

Abstract
Objective
The aim of this study was to evaluate the dentoalveolar and dentofacial effects of a mini-screw-anchored pendulum appliance in maxillary molar distalization.
Methods
Twenty patients with the Angle Class II molar relationship (mean age 14.05±2.4 years) were treated with a mini-screw-anchored pendulum appliance for molar distalization. A mini-screw 1.9 mm in diameter and 9 mm in length was used to support the pendulum appliance. The springs of the pendulum appliance were activated at 90° and exerted 250–300 gr force per side. Lateral cephalometric radiographs and dental cast models were obtained from all the patients before and after maxillary molar distalization.
Results
A 0.6° increase in the SNA and SNB angles, and a 0.3° decrease in the SN/GoGn angle were found to be statistically significant. In the maxillary first molars, 4.2-mm significant distalization, 0.6-mm significant intrusion, and 8.9° significant distal tipping were observed. The spontaneous distal drift of the maxillary second premolars was found to be statistically significant. In the maxillary first premolar and incisor positions, significant mesialization was observed; however, the changes in the angles of these teeth were found to be insignificant.
Conclusion
A mini-screw-anchored pendulum appliance is an effective method for maxillary molar distalization that controls the undesired anchorage loss observed in conventional methods.
Keywords: Class II, orthodontic anchorage, orthodontic appliance
INTRODUCTION
Since Kingsley (1) and Angle (2) introduced the headgears as an extra-oral appliance for orthopedic and/or dentoalveolar correction of Class II malocclusions in the late 1800s, these appliances have been used widely for distalization of maxillary molars. Patient cooperation has been the major concern of these extra-oral appliances; therefore, clinicians have investigated several intraoral molar distalization systems for correction of the dentoalveolar Class II malocclusions (3–6).
The pendulum appliance has been used as a fixed intraoral molar distalization device ever since it was introduced by Hilgers et al. (6) in 1992. Conventional pendulum anchors from the palatal tissue and upper premolars during the distalization of maxillary molars. The main disadvantage of this appliance is mesialization of the premolars and proclination of the incisors due to the reciprocal anchorage (6–8).
Since skeletal anchorage devices were introduced, they have been used for eliminating the loss of anchorage during orthodontic treatments (9–11). For this purpose, mini-screws have been widely used because of their easy insertion with non-surgical procedures and loading immediately after insertion (9, 11–13).
In the literature, mini-screw-anchored pendulum appliance studies have reported the use of one or two mini-screws without dental anchorage in the treatment of Class II malocclusions (9–11, 14). However, the authors, who used only one mini-screw, suggested the use of two mini-screws because of the mini-screw failure (10, 11). The aim of the present study was to evaluate dentoalveolar and dentofacial effects of a pendulum appliance with two occlusal rests on the maxillary first premolars and one mini-screw anchorage in the maxillary molar distalization.
METHODS
The sample size of the present study was estimated using the G*Power Software (v3.1.3; Franz Faul, Universität Kiel, Germany), and a total sample of 20 was required for a power of 95% confidence at the 0.05 significance level. Therefore, 20 patients were included in the present study from the Orthodontic Department of Orthodontics, Gazi University School of Dentistry.
The patients who fulfilled the following inclusion criteria were included in the study: (1) the ANB angle between 0° and 5°, (2) decreased or optimum vertical facial growth pattern (SN/GoGn≤38°), (3) Angle Class II malocclusion with at least 4 mm Class II molar relationship, (4) a minimal crowding in the mandibular arch (≤2 mm) and a moderate crowding in the maxillary arch (≤5 mm), (5) fully erupted maxillary second molars, and (6) no craniofacial anomalies or previous orthodontic treatment. All the patients and parents were informed about the orthodontic procedures throughout the study and signed an informed consent form. The study was approved by the Gazi University Ethics Committee (23.06.2014/321).
The study group comprised 13 females and 7 males (mean chronological age 14.05±2.4 years) and treated using the mini-screw anchored pendulum appliance for molar distalization.
Treatment Protocol
Before treatment, all the patients were examined to evaluate the presence and position of the maxillary third molar. Two of the patients had extracted their maxillary third molars previously; two of them had no third molar germs. Seven patients had third molars below the trifurcation line of second molars, and to achieve less resistance during distalization, these teeth were extracted. Nine of the patients had third molars above the trifurcation line of second molars, and they were not expected to affect the distalization; therefore, these teeth were not extracted.
