

Abstract
To evaluate the association between gene polymorphisms of TNF-α G308A, IL-6 C174G, and coronary atherosclerotic heart disease (CHD) risk.
We used computers to collect related case-control studies. After screening, a meta-analysis was conducted to assess the strength of association by Stata 12.0 software.
Thirty-five articles were included. Among them, 17 studies were related to TNF-α (G308A) gene mutation and CHD, and 18 studies examined IL-6 (C174G) gene mutation. According to the results of subgroup analysis of ethnicity, it suggested that TNF-α (G308A) polymorphism was not significantly associated with CHD risk under all models in Asians (P > .05). There were no connected of IL-6 C174G polymorphism with CHD risk under all models in Caucasians after subgroup analysis (P > .05).
The present evidence shows that TNF-α (G308A) have no connected with the risk of CHD in Asians; IL-6 (C174G) gene were not associated with the risk of CHD in Caucasians.
Keywords: coronary atherosclerotic heart disease, interleukin-6, meta-analysis, polymorphism, tumor necrosis factor-alpha
1. Introduction
Coronary atherosclerotic heart disease (CHD) characterizes as myocardial ischemia and hypoxia which arises from coronary atherosclerosis.[1] It is a worldwide medical problem and is still one of the leading causes of death in developed and developing countries.[2] At present, the occurrence and development of CHD is generally considered as a chronic inflammatory process characterized by highly specific cytokine response.[3] The regulation network formed by various proinflammatory and anti-inflammatory factors plays an immunomodulatory role in atherosclerosis.[4] Various proteins, cytokines, and adhesion molecules are involved in the development of coronary angiogenesis.[5] Among them, TNF-α and IL-6 have significant effects on the development of coronary heart disease.[6,7] It has been showed that both of them are capable to damage endothelium function and act on the plaque of the vessel wall, accelerating the rupture of the plaque and triggering the clinical coronary events.[8] As a complex disease, CHD results from the interaction between genetic and environmental factors.[9] Recent studies have suggested that the basic level and biological activity of TNF-α and IL-6 can be influenced by gene polymorphism, which may increase the risk of CHD[10,11] C863A of TNF-α and C174G of IL-6 are the mostly investigated but the results remain inconsistent. Asifa et al[12] considered that the TNF-α C863A gene polymorphism was associated with the pathogenesis of CHD through case-control study in Pakistan, while Chu et al[13] research in China drew an opposite conclusion. The studies on IL-6 gene polymorphism and risk of CHD are also inconsistent, similar to that research status of TNF-α.[14,15] This may be due to racial and regional differences, as well as the fact that the sample size is too small to truly reflect the relevance. In order to compare different research results more scientifically and objectively, meta-analysis on this issue coming to be widely carried out also generated conflicting results. Based on it, we carry out a meta-analysis including the genotype data from all eligible investigations in the latest years involving more extensive countries and regions to provide a more precise evaluation of the association between polymorphisms in –308G/A of TNF-α, C174G of IL-6 and CHD susceptibility.
2. Materials and methods
2.1. Search strategy
Our study followed the meta-analysis of Observational Studies in Epidemiology guidelines and the researches were investigated in the following databases since the establishment of the library to April 2018: the China National Knowledge Infrastructure (CNKI), China Wanfang Database, Chinese biomedical literature database and PubMed, EMBASE, Cochrane library, Web of Science, Sciencedirect. The following search words were combined: “G308A” or “TNF-α” or “C174G”or “IL-6” or “coronary atherosclerotic heart disease.” In addition, we searched the references in detail for further research. Furthermore all magazines were retrieved from the first issue, and the relevant conference literature was tracked. If necessary, contact the communication author to obtain information not found by the above retrieval strategies.
2.2. Inclusion and exclusion criteria
Studies that meet the following criteria will be adopted: the literature must be a case-control study published both at home and abroad, with good balance and comparability. Languages are limited to Chinese or English. The research should involve gene polymorphisms of TNF-α (G308A), IL-6 (C174G), and CHD. The research should meet the diagnostic criteria of coronary heart disease. Each genotype distribution and individual number in the case and control groups should be listed in the literature, or the corresponding number can be calculated by the frequency of each genotype given.
Studies with the following characteristics will be excluded: not associated with TNF-α (G308A), IL-6 (C174G) polymorphism, and CHD; not a case–control study; the data of genotype frequency and allele frequency in the literature are incomplete or unclear.
2.3. Data extraction and quality evaluation
The 2 researchers (Jiang and Zhao) sifted through the title and summary of the studies. Then they read the full text for the secondary screening and eliminated the studies that did not meet the above-mentioned inclusion criteria. For trials that were difficult to determine whether they should be included, consult an expert to discuss the solution. If the information provided in this article was uncertain, contact the original author by phone, email, and other measures to obtain relevant information. We used the 9-star Newcastle-Ottawa scale to evaluate the quality of the studies. It includes 3 aspects: study object selection, group comparability, and exposure factor measurement. In brief, a maximum of 9 points was assigned to each study: 4 for selection, 2 for comparability, and 3 for outcomes. A final score of >6 was regarded as high quality. Then we organized each article included and extracted relevant data: the first author's name, years of publication, country and region, genotype frequencies in the observation group and control group. Hardy–Weinberg equilibrium and quality score of case-control study were showed in Fig. 1.
