

Abstract
Purpose:
Racial discrimination has long-term consequences for cardiovascular health, potentially by dysregulating acute physiological responses. However, the role of psychological factors that may be protective or increase vulnerability for dysregulated responses, such as racial identity, remains unclear. This study examines the association between racial discrimination and acute parasympathetic responses, and the role of racial centrality, private regard, public regard in this association.
Methods:
Black young adults (N = 119, Mage = 19.45) recruited from a predominantly White institution in the southeastern United States completed an online survey (in which racial discrimination, racial identity, and control variables were reported) and a laboratory visit, during which they were exposed to a vignette of racial discrimination while their parasympathetic activity (indexed by respiratory sinus arrhythmia) was recorded.
Results:
While racial discrimination was not associated with respiratory sinus arrhythmia reactivity or recovery, centrality moderated this association such that more frequent racial discrimination was associated with greater parasympathetic reactivity and recovery only among participants low in racial centrality. Neither private regard nor public regard emerged as significant moderators.
Conclusions:
This study is the first to show that lower levels of racial centrality can mitigate the association between discrimination and acute parasympathetic responses, which has important implications for initiatives aimed at reducing cardiovascular risk for Black young adults.
Keywords: respiratory sinus arrhythmia, racial discrimination, racial identity, Black Americans, young adults
Black young adults are at higher risk for developing precursors to cardiovascular disease than other racial/ethnic groups in the United States (1). Racial discrimination (RD), defined as actions by members of dominant racial groups that have negative and differential impacts on members of non-dominant racial groups (2), is a contributor to poor health in Blacks (3) and poses developmental risks for Black youth transitioning from adolescence to adulthood (4). RD may negatively impact Black young adults’ physiological responses (5), a precursor to long-term cardiovascular health (6). However, not all Black young adults who encounter RD physiologically respond in unhealthy ways. Therefore, the present study examines racial identity, the significance and meaning that Black individuals place on race when defining themselves (7), as a protective or vulnerability factor in the link between RD and physiological functioning.
Racial Discrimination and Acute Physiological Responses
The Biopsychosocial Model of Racism affirms that RD engenders exaggerated and prolonged autonomic nervous system (ANS) responses to threat (8). Physiological overactivation or underactivation due to RD erodes health by conditioning cardiovascular responses to subsequently experienced acute stressors (9–12), preparing Black bodies for future social assaults (13). The present study extends the literature on RD and ANS activity by examining the parasympathetic nervous system (PNS), which has a wide range of control over heart rate regulation via the vagus nerve and is thereby a more sensitive marker of the impact of social stressors (14). We assessed PNS influence by calculating respiratory sinus arrhythmia (RSA) via the magnitude of heart rate variability (HRV) during the respiratory cycle. According to Porges’ Polyvagal Theory (15), RSA is sensitive to social interactions and therefore may be especially important for understanding social stressors such as RD. During a stressful situation, RSA should decrease from a baseline level (RSA withdrawal) as individuals bolster psychological resources. The degree of RSA withdrawal could signal disease risk, as lower HRV is a predictor of cardiovascular disease and all-cause mortality (16). During recovery, after the stressor has been removed, RSA activity should rebound (RSA augmentation), evidencing higher levels of PNS activity. The absence of such augmentation is associated with ventricular valve health and subsequent risk for chronic hypertension (17). Therefore, there are two stages of a physiological response to acute stress: a reactivity period wherein the individual is attending to a stressor during which RSA decreases from baseline levels (RSA withdrawal), and a recovery period wherein the stressor is removed and RSA increases from stress level (RSA augmentation). Experimental studies have documented PNS withdrawal during reactivity to racism tasks (18) and less PNS augmentation during recovery from these tasks (19). Negative associations between chronic RD and HRV have also been reported (5, 20). However, a paucity of studies consider the relationship between RD and RSA and examine differences in RSA during both reactivity and recovery periods.
The Role of Racial Identity
The transition from adolescence to young adulthood for Black individuals can be shaped by racial prejudice (4) and experiencing RD propels Black young adults to explore racial identities (21). The present study examines three dimensions of racial identity aligned with the Multidimensional Model of Racial Identity (7) - centrality (the degree to which one defines oneself in terms of race), private regard (how one views Black individuals and their own group membership), and public regard (how one believes others view Black individuals). Racial identity is believed to mitigate the adverse effects of RD on health (22, 23). However, examination of racial identity has produced inconsistent results, suggesting that racial identity could be a protective or vulnerability factor for health outcomes. For example, private regard has served as a protective factor in investigations spanning psychosocial and health outcomes for Black adolescents and young adults (24–25), but was not protective in others (26). While a preponderance of research documents a positive association between centrality and psychological distress (27–28), some studies have documented the inverse association (23). Low public regard is found to buffer individuals from the negative consequences of RD on well-being, specifically depressive symptoms (25). One of the first to examine past year RD and racial identity on RSA, this study helps contextualize these inconsistent results.