The mini-screws (Spider screw, HDC Company, Sarcedo, Italy) used in the present study are self-drill screws and are 1.9 mm in diameter and 9 mm in length. The mini-screws were placed in the paramedian area of the anterior palate under local anesthesia, approximately 4–5 mm posterior to the incisive papilla and 4–5 mm lateral to the median palatal suture (Figure 1a). Following the insertion of the mini-screw, maxillary first molars were banded, and a plaster model was obtained. A pendulum appliance with a Nance button on the palatal surface, two occlusal rests on maxillary first premolars, and two springs from the Nance button to the sheets of molar bands were constructed on the plaster models. The acrylic part of the Nance appliance corresponding to the area of the mini screw was removed.
Figure 1. a–c.

Placement of the mini-screw, activation of springs, and intraoral view of the pendulum appliance
After the appliance, adaptation was clinically checked, and occlusal rests were bonded to the first premolars to maintain the stability of the appliance. The appliance was connected and fixed to the mini-screw with the help of cold-curing methyl methacrylate free acrylic resin (Ufi Gel Hard; Voco GmbH, Cuxhaven, Germany). The springs were activated at 90° for approximately 250 gr of distalization force and inserted into the sheets of maxillary first molar bands (Figure 1b, c).
The patients were examined every 4 weeks, and the activation of the springs was checked during these appointments. Reactivation was performed when needed. The distalization was continued until the Angle Class I molar relationship was achieved in all the patients, and then the pendulum appliance was removed (Figure 2, 3). The Nance button as a reinforcement appliance was fixed using the same protocol as that used for the mini screw.
Figure 2.

Intraoral images of a patient before distalization
Figure 3.

Intraoral images of a patient after distalization
Lateral cephalograms and dental cast models were taken before the mini-screw insertion (T0) and after the Angle Class I molar relationship was achieved (T1). All cephalometric radiographs were traced and superimposed by the same operator. A local superimposition was done on the best fit of the palatal curvature and maxillary trabecular structures to evaluate the maxillary dentoalveolar changes by treatment. The maxillary horizontal reference plane (x) was drawn along the ANS-PNS plane and the maxillary vertical reference plane (y) was perpendicular to the ANS-PNS plane at the PNS point. Thirteen angular and 14 linear measurements were evaluated on each lateral cephalometric radiograph (Figure 4, 5). The dental cast models were scanned using a 3D scanner (3Shape, Copenhagen, Denmark), and digital cast models were obtained. The model analyses were done using the 3Shape OrthoAnalyzer™ (3Shape A/S) program, and two angular and two linear measurements were evaluated on each digital cast models (Figure 6).
Figure 4.
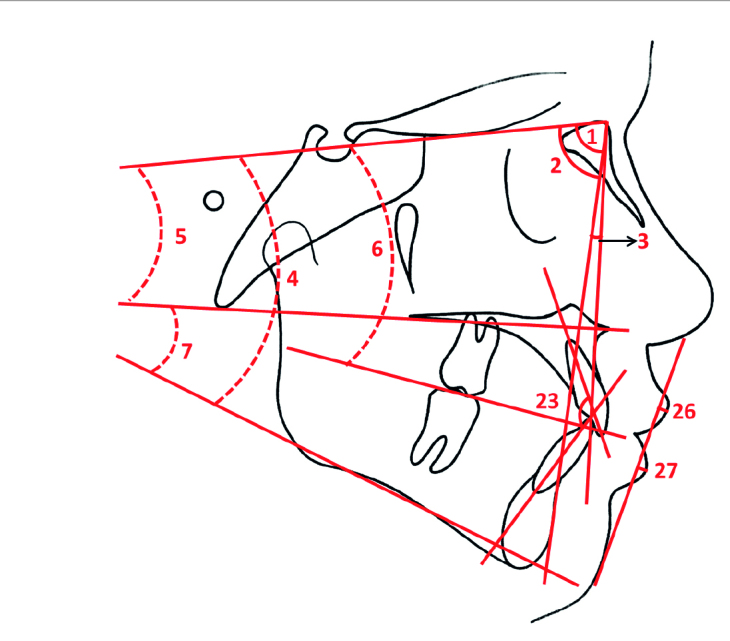
Cephalometric measurements evaluated in the present study: 1, SNA; 2, SNB; 3, ANB; 4, SN/GoGn; 5, SN/ANS-PNS; 6, SN/OP; 7, ANS-PNS/GoMe; 23, U1/L1; 26, UL-S Line; 27, LL-S Line
Figure 5.
