

Abstract
Background:
Adenomyosis is associated with implantation failure and poor reproductive performance in IVF/ICSI cycles.
Aims:
To compare if window of implantation (WOI) is displaced in patients having adenomyosis compared to controls using endometrial receptivity array (ERA) test.
Settings and Design:
Retrospective Case control study. 374 patients with previous one or more IVF failures who underwent ERA test between 2013-2016 at our centre were enrolled. Patients were divided into two groups; Group A-36 patients with adenomyosis (study group) and Group B- 338 patients without adenomyosis (controls).
Statistical Analysis:
Normality assumptions for continuous variables were tested using Kolmogorov Smirnov test. Mean values of two groups were compared using Student's t-independent test. Frequency data by categories were compared using Chi-square/Fisher's exact test. Risk ratio and 95% confidence limits were calculated. P < 0.05 was considered for statistical significance.
Results:
WOI was displaced (Non Receptive ERA) significantly in adenomyosis 47.2% (17/36) compared to controls 21.6% (73/338) (P < 0.001, CI-8.7%-42.5%) making risk ratio of displaced WOI in adenomyosis versus controls to be 2:1. The incidence of RIF was 66.6% in adenomyosis compared to 34.9% in controls (P < 0.001, CI- 15.5%-47.9%). Pregnancy rate after personalized embryo transfer in adenomyosis group was 62.5%, signifying displaced WOI as a cause of implantation failure in adenomyosis patients with previous implantation failure.
Conclusions:
Our study suggests it is prudent to evaluate Endometrial receptivity before embryo transfer in patients with adenomyosis to avoid wastage of good embryos.
KEYWORDS: Adenomyosis, endometrial receptivity assay, in vitro fertilization/intracytoplasmic sperm injection, pregnancy
INTRODUCTION
Adenomyosis is a disorder characterized by the presence of endometrial glands and stroma within the myometrium. The glandular invasion induces local myometrial hyperplasia leading to diffused or localized enlargement of the uterus. Studies have shown an association of adenomyosis with infertility[1,2] and poor reproductive performance in assisted reproduction technology (ART).[3] An increase in implantation failure and miscarriage rates has been reported by some authors,[4,5,6,7,8,9,10] while others have not been able to confirm these results.[11,12,13] The prevalence of adenomyosis ranges from 8% to 27%,[14] being higher in older women, women with recurrent pregnancy loss and recurrent implantation failure (RIF).[15] Screening for adenomyosis before ART has been advocated to initiate patient counseling and to optimize ART protocols.[16]
Failure of implantation in adenomyosis has been attributed to altered uterine peristaltic activity,[17] impaired endometrial receptivity (ER), alterations in the embryo-endometrial cross-talk,[2] and defective decidualization.[18] ER studies have identified defects in the expression of important implantation factors such as leukemia-inhibiting factor (LIF), HOX 10, and integrins that may play a role in the implantation failure associated with adenomyosis. The role of immune system in implantation failure is widely accepted though the exact mechanisms involved are yet to be elucidated. A statistically significant increase in the density of macrophages and natural killer cells has been demonstrated in the endometrial stroma of women with adenomyosis compared to women with mild focal adenomyosis or no disease.[19]
The diagnosis of ER poses a challenge with most available tests lacking accuracy and predictive value. In recent years, microarray technology has allowed identification of the transcriptomic signature of the window of implantation (WOI) leading to the development of an ER assay (ERA) for the diagnosis of altered ER.[20] ERA is an authenticated diagnostic assay that evaluates the expression of 238 selected genes which play a critical role in the development of ER during the WOI.[21] The accuracy and consistency of this assay have been established, and results are reproducible up to 3 years after the first ERA test.[22] This test determines the duration of progesterone exposure required by the endometrium to reach a receptive status and thus aids in creating a personalized WOI for frozen embryo transfer (ET), thereby improving reproductive performance in patients with RIF.[23,24] A recent study on global transcriptomics by Herndon et al. has found an altered transcriptome of proliferative endometrium in women with adenomyosis compared to controls.[25] The aim of our study was to determine if the WOI was displaced in patients with adenomyosis who had one or more implantation failures in in vitro fertilization (IVF)-ET, using ERA.