Figure 1.
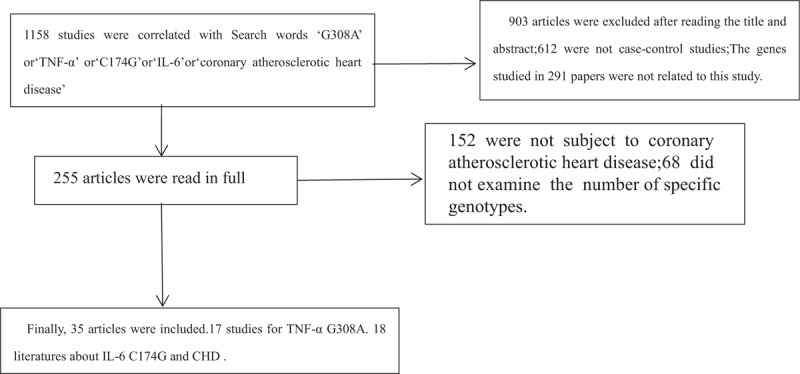
Article screening flowchart.
3. Statistical analysis
All the data were analyzed using Stata 12.0 software and the charts related were drawn below. Based on the odds ratio (OR) with a corresponding 95% confidence interval (CI), we counted the pooled odds which were used to analyze the effect on the association. While crossing these studies, Q test and I2 were used to test the heterogeneity of the included literature firstly. When I2 >50%, it was proved that there was heterogeneity between the studies, the random effect model was used, and if not, the fixed effect model was used instead. In order to Search for the sources of heterogeneity, we mainly apply subgroup analysis on the national and regional groups. In order to evaluate the stability of the combined results, a sensitivity analysis was conducted for the meta-analysis results after each removal of a case-control study. The Begg funnel plot was used as a criterion for assessing publication bias.
4. Results
4.1. Characteristics of the included studies
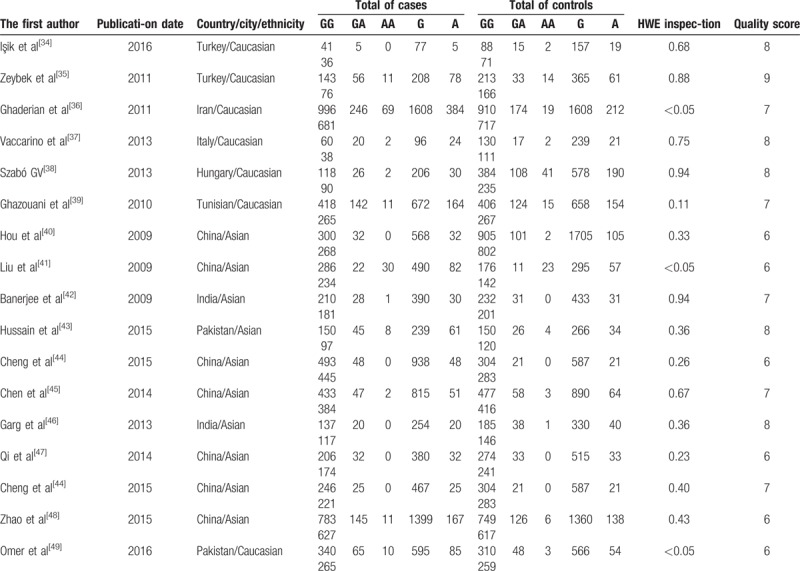
Overall, a total of 35 out of 1158 articles were selected for the final meta-analysis.[16–49] Among the 35 articles, 18 studies[16–33] reported the association between IL-6 (C174G) gene mutation and CHD with 5328 cases and 5077 controls. Seventeen articles[34–49] demonstrated the relationship between TNF-α (G308A) and CHD with 5360 cases and 6197 controls. The baseline characteristics of the studies related to mutation of IL-6 (C174G) and TNF-α (G308A) were respectively shown in Tables 1 and 2. All of the 35 articles were published before January 2018. In addition, 29 manuscripts were published in English, and 6 manuscripts were in Chinese.
Table 1.
Characteristics of studies on the association between C174G gene polymorphisms of IL-6 and CHD risk.
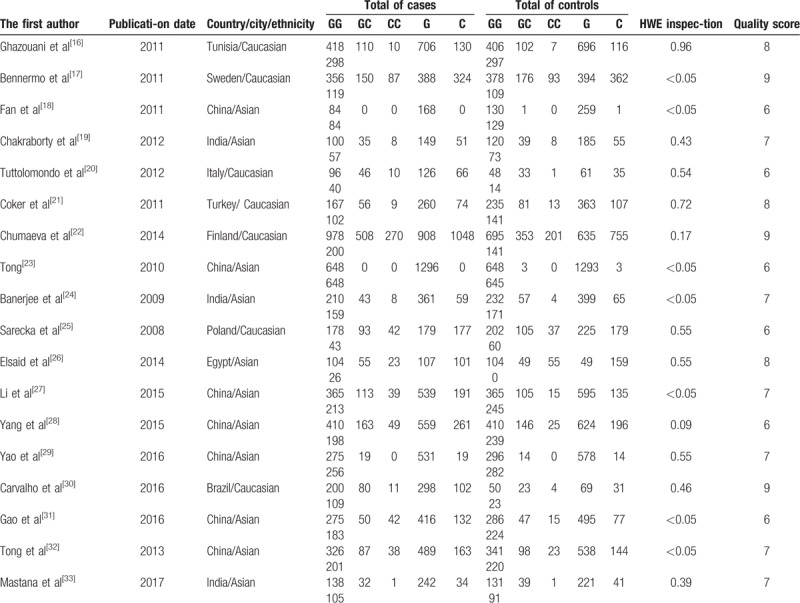
Table 2.