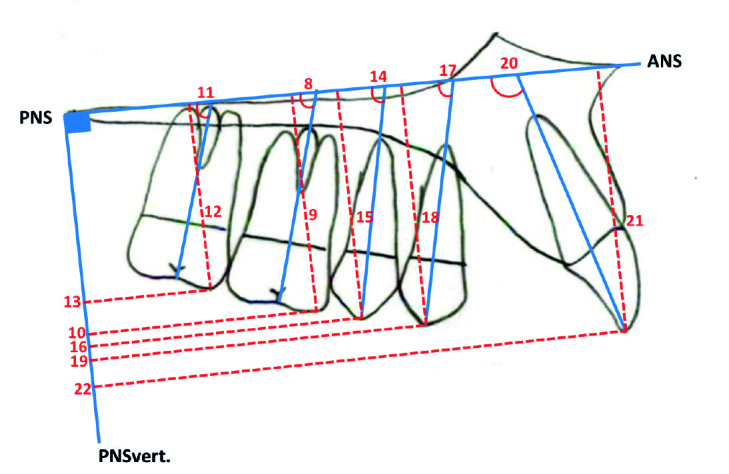
Maxillary dentoalveolar cephalometric measurements evaluated in the present study: 8, U6/ANS-PNS; 9, U6-ANS-PNS; 10, U6-PNS vert.; 11, U7/ANS-PNS; 12, U7-ANS-PNS; 13, U7-PNS vert.; 14, U5/ANS-PNS; 15, U5-ANS-PNS; 16, U5-PNS vert.; 17, U4/ANS-PNS; 18, U4-ANS-PNS; 19, U4-PNS vert.; 20, U1/ANS-PNS; 21, U1-ANS-PNS; 22, U1-PNS vert
Figure 6.
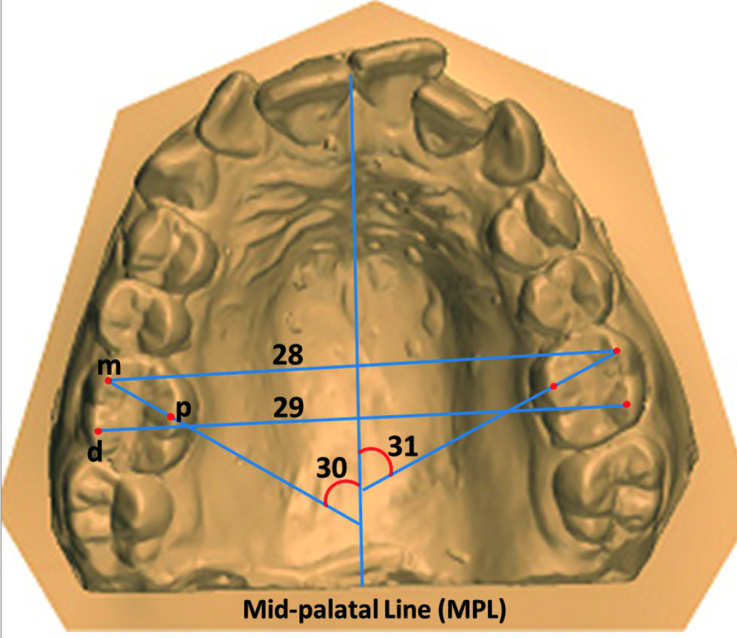
Maxillary dental cast model measurements evaluated in the present study: 28, UL6 m-UR6 m; 29, UL6d-UL6d; 30, UL6 mp/MPL; 31, UR6 mp/MPL (m, mesiobuccal cusp; d, distobuccal cusp; p, palatal cusp)
Statistical Analysis
The data obtained from the subjects were evaluated using the Statistical Package for Social Sciences version 20 (IBM Corp.; Armonk, NY, USA). Descriptive statistics were calculated for age, duration of treatment, and cephalometric measurements at T0 and T1. The normality of the distribution of the variables was examined using the Shapiro-Wilk test. Changes during the treatment were analyzed using the paired t-test for normally distributed variables and the Wilcoxon test for not normally distributed variables. p<0.05, p<0.01, and p<0.001 were considered statistically significant.
RESULTS
Table 1 represents the initial age, cephalometric and dental cast measurements of the patients, and the changes of these variables with the treatment.
Table 1.
