

Abstract
Introduction:
Osteoporosis is a well-recognized complication of Cushing's syndrome (CS). Data on bone health in patients with CS from south Asian countries, which are vitamin D deficient, are scarce.
Aims:
We assessed bone mineral density (BMD) in patients with CS in comparison to controls. We also looked into how BMD differs in different types of endogenous CS.
Materials and Methods:
Thirty-seven cases of CS and 48 matched controls were studied for clinical, biochemical, hormonal, and bone densitometry parameters.
Results:
BMD (both total lumbar spine (LS) and hip) as well as Z scores were significantly lower in CS patients as compared to controls. Neither LS nor hip BMD was significantly different among different etiological groups of CS. The difference in BMD was also not significant between eumenorrhoeic and oligo-/amenorrhoeic patients with CS.
Conclusion:
Patients with CS are at increased risk of having fracture secondary to osteopenia and osteoporosis. There is no significant association of vitamin D and intact parathormone with low BMD in patients with CS.
Keywords: Bone density, Cushing's syndrome, fracture, osteopenia, osteoporosis
INTRODUCTION
Osteoporosis is a well-recognized complication of Cushing's syndrome (CS). It results from an array of systemic and local effects that glucocorticoids have on bone and mineral metabolism. The prevalence of osteoporosis due to endogenous cortisol excess has been reported to be 50–59%[1,2] and about one-third to half of patients with hypercortisolemia-induced osteoporosis experience fragility fracture.[3] Trabecular bone is more severely affected in CS than cortical bone[4] although some studies do not agree with this.[5] As compared to cortical bone, trabecular bone responds more rapidly to any changes in bone balance, either positive or negative, as bone remodeling takes place at bone surfaces and trabecular bone has greater surface-to-volume ratio.[6] Spinal trabecular bone mineral density (BMD) as measured by quantitative computed tomography was the most severely affected when studied in eugonadal female patients.[7] Most of the studies on BMD in patients with CS are from western countries where the population is vitamin D sufficient. As majority of our population is vitamin D deficient or insufficient,[8,9,10] we decided to study bone health in CS patients to evaluate the extent of the problem in this population. Our primary objective was to assess BMD in patients with CS in comparison to controls. We also looked into how BMD differs in different types of endogenous CS.
MATERIALS AND METHODS
All patients admitted and diagnosed with endogenous CS in the Department of Endocrinology and Metabolism, All India Institute of Medical Sciences, New Delhi, during July 2015 to December 2016, were included in the study. Cases and controls were recruited after obtaining approval from Institutional Ethics Committee and informed consent from participants.
Age, gender, and season-matched controls were taken. They were healthy volunteers comprising siblings of the patients included in the study as well as health-care staff. Care was taken to ask controls for previous history of metabolic bone diseases and systemic diseases such as rheumatoid arthritis, bronchial asthma, or history of intake of antiepileptic drugs that affect bone health.
It was a case control study. We recruited 37 cases (age >18 years) of endogenous hypercortisolemia and 48 healthy controls. Endogenous CS was defined if any two of the following screening tests were positive: late-night salivary cortisol, overnight dexamethasone suppression test, or the 48-h low-dose dexamethasone suppression test. We excluded patients with exogenous CS, and previous history of metabolic bone diseases and systemic diseases such as rheumatoid arthritis, bronchial asthma, or history of intake of antiepileptic drugs that affect bone health.