Characteristics of studies on the association between G308A gene polymorphisms of TNF-α and CHD risk.
4.2. Results of the overall meta-analysis
4.2.1. Meta-analysis of TNF-αG308A polymorphism and CHD risk
Seventeen articles were related to G308A mutation and CHD risk. The results showed that I2 of all models were >50%, indicating that the included studies had heterogeneity. Subgroup analysis was needed to explore the source of heterogeneity.
4.3. Subgroup analysis
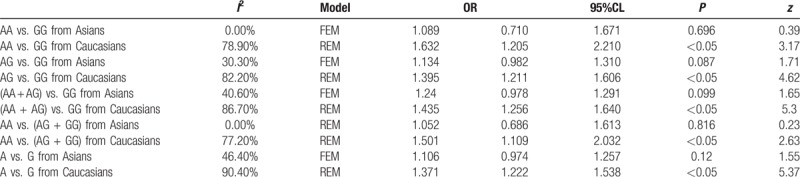
Of the 17 articles included, 10 articles were from Asians, 7 articles were from Caucasians. The results were shown in Table 4. And we conducted subgroup according to different ethnic groups. The I2 of all models in Asians were <50%, indicating that ethnic differences had an impact on heterogeneity. The results suggested that there was no significantly association between G308A polymorphism and CHD risk under all models from Asians (P > .05) (Table 3).
Table 4.
Results of IL-6 C174G polymorphism and CHD risk.

Table 3.
Meta-analysis of TNF-αG308A polymorphism and CHD risk.
4.4. Meta-analysis of IL-6 C174G polymorphism and CHD risk
Thirteen articles were related to IL-6 C174G polymorphism and CHD emotivity. The results showed that the polymorphism of C174G gene was not significantly associated with CHD risk under heterozygote model (CG vs GG; OR 0.998, 95% CI 0.902–1.103) (P > .05). The results were shown in Table 4, Fig. 2. Furthermore, sensitivity analysis revealed that omission of each study made no significant differences on the findings Fig. 3.
Figure 2.
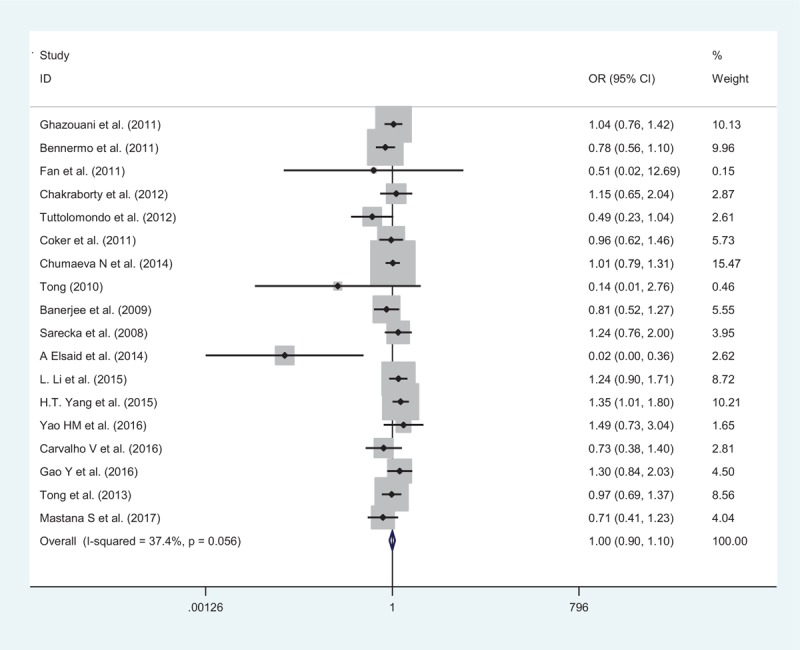
Forest plot of IL-6 C174G polymorphism and CHD risk. CHD = coronary atherosclerotic heart disease, IL-6 = interleukin-6.
Figure 3.
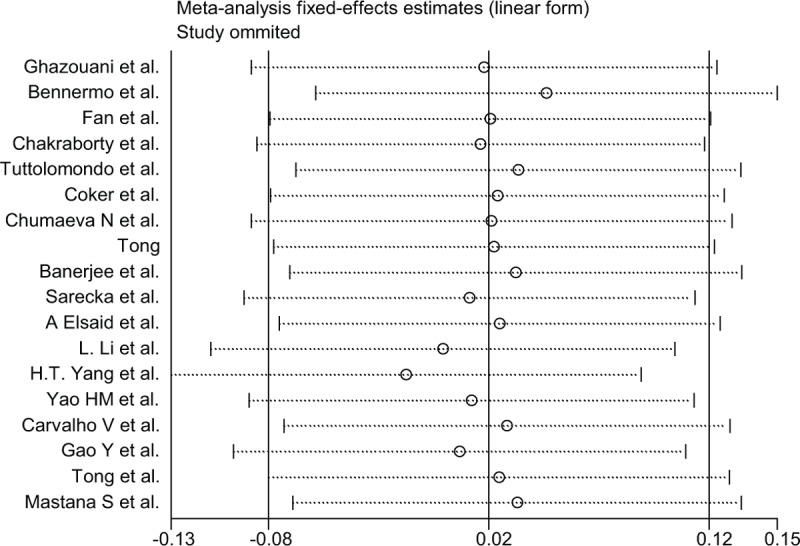
Sensitivity analyses for IL-6 C174G CG versus GG polymorphism and CHD. CHD = coronary atherosclerotic heart disease, IL-6 = interleukin-6.