Although racial identity has received attention as a protective factor, few studies consider the role of racial identity in the association between RD and acute PNS responses. In the one study of racial identity as protective for acute PNS responses, Black college students high on private regard and low on public regard exhibited RSA withdrawal during reactivity to racism vignettes with a White perpetrator, but RSA augmentation during recovery (24). No significant interactions were found for racial centrality. As this study did not examine past year RD, the present study is an important addition as frequent past year RD may condition dysregulated acute physiological responses to stressors, increasing the potential for cardiovascular risk over time.
The Present Study
Grounded in psychobiological (8, 15) and racial identity (7) frameworks, our investigation adds to the nascent body of literature examining how RD experiences may relate to Black young adults’ acute RSA responses to a lab-based racial stressor and the role of racial identity in this association. All moderation hypotheses were proposed in line with Neblett and Roberts (24). Our study examined the following questions:
RQ1. Is RD associated with acute RSA reactivity (RQ1a) and recovery to a lab-based racial stressor (RQ1b)? We hypothesized that RD would be associated with acute RSA withdrawal during reactivity (RQ1a) and recovery (RQ1b).
- RQ2. Do racial identity dimensions (centrality, private regard, and public regard) moderate the association between RD and acute RSA reactivity (RQ2a) and recovery (RQ2b)?
- RQ2a (RSA reactivity): For individuals high on private regard and low on public regard, we hypothesized that more frequent RD would be associated with RSA withdrawal, compared to no association between chronic RD and RSA reactivity for individuals low on private and high on public regard. We hypothesized that racial centrality would not moderate the association between RD and RSA reactivity.
- RQ2b (RSA recovery): For individuals high on private regard and low on public regard, we hypothesized that more frequent RD would be associated with RSA augmentation, compared to no association with RSA recovery for individuals low on private regard. We hypothesized that racial centrality would not be a moderator.
Methods
Participants
Data were collected as part of a larger study of Black college students attending a large public predominantly White institution in the southeastern United States. The sample comprised 131 Black undergraduate students whose RSA was measured via a laboratory visit, 12 of which were excluded due to missing predictor values or equipment errors, resulting in a final analytic sample of 119 (Mage= 19.45, SDage= 1.42, 76.5% female). The majority of students identified as first-year (34.5%) or sophomore (30.3%) students. A majority of the sample identified as Black/African American (84.9%), while 10.1% of participants identified as Bi-/multi-racial, .8% identified as African, and 4.2% identified as Afro-Central/South American or Caribbean Black. The analytic sample largely reported no history of cardiovascular concerns (95.8%).
Measures
Demographic measures.
Demographic measures of age, sex, highest level of parental education, and body mass index (BMI) were control variables in our analyses. Research identifies differences in RSA by age (28), sex (29), BMI (30), and parental education (as a proxy for socioeconomic status; 31). Participants were asked to identify their sex by indicating male, female, or other, and indicated highest level of education completed by their parents (mother or father) using the following options: did not finish high school, General Equivalency Diploma, Associate’s degree/Vocational training or licensure, Bachelor’s degree, or Master’s degree or higher. BMI was calculated for each participant from self-reported height and weight using the Center for Disease Control’s formula.
Racial discrimination.
The Daily Life Experiences Scale (DLE; sample α=.92), a subscale of the Racism and Life Experiences Scale (32), was utilized to assess the frequency with which participants experienced 18 racial hassles in the past year (e.g., “In the past year, how often have you been ignored, overlooked, or not given service because of your race?”). Responses were made on a 6-point Likert-type scale ranging from 0 (never) to 5 (once a week or more). Scores were computed by averaging responses resulting in a continuous variable with higher numbers equaling greater experiences of discrimination.
Racial identity.
Three subscales of the Multidimensional Inventory of Black Identity (MIBI; 33) were used to assess private regard, public regard, and centrality. The private regard subscale (sample α = .79) consisted of six items that measure participants’ feelings about being Black and Black people (e.g., “I am happy that I am Black”). The public regard subscale (sample α = .85) consisted of six items that measure participants’ feelings about how others view Black people (e.g., “Overall Blacks are considered good by others”). The centrality subscale (sample α= .82) consisted of eight items that measure the degree to which participants’ define themselves in terms of their race (e.g., “In general, being Black is an important part of my self-image”). Responses to the MIBI are rated from 1 (strongly disagree) to 7 (strongly agree) and sub-scale scores were computed by averaging sub-scale items, resulting in continuous variables with higher numbers equaling higher private regard, private regard, and centrality.
Respiratory Sinus Arrhythmia.