The patients were carefully assessed using a detailed pro forma including signs and symptoms of CS. Baseline investigations that consisted of serum calcium, phosphate, albumin, creatinine, alkaline phosphatase, 24-h urinary calcium, and 24-h urinary phosphate were measured on Hitachi 917, Roche, Germany. The intra-assay and inter-assay coefficients of variation were 3.5–5.0%. Serum thyroxine (T4), testosterone, cortisol, and dehydroepiandrosterone sulfate (DHEAS) were measured using electro-chemiluminescent immunoassay performed on a Roche, Cobas e411 autoanalyzer. Serum intact parathormone (iPTH), thyrotropin (TSH), leuteinising hormone, follicle stimulating hormone, and plasma adrenocorticotropin (ACTH) were done using electro-chemiluminescent immunometric assay performed on a Roche, Cobas e411 autoanalyzer. 25(OH) vitamin D was done using chemiluminescent immunoassay on the Diasorin LIASON autoanalyzer. X-ray chest postero-anterior view, X-ray of dorso-lumbar (D-L) spine antero-posterior (AP) and lateral view (D4-L5), and X-ray of pelvis AP view as well as BMD were measured in all the patients. X-rays were analyzed by an experienced radiologist and interpreted as presence or absence of fracture. X-rays of D-L spine were interpreted according to Genant's classification.[11]
BMD was measured by dual-energy X-ray absorptiometery (DXA) (Discovery A 84023, Hologic Inc., MA, USA) at lumbar spine (L1–L4, AP) and left hip as per the guidelines of the International Society for Clinical Densitometry (ISCD).[12] The precision was measured by testing BMD three times in 15 study subjects using ISCD precision assessment tool.[13] The coefficient of variation at lumbar spine and hip was 1.3% and 1.5% with least significant change being 0.046 and 0.038 at spine and hip, respectively. BMD of the patients was recorded in terms of absolute mineral content in g/cm2 and Z-score at both sites. The biochemical, hormonal (25(OH) vitamin D, iPTH, T4, TSH, and testosterone), and bone densitometry assessment was also done for the control group.
The data are represented as mean ± SD. The differences in the mean values of various parameters including BMD values at both sites between patients with CS and controls were compared using Student's t-test. Serum 25(OH) vitamin D, iPTH, testosterone, and DHEAS were correlated with BMD. Etiology of CS, duration of disease, and degree of hypercortisolemia were also correlated with BMD. P value less than 0.05 was considered significant.
RESULTS
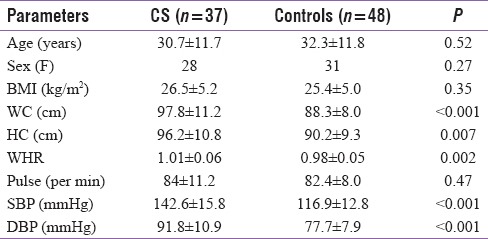
We included 37 patients with CS (28 females; 16 Cushing's disease [CD], 7 adrenal cause, 6 ectopic ACTH syndrome, and 8 unknown ACTH source) and 48 age-, sex-, and season-matched controls (31 females). We found significantly higher central obesity in CS group compared to controls. Eighty-one percent of CS subjects were hypertensive, whereas none of the controls was hypertensive. The demographic and anthropometric parameters are detailed in Table 1. Among the patients with CS, proximal muscle weakness was the most common presentation (94.6%) followed by abdominal striae (89%). Easy bruisability, moon face, and facial plethora were the other common findings (each 83.8%). Although 56.7% patients with CS complained of backache, only 8.1% gave positive history of any fracture.
Table 1.
Baseline parameters of both cases and controls
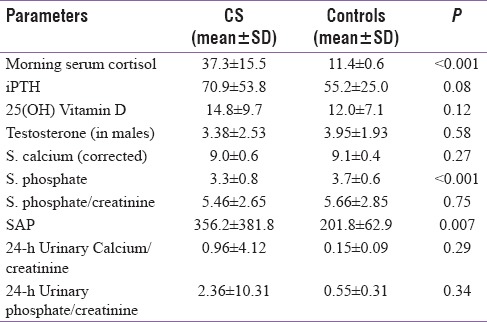
The details of hormonal and biochemical parameters are presented in Table 2. Serum phosphate was significantly lower in CS, but phosphate creatinine ratio was not statistically different. Serum alkaline phosphatase (SAP) was significantly higher in CS group. However, there was no difference between the two groups in serum levels of vitamin D, iPTH, and testosterone (in males) levels.