4.5. Test for heterogeneity
In the heterogeneity test for the IL-6 C174G genotypes of each model, I2 of C versus G, CC versus CG+GG, CC versus GG, CC+CG versus GG were >50%, indicating that the included studies had heterogeneity. Subgroup analysis was needed to explore the source of heterogeneity.
4.6. Subgroup analysis
Of the 18 articles included, 11 studies were from Asians and 7 were from Caucasians. We conducted subgroup analysis on CC versus GG, CC+CG versus GG, CC versus CG+GG, C versus G genotype, and CHD risk according to the ethnicity. The I2 of (CC vs GG, CC+CG vs GG, CC vs CG+GG, C vs G) in Caucasians were <50%, indicating that ethnic differences had an impact on heterogeneity. And there was no significantly association between CHD risk and IL-6 C174G polymorphism under CC versus GG, CC+CG versus GG, CC versus CG+GG, C versus G in Caucasians (P > .05). The results were shown in Table 5.
Table 5.
results of IL-6 C174G mutation and CHD risk in subgroup analysis.

4.7. Publication bias
We analyzed the publication bias of articles on the relationship between TNF-α (G308A) and IL-6 (C174G) with CHD risk. The 2 groups of gene funnel plot analysis showed asymmetry indicating the possibility of publication bias. The results were shown in Figures 4 and 5.
Figure 4.
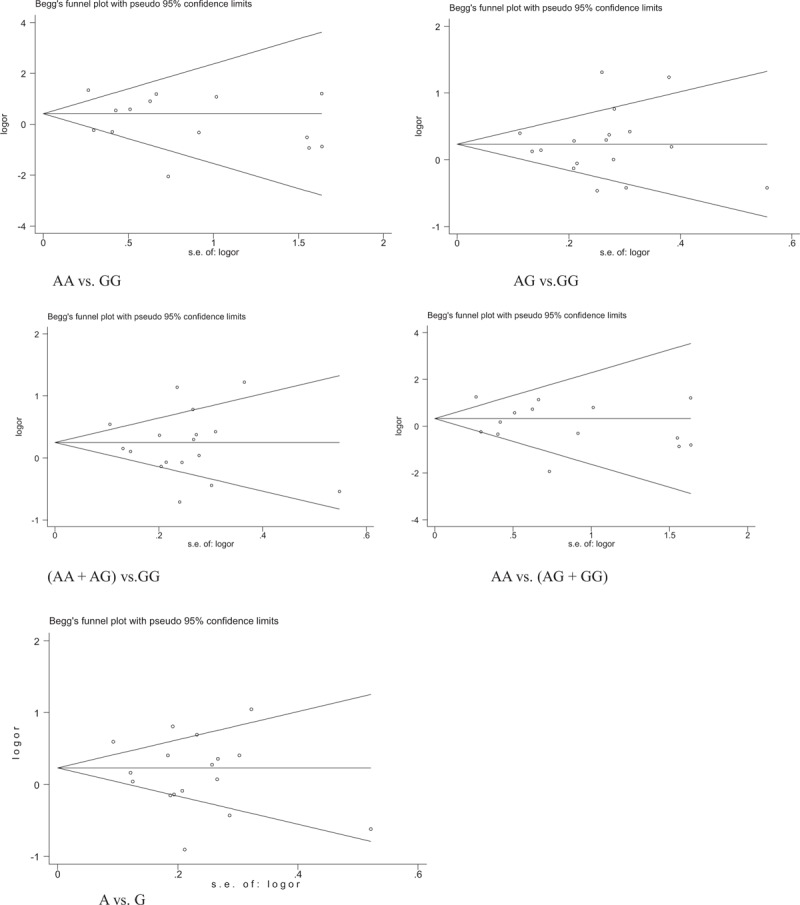
The publication bias of articles on the relationship between TNF-α G308A and CHD risk was shown in the funnel figure. CHD = coronary atherosclerotic heart disease, TNF-α = tumor necrosis factor-alpha.
Figure 5.