Electrocardiogram data were collected using a Biopac (Goleta, CA) MP150 amplifier. Interbeat intervals were extracted from the electrocardiogram waveform in the Biopac AcqKnowledge program. The waveform and interbeat interval sequence for each participant were aligned and visually inspected for movement artifacts in CardioEdit. Edits were minimal (no more than 1% of data per file), adhering with CardioEdit editing rules. Edited interbeat intervals were then submitted to the CardioBatch program, which calculated three RSA values for each participant (baseline, stress, and recovery) using the Porges-Bohrer Method for extracting the high frequency component of each interbeat interval sequence from the .12-.4 Hz spectral frequency band-pass for adults (34). From these three RSA scores, RSA change scores were calculated for each participant. RSA reactivity was calculated by subtracting baseline RSA from stress RSA, and RSA recovery was calculated by subtracting stress RSA from recovery RSA.
Procedure
The data were from a two-part study, with part one being an online Qualtrics survey and part two being a laboratory visit. Participants were recruited for the two-part study via campus organizations, class announcements, psychology department participant pool, and flyers. Eligibility criteria for each part of the study included: 18 years or older, fluent in written and spoken English, and undergraduate student. After electronic consent, participants self-reported demographic information, past year RD, and racial identity in part one. After in-person consent, part two measured participants’ RSA in response to a task. Participants must have completed part one in order to begin part two. A subset of participants completed both parts of the study. There were no meaningful differences on study variables between participants who completed the laboratory visit and those who did not (see Appendix A, which can be found online). Power analyses for the current investigation indicated that a sample size of 113 was necessary to detect a small effect (f2=.15) at a power level of .80 (α=.05). Participants earned $10 or participant pool credit for each part of the study. The study was approved by the University of North Carolina at Chapel Hill’s institutional review board.
During the laboratory visit, a Black research assistant administered an electrocardiogram and a White research assistant conducted a stress task. Three leads were secured to the participant’s body following a modified Lead III Einthoven’s equilateral triangle configuration. Participants were instructed to relax for five minutes (baseline period). Next, participants were presented with the stress task (stress period), which entailed being read a vignette about a student who experiences RD in a classroom setting (see Appendix B, which can be found online) and being asked to respond to the vignette as though they were experiencing it. This task was designed based on previous literature indicating that vignettes of RD produce acute physiological stress responses (24), and the vignette was based on data that indicates perceptions of affirmative action are common and frequent experiences for Black students (35, 36). Each participant was presented with the same vignette. Afterward, the participant engaged in another five minutes of relaxation (recovery period) and was debriefed.
Analysis Plan
Descriptive statistics and inter-correlations were first examined. Significant differences in RSA during baseline, stress, and recovery periods were then assessed to confirm the validity of the laboratory task as a measure of physiological stress. To address each research question, multivariate linear regression models (one for recovery and another for reactivity) were estimated using full information maximum likelihood (FIML) with robust standard errors to address non-normality in RSA change scores. FIML estimation was used to handle missing data. To address the first research question, the association between RD and RSA reactivity net the effects of control variables and baseline RSA score (RQ1a) and RD and RSA recovery net the effects of control variables, baseline RSA score, and stress RSA score (RQ1b) were examined. To address the second research question, we assessed whether centrality, private regard, and public regard moderated the associations between RD and RSA reactivity (RQ2a) and RSA recovery (R2b). Interaction terms were constructed using mean-centered variables. Significant interactions were probed at low (−1 SD), mean, and high (+1 SD) levels.
Results
Study analyses were conducted in Mplus version 8 (37). Descriptive statistics and inter-correlations are reported in Table 1. Repeated measures ANOVA indicated significant differences in RSA during baseline, stress, and recovery (F (1.58, 187.97) = 14.04, p < .01) after Greenhouse-Geisser corrections for violation of sphericity assumptions (χ2 (2) = 36.51, p < .01). Post-hoc pairwise comparison revealed that RSA during stress was lower than RSA during baseline (M difference = −.32, 95% C.I. [−.46, −.18]; Hedge’s g = −.31), RSA during recovery was higher than RSA during stress (M difference = .21, 95% C.I. [.07, .34]; Hedge’s g = .19), and RSA during baseline was higher than RSA during recovery (M difference = .11, 95% C.I. [.02, .20]; Hedge’s g = .10). Magnitude of the effect sizes were relatively small (Hedge’s g < .20), with the exception of the difference between RSA baseline and RSA stress (Hedge’s g = −.31; small-moderate).
Table 1.