Table 2.
Hormonal and biochemical parameters of patients with CS and controls
BMD (both total LS and hip) as well as Z scores were significantly lower in CS patients as compared to controls [Table 3 and Figure 1]. Neither LS nor hip BMD was significantly different among different etiological groups of CS [Table 4]. The difference in BMD was also not significant between eumenorrhoeic and oligo-/amenorrhoeic patients with CS. We found negative correlation with serum morning cortisol and BMD at both LS (r2 = 0.09, P = 0.08) and hip (r2 = 0.09, P = 0.09) though this was not statistically significant [Figure 2].
Table 3.
BMD of patients with CS and controls
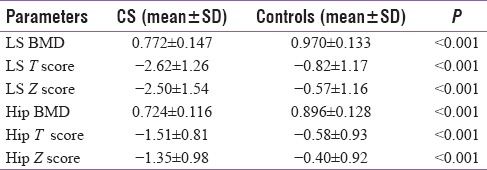
Figure 1.
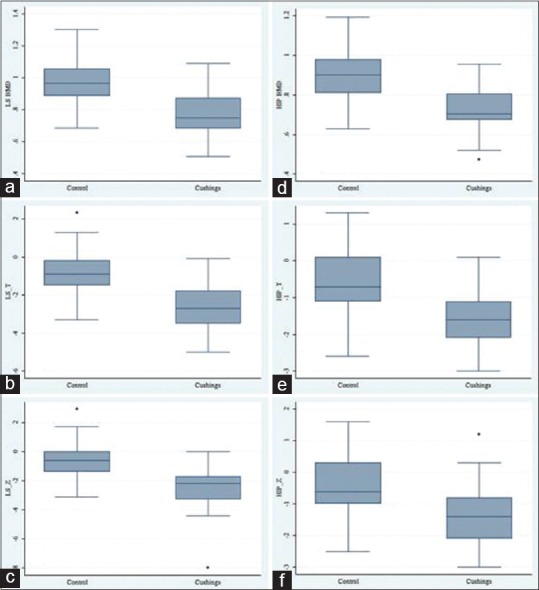
BMD: T (a,b,c) and Z (d,e,f) at LS and hip in both CS and controls
Table 4.
Distribution of hip and LS BMD according to etiology in patients with CS
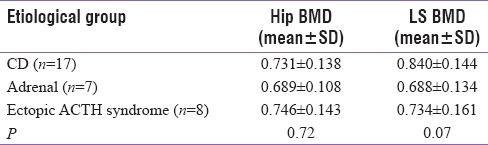
Figure 2.

Correlation of BMD and morning and evening cortisol
DISCUSSION
Our study confirms the fact that patients with CS are at very high risk of osteoporosis. We found significantly lower BMD and Z-scores at both LS and hip in patients with CS compared to controls. Bone loss was more severe in LS (Z score −2.50 ± 1.54) than hip (Z score −1.35 ± 0.98) as hypercortisolemia affects trabecular bone more than cortical bone.
BMD and Z-scores did not vary among different etiologies of CS such as pituitary adenoma, adrenal adenoma/carcinoma, or ectopic ACTH syndrome. In another study[14] too, no difference of BMD in relation to etiology of CS was found. However, few studies have shown that patients with CD maintain better BMD in comparison to patients with adrenal CS due to osteoanabolic effect of DHEAS in ACTH-dependent CS.[15,16]
In our study, the BMD parameters were not significantly different among male or female patients with CS neither did it vary significantly between eumenorrheic and hypo-/amenorrheic females. This is in concordance with other studies[14,17] which showed that neither gender nor gonadal status significantly related with BMD in CS. Duration of symptoms (r2 = 0.01, P = 0.53) and age of patients (r2 = 0.00008, P = 0.95) did not correlate with LS BMD. Similarly, they did not correlate with hip BMD. We found negative correlation with serum morning cortisol and BMD at both LS (r2 = 0.09, P = 0.08) and hip (r2 = 0.09, P = 0.09) though this was not statistically significant.