MATERIALS AND METHODS
Study design
A retrospective case–control analysis of the data was done. A total of 374 patients with previous one or more IVF failures who underwent ERA test at our center between 2013 and 2016 were included in the study. The patients were divided into two groups; Group A – 36 patients with adenomyosis (study group) and Group B – 338 patients without adenomyosis (controls). Aims of the study were:
To compare the alterations in ER between patients having adenomyosis (Group A) and no adenomyosis (Group B) using the ERA test
To compare the incidence of RIF between patients having adenomyosis (Group A) and patients with no adenomyosis (Group B).
Inclusion criteria
Patients with one or more failed frozen ET cycles in women with normal ovarian reserve (follicle-stimulating hormone <8, antral follicle count >10, and anti-mullerian hormone >2 ng/ml) were included in the study. All transfers had been done in a hormone replacement cycle with good quality day 3 or day 5 embryos. Failed cycles done outside our unit were included only if they were done at a reputed center and embryo grading was available for scrutiny.
Exclusion criteria
Patients with uncorrected uterine and adnexal pathology, for example, hydrosalpinx, submucous polyps or myomas, history of a previous difficult ET, poor embryo quality, and endometrium <7 mm, were excluded as these factors could have contributed to implantation failure.
Ethical approval was not required as it was a retrospective analysis of data.
Diagnosis of adenomyosis
Adenomyosis was diagnosed on two-dimensional/thre-imensional ultrasound using previously defined criteria.[15,26] The diagnosis was confirmed in doubtful cases by magnetic resonance imaging. Both diffuse and focal adenomyosis groups were included in the study. Any two of the following four ultrasound criteria were used to define diffuse adenomyosis: (1) globulous aspect of the uterus, not caused by fibroids or other uterine pathology; (2) uterine asymmetry or thickening of the anterior uterine wall versus the posterior, or vice versa; (3) irregular junctional zone (JZ) or increased JZ thickness with the presence of intramyometrial cysts; and (4) myometrial striations. Adenomyoma was defined as a heterogeneous nodular mass lacking well-defined margins and without internal calcifications.
Diagnosis of displaced window of implantation
ERA analyzes the expression levels of 238 genes linked to the status of ER; using RNA sequencing taken from the endometrial tissue. Following analysis, a specific computational predictor classifies the samples according to their expression profile as receptive or nonreceptive (NR). The NR endometrium is further classified as pre- or post-receptive meaning that the endometrium has not reached the receptive phase yet or has already passed it, respectively.[23,24] Results may also suggest a narrow WOI, for example, postreceptive at P + 5 and prereceptive at P + 4 implying the implantation window remaining open for <24 h.[23,24]
Definition of recurrent implantation failure
RIF was defined as failure of implantation after two ET cycles, where the cumulative number of transferred embryos was not <4 for cleavage stage embryos and not <2 for blastocyst, with all embryos being of good quality and of appropriate developmental stage.[27]
Procedure
All patients underwent the ERA test in a hormone replacement cycle (HRT cycle). Estradiol valerate (Progynova, Sun Pharmaceutical Industries Ltd, India) was started in a dose of 2 mg, this was increased to 6 mg or more till an appropriate endometrial thickness (≥7 mm) was achieved. Vaginal progesterone (P) suppository 400 mg (Gestone, Ferring Pharmaceutical, Saint-prex, Switzerland) twice a day was then started for 5 days (P + 5). Serum progesterone level was checked, and a cutoff value of ≤0.9 ng/mL was taken to start P administration. ERA testing was canceled if serum progesterone level was ≥1 ng/mL because high endogenous progesterone levels compromise the result of the test. Endometrial biopsies (EB) were collected from the uterine cavity with the use of Pipelle catheters (Gynetics) on day P + 5 in an HRT cycle and sent to Igenomix, Valencia, Spain for analysis.