Changes in age and cephalometric and dental cast measurements
| PARAMETER | Pre-treatment | Post-treatment | Treatment Difference | |||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|
||||||
| N | Mean | SD | Mean | SD | Mean | SD | p | |
| Age (years) | 20 | 14.05 | 2.4 | 14.75 | 2.3 | 0.7 | 0.3 | |
| SNA (°) | 20 | 78.7 | 3.7 | 79.3 | 3.6 | 0.6 | 0.8 | 0.003 ** |
| SNB (°) | 20 | 75.8 | 3.5 | 76.4 | 3.7 | 0.6 | 0.8 | 0.004 ** |
| ANB (°) | 20 | 2.9 | 1.4 | 3 | 1.5 | 0.1 | 0.5 | 0.666 NS |
| SN/GoGn (°) | 20 | 33.3 | 3.6 | 33 | 3.6 | −0.3 | 0.6 | 0.033 * |
| SN/ANS-PNS (°) | 20 | 9.8 | 3.5 | 9.9 | 3.4 | 0.1 | 1 | 0.832 NS |
| SN/OP (°) | 20 | 16.6 | 3.5 | 16.7 | 3.1 | 0.1 | 1.4 | 0.746 NS |
| ANS-PNS/GoMe (°) | 20 | 26.1 | 4 | 25.7 | 3.9 | −0.4 | 0.9 | 0.120 NS |
| U6/ANS-PNS (°) | 20 | 81.6 | 5.9 | 72.7 | 6.4 | −8.9 | 3.1 | 0.001 *** |
| U6-ANS-PNS (mm) | 20 | 24.9 | 2.8 | 24.3 | 2.9 | −0.6 | 1 | 0.019 * |
| U6-PNS vertical (mm) | 20 | 22.2 | 2.9 | 18 | 3.1 | −4.2 | 0.8 | 0.001 *** |
| U7/ANS-PNS (°) | 20 | 66.6 | 4.8 | 58.3 | 4.2 | −8.3 | −11 | 0.001 *** |
| U7-ANS-PNS (mm) | 20 | 18.5 | 4.2 | 18.1 | 4.3 | −0.4 | 0.7 | 0.010 * |
| U7-PNS vertical (mm) | 20 | 9.3 | 3.6 | 5.8 | 3.5 | −3.5 | 0.9 | 0.001 *** |
| U5/ANS-PNS (°) | 20 | 83.2 | 3.9 | 79.8 | 3.9 | −3.4 | 1.6 | 0.001 *** |
| U5-ANS-PNS (mm) | 20 | 25.9 | 2.9 | 26 | 2.8 | 0.1 | 0.5 | 0.287 NS |
| U5-PNS vertical (mm) | 20 | 28.1 | 3.8 | 26 | 3.8 | −2.1 | 0.6 | 0.001 *** |
| U4/ANS-PNS (°) | 20 | 91.6 | 5 | 90.8 | 5.2 | −0.8 | 1.7 | 0.066 NS |
| U4-ANS-PNS (mm) | 20 | 27.5 | 2.6 | 27.1 | 2.9 | −0.4 | 0.7 | 0.008 ** |
| U4-PNS vertical (mm) | 20 | 36.7 | 4.1 | 37.1 | 4.2 | 0.4 | 0.8 | 0.020 * |
| U1/ANS-PNS (°) | 20 | 110.1 | 5.7 | 110.4 | 6.5 | 0.3 | 1.6 | 0.444 NS |
| U1-ANS-PNS (mm) | 20 | 30.2 | 2.7 | 30.5 | 2.8 | 0.3 | 0.8 | 0.097 NS |
| U1-PNS vertical (mm) | 20 | 54.4 | 3.5 | 55 | 3.5 | 0.6 | 0.7 | 0.002 ** |
| U1/L1 (°) | 20 | 128.3 | 9 | 127.9 | 9.9 | −0.4 | 2.9 | 0.540 NS |
| Overjet (mm) | 20 | 3.5 | 2.2 | 3.6 | 2 | 0.1 | 0.6 | 0.172 NS |
| Overbite (mm) | 20 | 3 | 1.4 | 3.3 | 1.4 | 0.3 | 0.9 | 0.465 NS |
| UL-S line (mm) | 20 | −0.8 | 2.1 | −0.9 | 2 | −0.1 | 1.1 | 0.759 NS |
| LL-S line (mm) | 20 | −0.2 | 2.6 | −0.1 | 2.5 | 0.1 | 1 | 0.359 NS |
| UL6 m-UR6 m (mm) | 20 | 50 | 3.3 | 52.3 | 2.7 | 2.3 | 1,2 | 0.001 *** |
| UL6d-UR6d (mm) | 20 | 53.5 | 3.3 | 55.8 | 3.2 | 2.3 | 1 | 0.001 *** |
| UL6 mp/MPL (°) | 20 | 50.7 | 6.8 | 50.1 | 5.1 | −0.6 | 5.7 | 0.659 NS |
| UR6 mp/MPL (°) | 20 | 53.1 | 6.5 | 52.6 | 5 | −0.5 | 5.6 | 0.693 NS |
p<0.05*; p<0.01**; p<0.001***; NS: nonsignificant
m: mesiobuccal cusp; d: distobuccal cusp; p: palatal cusp; MPL: midpalatal line
The 0.7° increase in the SNA angle and 0.6° increase in the SNB angle was found to be statistically significant (p<0.01). The 0.3° anterior rotation of the mandible (SN/GoGn) was statistically significant (p<0.05).