On DXA scan, 44.5% (n = 12, total 27) of patients with CS had osteoporosis and 40.7% (n = 11, total 27) had osteopenia (3 patients did not have BMD and 7 patients were below 20 years of age, so T score not compared). Thirteen (35.1%) patients had radiological evidence of vertebral fracture (wedge deformity 6, biconcave deformity 6, and crush deformity 1). The most common site of vertebral fracture was D10-L2. Eight (21.6%) patients had one or more rib fractures and five patients had bilateral avascular necrosis (AVN) of femoral head (confirmed by magnetic resonance of hip; three with stage 2 and two patients with stage 3 AVN). However, clinical history of fracture and height loss was found only in 8.1% and 16.2% of patients with CS, respectively. This finding clearly suggests that patient with CS should be evaluated for bone health as there may be silent osteopenia and osteoporosis potential to cause significant morbidity and mortality. According to another study,[3] the risk of fracture increased within the last 2 years prior to diagnosis.
There was significantly lower serum phosphate in patients with CS as compared to controls. But when serum phosphate was corrected as phosphate creatinine ratio, the difference was no longer significant. Twenty-four hour urinary calcium and phosphate excretion did not differ significantly between the two groups. However, there was elevated SAP level in CS group as compared to control group. Although we did not measure bone-specific SAP or gamma glutamyl transpeptidase, the two groups did not differ in other liver enzymes such as SGOT and SGPT. This elevated SAP may be because of fracture in CS group. Previous studies have reported significantly low serum phosphate in patients with CS and adrenal incidentaloma[18] in comparison to controls with no difference in 24 h urinary excretion of phosphate.
This could be explained as majority of our population is vitamin D deficient; our patients with CS would also have low vitamin D and consequently secondary hyperparathyroidism, which would cause further bone loss. But we did not find significant difference in serum calcium, 24 h urinary calcium excretion, serum iPTH, and 25(OH) vitamin D between CS patients and healthy controls. However, we did not take into account history of vitamin D intake in study population.
Though this is the first study from Indian subcontinent to look into the bone health parameters in patients with CS, yet the limitations are that the bone turnover markers were not done and quantitative software analysis (e.g. SpineAnalyzer) to evaluate vertebral fracture was not used. Follow-up with parameters pertaining to bone health to see recovery after remission of CS was also not done.
CONCLUSION
Patients with CS are at increased risk of having fracture secondary to osteopenia and osteoporosis. Our study has clearly shown that LS BMD in patients with CS is more affected than hip BMD and the decrease in BMD is irrespective of menstrual status, duration, and severity of hypercortisolism and etiology of CS. There is no significant association of vitamin D and iPTH with loss of BMD in patients with CS.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ross EJ, Linch DC. Cushing's syndrome-killing disease: Discriminatory value of signs and symptoms aiding early diagnosis. Lancet. 1982;2:646–9. doi: 10.1016/s0140-6736(82)92749-0. [DOI] [PubMed] [Google Scholar]
- 2.Manelli F, Giustina A. Glucocorticoid-induced osteoporosis. Trends Endocrinol Metab. 2000;11:79–85. doi: 10.1016/s1043-2760(00)00234-4. [DOI] [PubMed] [Google Scholar]