The day of the EB in HRT cycle is after 5 full days ofP impregnation, that is on the 6th day (120 h after the first progesterone intake). After the biopsy, the endometrial tissue was transferred to a cryotube containing 1.5 mL RNA stabilizing agent (Qiagen), vigorously shaken for a few seconds, and kept at 4°C in refrigerator for 4 h. Care was taken that the tissue was adequate and well immersed in the fluid provided. A repeat ERA sample with changed number of days of P administration was performed on the day recommended by the laboratory, P + 4 (for the previous postreceptive result at P + 5), P + 6, or P + 7 (for previous prereceptive results at P + 5). Personalized ET (pET) was carried out based on the timing suggested by the report. Two good quality blastocysts were transferred under ultrasound guidance.
Statistical analysis
Normality assumptions for continuous variables were tested using the Kolmogorov-Smirnov test. For approximate to normally distributed data, descriptive statistics, such as mean, standard deviation, and range values, were calculated. Qualitative variables were expressed as frequency and percent values. Mean values of two groups were compared using the Student's t-independent test. Frequency data by categories were compared using the Chi-square/Fisher's exact test. Risk ratio and 95% confidence limits were calculated. All data analyses were carried out using Statistical Product Service solutions software IBM version 21.0. A two-sided probability of P < 0.05 was considered for statistical significance.
RESULTS
Basic demographic parameters were comparable in two groups. Mean age and body mass index of patients in adenomyosis (Group A) were 34.9 years and 27.8 kg/m2, while in controls (Group B), it was 33.7 years and 25.7 kg/m2, which was not statistically significant (P = 0.157 and 0.123, respectively) [Table 1].
Table 1.
Basic demographic parameters of the two groups

In Group A (patients with adenomyosis), the WOI was displaced (NR ERA result) in 47.2% (17/36) of patients while in Group B (patients without adenomyosis) only 21.6% (73/338) of patients showed a NR ERA, which was statistically significant (P < 0.001, confidence interval [CI] - 8.7%–42.5%). Hence, the risk ratio of a displaced WOI in adenomyosis versus controls was 2:1 [Table 2].
Table 2.
Displacement of WOI (Non Receptive ERA) between the two groups

Of 17 patients with displaced WOI in adenomyosis group, eight patients had prereceptive ERA, and nine patients had postreceptive ERA.
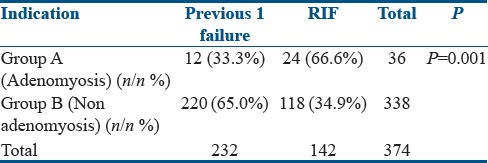
Further, a subgroup analysis was done to compare the incidence of RIF between the adenomyosis (Group A) and controls (Group B). The incidence of RIF was 66.7% (24/36) in adenomyosis (Group A) and 35% (118/338) in controls (Group B) which was statistically significant (P < 0.001, CI - 15.5%–47.9%) [Table 3].
Table 3.
Incidence of RIF in adenomyosis and controls
We also looked at the pregnancy rate (PR) in the adenomyosis group though this was not the part of the study design. Of the 36 patients in the adenomyosis group, 35 patients completed ET. The overall PR in this group was 62.9% (22/35), with a live birth rate of 28.5% (10/35) defined as number of deliveries that resulted in liveborn neonate per 100 ET cycles, early pregnancy loss (EPL) of 36.3% (8/22), and biochemical PR of 18.1% (4/22).
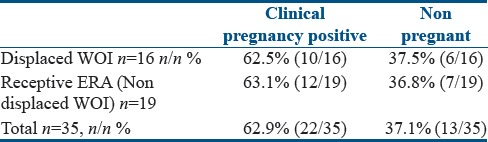
Out of 17 patients with NR ERA (displaced WOI) in this group, 16 completed pET with a PR of 62.5% (10/16) [Table 4]. However, there was a high first-trimester miscarriage rate of 40% (4/10), and 20% (2/10) of patients had a biochemical pregnancy in the pET group.
Table 4.
Pregnancy outcome in patients with adenomyosis (Group A) after pET
The overall PR in the control group of patients who completed ET (216/338) was 63.9% with a live birth rate of 45.8% defined as a number of deliveries that resulted in liveborn neonate per 100 ET cycles, an EPL of 16% with a biochemical PR of 12.7%. The PR for patients with altered WOI in the control group of patients who completed pET (50/73) was 68.5%.
