

Abstract
A single armed, prospective, two-center study was conducted with an aim of evaluating the effectiveness of the AMS 700 LGX cylinders in maintaining or increasing penile length postimplantation. The LGX has the unique ability to expand in length with inflation. Only 23.1% (6) of the patients were able to maintain stretched penile length. We now recommend leaving the implant inflated 60%–80% in the immediate postoperative setting for approximately 6 weeks. Then we teach pump training with deflation at around 6 weeks, prior to a maximum inflation protocol daily. Further studies would be required to validate if these interventions have significantly increased the number of patients who maintain or gain stretched penile length.
Worldwide, prevalence of erectile dysfunction (ED) is expected to reach 322 million cases by 2025, making it a major health problem.1 ED can be effectively treated with lifestyle modification and/or with the use of phosphodiesterase type 5 (PDE5) inhibitors, a variety of second line therapies, or definitive surgical implantation of an inflatable penile prosthesis (IPP).
A study showed that mean corporal length and implant device size increased from 2005 to 2010. However, clinically significant (0.5 cm or greater) decreases in corporal length were noted in patients with Peyronie's disease (PD) or a history of radical pelvic surgery (excluding prostatectomy). Mean average implant device sizes were 19.4 cm long in the USA compared to 17.7 cm outside the USA. Coloplast also recorded an increased use of 18 cm and 20 cm cylinders and decreased use of 16 cm cylinders during this study period.2 Despite discrepancy in etiology, the prevalence of penile shortening in this patient population is high, causing valid concern on the part of patients as well as surgeons to maintain penile length in these patients.
Other therapies have been studied to address penile shortening. A pilot randomized study is evaluating the use of vacuum erection devices and their effects on penile length and girth in corresponding cylinder size preoperatively.3 Results from a prospective study indicate that surgeons placing IPPs via a transcrotal approach resulted in an approximately 1–2 cm increased length of prosthesis inserted compared to IPP placement with infrapubic approach.4 In one noncontrolled pilot study evaluating the efficacy of external penile traction therapy, they found preservation of penile length as well as a small length gain in 70% of patients, however the technique is tedious and requires compliance to be effective.5
Recently, the AMS 700 LGX IPP was introduced with technical improvements to address penile length preservation. It includes improved Ultrex cylinders, which increase in both length and the girth of implant. Scovell et al.6 reported on ex vivo biomechanical data that showed a 3.1–3.9 cm increase in length with max inflation of the 18 cm and 21 cm AMS LGX, respectively. A prospective study showed that the use of the AMS 700 LGX corresponded to a 10% length restoration with at least 1 cm increase at 12 months postoperatively and an 80% overall satisfaction rate.7 The AMS 700 LGX could be a steadfast tool to prevent loss of penile length and should be considered in all patients (without fibrosis or scarring) to optimize penile length and girth in the postoperative setting. The aim of this study was evaluating the effectiveness of the AMS 700 LGX cylinders in maintaining or increasing penile length postimplantation.
PATIENTS AND TECHNIQUE
This was a single-armed, prospective, two-center study evaluating the AMS 700 LGX cylinder (Boston Scientific, Marlborough, MA, USA) in maintaining penile length after IPP implantation (IRB#: HSC-MS-08-0096 for University of Texas Health Sciences Center, Houston, TX, USA; and 1103171 for Ark La Tex Urology, Bossier City, LA, USA). Success was defined as the distal length of a patient's penis at 12 months postimplant being greater than the length of that patient's penis at preimplant (baseline). The LGX cylinders were used because of their ability to expand both in length as well as in diameter.
Twenty-six patients, with a mean age of 60.3 (standard deviation [s.d.]: 7.7) years, were enrolled in the study and 4 patients withdrew prior to completion. All devices were implanted using the penoscrotal approach. Following implantation, patients were evaluated at scheduled follow-up visits: activation (4–8 weeks), 6- and 12-month intervals from time of implantation.
The investigators followed the standard operating procedure and used the new length measurement technique (NLMT) method of cylinder sizing.8 Penile measurements were taken using a paper ruler calibrated to the nearest 0.5 cm. Each measurement was taken twice for accuracy and the mean value was used in data analysis. The first set of measurements was obtained in the preoperative holding area prior to any anesthetic medications. Width of the penis was measured by a caliper. The following measurements (in cm) were taken (Figure 1).
Figure 1.