Descriptive Statistics and Intercorrelations Between Study Variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | M(SD) or % | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| -- | 24.2% | |||||||||||||
| 1. Male | ||||||||||||||
| .18* | -- | 19.43 (1.42) | ||||||||||||
| 2. Age | ||||||||||||||
| <.01 | .17 | -- | 25.85 (5.23) | |||||||||||
| 3. BMI | ||||||||||||||
| 4. Parent Education Attainment | .09 | −.23* | −.12 | -- | 3.82 (1.18) | |||||||||
| 5. Racial Discrimination | .05 | −.05 | .12 | .19* | -- | 1.35 (.87) | ||||||||
| 6. Centrality | −.13 | −.08 | .12 | .10 | .42* | -- | 5.03 (1.11) | |||||||
| 7. Private Regard | −.21* | −.18* | −.15 | .11 | .05 | .34* | -- | 6.36 (.70) | ||||||
| 8. Public Regard | .19* | −.13 | −.07 | .12 | −.27* | −.18* | .10 | -- | 2.90 (1.07) | |||||
| 9. RSA (Baseline) | .07 | −.11 | .04 | .02 | −.08 | .13 | −.01 | .03 | -- | 6.48 (1.08) | ||||
| 10. RSA (Stress) | .20* | −.13 | .00 | −.03 | −.08 | −.09 | −11 | .11 | .74** | -- | 6.17 (1.03) | |||
| 11. RSA (Recovery) | .15 | −.06 | .05 | .05 | −.06 | −.11 | −.12 | −.04 | .90** | .77** | -- | 6.35 (1.14) | ||
| 12. RSA (∆Baselineto Stress) | .14 | .01 | −.04 | −.01 | −.01 | .03 | −.17 | .08 | −.39** | .29** | −.20* | -- | −.32 (.74) | |
| 13. RSA (∆Stress to Recovery) | −.09 | .04 | .03 | .04 | .05 | .01 | .02 | −.18* | .31** | −.24** | .40** | −.76** | -- | .17 (.71) |
Note.
is p < .05.
is p < .01.
RD and RSA Reactivity and Recovery
After control variables were incorporated, RD was not associated with RSA reactivity or RSA recovery (see Table 2).
Table 2.
Research Question 1: Associations between Racial Discrimination and RSA Changes
| RSA Reactivity | RSA Recovery | |||||
|---|---|---|---|---|---|---|
| Predictors | b | s.e | p | b | s.e | p |
| Male | .34 | .14 | .02 | .02 | .11 | .86 |
| Age | −.05 | .05 | .30 | .03 | .03 | .34 |
| Parental Education | −.02 | .06 | .75 | .002 | .05 | .97 |
| BMI | .001 | .01 | .96 | −.001 | .01 | .86 |
| RSA Baseline | −.29 | .06 | < .01 | .71 | .07 | < .01 |
| RSA Stress | -- | -- | -- | −.71 | .08 | < .01 |
| Racial Discrimination | −.04 | .07 | .63 | .03 | .04 | .52 |
Notes. BMI = body mass index, RSA = respiratory sinus arrhythmia.
Racial Identity Dimensions and RSA Reactivity
The interaction between RD and centrality (b = −.18) was associated with RSA reactivity (see Table 3). In particular, more frequent RD was associated with augmentation in RSA reactivity from baseline to stress at low levels of racial centrality (b = .25), but not at moderate and high levels of racial centrality (see Figure 1). The interactions between RD and private regard and RD and public regard were nonsignificant.
Table 3.
Research Question 2: Racial Identity Dimensions as Moderators of the Association between Discrimination and RSA Changes
| RSA Reactivity |
RSA Recovery |
|||||
|---|---|---|---|---|---|---|
| Centrality | b | s.e | p | b | s.e | p |
| Male | .32 | .14 | .02 | .02 | .11 | .83 |
| Age | −.04 | .05 | .43 | .04 | .03 | .23 |
| Parental Education | −.03 | .05 | .62 | −.004 | .04 | .93 |
| BMI | −.002 | .01 | .88 | −.003 | .01 | .71 |
| RSA Baseline | −.29 | .06 | < .01 | .73 | .07 | < .01 |
| RSA Stress | -- | -- | -- | −.74 | .08 | < .01 |
| Racial Discrimination | .03 | .08 | .67 | .06 | .05 | .22 |
| Centrality | −.002 | .06 | .98 | .01 | .04 | .72 |
| Racial Discrimination X | −.18 | .06 | < .01 | −.11 | .04 | .01 |
| Centrality | ||||||
|
Conditional Effects for Centrality | ||||||
| −1 SD of Centrality | .25 | .12 | .04 | .19 | .09 | .02 |
| Mean of Centrality | .03 | .08 | .67 | .06 | .05 | .22 |
| +1 SD of Centrality | −.18 | .11 | .10 | −.07 | .05 | .21 |
| Private Regard | ||||||
| Male | .29 | .14 | .03 | .01 | .11 | .92 |
| Age | −.06 | .04 | .14 | .03 | .03 | .39 |
| Parental Education | −.02 | .06 | .78 | .003 | .05 | .94 |
| BMI | −.01 | .01 | .72 | −.002 | .01 | .81 |
| RSA Baseline | −.29 | .06 | < .01 | .71 | .06 | < .01 |
| RSA Stress | -- | -- | -- | −.71 | .08 | < .01 |
| Racial Discrimination | −.02 | .08 | .84 | .03 | .05 | .53 |
| Private Regard | −.21 | .09 | .01 | −.04 | .07 | .57 |
| Racial Discrimination X Private | −.10 | .13 | .43 | .004 | .10 | .97 |
| Regard | ||||||
| Public Regard | ||||||
| Male | .31 | .16 | .05 | .05 | .12 | .69 |
| Age | −.05 | .04 | .29 | .02 | .04 | .58 |
| Parental Education | −.02 | .06 | .74 | .01 | .05 | .79 |
| BMI | < .001 | .01 | .98 | < .001 | .01 | .99 |
| RSA Baseline | −.29 | .06 | < .01 | .71 | .06 | < .01 |
| RSA Stress | -- | -- | -- | −.71 | .08 | < .01 |
| Racial Discrimination | −.01 | .09 | .88 | .02 | .05 | .71 |
| Public Regard | .03 | .07 | .63 | −.06 | .05 | .23 |
| Racial Discrimination X Public | .04 | .07 | .60 | .06 | .06 | .27 |
| Regard | ||||||
Notes. BMI = body mass index, RSA = respiratory sinus arrhythmia.