- 3.Vestergaard P, Lindholm J, Jorgensen JO, Hagen C, Hoeck HC, Laurberg P, et al. Increased risk of osteoporotic fractures in patients with Cushing's syndrome. Eur J Endocrinol. 2002;146:51–6. doi: 10.1530/eje.0.1460051. [DOI] [PubMed] [Google Scholar]
- 4.Calvo MS, Eyre DR, Gundberg CM. Molecular basis and clinical application of biological markers of bone turnover. Endocr Rev. 1996;17:333–68. doi: 10.1210/edrv-17-4-333. [DOI] [PubMed] [Google Scholar]
- 5.Cortet B, Cortet C, Blanckaert F, d’Herbomez M, Marchandise X, Wémeau JL, et al. Quantitative ultrasound of bone and markers of bone turnover in Cushings syndrome. Osteoporos Int. 2001;12:117–23. doi: 10.1007/s001980170143. [DOI] [PubMed] [Google Scholar]
- 6.Reid IR. Glucocorticoid effects on bone. J Clin Endo Metab. 1998;83:1860–1. doi: 10.1210/jcem.83.6.4911. [DOI] [PubMed] [Google Scholar]
- 7.Chiodini I, Carnevale V, Torlontano M, Fusilli S, Guglielmi G, Pileri M, et al. Alterations of bone turnover and mass at different skeletal sites due to pure glucocorticoid excess: Study in eumenorrheic patients with Cushing's syndrome. J Clin Endocrinol Metab. 1998;83:1863–7. doi: 10.1210/jcem.83.6.4880. [DOI] [PubMed] [Google Scholar]
- 8.Ritu G, Gupta A. Vitamin D deficiency in India: Prevalence, casualities and interventions. Nutrients. 2014;21:729–37. doi: 10.3390/nu6020729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shukla K, Sharma S, Gupta A, Raizada A, Vinayak K. Current scenario of prevalence of vitamin D deficiency in ostensibly healthy Indian population: A hospital based retrospective study. Indian J Clin Biochem. 2016;31:452–7. doi: 10.1007/s12291-016-0552-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shatrugna V, Kulkarni B, Kumar PA, Rani KU, Balakrishna N. Bone status of Indian women from a low-income group and its relationship to the nutritional status. Osteoporos Int. 2005;16:1827–35. doi: 10.1007/s00198-005-1933-1. [DOI] [PubMed] [Google Scholar]
- 11.Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 1993;8:1137–48. doi: 10.1002/jbmr.5650080915. [DOI] [PubMed] [Google Scholar]
- 12.ISCD Official position statement 2015. [Last accessed on 2017 May 13]. Available from: http://www.iscd.org/official-positions/2015-iscd-official-positions-adult .
- 13. [Last accessed on 2017 May 13]. Available from: http://www.iscd.org/resources/calculators .
- 14.Tauchmanova L, Pivonello R, De Martino MC, Rusciano A, De Leo M, Ruosi C, et al. Effects of sex steroids on bone in women with subclinical or overt endogenous hypercortisolism. Eur J Endocrinol. 2007;157:359–66. doi: 10.1530/EJE-07-0137. [DOI] [PubMed] [Google Scholar]
- 15.Ohmori N, Nomura K, Ohmori K, Kato Y, Itoh T, Takano K. Osteoporosis is more prevalent in adrenal than in pituitary Cushing's syndrome. Endocr J. 2003;50:1–7. doi: 10.1507/endocrj.50.1. [DOI] [PubMed] [Google Scholar]
- 16.Minetto M, Reimondo G, Osella G, Ventura M, Angeli A, Terzolo M. Bone loss is more severe in primary adrenal than in pituitary-dependent Cushing's syndrome. Osteoporos Int. 2004;15:855–61. doi: 10.1007/s00198-004-1616-3. [DOI] [PubMed] [Google Scholar]
- 17.Tauchmanovà L, Pivonello R, Di Somma C, Rossi R, De Martino MC, Camera L, et al. Bone demineralization and vertebral fractures in endogenous cortisol excess: Role of disease etiology and gonadal status. J Clin Endocrinol Metab. 2006;91:1779–84. doi: 10.1210/jc.2005-0582. [DOI] [PubMed] [Google Scholar]
- 18.Francucci CM, Pantanetti P, Garrapa GG Massi F, Arnaldi G, Mantero F. Bone metabolism and mass in women with Cushing's syndrome and adrenal incidentalomas. Clin Endocrinol. 2002;57:587–93. doi: 10.1046/j.1365-2265.2002.01602.x. [DOI] [PubMed] [Google Scholar]