

Abstract
Purpose:
Safety and feasibility of distal radial artery cannulation at the anatomic snuffbox in the perioperative settings in adult patients have been assessed in this study.
Methods:
Adult patients undergoing elective surgery requiring arterial cannulation were recruited in this retrospective cohort study.
Results:
Data of 55 patients have been reviewed here; among which in 21 patients, arterial puncture was performed ultrasound guidance and in 34 patients puncture was guided by the pulsation of the distal radial artery at the anatomical snuffbox. First attempt success rate of distal radial arterial cannulation was 76.3% (42 of 55 patients) and it was similar between ultrasound guided (USG) and palpation technique (P = 0.53, Chi-square test). Overall, cannulation success rate was 87.3% (48 of 55 patients) and it was also similar between USG and palpation technique (P = 0.79, Chi-square test).
Conclusion:
Distal radial artery cannulation is technically feasible in patients undergoing elective surgery. However, further randomized controlled trials are required to establish its clinical utility and safety profile in comparison to conventional radial artery cannulation.
Keywords: Arterial cannulation, distal radial artery, ultrasonography, vascular access
Introduction
Arterial cannulation is a commonly performed invasive procedure used in operating room, intensive care unit, emergency department, and in cardiac catheterization laboratory. Arterial cannulation allows beat-to-beat blood pressure measurement, blood sampling for blood gas analysis, and can be used for guiding fluid therapy in critically ill or surgical patients.[1,2] Radial artery, being easily accessible because of its superficial location, is one of the most preferred sites for arterial cannulation and has a low rate of procedural complications from arterial cannulation.[3,4] Classically radial artery cannulation is performed by digital palpation method at the volar aspect of the wrist. Complications of radial artery cannulation are bleeding, hematoma formation, infection, arterial thrombosis, pseudoaneurysm formation, injury to the median nerve, etc.[1] Though the complications are uncommon, some of them have serious implications.
Distal radial artery cannulation at the anatomical snuffbox is a relatively less evaluated procedure. Distal radial artery cannulation has several possible advantages over the conventional radial artery cannulation at the wrist, such as catheterizing the dorsal radial artery has the advantage of cannulating more distally than with the traditional transradial approach, beyond the origin of the superficial palmar branch and in the anatomical snuff-box radial artery is not accompanied by any major motor nerve.
In this retrospective study, we have assessed safety and feasibility of distal radial artery cannulation at the anatomic snuffbox in the perioperative settings.
Methods
After obtaining permission from the Institute Ethics Committee, case records of 35 patients, where distal radial artery cannulation was used for perioperative management, were evaluated. Following data were collected for each patient: demographic data (age, sex, and body weight), use of USG for cannulation, first attempt success, overall success, use of any alternative technique, any complications (such as bleeding/thrombosis/hematoma/digital ischemia, etc.). Any intraoperative catheter-related complications, such as catheter dislodgement, blockages, etc., were also noted.
Results
Data of the 55 consecutive patients who underwent elective surgery requiring arterial cannulation for perioperative management were included in this cohort study. Median [interquartile range, IQR] of the included patients was 67 [58–79] years and 78% patients were male. A total of 47 patients were undergoing urological cancer surgery, 4 were undergoing gastrointestinal (GI) cancer surgery, and rests were undergoing thoracotomy. Median [IQR] duration of surgery was 210 [165–240] min. In all patients, arterial cannulation was performed after induction of general anesthesia and none of the patients had coronary or peripheral vascular diseases.
In 21 patients, arterial puncture was performed under real-time ultrasound guidance and in 34 patients puncture was guided by the pulsation of the distal radial artery at the anatomical snuffbox. First attempt success rate of arterial cannulation was 76.4% (42 of 55 patients) and it was similar between USG guided and palpation technique (17 of 21 patients in USG technique versus 25 of 34 patients in palpation technique; P = 0.53, Chi-square test). Overall, cannulation success rate was 87.3% (48 of 55 patients) and it was also similar between USG and palpation technique (18 of 21 patients in USG technique versus 30 of 34 patients in palpation technique; P = 0.79, Chi-square test). Hematoma was noted in only one patient and in none of the cases had intraoperative dislodgement or any other catheter-related problem. In all cases, arterial cannula was removed after uneventful recovery and no ischemic complication was documented. In all cases, a 20G polyurethane catheter was used for cannulation by Seldinger technique over a J-tipped guide wire.
Discussion
Our retrospective cohort study reported that distal radial artery cannulation was a technically feasible technique in perioperative medicine. Both palpation and USG-guided technique are feasible for this purpose.
Distal radial artery cannulation is relatively less explored technique in perioperative medicine. In 2014, a single case was reported where authors used distal radial artery cannulation in a 29-year-old patient who was undergoing living donor kidney transplantation surgery.[5] A recent cohort study reported that overall success rate of left distal artery cannulation was around 88%; however, USG was not used in cannulation in that study.[6] Soydan and Akın recently evaluated left distal radial artery cannulation for coronary angiography and intervention in 54 patients; they reported need for an alternative arterial cannulation site in 3.7% of the patients.[7] They also did not report any hematoma or neurological complications. Overall, success rate in our cohort was similar to the previous studies. Distal radial artery at the anatomical (Figure 1: Surface anatomy of ‘anatomical snuffbox’) has several possible advantages over conventional radial artery cannulation at the wrist including less chance of digital ischemia. However, whether actually this theoretical advantage is translated into a clinical one is not possible to interpret from this study. Distal radial artery cannulation has few important limitations; such as being a smaller diameter artery, it is prone to puncture mediated vasospasm.[7] In a number of cases, we noticed difficulty in negotiating guide-wire despite of pulsatile blood flow at the puncture needle hub, which was probably due to tortuous course of the distal radial artery at the anatomical snuffbox [Figure 2]. As radial artery at the anatomical snuffbox takes a curved course below the tendon of extensor pollicis brevis and abductor pollicis longus; it may also be difficult to negotiate an arterial catheter over the needle. Figure 3 shows position of a distal radial artery cannula at the anatomical snuff box.
Figure 1.