Figure 1.
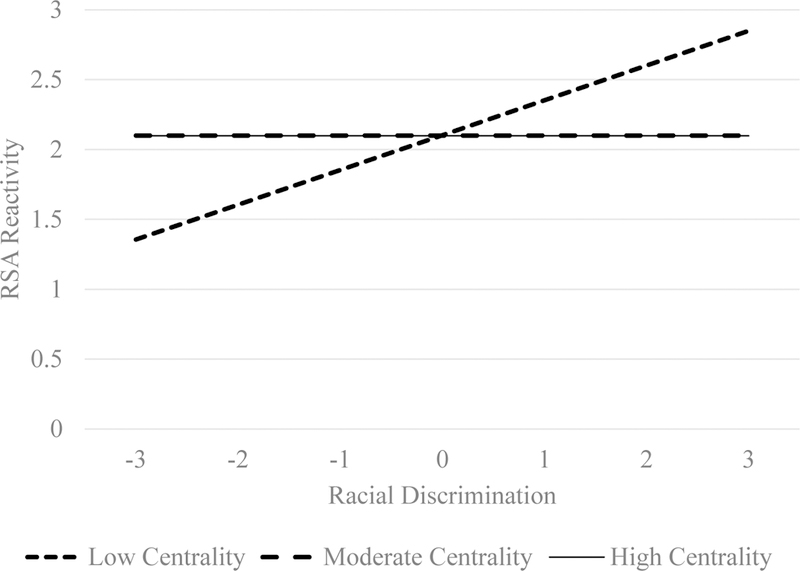
Moderation of Racial Discrimination and RSA Reactivity by Racial Centrality.
Note. RSA = respiratory sinus arrhythmia.
Racial Identity Dimensions and RSA Recovery
The interaction between RD and centrality (b = −.11) was associated with RSA recovery (see Table 3). In particular, more frequent RD was associated with augmentation in RSA recovery from stress to recovery at low levels of racial centrality (b = .19), but not at moderate and high levels of racial centrality (see Figure 2). The interactions between RD and private and public regard were nonsignificant.
Figure 2.
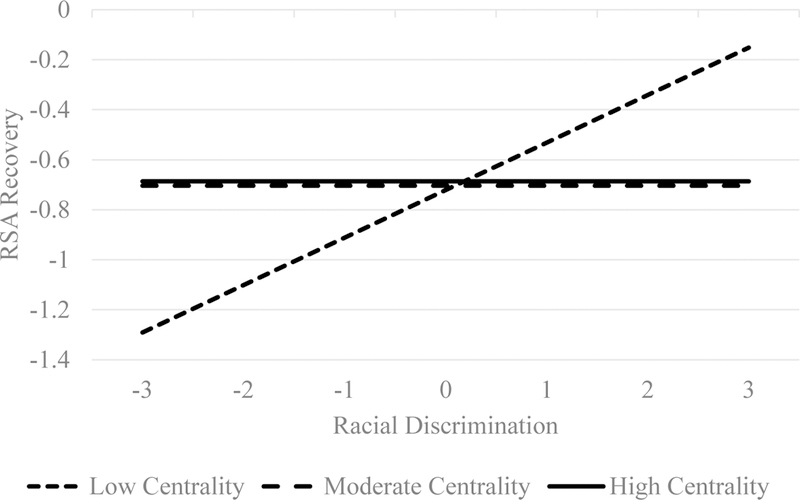
Moderation of Racial Discrimination and RSA Recovery by Racial Centrality.
Note. RSA = respiratory sinus arrhythmia.
Discussion
Contrary to our first hypothesis, RD was not associated with RSA reactivity or recovery. This was unexpected given that RD is found to produce dysregulated physiological systems (38). However, the few studies that link RD with acute PNS stress responses find that higher lifetime RD is associated with lower PNS activity at baseline (5) and withdrawal of PNS during experimental stress tasks (20). Our findings suggest that self-reporting frequency of RD during the past year may not be as predictive of RSA as lifetime RD, which future research should examine. Nevertheless, this study is one of the first to explore the connection between past year RD and RSA reactivity and recovery. Alternatively, one study found that only discrimination attributable to threat was a significant predictor of low HRV (5), indicating that certain aspects of RD may have differential effects on physiology. However, studies that find a significant association between RD and the PNS often only examine resting rates rather than reactivity and recovery. Perhaps we were unable to detect a significant association because a majority of participants reported infrequent experiences of racial discrimination, a consideration meriting further research. Finally, perhaps the association between RD and RSA variables is not direct but can be better understood within the context of racial identity (24).
