobacter pylori among upper gastrointestinal symptomatic adult patients attending Mekanesalem hospital, Northeast Ethiopia. BMC Res Notes. 2018;11(1):144. doi: 10.1186/s13104-018-3246-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Seid A, Tamir Z, Demsiss W. Uninvestigated dyspepsia and associated factors of patients with gastrointestinal disorders in Dessie referral hospital, Northeast Ethiopia. BMC Gastroenterol. 2018;18(1):13. doi: 10.1186/s12876-017-0723-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kumera Terfa KD. Prevalence of helicobacter pylori infections and associated risk factors among women of child bearing ages in selected health centers, Kolfe Keranio sub city, Addis Ababa. 2015. [Google Scholar]
- 53.Kassu Desta DA, Derbie F. Seroprevalence of Helicobacter pylori infection among health blood donors in Addis Ababa Ethiopia. Ethiop J Health Sci. 2002;12:2. [Google Scholar]
- 54.Hailu G. Prevalence and Risk Factors of Helicobacter pylori among Adults at Jinka Zonal Hospital, Debub Omo Zone, Southwest Ethiopia. Autoimmune Infect Dis. 2016;2:2. [Google Scholar]
- 55.Getachew Alebie DK. Prevalence of Helicobacter PyloriInfection and Associated Factors among Gastritis Students in Jigjiga University, Jigjiga, Somali Regional State of Ethiopia. J Bacteriol Mycol. 2016;3:3. [Google Scholar]
- 56.Eden Ababu KD, Hailu M. H.Pyloriinfection and its association with CD4 T cell count among HIV infected individuals who attended the ART service in kotebe health center, Yeka subcity, Addis Ababa, Ethiopia. 2017. [Google Scholar]
- 57.Misganaw Birhaneselassie AA. The relationship between dyspepsia and H. pylori infection in Southern Ethiopia Global Advanced Research. J Med Med Sci. 2017;6(5):086–090. [Google Scholar]
- 58.Alemayehu A. Seroprevalence of helicobacter pylori infection and its risk factors among adult patients with dyspepsia in Hawassa teaching and referral hospital, south Ethiopia. 2011. [Google Scholar]
- 59.Lindkvist P, Enquselassie F, Asrat D, et al. Helicobacter pylori infection in Ethiopian children: a cohort study. Scand J Infect Dis. 1999;31(5):475–480. doi: 10.1080/00365549950163996. [DOI] [PubMed] [Google Scholar]
- 60.Lindkvist P, Enquselassie F, Asrat D, et al. Risk factors for infection with helicobacter pylori - a study of children in rural Ethiopia. Scand J Infect Dis. 1998;30(4):371–376. doi: 10.1080/00365549850160666. [DOI] [PubMed] [Google Scholar]
- 61.Amberbir A, Medhin G, Erku W, et al. Effects of helicobacter pylori, geohelminth infection and selected commensal bacteria on the risk of allergic disease and sensitization in 3-year-old Ethiopian children. Clin Exp Allergy. 2011;41(10):1422–1430. doi: 10.1111/j.1365-2222.2011.03831.x. [DOI] [PubMed] [Google Scholar]
- 62.Amberbir A, Medhin G, Abegaz W, et al. Exposure to helicobacter pylori infection in early childhood and the risk of allergic disease and atopic sensitization: a longitudinal birth cohort study. Clin Exp Allergy. 2014;44(4):563–571. doi: 10.1111/cea.12289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Gobena MT. Association of Helicobacter pylori infection with atopy and allergic disorders in Ziway, Central Ethiopia. 2017. [Google Scholar]
- 64.Ahmed Kemal GM. Prevalence of H.pylori infection in pediatric patients who is clinically diagnosed for gastroenteritis in Beham specialized children’s higher clinic, Addis Ababa, Ethiopia. 2014. [Google Scholar]
- 65.Abebe Worku KD, Wolde M. Prevalence of Helicobacter pylori and intestinal parasite and their associated risk factors among school children at Selam Fire Elementary School in Akaki Kality, Addis Ababa, Ethiopia. 2017. [Google Scholar]
- 66.Workineh M, Andargie D. A 5-year trend of helicobacter pylori seroprevalence among dyspeptic patients at Bahir Dar Felege Hiwot referral hospital, Northwest Ethiopia. Res Rep Trop Med. 2016;7:17–22. doi: 10.2147/RRTM.S105361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Seid A, Demsiss W. Feco-prevalence and risk factors of helicobacter pylori infection among symptomatic patients at Dessie referral hospital, Ethiopia. BMC Infect Dis. 2018;18(1):260. doi: 10.1186/s12879-018-3179-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Mathewos B, Moges B, Dagnew M. Seroprevalence and trend of Helicobacter pylori infection in Gondar University Hospital among dyspeptic patients, Gondar, North West Ethiopia. BMC Res Notes. 2013;6:346. doi: 10.1186/1756-0500-6-346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Kasew D, Abebe A, Munea U, et al. Magnitude of helicobacter pylori among dyspeptic patients attending at University of Gondar Hospital, Gondar, Northwest Ethiopia. Ethiop J Health Sci. 2017;27(6):571–580. doi: 10.4314/ejhs.v27i6.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Henriksen TH, Nysaeter G, Madebo T, et al. Peptic ulcer disease in South Ethiopia is strongly associated with helicobacter pylori. Trans R Soc Trop Med Hyg. 1999;93(2):171–173. doi: 10.1016/S0035-9203(99)90297-3. [DOI] [PubMed] [Google Scholar]