DISCUSSION
Adenomyosis an estrogen-responsive disorder is associated with infertility and implantation failure in IVF. Conflicting reports regarding reproductive outcome in patients with adenomyosis using ART have intensified the search for molecular or clinical markers of ER. Impaired ER[2] and decidualization[18] are considered important causative factors. Oocyte donor-recipient cycles have often been used as an ideal model to differentiate between an endometrial or embryonic factor for a negative outcome in IVF. Using this model, Martínez-Conejero et al., reported a decreased live birth rate and a doubling of miscarriage rate in recipients with adenomyosis, suggesting thereby that the initial stages of embryo invasion and placentation may be disrupted.[6] Sudoma demonstrated retardation in pinopode formation in >45% of patients with adenomyosis in his study.[28] Studies at a molecular and genetic level have identified defects in expression of integrin β3, osteopontin, LIF, an impairment of HOXA-10 gene function, and induction of inflammatory factors within the endometrium during the WOI.[29] Zhihong et al. demonstrated that macrophages, interleukin (IL)-6, IL-10, and monocyte chemoattractant protein-1 were expressed differently in the endometrium of women with adenomyosis within the WOI during ovarian stimulation. They postulated that cytokines of endometrial secretions are expressed differently in patients with adenomyosis and may contribute to impaired endometrium receptivity in these patients.[30] The role of oxidative stress in infertility and miscarriage is elucidated by a persistent overexpression of superoxide dismutase in patients with endometriosis and adenomyosis.[31]
An overexpression of aromatase P450 has also been found in the endometrium of women with adenomyosis and has been implicated in implantation failure.[32] Pretreatment with GnRH agonist, which reduces the hyperestrogenic milieu, is known to improve PR's.[33] Transcriptomic analysis of endometrium in a mouse adenomyosis model revealed that the expression of estrogen-linked genes, such as Tff1 and Sprr2a1, was significantly decreased in mice treated with a GnRH agonist.[34]
Global transcriptomics studies of isolated human eutopic endometrium found that the transcriptomes of proliferative endometrium revealed 140 upregulated and 884 downregulated genes in samples from women with adenomyosis compared to controls. Genes that were highly differentially expressed included those involved in regulation of apoptosis, steroid hormone responsiveness, and proteins involved in extracellular matrix remodeling.[25]
We undertook this study to see if WOI is displaced in patients with adenomyosis with previous one or more IVF failures compared to patients with no adenomyosis using the ERA test. Our results suggest that the WOI is displaced significantly in patients with adenomyosis (47.2%) compared to the no adenomyosis (control) group (21.6%) (P < 0.001). Our results suggested that the risk of finding a NR ERA, i.e., a displaced WOI among adenomyosis patients was two times higher (47.2%) than controls (21.6%); risk ratio of 2:1. This could explain in part the lowered pregnancy and implantation rates reported in adenomyosis.
The subgroup analysis of patients in our study revealed that the incidence of RIF in adenomyosis group (66.7%; 24/36) was significantly higher than controls (34.9.0%; 118/338); (P < 0.001, CI - 15.5%–47.9%). Among the RIF adenomyosis group, ERA was found NR (displaced WOI) in 66.7% (16/24), suggesting that an altered ER in adenomyosis is involved in the recurrent failure of implantation.
Out of 36 patients with adenomyosis (Group A), 35 underwent ET. The overall PR in adenomyosis group was 62.9% (22/35), with a live birth rate of 28.5% (10/35), EPL of 36.3% (8/22), and biochemical PR of 18.2% (4/22). Martínez-Conejero et al. also reported a lower live birth rate and high miscarriage rate in adenomyosis patients which they hypothesized could be a result of unknown molecular mechanisms related to trophoblastic invasion or the establishment of pregnancy.[6]
Out of 36 patients with adenomyosis (Group A), 17 patients had displaced WOI. Of 17 patients with displaced WOI (NR ERA), 16 patients underwent pET, resulting in PR of 62.5% (10/16), which is higher than reported by earlier studies and meta-analysis by Vercellini et al., in 2014 who reported clinical PR after IVF/intracytoplasmic sperm injection to be 40.5% in women with adenomyosis versus 49.8% in those without adenomyosis,[16] thus signifying the improvement of clinical PR after pET in adenomyosis. Miscarriage rate in our study in this group was 40% (4/10), this higher miscarriage rate could be due to small numbers in the study.