Contrary to our hypotheses, only the dimension of racial centrality had a significant role in the association between RD and acute RSA reactivity and recovery. This is surprising given that Neblett and Roberts (24) found that both private regard and public regard were associated with RSA, while racial centrality was not. However, their study examined racial identity and physiology in tandem with situational factors (e.g., race of perpetrator, variation of task), which is different from our assessment of RD. Taken together, while we based our hypotheses on prior empirical results (24) future research is necessary to clarify the role of racial identity.
Lower racial centrality was found to be protective for both acute RSA reactivity and recovery, yet RD and RSA reactivity and recovery were not significantly associated at moderate or high levels of racial centrality. This contradicts the centrality hypothesis (39), which suggests that high racial centrality exacerbates psychological distress when experiencing RD. Yet support for this hypothesis is mixed (26, 40), previous research on the protective role of racial centrality is unclear, and few studies examine physiological outcomes. Young adulthood for Black students at a predominantly White institution is a time of increased risk of experiencing RD (4). Lower centrality may be associated with the perception that unfair treatment experienced is not race-related, as lower centrality individuals may be less likely to attribute much importance to race in their lives (23, 26, 40). Indeed, centrality was positively associated with racial discrimination in our sample. If a vignette of RD is not appraised as stressful for individuals with low racial centrality because they perceive the event as irrelevant, the RD vignette may be appraised as positive, reminding them that they are “not like other Black Americans” who would be especially affected by such an event. The current study did not examine appraisals, therefore future research should explore this possibility.
Several limitations of the present study should be noted. The analytic sample size was limited. Although we were able to detect effects, it is important that our findings are replicated. Our sample was predominantly female and sex was associated with racial identity and RSA reactivity, suggesting that future research should examine sex as a moderator. Due to the cross-sectional nature of the study, causation cannot be inferred from our results. Longitudinal research should examine how racial identity may protect Black young adults’ physiological responses from the deleterious effects of discrimination across time and examine other components of racial identity – salience and ideology. Due to the nature of the laboratory task in which vignettes were not manipulated, we cannot conclude whether responses to this task were equivalent to responses to in vivo experiences of RD 1) above and beyond another type of potentially stress-inducing task, and 2) outside the laboratory setting. However, results comparing RSA levels during baseline, stress, and recovery suggest that the task elicited a stress-related physiological response. The task was designed to elicit participant reactivity via the use of a White research assistant to deliver the vignette, and therefore the magnitude of participant reactivity may not be representative of reactivity to other experiences or situations. Fourth, in the Qualtrics survey, questions were not randomized and attention check items were not included. Although surveys were visually inspected for unusual data patterns, participants’ responses may have been impacted by order effects and/or inattentiveness.
Despite these limitations, this study has important implications for the health of Black young adults. The centrality of one’s racial identification may play an important role in shaping acute physiological responses to racism-related stress. While racial centrality is generally salutary, our study suggests that lower racial centrality can reduce risk in the context of RD. Thus, it is important for health professionals and college counseling centers to have an understanding of the racial identities of their Black young adult clients who attend predominantly White institutions. They should discuss, consider, and evaluate the impact of racial discrimination experiences in the context of the significance of race with their clients, which would allow them to tailor and individualize their strategies and interventions that aim to better equip Black young adults to thrive in the face of RD.
Our investigation begins to inform understandings of racial identity as resilience-promoting factors. If race centrality does serve as a protective factor for Black young adults in the context of the environmental demands of RD, it is imperative to examine the processes through which racial centrality is associated with situational characteristics of RD in the moment. Such an understanding can help health practitioners and researchers promote the resilience of Black young adults, such that we may work to reduce cardiovascular health disparities.
Acknowledgements:
This study was funded by a Basic Psychological Science Research Grant awarded to the PI (Vanessa V. Volpe) by the American Psychological Association and an Emerging Scholars Fellowship awarded to the PI (Vanessa V. Volpe) by the Steve Fund and Active Minds. The second author (Daniel B. Lee) was supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Development (NICHD) (T32 HD 79350-2).