- 71.Teka B, Gebre-Selassie S, Abebe T. Sero-prevalence of helicobacter Pylori in HIV positive patients and HIV negative controls in St. Paul’s general specialized hospital, Addis Ababa, Ethiopia. Sci J Public Health. 2016;4(5):387–393. doi: 10.11648/j.sjph.20160405.14. [DOI] [Google Scholar]
- 72.Abebaw W, Kibret M, Abera B. Prevalence and risk factors of H. pylori from dyspeptic patients in northwest Ethiopia: a hospital based cross-sectional study. Asian Pac J Cancer Prev. 2014;15(11):4459–4463. doi: 10.7314/APJCP.2014.15.11.4459. [DOI] [PubMed] [Google Scholar]
- 73.Tsega E, Gebre W, Manley P, Asfaw T. Helicobacter pylori, gastritis and non-ulcer dyspepsia in Ethiopian patients. Ethiop Med J. 1996;34(2):65–71. [PubMed] [Google Scholar]
- 74.Daniel Asrat EK, Mengistu Y, et al. Comparison of Diagnostic Methods for Detection of Helicobacter pyloriInfection in Different Clinical Samples of Ethiopian Dyspeptic Patients. Asian J Cancer. 2007;6:4. [Google Scholar]
- 75.Fatemeh Khadangi MY, Kerachian MA. Review: Diagnostic accuracy of PCR-based detection tests for Helicobacter Pylori in stool samples. Helicobacter. 2017;22:e12444. doi: 10.1111/hel.12444. [DOI] [PubMed] [Google Scholar]
- 76.Calvet X, Sánchez-Delgado J, Montserrat A, et al. Accuracy of Diagnostic Tests for Helicobacter pylori: A Reappraisal. Clin Infect Dis. 2009;48:1385–1391. doi: 10.1086/598198. [DOI] [PubMed] [Google Scholar]
- 77.Ante Tonkic MT, Lehours P, Mégraud F. Epidemiology and diagnosis of helicobacter pylori infection. Helicobacter. 2012;17:1–8. doi: 10.1111/j.1523-5378.2012.00975.x. [DOI] [PubMed] [Google Scholar]
- 78.Chen Y, Segers S, Blaser MJ. Association between Helicobacter pylori and mortality in the NHANES III study. MJ Gut. 2013;62:1262–1269. doi: 10.1136/gutjnl-2012-303018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Megraud F, Gisbert JP. Towards effective empirical treatment for Helicobacter pylori eradication. Lancet. 2016;388:2325–2326. doi: 10.1016/S0140-6736(16)31657-9. [DOI] [PubMed] [Google Scholar]
- 80.Macías-García F, Llovo-Taboada J, Díaz-López M, et al. High primary antibiotic resistance of Helicobacter Pylori strains isolated from dyspeptic patients: A prevalence cross-sectional study in Spain. Helicobacter. 2017. 10.1111/hel.12440. [DOI] [PubMed]
- 81.Shanks AM, El-Omar EM. Helicobacter pylori infection, host genetics and gastric cancer. J Dig Dis. 2009;10:157–164. doi: 10.1111/j.1751-2980.2009.00380.x. [DOI] [PubMed] [Google Scholar]
- 82.Manfred Stolte AM. Helicobacter pyloriand gastric Cancer. Oncologist. 1998;3:124–128. [PubMed] [Google Scholar]
- 83.Nikanne JH. Effect of alcohol consumption on the risk of helicobacter pylori infection. Digestion. 1991;50:92–98. doi: 10.1159/000200745. [DOI] [PubMed] [Google Scholar]
- 84.Hermann Brenner GB, Lappus N, et al. Alcohol consumption and helicobacter pylori infection: results from the German National Health and nutrition survey. Epidemiology. 1999;10(3):214–218. doi: 10.1097/00001648-199905000-00004. [DOI] [PubMed] [Google Scholar]
- 85.Atsushi Ogihara SK, Hasegawa A, et al. Relationship between helicobacter pylori infection and smoking and drinking habits. J Gastroenterol Hepatol. 2000;15:271–276. doi: 10.1046/j.1440-1746.2000.02077.x. [DOI] [PubMed] [Google Scholar]
- 86.Mark Woodward CM, McColl K. An investigation into factors associated with Helicobacter pylori infection. J Clin Epidemiol. 2000;53:175–181. doi: 10.1016/S0895-4356(99)00171-7. [DOI] [PubMed] [Google Scholar]
- 87.Li Zhang GDE, Harry H, et al. Relationship between alcohol consumption and active helicobacter pylori infection. Alcohol Alcohol. 2010;45(1):89–94. doi: 10.1093/alcalc/agp068. [DOI] [PubMed] [Google Scholar]
- 88.Eusebi LH, Zagari RM, Bazzoli F. Epidemiology of Helicobacter pylori infection. Helicobacter. 2014;19(Suppl. 1):1–5. doi: 10.1111/hel.12165. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Newcastle-Ottawa Scale for cross sectional studies. (DOC 34 kb)
Data Availability Statement
All data generated or analyzed are included in the results of the manuscript and its supplementary files.