Our study highlights the importance of displaced WOI as a cause of implantation failure in patients with adenomyosis who have experienced one or more IVF failures. Considering the high risk (2:1) of displaced WOI in adenomyosis, it might be prudent to evaluate ER by an ERA test before proceeding to ET to avoid wastage of good embryos.
CONCLUSION
Patients with adenomyosis having one or more implantation failures in IVF exhibit a displaced WOI as determined using the ERA test, with a risk ratio of 2:1 compared to controls. pET should be performed in such patients after correcting the WOI to improve reproductive outcome in IVF.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kunz G, Beil D, Huppert P, Noe M, Kissler S, Leyendecker G, et al. Adenomyosis in endometriosis – Prevalence and impact on fertility. Evidence from magnetic resonance imaging. Hum Reprod. 2005;20:2309–16. doi: 10.1093/humrep/dei021. [DOI] [PubMed] [Google Scholar]
- 2.Campo S, Campo V, Benagiano G. Infertility and adenomyosis. Obstet Gynecol Int. 2012;2012:786132. doi: 10.1155/2012/786132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tomassetti C, Meuleman C, Timmerman D, D'Hooghe T. Adenomyosis and subfertility: Evidence of association and causation. Semin Reprod Med. 2013;31:101–8. doi: 10.1055/s-0032-1333475. [DOI] [PubMed] [Google Scholar]
- 4.Ballester M, d'Argent EM, Morcel K, Belaisch-Allart J, Nisolle M, Daraï E, et al. Cumulative pregnancy rate after ICSI-IVF in patients with colorectal endometriosis: Results of a multicentre study. Hum Reprod. 2012;27:1043–9. doi: 10.1093/humrep/des012. [DOI] [PubMed] [Google Scholar]
- 5.Maubon A, Faury A, Kapella M, Pouquet M, Piver P. Uterine junctional zone at magnetic resonance imaging: A predictor of in vitro fertilization implantation failure. J Obstet Gynaecol Res. 2010;36:611–8. doi: 10.1111/j.1447-0756.2010.01189.x. [DOI] [PubMed] [Google Scholar]
- 6.Martínez-Conejero JA, Morgan M, Montesinos M, Fortuño S, Meseguer M, Simón C, et al. Adenomyosis does not affect implantation, but is associated with miscarriage in patients undergoing oocyte donation. Fertil Steril. 2011;96:943–50. doi: 10.1016/j.fertnstert.2011.07.1088. [DOI] [PubMed] [Google Scholar]
- 7.Salim R, Riris S, Saab W, Abramov B, Khadum I, Serhal P, et al. Adenomyosis reduces pregnancy rates in infertile women undergoing IVF. Reprod Biomed Online. 2012;25:273–7. doi: 10.1016/j.rbmo.2012.05.003. [DOI] [PubMed] [Google Scholar]
- 8.Thalluri V, Tremellen KP. Ultrasound diagnosed adenomyosis has a negative impact on successful implantation following GnRH antagonist IVF treatment. Hum Reprod. 2012;27:3487–92. doi: 10.1093/humrep/des305. [DOI] [PubMed] [Google Scholar]
- 9.Tao T, Chen S, Chen X, Ye D, Xu L, Tian X, et al. Effects of uterine adenomyosis on clinical outcomes of infertility patients treated with in vitro fertilization/intracytoplasmic sperm injection-embryo transfer (IVF/ICSI-ET) Nan Fang Yi Ke Da Xue Xue Bao. 2015;35:248–51. [PubMed] [Google Scholar]