In the upper first molars, a 4.2 mm significant distalization (p<0.001), 0.6 mm significant intrusion (p<0.05), and 8.9° significant distal tipping (p<0.001) were observed with treatment. Moreover, in the upper second molars, a 3.5 mm significant distalization (p<0.001), 0.5 mm significant intrusion (p<0.05), and 8.3° significant distal tipping (p<0.001) were achieved.
A 2.2 mm significant decrease in the sagittal position of the upper second premolar (p<0.001) and the 3.4° decrease in the U5/ANS-PNS angle were found to be statistically significant (p<0.001).
The vertical position of the upper first premolar was found to be significantly decreased by 0.5 mm (p<0.01) and the sagittal position of the upper first premolar was found to be significantly increased by 0.4 mm (p<0.05). However, the 0.8° decrease in the U4/ANS-PNS angle was found to be insignificant.
The changes in the upper incisor angle (U1/ANS-PNS) and upper incisor vertical position (U1-ANS-PNS) were found to be insignificant. The sagittal position of the upper incisors (U1-PNSvert) significantly increased (p<0.01).
The changes in the overjet and interincisal angle were found to be insignificant; however, the overbite significantly increased (p<0.05).
In the dental cast measurements, the distance between the mesiobuccal and distobuccal cusps of the upper first molars significantly increased by 2.4 mm and 3.3 mm, respectively (p<0.001). Insignificant mesiopalatal rotations in the upper first molars were observed after the treatment.
DISCUSSION
In skeletal Class I cases with mesialized maxillary molars or mild to moderate skeletal Class II cases, pendulum has been used with less patient cooperation for maxillary molar distalization (7, 8, 14–16). However, the main disadvantage of this appliance is mesialization of anchorage teeth (6–8, 14–16). Many studies demonstrated that mini-screw supported pendulum appliances provide rigid anchorage during maxillary molar distalization. In the mentioned studies, usually two mini-screws were used to increase the anchorage of the pendulum appliance (9–11, 17–19). Some authors used only one mini-screw; however, they suggested the use of two mini-screws to prevent the mini-screw failure (10, 11). In the present study, the pendulum appliance was supported with one mini-screw to avoid the anchorage loss, and the appliance was fixed to maxillary first premolars with two occlusal clasps to eliminate the failure of the mini-screw; therefore, mobility or loss of mini-screws was not observed during the distalization period.
In the orthodontic literature, it was reported that the anterior palatal plate has sufficient bone thickness for mini-screw insertion (13, 20, 21). Some authors suggested paramedian palatal suture as a safe zone for mini-screw insertion in the adolescents (22–24) because of the growth pattern of maxilla, whereas some others reported any objection about the median palatal suture for the mini-screws (12, 20). In the present study, all the subjects were adolescents and young adults, and the mini-screws were inserted into the paramedian palatal suture.
The length of the mini-screw is one of the important factors during insertion into the anterior palatal area. The shorter mini-screws decrease the stability of the mini-screw; however, the longer mini-screws might damage the roots of the teeth, incisive canal, or nasal cavity (20, 25). In the literature, the length of the mini-screw inserted into the palatal area range between 8 and 14 mm (10, 13, 19, 22, 23). Nienkemper et al. (20) reported similar and satisfying stability results with the mini-screws that were 9 mm and 11 mm in length. Considering the previous studies, the mini-screws that are 9 mm in length were used in the present study.
In the mini-screw-anchored pendulum appliance studies, it was reported that 200–250 gr force could be obtained with the 60° or 90° activation of springs, and the average distalization period ranged between 6.8 and 8.2 months (9–11, 19). In the present study, an average of 250 gr force was applied with the 90° activation of the pendulum springs, and the mean distalization period was found to be 8.4 months.
The significant increase in the SNA angle was found to be statistically significant (p<0.05). Kırcelli et al. (10) reported that a remodeling at the point A might be induced by the pressure of the acrylic Nance part of the bone-anchored pendulum appliance during maxillary molar distalization.
In the mandible, the anterior rotation was observed with a 0.6° significant increase in the SNB angle (p<0.01) and a 0.3° significant decrease in the SN/GoGn angle (p<0.05). This slight anterior rotation was because of the significant intrusion on the maxillary molars with the mini-screw-supported pendulum appliance. Escobar et al. (9) reported posterior rotation in the mandibular plane with bone-supported pendulum because of the inclination and rotation of the molars that create premature contacts with a tendency to open the bite.