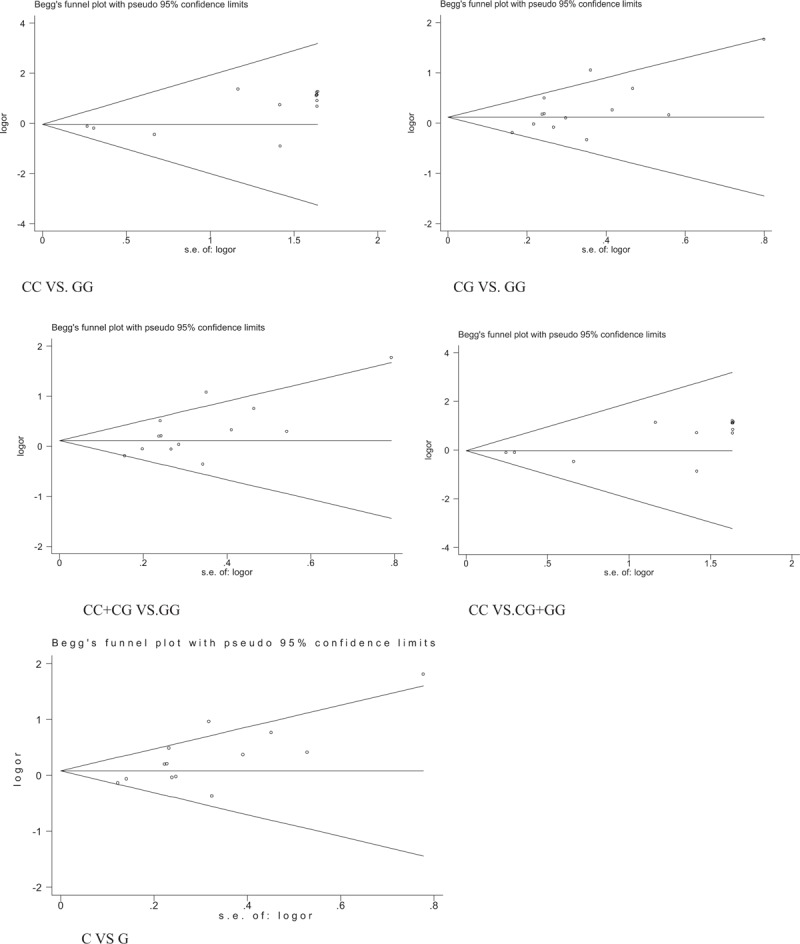
The publication bias of articles on the relationship between IL-6 C174G and CHD risk was shown in the funnel figure. CHD = coronary atherosclerotic heart disease, IL-6 = interleukin-6.
5. Discussion
Recently the polymorphisms of TNF-α, IL-6 have aroused great concern among researchers. It has been found that both TNF-α and IL-6 genes have gene polymorphism, which may affect the transcription and expression of genes, and are closely related to the significant increase of CHD risk.[50]
TNF-α is an inflammatory cytokine secreted by macrophages and has multiple biological activities. As a starting factor for endothelial dysfunction and endometrial thickening, it can directly damage the vascular endothelial cells and then increase permeability to make more cholesterol deposited in the vascular wall, forming atherosclerotic plaques.[51] Besides it is also capable of promoting the formation of platelet-derived growth factor, breaking blood coagulation–anticoagulant balance, and contributing to thrombosis.[52] Moreover TNF-α reduces lipoprotein activity, participates in insulin resistance, and affects the synthesis of other inflammatory factors.[53] The concentration of TNF-α in plasma can be influenced by gene polymorphism. Among several common mutation sites, the G-308A was the most studied, which is a single nucleotide conversion from guanine (G) to adenine (A) in the TNF-α promoter at position –308.[54] In our conclusions TNF-α (G308A) polymorphism was not significantly associated with CHD risk under all models in Asians (P > .05), which is consistent with the results of Wang et al[55] research. To further identify this association, more high quality studies should be merited.
IL-6 is another important cytokine in the proinflammatory response mainly produced by monocytes and macrophages.[56] In the acute stage of inflammation, IL-6 can induce the production of acute inflammatory reactants such as c-reactive protein and fibrinogen, and interact with cytokine network, involved in the pathogenesis of CHD.[57] A study shows that its mRNA levels in atherosclerotic arteries are 40 to 50 times higher than that in nonatherosclerotic vessels.[58] The plasma level of IL-6 are partly adjusted by the IL-6 C174G polymorphism[59] which is located in the upstream promoter region of IL-6 gene. C174G mutation site transforms from a guanine (G) to cytosine (C) at position –174. A 6-year follow-up study in the UK showed that people with genotype of G/C or C/C were more likely to develop CHD when compared with people carrying G/G genotype (OR = 1.54).[60] In our research, there were no connection between IL-6 C174G polymorphism and CHD risk under all models in Caucasians.
Our meta-analysis also has its own drawbacks. For instance the inspections of the funnel plots suggest that they are not symmetrical. This may be due to the fact that sample sizes of many studies included in our meta-analysis were relatively small, and the number of eligible studies included is also not enough. This requires more relevant case-control studies in the future to make the meta-results more objective and scientific.
Acknowledgments
The authors thank all patients for their participation. Special thanks are also extended to colleagues at the First Affiliated Hospital of Heilongjiang University Of Chinese Medicine.
Author contributions
Conceptualization: Yuepeng Jiang, Xiaoxuan Zhao.
Data curation: Yuepeng Jiang, Xiaoxuan Zhao.
Formal analysis: Yang Zhao.
Funding acquisition: Xiaoxuan Zhao, Li Liu.
Investigation: Yuepeng Jiang, Li Liu.
Methodology: Yang Zhao.
Project administration: Yuepeng Jiang, Xiaoxuan Zhao.
