

Sir,
A 73-year-old male was referred to our department during admission in the gastroenterology department to receive sorafenib therapy for hepatocellular carcinoma with metastasis to the peritoneal lymph nodes. He had suffered from plaque-type psoriasis for over 30 years, and had been treated with topical corticosteroids and vitamin D3 ointment for psoriasis, without episodes of pustulation. Physical examination revealed multiple scaly erythematous plaques on the trunk, upper and lower limbs, and scalp. Oral administration of 400 mg/day sorafenib (Nexavar®, Bayer Co., Germany) was started. One week later, he developed pyrexia of 38°C and stomachache, and laboratory examination showed an increased level of C-reactive protein (7.03 mg/dl). After one week, his psoriatic lesions exacerbated with itching, and multiple pustules appeared on and around the psoriatic plaques [Figures 1a and b]. Laboratory examination showed an elevated ratio of eosinophils (10%). A biopsy specimen from the scaly erythema showed hyperproliferative epidermis with parakeratosis and neutrophil accumulation in the corneal layers [Figure 1c]. Another biopsy specimen from the pustular lesion showed a subcorneal spongiform abscess in the upper epidermis [Figure 1d]. Furthermore, eosinophils were scattered in the upper dermis, which were positively stained by Congo-red [Figure 1e]. After stopping sorafenib, the pustules rapidly disappeared; however, the scaly erythemas spread on the back. The patient was treated with topical corticosteroids thereafter.
Figure 1.
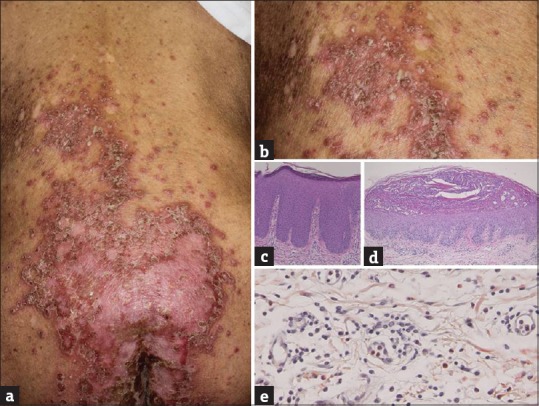
(a) Deterioration of psoriasis (b) with multiple pustules. (c) Histopathological findings showed regular epidermal proliferation with parakeratosis (H and E, ×100), (d) a subcorneal neutrophilic abscess (H and E, ×40) and (e) infiltration of eosinophils in the upper dermis (Congo-red, ×400)
Several cases have been reported in which tyrosine kinase inhibitors were effective for psoriasis. Sorafenib, which is used for unresectable hepatocellular carcinoma, is a multikinase inhibitor that targets vascular endothelial growth factor (VEGF) receptors 1–3, platelet-derived growth factor receptor-α and -β, c-Kit, Flt-3, colony-stimulating factor receptor 1, and glial cell line-derived neurotrophic factor receptor. VEGF is one of the key molecules that plays an important role in the pathogenesis of psoriasis, and inhibition of VEGF signaling may result in beneficial effect for psoriasis. By contrast, there are several reports demonstrating adverse effects of sorafenib which either induced a new onset of psoriasis or exacerbated preexisting psoriasis.[1] In the previous reports, all patients were male, and skin lesions appeared some days to 9 months after the treatment with sorafenib 200 mg to 800 mg daily. Among the cases that developed pustular lesions with preexisting psoriasis,[2,3,4] the severity varied. In certain cases, complete blockade of VEGF signaling pathways may also induce adverse reactions, and even worsen psoriasis, due to inflammatory and immune feedback reactions. It is suggested that sorafenib reduces the number, as well as the function, of regulatory T cells and effector T cells by blocking the signal transduction pathways.[1] Alternatively, sorafenib upregulates hypoxia-inducible factor (HIF)-2α by HIF-1α inhibition.[5] HIF-2α activates the transforming growth factor-α/epidermal growth factor receptor pathway,[5] leading to epidermal hyperproliferation and inflammation. Furthermore, like HIF-1α, HIF-2α induces many angiogenesis-related genes, which may play a role in the psoriasis induction or worsening. Psoriasis may be exacerbated with pustulation by administration of sorafenib.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Yiu ZZ, Ali FR, Griffiths CE. Paradoxical exacerbation of chronic plaque psoriasis by sorafenib. Clin Exp Dermatol. 2016;41:407–9. doi: 10.1111/ced.12788. [DOI] [PubMed] [Google Scholar]
- 2.Laquer V, Saedi N, Dann F, Kelly K. Sorafenib-associated psoriasiform skin changes. Cutis. 2010;85:301–2. [PubMed] [Google Scholar]
- 3.Maki N, Komine M, Takatsuka Y, Maekawa T, Murata S, Ohtsuki M, et al. Pustular eruption induced by sorafenib in a case of psoriasis vulgaris. J Dermatol. 2013;40:299–300. doi: 10.1111/1346-8138.12097. [DOI] [PubMed] [Google Scholar]
- 4.Du-Thanh A, Girard C, Pageaux GP, Guillot B, Dereure O. Sorafenib-induced annular pustular psoriasis (Milian-Katchoura type) Eur J Dermatol. 2013;23:900–1. doi: 10.1684/ejd.2013.2184. [DOI] [PubMed] [Google Scholar]
- 5.Zhao D, Zhai B, He C, Tan G, Jiang X, Pan S, et al. Upregulation of HIF-2α induced by sorafenib contributes to the resistance by activating the TGF-α/EGFR pathway in hepatocellular carcinoma cells. Cell Signal. 2014;26:1030–9. doi: 10.1016/j.cellsig.2014.01.026. [DOI] [PubMed] [Google Scholar]