In the maxillary first molars, a 4.2±0.8 mm distal movement and 8.9±3.1° distal tipping were found to be statistically significant (p<0.001). In the previous skeletally anchored pendulum studies, the distal movement of the maxillary first molars was reported to range between 2.9 mm and 6.4 mm, and distal tipping was reported between 8.8° and 11.3° in line with the results of the present study (9–11, 18, 19). Byloff and Darendeliler (8) demonstrated 10°–15° uprighting bends on the pendulum springs to prevent the tipping and achieve more bodily distal movement of the maxillary first molars; however, in the present study, a complete bodily distal movement could not be achieved despite performing the uprighting bends as reported by the authors.
On the maxillary second molars, a 3.5 mm significant distal movement (p<0.001) and 8.3° significant distal tipping (p<0.001) were observed after distalization. Kinzinger et al. (26) reported that the tipping of the maxillary first molar was much greater when the second molar was still at the budding stage. Similarly, if the maxillary third molar was still in the budding stage, tipping of the erupted second molar was greater. Therefore, the author suggested the germectomy of the third molars to achieve a more bodily distalization of both molars. In the present study, if the maxillary third molars were above the trifurcation line of the second molars, they were extracted before the treatment to provide less resistance during distalization.
Maxillary first and second molars were intruded significantly with 0.6 mm and 0.5 mm, respectively (p<0.05). When the ANS-PNS line was used as the reference line to determine the vertical changes of maxillary molars, because of the significant distal tipping of these teeth after distalization using the pendulum appliance, the crowns repositioned closer to the reference line, and this was interpreted as intrusion, which was previously mentioned by Byloff and Darendeliler (8). The authors also associated the intrusion with the prevention of dentoalveolar vertical growth by the rigid bonded appliance, intrusive force of tongue, and the design of the TMA loops of the appliance. Contrary to these findings, Kırcelli et al. (10) reported insignificant vertical changes in maxillary first molars with bone-anchored pendulum appliance.
The maxillary first and second premolars were used as the anchorage unit with conventional pendulum appliances. Therefore, the reciprocal effects of distalization force result with the mesialization of maxillary premolars (6–8, 15, 16). The previous studies reported a 1.4–2.55 mm mesial movement with 1.29°–4.84° mesial tipping using conventional pendulum appliances (7, 8, 15, 16). During the distalization of maxillary molars, to overcome this side effect and to achieve a spontaneous distal drifting on the maxillary premolars, clinicians supported the pendulum appliance with skeletal anchorage devices. Several of them excluded all the premolars from the anchorage unit (9, 10, 17, 18, 27, 28), whereas others excluded only the second premolars (22, 27, 29). In the present study, only the first premolars were included in the anchorage unit with two occlusal rests. Therefore, a 0.4 mm significant mesialization (p<0.05) and a 0.5 mm significant intrusion (p<0.01) of maxillary first premolars were observed. The second premolars, not included in the anchorage unit, were observed to be significantly drifted with a 2.2 mm distal movement and 3.4° distal tipping (p<0.05) because of the tensile strength of the trans-septal fibers between the maxillary first molars and second premolars.
Proclination of the maxillary incisors is one of the most observed side effect in conventional pendulum appliances studies (7, 8, 15). Also, Kinzinger et al. (22), Gelgor et al. (30), and Oncag et al. (28) reported maxillary incisor proclination with skeletal anchored molar distalization. In the present study, a significant increase in the sagittal position of maxillary incisors was observed; however, the increase in the U1/ANS-PNS angle was found to be insignificant. The sagittal position of incisors was measured between the incisal edge of the most labial incisor and the PNS-vertical line; therefore, the posterior growth on the PNS point could be affecting this distance.
Kırcelli et al. (10) reported a significant increase in the intermolar distance and insignificant molar rotation after maxillary molar distalization with bone-anchored pendulum appliance. In line with these findings, the intermolar distance significantly increased, and insignificant molar rotations in the upper first molars were observed in the present study. The significant increase of intermolar distance demonstrated an expansive force of pendulum springs during distalization. Beside the distalization and expansion forces, the pendulum springs exert two different rotation forces on the maxillary first molars. When the maxillary first molars undergo any rotations before distalization, the rotation force of springs is in the mesiopalatal direction; however, whether the maxillary first molars have a mesiopalatal rotation because of the early loss of deciduous second molars the springs apply a de-rotation force in the disto-palatal direction. In the present study, some of the patients had rotated maxillary first molars at the beginning of distalization and de-rotated using the pendulum springs; therefore, the maxillary first molar rotations remained at an insignificant level.
