

Sir,
Pulmonary sequestration (PS) is a rare structural lung disease, characterized by a mass of pulmonary tissue that is separated from the normal bronchopulmonary tree and supplied by one or more aberrant systemic arteries.[1] It accounts for 0.15%–6% of all congenital pulmonary malfunctions.[2] We present a case of intralobar sequestration in a 4 ½-year-old child which was diagnosed late after receiving 2 years of anti-tuberculous treatment (ATT).
A 4 ½-year-old boy presented with productive cough, occasional hemoptysis, and intermittent fever for 1 year. For these complaints, he had received first-line ATT for 6 months as chest X-ray had shown right lower zone consolidation, but had no response and thus was referred to our pediatric tuberculosis (TB) clinic for further management as a suspected case of drug-resistant-TB. His weight was 7.8 kg (<3rd centile) and height was 85 cm (<3rd centile). He had clubbing, wheezing with intercostal and subcostal retraction, and scoliosis [Figure 1]. Other systems were normal. Chest X-ray showed a persistent right lower zone inhomogeneous opacity [Figure 2]. A sputum TB-mycobacterial growth indicator tube culture was sent and he was started on second-line ATT pending the culture report which showed no growth at 6 weeks. He showed no clinical improvement after 6 months of second-line ATT and was thus suspected to have an underlying congenital malformation.
Figure 1.

A 4 ½-year-old child with scoliosis
Figure 2.