Resources: Li Liu.
Software: Yang Zhao.
Validation: Li Liu.
Visualization: Li Liu.
Writing – original draft: Yuepeng Jiang, Xiaoxuan Zhao.
Writing – review & editing: Yuepeng Jiang.
Footnotes
Abbreviations: CHD = atherosclerotic heart disease, IL-6 = interleukin-6, OR = odds ratio, TNF-α = tumor necrosis factor-alpha.
Statement: The ethical approval was not necessary. Because this study is about the Gene polymorphism associated with TNF-α (G308A) IL-6 (C174G) and susceptibility to coronary atherosclerotic heart disease: a meta-analysis. Because this paper is not a clinical trial study, ethical approval and informed consent are not required. All included articles have passed ethical approval and informed consent.
On behalf of all authors, the corresponding author states that there are no conflicts of interest. And manuscript is approved by all authors for publication.
References
- [1].Willerson JT, Ridker PM. Inflammation as a cardiovascular risk factor. Circulation 2004;109(21 suppl 1):II2–10. [DOI] [PubMed] [Google Scholar]
- [2].Sara JD, Eleid MF, Gulati R, et al. Sudden cardiac death from the perspective of coronary artery disease. Mayo Clin Proc 2014;89:1685–98. [DOI] [PubMed] [Google Scholar]
- [3].Hansson GK, Hermansson A. The immune system in atherosclerosis. Nat Immunol 2011;12:204–12. [DOI] [PubMed] [Google Scholar]
- [4].Tousoulis D, Economou EK, Oikonomou E, et al. The role and predictive value of cytokines in atherosclerosis and coronary artery disease. Curr Med Chem 2015;22:245–7. [DOI] [PubMed] [Google Scholar]
- [5].Christodoulidis G, Vittorio TJ, Fudim M, et al. Inflammation in coronary artery disease. Cardiol Rev 2014;22:279–88. [DOI] [PubMed] [Google Scholar]
- [6].Mirhafez SR, Zarifian A, Ebrahimi M, et al. Relationship between serum cytokine and growth factor concentrations and coronary artery disease. Clin Biochem 2015;48:575–80. [DOI] [PubMed] [Google Scholar]
- [7].Anderson DR, Poterucha JT, Mikuls TR, et al. IL-6 and its receptors in coronary artery disease and acute myocardial infarction. Cytokine 2013;62:395–400. [DOI] [PubMed] [Google Scholar]
- [8].Rajappa M, Sen SK, Sharma A. Role of pro-/anti-inflammatory cytokines and their correlation with established risk factors in South Indians with coronary artery disease. Angiology 2009;60:419–26. [DOI] [PubMed] [Google Scholar]
- [9].Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2197–223. [DOI] [PubMed] [Google Scholar]
- [10].Schulz S, Schlitt A, Lutze A, et al. Genetic variants in TNF-a and the one-year cardiovascular outcome in patients with coronary heart disease. Int J Cardiol 2013;168:1688–90. [DOI] [PubMed] [Google Scholar]
- [11].Satti HS, Hussain S, Javed Q. Association of interleukin-6 gene promoter polymorphism with coronary artery disease in Pakistani families. ScientificWorldJournal 2013;2013:538365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Asifa GZ, Liaquat A, Murtaza I, et al. Tumor necrosis factor-alpha gene promoter region polymorphism and the risk of coronary heart disease. ScientificWorldJournal 2013;2013:203492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Chu H, Yang J, Mi S, et al. Tumor necrosis factor-alpha G308A polymorphism and risk of coronary heart disease and myocardial infarction: a case-control study and meta-analysis. J Cardiovasc Dis Res 2012;3:84–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Bhanushali AA, Das BR. Promoter variants in interleukin-6 and tumor necrosis factor alpha and risk of coronary artery disease in a population from Western India. Indian J Hum Genet 2013;19:430–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Elsaid A, Abdel-Aziz AF, Elmougy R, et al. Association of polymorphisms G (-174)C in IL-6 gene and G (-1082)A in IL-10 gene with traditional cardiovascular risk factors in patients with coronary artery disease. Indian J Biochem Biophys 2014;51:282–92. [PubMed] [Google Scholar]
- [16].Ghazouani L, Abboud N, Khalifa SH, et al. 174G>C interleukin-6 gene polymorphism in Tunisian patients with coronary artery disease. Ann Saudi Med 2011;31:40–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Bennermo M, Nordin M, Lundman P, et al. Genetic and environmental influenceson the plasma interleukin-6concentration inpatients with a recent myocardial infarction: a case–control study. J Interferon Cytokine Res 2011;31:259–64. [DOI] [PubMed] [Google Scholar]
- [18].Fan WH, Liu DL, Xiao LM, et al. Coronary heart disease and chronic periodontitis: ispolymorphism of interleukin-6 gene the common risk factor in a Chinese population? Oral Dis 2011;17:270–6. [DOI] [PubMed] [Google Scholar]