CONCLUSION
In this study, we aimed to evaluate the dentialveolar and dentofacial effects of a pendulum appliance using two occlusal rests on maxillary first premolars and one mini-screw anchorage in the maxillary molar distalization. The following results were obtained:
Maxillary first and second molar distalization was achieved with spontaneous second premolar distalization.
Mesialization of anchorage unit was controlled successfully with the mini-screw support.
Mandible showed anterior rotation with a significant increase in the SNB angle and a significant decrease in the SN/GoGn angle due to the significant intrusion of maxillary first molars.
Footnotes
Ethics Committee Approval: Ethics committee approval was received for this study from the Gazi University Ethics Committee (23.06.2014/321).
Informed Consent: Written informed consent was obtained from the volunteers who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - M.K., A.S.Y.; Design - M.K., A.S.Y.; Supervision - M.K., A.S.Y.; Data Collection and/or Processing - M.K., A.S.Y.; Analysis and/or Interpretation - M.K., A.S.Y.; Writing Manuscript - M.K., A.S.Y.; Critical Reviews - M.K., A.S.Y.
Conflict of Interest: The authors have no conflict of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Kingsley N. Treatise on Oral Deformities as a Branch of Medical Surgery. New York: D Appleton; 1980. pp. 131–4. [Google Scholar]
- 2.Angle EH. Classification of malocclusion. Dental Cosmos. 1899;41:248–64. [Google Scholar]
- 3.Keles A. Maxillary unilateral molar distalization with sliding mechanics: a preliminary investigation. Eur J Orthod. 2001;23:507–15. doi: 10.1093/ejo/23.5.507. [DOI] [PubMed] [Google Scholar]
- 4.Carano A, Testa M. The distal jet for upper molar distalization. J Clin Orthod. 1996;30:374–80. [PubMed] [Google Scholar]
- 5.Kalra V. The K-loop molar distalizing appliance. J Clin Orthod. 1995;29:298–301. [PubMed] [Google Scholar]
- 6.Hilgers JJ. The pendulum appliance for Class II non-compliance therapy. J Clin Orthod. 1992;26:706–14. [PubMed] [Google Scholar]
- 7.Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofacial Orthop. 1996;110:639–46. doi: 10.1016/S0889-5406(96)80041-2. [DOI] [PubMed] [Google Scholar]
- 8.Byloff FK, Darendeliler MA. Distal molar movement using the pendulum appliance. Part 1: Clinical and radiological evaluation. Angle Orthod. 1997;67:249–60. doi: 10.1043/0003-3219(1997)067<0249:DMMUTP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Escobar SA, Tellez PA, Moncada CA, Villegas CA, Latorre CM, Oberti G. Distalization of maxillary molars with the bone-supported pendulum: a clinical study. Am J Orthod Dentofacial Orthop. 2007;131:545–9. doi: 10.1016/j.ajodo.2006.08.012. [DOI] [PubMed] [Google Scholar]
- 10.Kircelli BH, Pektas ZO, Kircelli C. Maxillary molar distalization with a bone-anchored pendulum appliance. Angle Orthod. 2006;76:650–9. doi: 10.1043/0003-3219(2006)076[0650:MMDWAB]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Polat-Ozsoy O, Kircelli BH, Arman-Ozcirpici A, Pektas ZO, Uckan S. Pendulum appliances with 2 anchorage designs: conventional anchorage vs bone anchorage. Am J Orthod Dentofacial Orthop. 2008;133:339.e9–339.e-17. doi: 10.1016/j.ajodo.2007.10.002. [DOI] [PubMed] [Google Scholar]
- 12.Wilmes B, Nienkemper M, Ludwig B, Kau CH, Pauls A, Drescher D. Esthetic Class II treatment with the Beneslider and aligners. J Clin Orthod. 2012;46:390–8. quiz 437. [PubMed] [Google Scholar]
- 13.Sa’aed NL, Park CO, Bayome M, Park JH, Kim Y, Kook YA. Skeletal and dental effects of molar distalization using a modified palatal anchorage plate in adolescents. Angle Orthod. 2015;85:657–64. doi: 10.2319/060114-392.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kinzinger GS, Wehrbein H, Diedrich PR. Molar distalization with a modified pendulum appliance-in vitro analysis of the force systems and in vivo study in children and adolescents. Angle Orthod. 2005;75:558–67. doi: 10.1043/0003-3219(2005)75[558:MDWAMP]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Bussick TJ, McNamara JA., Jr Dentoalveolar and skeletal changes associated with the pendulum appliance. Am J Orthod Dentofacial Orthop. 2000;117:333–43. doi: 10.1016/S0889-5406(00)70238-1. [DOI] [PubMed] [Google Scholar]
