

Abstract
Objective
In Turkey, orthodontic treatments of individuals aged <18 years are covered by the Social Security Institution (SSI) according to the Index of Complexity, Outcome, and Need (ICON) index at contracted healthcare providers. The aim of this study was to determine treatment needs and difficulties of patients applying to orthodontic clinics in state and foundation universities in Istanbul according to the ICON and to evaluate the extent of treatment coverage by the SSI.
Methods
Pre-treatment study casts of 831 patients were evaluated in terms of treatment needs and difficulties according to the ICON. This sample was distributed as 677 patients who applied to a State University’s Orthodontic Department and 154 who applied to a Foundation University’s Orthodontic Department.
Results
At the state university, 27.9% of the 437 patients had a score of <43 and were thus, described as “no treatment needed.” At the foundation university, 35% of the 154 patients had a score <43 and were thus, described as “no treatment needed.” When the ICON scores of the two universities were compared, no statistically significant difference was found between treatment needs distributions.
Conclusion
The number of patients who applied for treatment for the same period was three times higher in the state university than in the foundation university, whereas the rates of treatment needs were found to be similar between both state and foundation universities. At both universities, nearly one-third of patients were evaluated as “no treatment needed.” The ICON index was found to be a reliable index in terms of reproducibility.
Keywords: ICON, orthodontic treatment difficulty, orthodontic treatment need
INTRODUCTION
Nowadays, increased aesthetic expectations have increased the demand for orthodontic treatments (1). Therefore, several indices have been developed that, together, assess the treatment needs, difficulties, or both (2,3,4,5,6).
In 2000, the Index of Complexity, Outcome, and Need (ICON) was developed by Daniels and Richmond by consulting opinions of 97 orthodontists in nine different countries, and its applications have been wide-ranging. The index is evaluated over five sections, namely the aesthetic component, upper arch crowding/spacing, crossbite, overbite/open bite, and right and left buccal antero-posterior relationships. The aesthetic component is evaluated on a scale comprising 10 photographs from the Index of Orthodontic Treatment Need (IOTN) (Figure 1). Scores obtained from each section are multiplied by their own weight coefficients to obtain the total score (table 1) (2).
Figure 1.
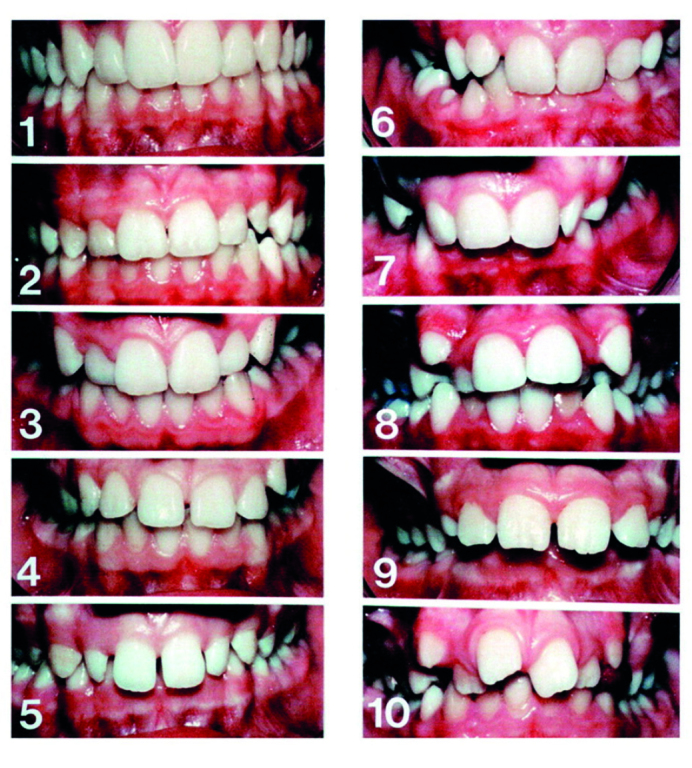
Aesthetic Component (AC) of the IOTN (2). 1–10. 10 photographs display dental attractiveness: (1) The most attractive and (10) the least attractive
Table 1.
ICON scoring protocol
| Score | |||||||
|---|---|---|---|---|---|---|---|
|
|
|||||||
| Component | 0 | 1 | 2 | 3 | 4 | 5 | Weight |
| 1. Aesthetic assessment | Score 1–10 | 7 | |||||
| 2. Upper arch Crowding | <2 mm | 2.1–5 mm | 5.1–9 mm | 9.1–13 mm | 13.1–17 mm | >17 mm or Impacted teeth | 5 |
| Spacing | <2 mm | 2.1–5 mm | 5.1–9 mm | >9 mm | 5 | ||
| 3. Crossbite | No crossbite | Crossbite present | 5 | ||||
| 4. Anterior Openbite | Edge to edge | <1 mm | 1.1–2 mm | 2.1–4 mm | >4 mm | 4 | |
| Overbite | <1/3 lower incisor coverage | 1/3–2/3 coverage | 2/3 up to completely covered | Completely covered | 4 | ||
| 5. Buccal Segment Antero-posterior | Cusp to embrasure only. Class I, II, III | Any cusp relation up to but not including cusp to cusp | Cusp to cusp | 3 | |||
Over the past years in our country, orthodontic treatment has been offered free of charge at contracted healthcare providers to all those aged <18 years by the Social Security Institution (SSI) (7). However, the number of individuals in need of orthodontic treatment is increasing day by day, leading to the necessity of a better management of health resources and their more effective use based on the treatment need.