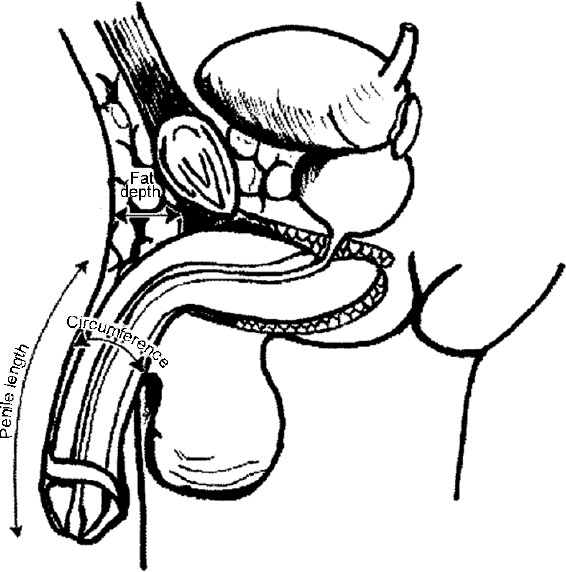
Penile measurements.
Stretched penile length: from the pubopenile skin junction to the meatus with maximal extension of the phallus.
Penile circumference: at midshaft
Width of penis: measured by a caliper 1 cm proximal to the corona.
The IPP was left deflated postimplantation until the activation follow-up visit. At 4 months postimplant, patients were given max-inflation instructions. The patient was instructed to inflate their IPP daily, until it became slightly uncomfortable, and then leave it maximally inflated for 30–90 min (Table 1).
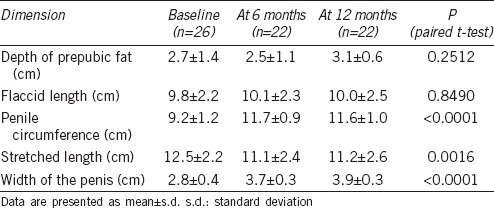
Table 1.
Penile measurements
Physicians assessed device function, measurement of penile length, measurement of penile girth, and adverse events. A paired t-test was used to evaluate the change in each dimension at 12 months compared to baseline for all subjects. Subjects were questioned on their satisfaction as measured by the nonvalidated Penile Prosthesis Patient Satisfaction Survey (PPPSS) as well as improvement in their ED as measured by the validated International Index of Erectile Function (IIEF).
Patient demographics are listed in Supplementary Table 1 (733.4KB, tif) . The most common etiology for ED was postprostatectomy (50.0%). Thirteen (50.0%) of these patients had ED for more than 5 years. Mean procedure time was 38 ± 20.9 min, and all patients were discharged the day of the procedure. No surgical complications were reported and blood loss was minimal. Fourteen (53.8%) patients received 21 cm cylinders.
Patient demographics
All subjects showed an increase in penile circumference (Figure 2a; 9.2–11.6 cm, P < 0.0001) and penile width increased from 2.8 cm to 3.9 cm (P = 0.0001). On average, there was a statistically significant decrease in stretched penile length (Figure 2b; 12.5–11.2 cm, P = 0.0016). There was no change in depth of prepubic fat and flaccid penile length across visits. An increase in stretched penile length was seen in only 6 (23.1%) patients. Improvement of ED symptoms were measured using the IIEF questionnaire, as reported in Supplementary Table 2 (453.2KB, tif) . Eighteen (69.2%) patients reported having no ED at 12 months postimplantation, while 2 (7.7%) patients reported having mild ED. Mean IIEF scores increased from 8.1 (s.d.: 2.3) at 6 months to 8.4 (s.d.: 2.3) at 12 months. Patient satisfaction was reported through the PPPSS. High or very high satisfaction was reported in 73.0% of the patients. Sixteen (61.5%) and 17 (65.4%) patients were satisfied with the length and width of their erections, respectively. Twenty-one (80.7%) patients were satisfied with the firmness of their erections, and 22 (84.5%) were satisfied with their ability to have intercourse.
Figure 2.
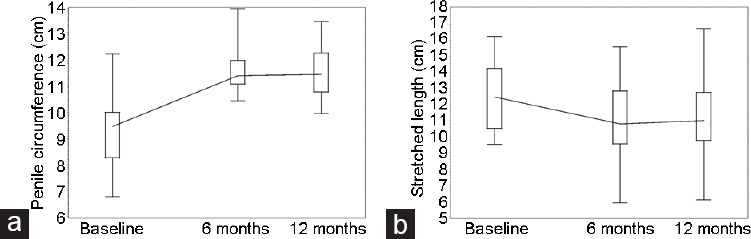
(a) Penile circumference and (b) stretched penile length across visits.