- 16.Byloff FK, Darendeliler MA, Clar E, Darendeliler A. Distal molar movement using the pendulum appliance. Part 2: The effects of maxillary molar root uprighting bends. Angle Orthod. 1997;67:261–70. doi: 10.1043/0003-3219(1997)067<0261:DMMUTP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Karcher H, Byloff FK, Clar E. The Graz implant supported pendulum, a technical note. J Craniomaxillofac Surg. 2002;30:87–90. doi: 10.1054/jcms.2002.0281. [DOI] [PubMed] [Google Scholar]
- 18.Kaya B, Sar C, Arman-Ozcirpici A, Polat-Ozsoy O. Palatal implant versus zygoma plate anchorage for distalization of maxillary posterior teeth. Eur J Orthod. 2013;35:507–14. doi: 10.1093/ejo/cjs059. [DOI] [PubMed] [Google Scholar]
- 19.Sar C, Kaya B, Ozsoy O, Ozcirpici AA. Comparison of two implant-supported molar distalization systems. Angle Orthod. 2013;83:460–7. doi: 10.2319/080512-630.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nienkemper M, Wilmes B, Pauls A, Drescher D. Impact of mini-implant length on stability at the initial healing period: a controlled clinical study. Head Face Med. 2013;9:30. doi: 10.1186/1746-160X-9-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kang S, Lee SJ, Ahn SJ, Heo MS, Kim TW. Bone thickness of the palate for orthodontic mini-implant anchorage in adults. Am J Orthod Dentofacial Orthop. 2007;131:S74–81. doi: 10.1016/j.ajodo.2005.09.029. [DOI] [PubMed] [Google Scholar]
- 22.Kinzinger GS, Gulden N, Yildizhan F, Diedrich PR. Efficiency of a skeletonized distal jet appliance supported by miniscrew anchorage for noncompliance maxillary molar distalization. Am J Orthod Dentofacial Orthop. 2009;136:578–86. doi: 10.1016/j.ajodo.2007.10.049. [DOI] [PubMed] [Google Scholar]
- 23.Keles A, Erverdi N, Sezen S. Bodily distalization of molars with absolute anchorage. Angle Orthod. 2003;73:471–82. doi: 10.1043/0003-3219(2003)073<0471:BDOMWA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.King KS, Lam EW, Faulkner MG, Heo G, Major PW. Vertical bone volume in the paramedian palate of adolescents: a computed tomography study. Am J Orthod Dentofacial Orthop. 2007;132:783–8. doi: 10.1016/j.ajodo.2005.11.042. [DOI] [PubMed] [Google Scholar]
- 25.Ludwig B, Glasl B, Bowman SJ, Wilmes B, Kinzinger GS, Lisson JA. Anatomical guidelines for miniscrew insertion: palatal sites. J Clin Orthod. 2011;45:433–41. quiz 67. [PubMed] [Google Scholar]
- 26.Kinzinger GS, Fritz UB, Sander FG, Diedrich PR. Efficiency of a pendulum appliance for molar distalization related to second and third molar eruption stage. Am J Orthod Dentofacial Orthop. 2004;125:8–23. doi: 10.1016/j.ajodo.2003.02.002. [DOI] [PubMed] [Google Scholar]
- 27.Gelgor IE, Karaman AI, Buyukyilmaz T. Comparison of 2 distalization systems supported by intraosseous screws. Am J Orthod Dentofacial Orthop. 2007;131:161.e1–8. doi: 10.1016/j.ajodo.2006.03.027. [DOI] [PubMed] [Google Scholar]
- 28.Oncag G, Seckin O, Dincer B, Arikan F. Osseointegrated implants with pendulum springs for maxillary molar distalization: a cephalometric study. Am J Orthod Dentofacial Orthop. 2007;131:16–26. doi: 10.1016/j.ajodo.2005.07.015. [DOI] [PubMed] [Google Scholar]
- 29.Carano A, Testa M, Bowman SJ. The distal jet simplified and updated. J Clin Orthod. 2002;36:586–90. [PubMed] [Google Scholar]
- 30.Gelgor IE, Buyukyilmaz T, Karaman AI, Dolanmaz D, Kalayci A. Intraosseous screw-supported upper molar distalization. Angle Orthod. 2004;74:838–50. doi: 10.1043/0003-3219(2004)074<0838:ISUMD>2.0.CO;2. [DOI] [PubMed] [Google Scholar]