List of abbreviations:
- RD
Racial discrimination
- ANS
Autonomic nervous system
- PNS
Parasympathetic nervous system
- HRV
Heart rate variability
- RSA
Respiratory sinus arrhythmia
- BMI
Body mass index
- RQ1
Research question 1
- RQ1a
Research question 1a
- RQ1b
Research question 1b
- RQ2
Research question 2
- RQ2a
Research question 2a
- RQ2b
Research Question 2b
- MIBI
Multidimensional Inventory of Black Identity
- FIML
Full information maximum likelihood
Appendix A
Only a subset of participants completed both parts of the study (n = 131; online survey, laboratory visit), whereas the remainder of the participants completed only the online survey (n = 103; no RSA data) as the laboratory portion was inaccessible due to a change in facilities in 2014. Among those who completed only the online survey, missing data ranged from .40% to 10.3% across study variables. Moreover, there were no differences between participants who completed the laboratory stress task and participants who only completed the online survey: sex (χ2 (1) = 3.81; p = .051), parental education (t (231) = .49, p = .622), public regard (t (220) = 1.46, p = .146), racial centrality (t (220) = −1.15, p = .252), BMI (t (123.72) = .67, p = .505), and chronic racial discrimination (t (227) = .47, p = .636). Although there was a difference in private regard between participants who completed the laboratory stress task (M = 6.34) versus participants who did not (M = 5.96; t (151.67) = −3.05, p = .003), the difference is not conceptually meaningful as both groups identically report high levels of private regard.
Appendix B
Vignette: It is the first day of class. The instructor asks you to exchange contact information and get to know the person sitting next to you. The person sitting next to you looks like me. After exchanging contact information, the person sitting next to you says, “Oh wow, you got into (college name)! So, are you actually really smart or did they just have to let a certain number of Black people in?”
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest: Authors report no conflicts of interest. The authors listed above wrote the first draft of the manuscript and no form of payment was given to any author to produce the manuscript.
Implications and Contribution:
This study finds that the less central race is to one’s self-concept, the more one is able to mitigate acute physiological responses when facing racial discrimination. Programs that help Black young adults cope with racism may thereby protect against cardiovascular risk.
References
- 1.Clark CJ, Alonso A, Spencer RA, Pencina M, Williams K, Everson-Rose SA. Predicted long-term cardiovascular risk among young adults in the national longitudinal study of adolescent health. Am J Public Health 2014;104:e108–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: findings from community studies. Am J Public Health 2003;93:200–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Williams DR, Mohammed SA. Discrimination and racial disparities in health: evidence and needed research. J Behav Med 2009;32:20–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hope EC, Hoggard LS, Thomas A. Emerging into adulthood in the face of racial discrimination: Physiological, psychological, and sociopolitical consequences for African American youth. Transl Issues Psychol Sci 2015;1:342–51. [Google Scholar]
- 5.Hill LK, Hoggard LS, Richmond SA, et al. Examining the association between perceived discrimination and heart rate variability in African Americans. Cultur Divers Ethnic Minor Psychol 2017;23:5–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Geronimus AT, Hicken M, Keene D, Bound J. “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. Am J Public Health 2006;5:826–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sellers RM, Smith MA, Shelton JN, et al. Multidimensional model of racial identity: A reconceptualization of African American racial identity. Pers Soc Psychol Rev 1998;1:18–39. [DOI] [PubMed] [Google Scholar]
- 8.Clark R, Anderson NB, Clark VR, Williams DR Racism as a stressor for African Americans: A biopsychosocial model. Am Psychol 1999:10, 805–816. [DOI] [PubMed] [Google Scholar]
- 9.McEwen BS, Stellar E. Stress and the individual: Mechanisms leading to disease. Arch Intern Med 1993;18:2093–101. [PubMed] [Google Scholar]
- 10.Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn Dis 1992;2:207–21. [PubMed] [Google Scholar]
- 11.Guyll M, Matthews KA, Bromberger JT. Discrimination and unfair treatment: Relationship to cardiovascular reactivity among African American and European American women. Health Psychol 2001;20:315–25. [DOI] [PubMed] [Google Scholar]
- 12.Smart Richman L, Bennett GG, Pek J, et al. Discrimination, dispositions, and cardiovascular responses to stress. Health Psychol 2007;26:675–83. [DOI] [PubMed] [Google Scholar]
- 13.Smart Richman L, Pek J, Pascoe E, Bauer DJ. The effects of perceived discrimination on ambulatory blood pressure and affective responses to interpersonal stress modeled over 24 hours. Health Psychol 2010;29:403–11. [DOI] [PubMed] [Google Scholar]
- 14.Appelhans MB, Luecken JL. Heart rate variability as an index of regulated emotional responding. Rev Gen Psychol 2006;10:229–40. [Google Scholar]