EF and OS domains of IIEF at 6 and 12 months
COMMENTS
Implantation of IPP is a successful intervention with high rates of satisfaction. Complications such as mechanical failure (7%–15%) and infection (1%–3%) are less common. However, for many patients with ED who choose surgical treatment, loss of penile length after implantation of an IPP is a major concern.9 Many of them perceive or experience shortening after their procedure causing frustration and dissatisfaction. Placement of IPPs for management of refractory ED shows excellent outcomes with satisfaction rates averaging 92%–100%, however, up to 30% of patients complain of penile shortening (average 0.75 cm) postprocedure.4 Patients who have undergone a radical prostatectomy or other radical pelvic surgery, those who have undergone androgen suppression plus radiation therapy, and patients with PD often experience penile shortening.10,11,12 The exact cause of this physiology is unknown, however, possible explanations for penile shortening include postoperative fibrotic changes, lack of glans tumescence, denervation atrophy, hypoxia, or apoptosis of penile erectile tissue.12 It could also be due to the conventional method of sizing of cylinders in the IPP procedure, where cylinders are sometimes down-sized 0.5 cm to 2 cm in length compared to the length of the corpora.13,14,15 This is no longer advocated.
All subjects showed increases in penile circumference and width. Overall, there was a slight decrease in stretched penile length, likely due to postoperative fibrotic changes, lack of glans tumescence, denervation atrophy, hypoxia, apoptosis of penile erectile tissue, capsular contraction, or a combination of these entities. The relatively long latency time (4 months) prior to activation of max inflation protocols may play a large role in the loss of length due to formation of the surgical capsule and capsular contraction prior to routine device usage. In our clinical practice, we now recommend leaving the implant inflated 60%–80% in the immediate postoperative setting for approximately 6 weeks, and then teaching pump training with deflation at around 6 weeks. Now, we also typically ask patients to begin daily maximum inflation protocols in which they inflate as much as they can, without causing pain, for 30–90 min each day. There were no statistically significant changes in depth of prepubic fat and flaccid penile length across visits so this did not seem to account for decreases in length.
In a study comparing Coloplast Titan and AMS LGX, it was found that AMS LGX increased penile length especially with increased filling pressures compared to minimal lengthening with the Titan.15 Additionally, with maximum inflation, the 18 cm Coloplast remained at 18 cm compared to the 18 cm AMS 700 LGX which increased in length to 18.9 cm. In another study of ex vivo implants, the AMS 700 LGX increased in length on average 13 mm from baseline, a unique characteristic from other prostheses.6 It was concluded that patients who were more concerned with preserving length, the AMS LGX was optimal. Based on these findings, it is unlikely the LGX itself is the cause of penile shortening. It is instead more likely the time delay after surgery in which patients were deactivated with minimal inflation caused penile shortening.
In our cohort an increase in stretched penile length was seen in only 6 (23.1%) patients. Future studies could assess comparative effectiveness of NLMT and early max-inflation protocol in maintaining or increasing stretched penile length, both alone and in combination. In regard, to those patients who did not experience increased length, inflation protocols could be implemented immediately postoperative, as in our clinic, to decrease the latency period and prevent capsular contraction.
Most patients reported no ED at 12 months postimplantation. Two patients reported mild ED. IIEF scores increased between 6 months and 12 months. High or very high overall satisfaction, with high rates of satisfaction with erectile length, firmness, width, and ability to have intercourse was reported, consistent with historic outcomes.
A weakness of this study was the inability to compare preimplant erection length and immediate postimplantation inflated length to assess comparative degree of improvement or change. A second, key weakness is that there are only 26 patients included in our study. Additionally, only 12-month follow-up data was available for review and longer-term follow-up had poor participation.
CONCLUSION
Implantation of the length expanding AMS 700 LGX cylinders are not sufficient for increasing stretched penile length. Early postoperative inflation guidelines are essential for maintaining or increasing penile length. In our clinical practice we now recommend leaving the implant inflated 60%–80% in the immediate postoperative setting for approximately 6 weeks. Then we teach pump training with deflation at around 6 weeks, prior to instituting a maximum inflation protocol for 30–90 min daily. Further studies would be required to validate if these interventions have significantly increased the number of patients who maintain stretched penile length.
AUTHOR CONTRIBUTIONS
JJW, SKM and GDH developed original content. GDH and RW provided patient database from 2 separate centers. All were involved in editing this paper to its final version, however, JJW was the main organizer and editor. All authors read and approved the final manuscript.
COMPETING INTERESTS
GDH and RW are both consultants for Coloplast (Minneapolis, MN, USA) and Boston Scientific (Marlborough, MA, USA).