- 10.Youm HS, Choi YS, Han HD. In vitro fertilization and embryo transfer outcomes in relation to myometrial thickness. J Assist Reprod Genet. 2011;28:1135–40. doi: 10.1007/s10815-011-9640-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Benaglia L, Cardellicchio L, Leonardi M, Faulisi S, Vercellini P, Paffoni A, et al. Asymptomatic adenomyosis and embryo implantation in IVF cycles. Reprod Biomed Online. 2014;29:606–11. doi: 10.1016/j.rbmo.2014.07.021. [DOI] [PubMed] [Google Scholar]
- 12.Costello MF, Lindsay K, McNally G. The effect of adenomyosis on in vitro fertilisation and intra-cytoplasmic sperm injection treatment outcome. Eur J Obstet Gynecol Reprod Biol. 2011;158:229–34. doi: 10.1016/j.ejogrb.2011.04.030. [DOI] [PubMed] [Google Scholar]
- 13.Mijatovic V, Florijn E, Halim N, Schats R, Hompes P. Adenomyosis has no adverse effects on IVF/ICSI outcomes in women with endometriosis treated with long-term pituitary down-regulation before IVF/ICSI. Eur J Obstet Gynecol Reprod Biol. 2010;151:62–5. doi: 10.1016/j.ejogrb.2010.02.047. [DOI] [PubMed] [Google Scholar]
- 14.Maheshwari A, Gurunath S, Fatima F, Bhattacharya S. Adenomyosis and subfertility: A systematic review of prevalence, diagnosis, treatment and fertility outcomes. Hum Reprod Update. 2012;18:374–92. doi: 10.1093/humupd/dms006. [DOI] [PubMed] [Google Scholar]
- 15.Puente JM, Fabris A, Patel J, Patel A, Cerrillo M, Requena A, et al. Adenomyosis in infertile women: Prevalence and the role of 3D ultrasound as a marker of severity of the disease. Reprod Biol Endocrinol. 2016;14:60. doi: 10.1186/s12958-016-0185-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Vercellini P, Consonni D, Dridi D, Bracco B, Frattaruolo MP, Somigliana E, et al. Uterine adenomyosis and in vitro fertilization outcome: A systematic review and meta-analysis. Hum Reprod. 2014;29:964–77. doi: 10.1093/humrep/deu041. [DOI] [PubMed] [Google Scholar]
- 17.Kissler S, Hamscho N, Zangos S, Wiegratz I, Schlichter S, Menzel C, et al. Uterotubal transport disorder in adenomyosis and endometriosis – A cause for infertility. BJOG. 2006;113:902–8. doi: 10.1111/j.1471-0528.2006.00970.x. [DOI] [PubMed] [Google Scholar]
- 18.Jiang Y, Jiang R, Cheng X, Zhang Q, Hu Y, Zhang H, et al. Decreased expression of NR4A nuclear receptors in adenomyosis impairs endometrial decidualization. Mol Hum Reprod. 2016;22:655–68. doi: 10.1093/molehr/gaw042. [DOI] [PubMed] [Google Scholar]
- 19.Tremellen KP, Russell P. The distribution of immune cells and macrophages in the endometrium of women with recurrent reproductive failure. II: Adenomyosis and macrophages. J Reprod Immunol. 2012;93:58–63. doi: 10.1016/j.jri.2011.12.001. [DOI] [PubMed] [Google Scholar]
- 20.Talbi S, Hamilton AE, Vo KC, Tulac S, Overgaard MT, Dosiou C, et al. Molecular phenotyping of human endometrium distinguishes menstrual cycle phases and underlying biological processes in normo-ovulatory women. Endocrinology. 2006;147:1097–121. doi: 10.1210/en.2005-1076. [DOI] [PubMed] [Google Scholar]
- 21.Díaz-Gimeno P, Horcajadas JA, Martínez-Conejero JA, Esteban FJ, Alamá P, Pellicer A, et al. Agenomic diagnostic tool for human endometrial receptivity based on the transcriptomic signature. Fertil Steril. 2011;95:50–60. 60.e1–15. doi: 10.1016/j.fertnstert.2010.04.063. [DOI] [PubMed] [Google Scholar]