Surface anatomy of ‘anatomical snuffbox’ [Black triangle represents surface anatomy of the snuffbox]
Figure 2.
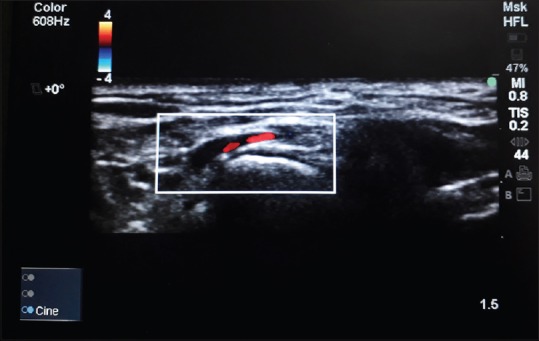
Ultrasonographic anatomy of distal radial artery at the ‘anatomical snuffbox’
Figure 3.

A 20G arterial line in situ in the anatomical snuffbox
Limitations
Our study has several limitations; such as being a small study with retrospective design, it is impossible to comment upon the safety profile of the technique. We used this technique only in patients undergoing elective surgery; so distal radial artery cannulation may not be feasible in patients who are hemodynamically unstable or requires inotropic support.
Conclusion
Distal radial artery cannulation is technically feasible in patients undergoing elective surgery. However, further randomized controlled trials are required to establish its clinical utility and safety profile in comparison to conventional radial artery cannulation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Scheer B, Perel A, Pfeiffer UJ. Clinical review: Complications and risk factors of peripheral arterial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care. 2002;6:199–204. doi: 10.1186/cc1489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gu WJ, Wu XD, Wang F, Ma ZL, Gu XP. Ultrasound guidance facilitates radial artery catheterization: A meta-analysis with trial sequential analysis of randomized controlled trials. Chest. 2016;149:166–79. doi: 10.1378/chest.15-1784. [DOI] [PubMed] [Google Scholar]
- 3.Brzezinski M, Luisetti T, London MJ. Radial artery cannulation: A comprehensive review of recent anatomic and physiologic investigations. Anesth Analg. 2009;109:1763–81. doi: 10.1213/ANE.0b013e3181bbd416. [DOI] [PubMed] [Google Scholar]
- 4.Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomised, parallel group, multicenter trial. Lancet. 2011;377:1409–20. doi: 10.1016/S0140-6736(11)60404-2. [DOI] [PubMed] [Google Scholar]
- 5.Choi S, Park JM, Nam SH, Kim EJ. Cannulation of the dorsal radial artery: An underused, yet useful, technique. Korean J Anesthesiol. 2014;67:S11–2. doi: 10.4097/kjae.2014.67.S.S11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kiemeneij F. Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI) EuroIntervention. 2017;13:851–7. doi: 10.4244/EIJ-D-17-00079. [DOI] [PubMed] [Google Scholar]
- 7.Soydan E, Akın M. Coronary angiography using the left distal radial approach - An alternative site to conventional radial coronary angiography. Anatol J Cardiol. doi: 10.14744/AnatolJCardiol.2018.59932. 2018 Mar 21. doi: 10.14744/Anatol JCardiol.2018.59932. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]