ACKNOWLEDGMENTS
This work was funded by American Medical Systems and Boston Scientific.
Supplementary Information is linked to the online version of the paper on the Asian Journal of Andrology website.
REFERENCES
- 1.Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts male aging study. J Urol. 1994;151:54–61. doi: 10.1016/s0022-5347(17)34871-1. [DOI] [PubMed] [Google Scholar]
- 2.Welliver C, Kottwitz M, Ahmad AE, Wilson SK, Kohler TS. Manufacturers’ data show increasing implanted cylinder sizes and measured corporal lengths in inflatable penile implants. World J Urol. 2016;34:993–8. doi: 10.1007/s00345-015-1705-2. [DOI] [PubMed] [Google Scholar]
- 3.Pahlajani G, Raina R, Jones S, Ali M, Zippe C. Vacuum erection devices revisited: its emerging role in the treatment of erectile dysfunction and early penile rehabilitation following prostate cancer therapy. J Sex Med. 2012;9:1182–9. doi: 10.1111/j.1743-6109.2010.01881.x. [DOI] [PubMed] [Google Scholar]
- 4.Trost LW, Boonjindasup AG, Hellstrom WJ. Comparison of infrapubic versus transcrotal approaches for inflatable penile prosthesis placement: a multi-institution report. Int J Impot Res. 2015;27:86–9. doi: 10.1038/ijir.2014.35. [DOI] [PubMed] [Google Scholar]
- 5.Levine LA, Rybak J. Traction therapy for men with shortened penis prior to penile prosthesis implantation: a pilot study. J Sex Med. 2011;8:2112–7. doi: 10.1111/j.1743-6109.2011.02285.x. [DOI] [PubMed] [Google Scholar]
- 6.Scovell JM, Ge L, Barrera EV, Wilson SK, Carrion RE, et al. Longitudinal and horizontal load testing of inflatable penile implant cylinders of two manufacturers: an ex vivo demonstration of inflated rigidity. J Sex Med. 2016;13:1750–7. doi: 10.1016/j.jsxm.2016.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Negro CL, Paradiso M, Rocca A, Bardari F. Implantation of AMS 700 LGX penile prosthesis preserves penile length without the need for penile lengthening procedures. Asian J Androl. 2016;18:114–7. doi: 10.4103/1008-682X.154311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Henry G, Houghton L, Culkin D, Otheguy J, Shabsigh R, et al. Comparison of a new length measurement technique for inflatable penile prosthesis implantation to standard techniques: outcomes and patient satisfaction. J Sex Med. 2011;8:2640–6. doi: 10.1111/j.1743-6109.2011.02340.x. [DOI] [PubMed] [Google Scholar]
- 9.Deveci S, Martin D, Parker M, Mulhall JP. Penile length alterations following penile prosthesis surgery. Eur Urol. 2007;51:1128–31. doi: 10.1016/j.eururo.2006.10.026. [DOI] [PubMed] [Google Scholar]
- 10.Haliloglu A, Baltaci S, Yaman O. Penile length changes in men treated with androgen suppression plus radiation therapy for local or locally advanced prostate cancer. J Urol. 2007;177:128–30. doi: 10.1016/j.juro.2006.08.113. [DOI] [PubMed] [Google Scholar]
- 11.Savoie M, Kim SS, Soloway MS. A prospective study measuring penile length in men treated with radical prostatectomy for prostate cancer. J Urol. 2003;169:1462–4. doi: 10.1097/01.ju.0000053720.93303.33. [DOI] [PubMed] [Google Scholar]
- 12.Munding MD, Wessells HB, Dalkin BL. Pilot study of changes in stretched penile length 3 months after radical retropubic prostatectomy. Urology. 2001;58:567–9. doi: 10.1016/s0090-4295(01)01270-5. [DOI] [PubMed] [Google Scholar]
- 13.Montague DK, Angermeier KW. Increasing size with penile implants. Curr Urol Rep. 2008;9:483–6. doi: 10.1007/s11934-008-0082-4. [DOI] [PubMed] [Google Scholar]
- 14.Wilson SK, Henry GD. Penoscrotal approach for three-piece and two-piece hydraulic penile implants. Atlas Urol Clin North Am. 2002;10:169–80. [Google Scholar]
- 15.Barboglio Romo P, Chikkatur HP, Beldona S, Yi Y, Bruns TM, et al. Comparative evaluation of physical characteristics of different inflatable penile prostheses. Scand J Urol. 2017;51:420–5. doi: 10.1080/21681805.2017.1339292. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Patient demographics
EF and OS domains of IIEF at 6 and 12 months