Chest X-ray: Right mid- and lower-zone in-homogeneous opacity
Lung perfusion studies showed large perfusion defect involving the right middle and lower lobes with reduced perfusion to the upper-lobe segments and normal perfusion to the left lung. Right lung function was 14% and left lung was 86%. Magnetic resonance (MR) imaging cervicodorsal spine showed scoliotic convexity to the left with minimal paravertebral soft tissue in the lower cervical region and D4 vertebra had a butterfly configuration. High-resolution computed tomography (CT)-chest and CT-pulmonary angiogram showed consolidation in the whole right lower lobe without air bronchogram, and right lower-lobe bronchus had an abrupt cutoff with multiple arterial feeders from lower descending thoracic aorta and upper abdominal aorta, with areas of artery venous shunting within the nonaerated consolidated right lower lobe suggestive of right lower-lobe intralobar sequestration [Figure 3]. ATT was stopped and the patient was referred to the surgeons for excision of the sequestered segment.
Figure 3.
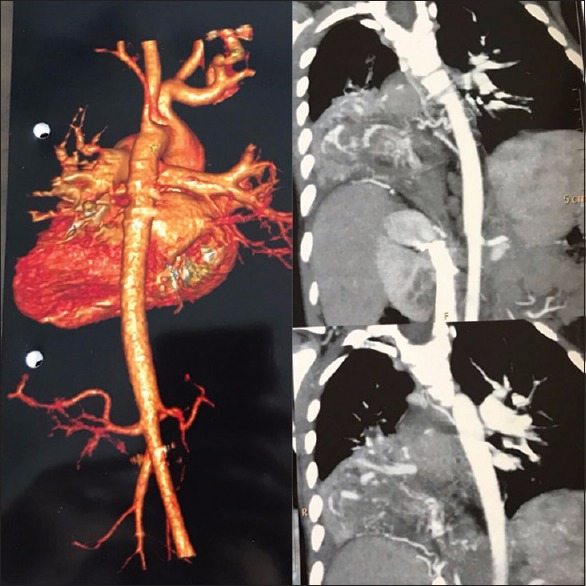
Computed tomography pulmonary angiogram – Blood supply to the sequestered segment from descending thoracic aorta
Broncho PS (BPS) is an area of nonfunctioning lung tissue that commonly receives its arterial blood supply from the descending aorta. The sequestered lobe has no communication with the tracheobronchial tree. BPS is classified as either intralobar sequestration (ILS), in which the lesion is located within a normal lobe and lacks its own visceral pleura or extralobar (ELS), in which the lesion is located outside the lung and has its own visceral pleura. ILS comprises 75%–86% and ELS comprises 14%–25% of the cases. Males are more likely to have PS than females and our patient was also a boy.[3] Both are frequently encountered in left hemithorax and lower lobe though our child had an ILS in the right lower lobe which is rare. With respect to ILS, the venous drainage is usually to the pulmonary circulation as seen in our patient too. However, ELS frequently has systemic venous drainage. Other congenital anomalies seen with BPS are congenital heart disease, diaphragmatic hernia, funnel chest, congenital pulmonary cyst, and bronchial gastric/esophageal fistula.[4] Our patient had no other congenital abnormality though he had developed scoliosis.
Patients with ELS usually show early signs of respiratory distress during childhood, while patients with ILS are more commonly diagnosed during adolescence or adulthood and show recurrent pneumonias or hemoptysis.[5] Presenting symptoms include cough, sputum production, and recurrent pulmonary infection similar to our patient. In about 15% of cases, ILS is asymptomatic when the abnormality is discovered.
Chest radiograph can provide a diagnostic clue. Recurrent localized pulmonary infection with opacity in the chest X-ray, as in our patient, is suggestive of lung sequestration. The gold standard for identifying BPS is CT/MR angiography as it confirms the anatomy, identifies the anomalous systemic arterial supply, and shows the venous drainage.
Management of the asymptomatic lung sequestration is controversial. In symptomatic patients, anomalous lung may be removed surgically or embolized with endovascular intervention. With regard to surgery, sequestrectomy or pulmonary lobectomy can be performed.[6] In children, surgery may be associated with a high risk of skeletal and muscular deformities.[7] Open thoracotomy remains the best approach with safe isolation and division of anomalous systemic feeding arteries. However, complete thoracoscopic resection has low morbidity and mortality.[8]
Congenital BPS should be suspected in any patient with localized recurrent pulmonary infection. TB can be a masquerader of this condition.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Yucel O, Gurkok S, Gozubuyuk A, Caylak H, Sapmaz E, Kavakli K, et al. Diagnosis and surgical treatment of pulmonary sequestration. Thorac Cardiovasc Surg. 2008;56:154–7. doi: 10.1055/s-2007-965572. [DOI] [PubMed] [Google Scholar]
- 2.Savic B, Birtel FJ, Tholen W, Funke HD, Knoche R. Lung sequestration: Report of seven cases and review of 540 published cases. Thorax. 1979;34:96–101. doi: 10.1136/thx.34.1.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Frazier AA, Rosado de Christenson ML, Stocker JT, Templeton PA. Intralobar sequestration: Radiologic-pathologic correlation. Radiographics. 1997;17:725–45. doi: 10.1148/radiographics.17.3.9153708. [DOI] [PubMed] [Google Scholar]
- 4.Sersar Sameh I, El Diasty M, Ibrahim Hammad R, Mounir El Saeid Awadalla M. Lower lobe segments and pulmonary sequestrations. J Thorac Cardiovasc Surg. 2004;127:898–9. doi: 10.1016/j.jtcvs.2003.12.002. [DOI] [PubMed] [Google Scholar]
- 5.Van Raemdonck D, De Boeck K, Devlieger H, Demedts M, Moerman P, Coosemans W, et al. Pulmonary sequestration: A comparison between pediatric and adult patients. Eur J Cardiothorac Surg. 2001;19:388–95. doi: 10.1016/s1010-7940(01)00603-0. [DOI] [PubMed] [Google Scholar]
- 6.Andrade CF, Ferreira HP, Fischer GB. Congenital lung malformations. J Bras Pneumol. 2011;37:259–71. doi: 10.1590/s1806-37132011000200017. [DOI] [PubMed] [Google Scholar]
- 7.Corbett HJ, Humphrey GM. Pulmonary sequestration. Paediatr Respir Rev. 2004;5:59–68. doi: 10.1016/j.prrv.2003.09.009. [DOI] [PubMed] [Google Scholar]
- 8.Albanese CT, Rothenberg SS. Experience with 144 consecutive pediatric thoracoscopic lobectomies. J Laparoendosc Adv Surg Tech A. 2007;17:339–41. doi: 10.1089/lap.2006.0184. [DOI] [PubMed] [Google Scholar]