- 22.Díaz-Gimeno P, Ruiz-Alonso M, Blesa D, Bosch N, Martínez-Conejero JA, Alamá P, et al. The accuracy and reproducibility of the endometrial receptivity array is superior to histology as a diagnostic method for endometrial receptivity. Fertil Steril. 2013;99:508–17. doi: 10.1016/j.fertnstert.2012.09.046. [DOI] [PubMed] [Google Scholar]
- 23.Ruiz-Alonso M, Blesa D, Díaz-Gimeno P, Gómez E, Fernández-Sánchez M, Carranza F, et al. The endometrial receptivity array for diagnosis and personalized embryo transfer as a treatment for patients with repeated implantation failure. Fertil Steril. 2013;100:818–24. doi: 10.1016/j.fertnstert.2013.05.004. [DOI] [PubMed] [Google Scholar]
- 24.Mahajan N. Endometrial receptivity array: Clinical application. J Hum Reprod Sci. 2015;8:121–9. doi: 10.4103/0974-1208.165153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Herndon CN, Aghajanova L, Balayan S, Erikson D, Barragan F, Goldfien G, et al. Global transcriptome abnormalities of the eutopic endometrium from women with adenomyosis. Reprod Sci. 2016;23:1289–303. doi: 10.1177/1933719116650758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Devlieger R, D'Hooghe T, Timmerman D. Uterine adenomyosis in the infertility clinic. Hum Reprod Update. 2003;9:139–47. doi: 10.1093/humupd/dmg010. [DOI] [PubMed] [Google Scholar]
- 27.Polanski LT, Baumgarten MN, Quenby S, Brosens J, Campbell BK, Raine-Fenning NJ, et al. What exactly do we mean by 'recurrent implantation failure'.A systematic review and opinion? Reprod Biomed Online. 2014;28:409–23. doi: 10.1016/j.rbmo.2013.12.006. [DOI] [PubMed] [Google Scholar]
- 28.Sudoma I. The evaluation of pinopode formation in patients with adenomyosis. Fertil Steril. 2002;77:S27. [Google Scholar]
- 29.Yang JH, Wu MY, Chang DY, Chang CH, Yang YS, Ho HN, et al. Increased interleukin-6 messenger RNA expression in macrophage-cocultured endometrial stromal cells in adenomyosis. Am J Reprod Immunol. 2006;55:181–7. doi: 10.1111/j.1600-0897.2005.00363.x. [DOI] [PubMed] [Google Scholar]
- 30.Zhihong N, Yun F, Pinggui Z, Sulian Z, Zhang A. Cytokine profiling in the eutopic endometrium of adenomyosis during the implantation window after ovarian stimulation. Reprod Sci. 2016;23:124–33. doi: 10.1177/1933719115597761. [DOI] [PubMed] [Google Scholar]
- 31.Ota H, Igarashi S, Hatazawa J, Tanaka T. Immunohistochemical assessment of superoxide dismutase expression in the endometrium in endometriosis and adenomyosis. Fertil Steril. 1999;72:129–34. doi: 10.1016/s0015-0282(99)00152-1. [DOI] [PubMed] [Google Scholar]
- 32.Harada T, Khine YM, Kaponis A, Nikellis T, Decavalas G, Taniguchi F, et al. The impact of adenomyosis on women's fertility. Obstet Gynecol Surv. 2016;71:557–68. doi: 10.1097/OGX.0000000000000346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Park CW, Choi MH, Yang KM, Song IO. Pregnancy rate in women with adenomyosis undergoing fresh or frozen embryo transfer cycles following gonadotropin-releasing hormone agonist treatment. Clin Exp Reprod Med. 2016;43:169–73. doi: 10.5653/cerm.2016.43.3.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Guo S, Lu X, Gu R, Zhang D, Sun Y, Feng Y, et al. Transcriptome analysis of endometrial tissues following GnRH agonist treatment in a mouse adenomyosis model. Drug Des Devel Ther. 2017;11:695–704. doi: 10.2147/DDDT.S127889. [DOI] [PMC free article] [PubMed] [Google Scholar]