

Introduction
Atopic diseases, including atopic dermatitis and alopecia areata, are disease entities with much active research, as new biologic medications are emerging targeting each of these diseases. We report a case of a single biologic medication used to treat atopic dermatitis, leading to unexpected treatment for concurrent alopecia areata.
Case report
A 49-year-old woman with a long-standing history of atopic dermatitis since childhood presented with refractory atopic dermatitis. Past treatments included topical steroids, topical calcineurin inhibitors, phototherapy, and oral methotrexate, 20 mg/wk, all with mild to moderate control of disease. She necessitated intermittent oral prednisone bursts for severe flares. Her atopic dermatitis would often exceed 50% of body surface area (BSA) during flares, which she experienced monthly on average. At best with treatments, her atopic dermatitis covered 15% to 20% BSA. Complementary and alternative medicine methods were also pursued without improvement, including acupuncture and herbal supplements. Other significant comorbidities included a 6-year history of unrelated, sudden, adult-onset scalp alopecia areata that quickly progressed to alopecia universalis (Fig 1). She had cyclic sparse and patchy hair regrowth and loss over the course of the disease, without permanent hair regrowth or growth involving more than 5% of the scalp. Her eczema rarely involved the scalp, however.
Fig 1.
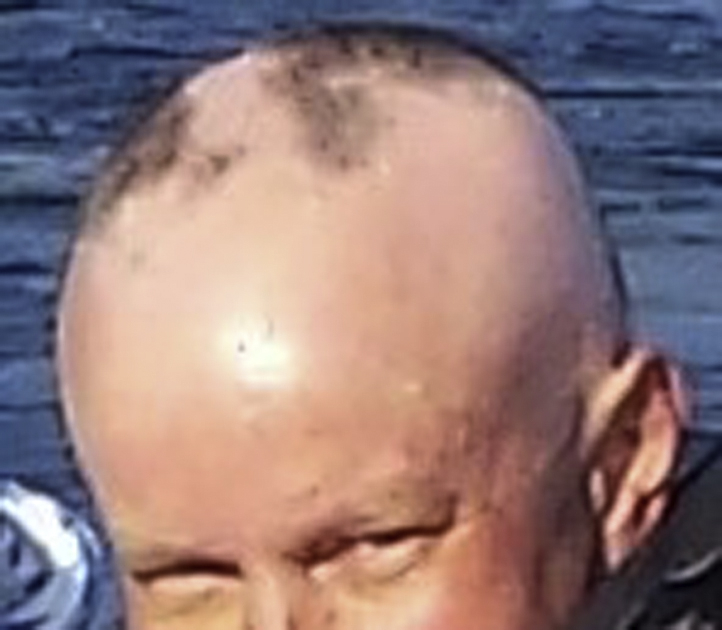
Patient with atopic dermatitis and alopecia universalis before therapy with dupilumab.
For the refractory atopic dermatitis, the patient was started on dupilumab, 300 mg subcutaneously, every other week after a loading dose of 600 mg subcutaneously, with significant improvement of cutaneous disease and quality of life. She currently only requires minimal topical treatments to control minor flares, with a BSA of less than 5% at all times.
After starting dupilumab for refractory atopic dermatitis, she noted immediate hair regrowth on the scalp. After 8 months of dupilumab use, she had full scalp hair regrowth, which she had lacked for the previous 6 years (Fig 2). Her eyebrows have also shown some regrowth, although the eyelashes and remainder of the body hair have yet to regrow. No adverse clinical symptoms or abnormal laboratory tests were observed with use of dupilumab in this patient.
Fig 2.

Patient with alopecia universalis shows full scalp hair regrowth and the start of eyebrow regrowth after 8 months of dupilumab therapy for concurrent atopic dermatitis.
Discussion
As many diseases have cytokine production pathways in common, it fits that one drug may be used to target multiple disease courses. Case reports and studies are beginning to emerge regarding the use of biologics for one disease that have concurrent effects on other diseases. For example, tofacitinib, a JAK 1/3 inhibitor, was originally approved for rheumatoid arthritis but has shown promising effects for patients with alopecia universalis.1 Although the pathophysiology of both atopic dermatitis and alopecia areata are still under research and debate, because atopic dermatitis and alopecia areata have similar robust helper T cell 2–mediated cytokine pathways with downstream effects manifesting in the skin, it is understandable that dupilumab, an interleukin (IL)-4 and IL-13 monoclonal antibody, would have effects on both diseases.2 Studies describe the association between these 2 diseases, indicating that IL-4 leads to production of inflammatory mediators such as IgE, mast cells, and eosinophils and that this inflammation is a main factor in disease manifestation. Blocking IL-4, in addition to inflammatory mediator IL-13, therefore, inhibits the downstream effects of inflammation that leads to these 2 pathologic diseases.3 In fact, dupilumab was recently reported to be effective in a patient with atopic dermatitis and concomitant alopecia areata.4 Although our patient's hair regrowth could have occurred spontaneously and without relation to dupilumab, our report of dupilumab being used for atopic dermatitis with striking hair regrowth in a patient with alopecia universalis is the second reported case, to the best of our knowledge, which may indicate the promising result of dupilumab in treating alopecia universalis, totalis, and areata, along with the already known positive effect on atopic dermatitis. However, further and larger studies are needed to fully assess the effects of dupilumab on diseases shared by the helper T cell 2 pathway, as a recent case emerged of alopecia areata onset after treatment of atopic dermatitis with dupilumab.5 Further and continued use of biologics will elucidate their effects on disease, as more patients continue to use systemic medications for myriad dermatologic conditions.
Footnotes
Funding sources: None.
Conflicts of interest: None disclosed.
References
- 1.Morris G.M., Nahmias Z.P., Kim B.S. Simultaneous improvement of alopecia universalis and atopic dermatitis in a patient treated with a JAK inhibitor. JAAD Case Rep. 2018;4(6):515–517. doi: 10.1016/j.jdcr.2017.12.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kilic, Arzu. New modalities in the treatment of refractory alopecia areata, hair, and scalp disorders. IntechOpen. DOI: 10.5772/66591.
- 3.Barahmani N., Schabath M.B., Duvic M. History of atopy or autoimmunity increases risk of alopecia areata. JAAD. 2009;61(4):581–591. doi: 10.1016/j.jaad.2009.04.031. [DOI] [PubMed] [Google Scholar]
- 4.Darrigade A.S., Legrand A., Andreu N. Dual efficacy of dupilumab in a patient with concomitant atopic dermatitis and alopecia areata. Br J Dermatol. 2018 doi: 10.1111/bjd.16711. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 5.Mitchell K., Levitt J. Alopecia areata after dupilumab for atopic dermatitis. JAAD Case Rep. 2018;4(2):143–144. doi: 10.1016/j.jdcr.2017.11.020. [DOI] [PMC free article] [PubMed] [Google Scholar]