- [19].Chakraborty B, Chowdhury D, Vishnoi G, et al. Interleukin-6 gene −174G/C promoter polymorphism predicts severity and outcome in acute ischemic stroke patients from north India. J Stroke Cerebrovasc 2012;22:683–9. [DOI] [PubMed] [Google Scholar]
- [20].Tuttolomondo A, Di Raimondo D, Forte GI, et al. Single nucleotide polymorphisms (SNPs) of pro-inflammatory/anti-inflammatory and thrombotic/fibrinolytic genes in patients with acute ischemic stroke in relation to TOAST subtype. Cytokine 2012;58:398–405. [DOI] [PubMed] [Google Scholar]
- [21].Çoker A, Arman A, Soylu O, et al. Lack of association between IL-1 and IL-6 gene polymorphisms and myocardial infarction in Turkish population. Int J Immunogenet 2011;38:201–8. [DOI] [PubMed] [Google Scholar]
- [22].Chumaeva N, Hintsanen M, Pulkki-Råback L, et al. Interleukin-6 gene polymorphism, chronic stress and atherosclerosis: interleukin-6-174G> C polymorphism, chronic stress and risk of early atherosclerosis in the Cardiovascular Risk in Young Finns Study. J Psychosom Res 2014;76:333–8. [DOI] [PubMed] [Google Scholar]
- [23].Huazhong University, Tong YQ. The Molecular Epidemiological Study of theAssociation Between Inflammatory Cytokines and Candidate Gene Polymorphisms and Environmental Exposures with Ischemic Stroke. 2011;1–151 (Doctor thesis). [Google Scholar]
- [24].Banerjee I, Pandey U, Hasan OM, et al. Association between inflammatory gene polymorphisms andcoronaryartery disease in an Indian population. J Thromb Thrombolysis 2009;27:88–94. [DOI] [PubMed] [Google Scholar]
- [25].Sarecka B, Zak I, Krauze J. Synergistic effects of the polymorphisms in the PAI-1 and IL-6 genes with smoking in determining their associated risk with coronary artery disease. Clin Biochem 2008;41:467–73. [DOI] [PubMed] [Google Scholar]
- [26].Elsaid A, Abdel-Aziz AF, Elmougy R, et al. Association of polymorphisms G (–174) C in IL-6 gene and G (–1082) A in IL-10 gene with traditional cardiovascular risk factorsin patients with coronary artery disease. Indian J Biochem Biophys 2014;51:282–92. [PubMed] [Google Scholar]
- [27].Li L, Li E, Zhang LH, et al. IL-6-174G/C and IL-6-572C/G polymorphisms are associated with increased risk of coronary artery disease. Genet Mol Res 2015;14:8451–7. [DOI] [PubMed] [Google Scholar]
- [28].Yang HT, Wang SL, Yan LJ, et al. Association of interleukin gene polymorphisms with the risk of coronary artery disease. Genet Mol Res 2015;14:12489–96. [DOI] [PubMed] [Google Scholar]
- [29].Hongmei Y, Yongping J, Jiyuan L. Interleukin-6 polymorphisms and risk of coronary artery diseases in a Chinese population: a case-control study. Pak J Med Sci 2016;32:880–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Carvalho V, Silva L, Werkhauser R, et al. Evaluation of IL-6 (-174 H/C) polymorphism in acute coronary syndrome in the northeast of Brazil. Int J Cardiovasc Sci 2016;29:288–94. [Google Scholar]
- [31].Gao Y, Jiang W, Yan Q, et al. Association between IL-6-174G/C and-572G/C polymorphisms and risk of coronary artery disease in a Chinese population. Int J Clin Exp Pathol 2016;9:282–7. [Google Scholar]
- [32].Tong Z, Li Q, Zhang J, et al. Association between interleukin 6 and interleukin 16 gene polymorphisms and coronary heart disease risk in a Chinese population. J Int Med Res 2013;41:1049–56. [DOI] [PubMed] [Google Scholar]
- [33].Mastana S, Prakash S, Akam EC, et al. Genetic association of pro-inflammatory cytokine gene polymorphisms with coronary artery disease (CAD) in a North Indian population. Gene 2017;628:301–7. [DOI] [PubMed] [Google Scholar]
- [34].Işik S, Hiz MM, Kiliç S, et al. Is there any increased risk of hypertension, diabetes and cardiac diseases in psoriatic patients with TNF-α G238A and G308A polymorphism? Postepy Dermatol Alergol 2016;33:440–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Zeybek U, Toptas B, Karaali ZE, et al. Effect of TNF-α and IL-1β genetic variants on the development of myocardial infarction in Turkish population. Mol Biol Rep 2011;38:5453–7. [DOI] [PubMed] [Google Scholar]
- [36].Ghaderian SM, Najar RA, Panah AST. Tumor necrosis factor-α: investigation of genepolymorphism and regulation of TACE–TNF-α system in patients with acute myocardial infarction. Mol Biol Rep 2011;38:4971–7. [DOI] [PubMed] [Google Scholar]
- [37].Vaccarino L, Vitale S, Caruso M, et al. Myocardial infarction marker levels are influenced by prothrombin and tumor necrosis factor-α gene polymorphisms in young patients. Cytokine 2013;61:218–22. [DOI] [PubMed] [Google Scholar]
- [38].Szabo GV. The role and importance of gene polymorphisms in the development of atherosclerosis. Interv Med Appl Sci 2013;5:46–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Ghazouani L, Ben HKS, Abboud N, et al. TNF-alpha -308 GNA and IL-6-174 GNC polymorphisms in the Tunisian patients with coronary artery disease. Clin Biochem 2010;43:1085–9. [DOI] [PubMed] [Google Scholar]