- 15.Porges SW. The polyvagal theory: new insights into adaptive reactions of the autonomic nervous system. Cleve Clin J Med 2009;76:S86–S90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Thayer JF, Lane RD. The role of vagal function in the risk for cardiovascular disease and mortality. Biol Psychol 2007;74:224–242. [DOI] [PubMed] [Google Scholar]
- 17.Mezzacappa ES, Kelsey RM, Katkin ES, Sloan RP. Vagal rebound and recovery from psychological stress. Psychosom Med 2001;63:650–7. [DOI] [PubMed] [Google Scholar]
- 18.Dorr N, Brosschot FJ, Sollers JJ, Thayer FJ. Damned if you do, damned if you don’t: The differential effect of expression and inhibition of anger on cardiovascular recovery in Black and White males. Int J Psychophysiol 2007;66:125–34. [DOI] [PubMed] [Google Scholar]
- 19.Wagner AJ, Lambert R, Tennen H, Feinn R. Exposure to discrimination and heart rate variability reactivity to acute stress among women with diabetes. Stress Health 2015;31:255–62. [DOI] [PubMed] [Google Scholar]
- 20.Arnett JJ, Brody HG. A fraught passage: The identity challenges of African American young adults. Hum Dev 2008;51:291–3. [Google Scholar]
- 21.Hoggard LS, Jones SCT, Sellers RM. Race cues and racial identity: Implications for how African Americans experience and respond to racial discrimination. J Black Psychol 2016;43:409–32. [Google Scholar]
- 22.Jones SC, Neblett EW Jr. Future directions in research on racism-related stress and racial-ethnic protective factors for Black youth. J Clin Child Adolesc Psychol 2017;46:1–13. [DOI] [PubMed] [Google Scholar]
- 23.Sellers R, Caldwell CH, Schmeelk-Cone KH, Zimmerman MA. Racial identity, racial discrimination, perceived stress and psychological distress among African American young adults. J Health Soc Behav 2003;3:302–17. [PubMed] [Google Scholar]
- 24.Neblett EW Jr, Roberts OS. Racial identity and autonomic responses to racial discrimination. Psychophysiology 2013;10:943–53. [DOI] [PubMed] [Google Scholar]
- 25.Sellers RM, Copeland-Linder N, Martin PP, Lewis RH. Racial identity matters: The relationship between racial discrimination and psychological functioning in African American adolescents. J Adolesc Red 2006;2:187–216. [Google Scholar]
- 26.Sellers RM, Shelton JN. The role of racial identity in perceived racial discrimination. J Pers Soc Psychol 2003;5:1079–92. [DOI] [PubMed] [Google Scholar]
- 27.Neblett EW Jr, Shelton JN, Sellers RM. The role of racial identity in managing daily racial hassles. In: Philogene G ed. Racial identity in context: The legacy of Kenneth B. Clark Washington, DC: American Psychology Association, 2004:77–90. [Google Scholar]
- 28.Umetani K, Singer DH, McCraty R, Atkinson M. Twenty-four hour time domain heart rate variability and heart rate: relations to age and gender over nine decades. J Am Coll Cardiol 1998;31:593–601. [DOI] [PubMed] [Google Scholar]
- 29.Koenig J, Thayer JF. Sex difference in healthy human heart rate variability: A meta-analysis. Neurosci Biobehav Rev 2016;64:288–310. [DOI] [PubMed] [Google Scholar]
- 30.Tonhajzerova I, Javorka M, Trunkvalterova Z, et al. Cardio-respiratory interaction and autonomic dysfunction in obesity. J Physiol Pharmacol 2008;59(Suppl 6):709–18. [PubMed] [Google Scholar]
- 31.Williams DR, Priest N, Anderson NB. Understanding associations among race, socioeconomic status, and health: Patterns and prospects. Health Psychol 2016;4:407–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Harrell SP, Merchant MA, Young SA. Psychometric properties of the racism and life experiences scales (RaLES) Annual convention of the American Psychological Association, Chicago, IL: 1997. [Google Scholar]
- 33.Sellers RM, Rowley SA, Chavous TM, et al. The Multidimensional Inventory of Black Identity: A preliminary investigation of reliability and construct validity. J Pers Soc Psychol 1997;73:805–815. [Google Scholar]
- 34.Lewis GF, Furman SA, McCool MF, Porges SW. Statistical strategies to quantify respiratory sinus arrhythmia: Are commonly used metrics equivalent?. Biol Psychol 2012;89:349–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fries-Britt S, Griffin K. The Black box: How high-achieving Blacks resist stereotypes about Black Americans. J Coll Stud Dev 2007;5:509–24. [Google Scholar]
- 36.Solorzano D, Ceja M, Yosso T. Critical race theory, racial microaggressions, and campus racial climate: The experiences of African American college students. J Negro Educ 2000;69:60–73. [Google Scholar]
- 37.Muthén LK, Muthén BO. Mplus version 8 Los Angeles, CA: Muthén & Muthén; 2017. [Google Scholar]
- 38.Lampert R, Ickovics J, Horwitz R, Lee F. Depressed autonomic nervous system function in African Americans and individuals of lower social class: A potential mechanism of race- and class-related disparities in health outcomes. Am Heart J 2005;150:153–160. [DOI] [PubMed] [Google Scholar]
- 39.Yip T, Gee GC, Takeuchi DT. Racial discrimination and psychological distress: The impact of ethnic identity and age among immigrant and United States-born Asian adults. Dev Psychol 2008;44:787–800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Burrow AL, Ong AD. Racial identity as a moderator of daily exposure and reactivity to racial discrimination. Self Identity 2010;9:383–402. [Google Scholar]