- [40].Hou L, Huang J, Lu X, et al. Polymorphisms of tumor necrosis factor-alpha gene and coronary heart disease in a Chinese Han population: interaction with cigarette smoking. Thromb Res 2009;123:822–6. [DOI] [PubMed] [Google Scholar]
- [41].Liu Y, Jin W, Lu L, et al. Association between single nucleotide polymorphism in thepromoter of tumor necrosis factor-α gene and coronary heart disease. J Diagn Concepts Pract 2009;5:506–9. [Google Scholar]
- [42].Banerjee I, Pandey U, Hasan OM, et al. Association between inflammatory gene polymorphisms and coronary artery disease in an Indian population. J Thromb Thrombolysis 2009;27:88–94. [DOI] [PubMed] [Google Scholar]
- [43].Hussain S, Iqbal T, Javed Q. TNF-alpha-308GOA polymorphism and the risk of familial CAD in a Pakistani population. Hum Immunol 2015;76:13–8. [DOI] [PubMed] [Google Scholar]
- [44].Cheng Y, An B, Jiang M, et al. Association of tumor necrosis factor-alpha polymorphisms and risk of coronary artery disease in patients with non-alcoholic fatty liver disease. Hepat Mon 2015;15:e26818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Chen W, Hua K, Gu H, et al. Methylenetetrahydrofolate reductase C667T polymorphism is associated with increased risk of coronary artery disease in a Chinese population. Scand J Immunol 2014;80:346–53. [DOI] [PubMed] [Google Scholar]
- [46].Garg PR, Saraswathy KN, Kalla AK, et al. Pro-inflammatory cytokine gene polymorphisms and threat for coronary heart disease in a North Indian Agrawal population. Gene 2013;514:69e74. [DOI] [PubMed] [Google Scholar]
- [47].Qi XM, Zhang R, Li JN, et al. High resolution fusion technology to detect patients with coronary heart disease. TNF- alpha and its receptor gene polymorphism. Clin Lab J 2014;32:405–9. [Google Scholar]
- [48].Zhao XL, Lin MH, Fan A, et al. Tumor necrosis factor single nucleotide polymorphism and association analysis of coronary heart disease in guangdong. Mod Prev Med 2015;42:2389–92. [Google Scholar]
- [49].Omer W, Naveed AK, Khan OJ, et al. Role of cytokine gene score in risk prediction of premature coronary artery disease. Genet Test Mol Biomarkers 2016;20:685–91. [DOI] [PubMed] [Google Scholar]
- [50].Anand V, Vaitheeshvaran S, Hedina MA, et al. Serum concentration and gene polymorphisms of IL-6 and TNF-α in cardiovascular disease. Int J Med Health Res 2016;2:7–11. [Google Scholar]
- [51].Gontsaruyk DA. Indicators proinflammatory cytokines tnf-α in patients with chronic pancreatitis and coronary heart disease. Pancreatology 2012;12:519–20. [Google Scholar]
- [52].Wang D, Wang R, Fang J, et al. Elevated serum levels of Ghrelin, TNF-α and IL-6 in congenital heart disease. Pediatrics Int 2015;58:259–64. [DOI] [PubMed] [Google Scholar]
- [53].Ahmad J, Ahmned F, Siddiqui MA, et al. Inflammatory markers, insulin resistance and carotid intima-media thickness in North-Indian type 2 diabetic subjects. J Assoc Phys India 2007;55:693. [PubMed] [Google Scholar]
- [54].Almohaya MA, Alharthi F, Arfin M, et al. TNF-α, and IL-10gene polymorphism and association with oral lichen planus risk in Saudi patients. J Appl Oral Sci 2015;23:295–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Wang J, He Y, Yang Y, et al. Association between the TNF-α G-308A polymorphism and risk of ischemic heart disease: a meta-analysis. Int J Clin Exp Med 2015;8:8880–92. [PMC free article] [PubMed] [Google Scholar]
- [56].Drutskaya MS, Nosenko MA, Atretkhany KN, et al. Interleukin-6: from molecularmechanisms of signal transduction to physiological properties and therapeutic targeting. Mol Biol 2015;49:837–42. [DOI] [PubMed] [Google Scholar]
- [57].Reichert S, Schlitt A, Benten AC, et al. The interleukin 6 C174T genotype is a predictor for new cardiovascular events in patients with coronary heart disease within three years follow-up. Cytokine 2016;83:136–8. [DOI] [PubMed] [Google Scholar]
- [58].Seino Y, Ikeda U, Ikeda M, et al. Interleukin 6gene transcripts are expressed in human atherosclerotic lesions. Cytokine 1994;6:87–91. [DOI] [PubMed] [Google Scholar]
- [59].Fishman D, Faulds G, Jeffery R, et al. The effect of novel polymorphisms in the interleukin-6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and an association with systemic-onset juvenile chronic arthritis. J Clin Invest 1998;102:1369–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [60].Nauck M, Winkelmann BR, Hoffmann MM, et al. The interleukin-6 C174G promoter polymorphism in the LURIC cohort: no association with plasma interleukin -6, coronary artery disease, and myocardialinfarction. J Mol Med (Berl) 2002;80:507–13. [DOI] [PubMed] [Google Scholar]