Our Ministry of Health has reported to file number 23642684/010/2013.5363.34716 that the ICON will be used to determine the need for orthodontic treatment. In accordance with this decision, a report by the patient health board has determined that anybody aged <18 years and with a score of ≥43 on the ICON will be able to access treatment and have their fee repaid by the SSI, whereas those with a score <43 will be treated for a fee for “aesthetic purposes,” except in the case of some criteria (8).
The aim of this study was to determine treatment needs and difficulties of patients applying to orthodontic clinics in state and foundation universities in Istanbul according to the ICON and to evaluate the extent of treatment coverage by the SSI.
METHODS
In this study, pre-treatment study casts and panoramic radiographs of 831 patients who applied to universities between 2013 and 2014 were evaluated. This sample was distributed as follows: 677 patients (392 women and 285 men) who applied to a State University’s Orthodontic Department (first clinic) and 154 patients (94 women and 60 men) who applied to a Foundation University’s Orthodontic Department (second clinic). The exclusion criteria were as follows: patients whose orthodontic models and panoramic X-rays were unclear and who previously underwent orthodontic treatment. A written informed consent form allowing the use of treatment records was obtained from all patients (or the patients’ parents) at the beginning of treatment. Ethics committee approval was obtained from the Istanbul University Faculty of Dentistry’s Clinical Research Ethics Committee with the file number 2016/25.
Pre-treatment study casts were evaluated according to the ICON. Panoramic radiographs were used to detect missing teeth. They were rated by the same researcher at both universities, with the orthodontic models viewed from the frontal plane while in occlusal contact. Obtained scores were multiplied by their own weight coefficients, and the total score was determined. Those with a total score of ≥43 were considered as “treatment is indicated” and those with a score <43 were considered as “no treatment needed.” Orthodontic treatment complexity was evaluated as “easy” if the score was <29, as “mild” if it was between 29 and 50, as “moderate” if it was between 51 and 63, as “difficult” if it was between 64 and 77, and as “very difficult” if it was >77 (2).
Statistical Analysis
To evaluate the repeatability of the ICON index, 160 models from the first clinic and 35 from the second clinic were randomly selected from the total of 831 models, and second measurements were taken by the same investigator 1 month later. The Number Cruncher Statistical System (NCSS) 2007 (version 1) Statistical Software (Utah, USA) package program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation) were used in the evaluation of data as well as an independent t-test for comparison of binary groups and chi-square test for comparison of qualitative data. Results were evaluated at a significance level of p<0.05. The intraclass correlation coefficient (ICC) was calculated to analyze the level of coherence of researchers regarding their ICON index scoring measures.
RESULTS
The mean age distribution of patients evaluated at the first clinic was 16 years and 5 months; 27.9% (189 patients) out of the 437 patients had a score of <43 and were thus, described as “no treatment needed,” whereas 72.1% (488 patients) had a score of ≥43 and were thus, described as “treatment needed.” In terms of treatment difficulty, 7.97% of the scored patients were evaluated as “easy” and 16.2% were evaluated as “very difficult” (table 2).
Table 2.
ICON scores, age, and sex distributions of patients at the state university
| Number | Percentage (%) | Mean Deviation±SD | |||
|---|---|---|---|---|---|
| Sex | Female | 392 | 58 | ||
| Male | 285 | 42 | |||
| Total | 677 | ||||
| Age | Female | 392 | 16.74±3.77 | ||
| Male | 285 | 16.36±4.01 | |||
| Total | 677 | 16.58±3.99 | |||
| ICON Scoring | Treatment need: Yes | ≥43 | 488 | 72.1 | 65.42±16.70 |
| Treatment need: No | <43 | 189 | 27.9 | 32.44±7.73 | |
| Complexity Grade | Easy (0–28) | 54 | 7.97 | 22.44±5.08 | |
| Mild (29–50) | 252 | 37.2 | 40.98±5.96 | ||
| Moderate (51–63) | 124 | 18.3 | 56.62±3.74 | ||
| Difficult (64–77) | 137 | 20.2 | 70.38±3.60 | ||
| Very difficult (77–100) | 110 | 16.2 | 89.04±11.14 |
The mean age distribution of patients evaluated at the second clinic was 17 years and 1 month; 35% (54 patients) of the 154 patients had a score of <43 and were thus, described as “no treatment needed,” whereas 65% (100 patients) had a score of ≥43 and were thus, described as “treatment needed.” In terms of treatment difficulty, 12.98% of the scored patients were evaluated as “easy” and 20.12% were evaluated as “very difficult” (table 3). The female average was significantly higher in the second clinic than in the first clinic (p=0.016). When the ICON scores of the two universities were compared, no statistically significant differences were found between treatment needs distributions (p=0.096). The average score of “treatment needed” (score, >43) group was significantly lower in the second clinic than in the first clinic (p=0.011). The complexity grades “easy” (0–28) and “very difficult” (77–100) scores were significantly higher in the second clinic than in the first clinic (p=0.032), whereas grade “mild” (29–50) score was significantly lower in the second clinic (p=0.031). The complexity grade “very difficult” (77–100) score average was significantly lower in the second clinic than in the first clinic (p=0.011) (table 4).
Table 3.
ICON scores, age, and sex distributions of the patients at the foundation university
| Number | Percentage (%) | Mean Deviation±SD | |||
|---|---|---|---|---|---|
| Sex | Female | 94 | 61 | ||
| Male | 60 | 39 | |||
| Total | 154 | ||||
| Age | Female | 94 | 17.81±4.21 | ||
| Male | 60 | 16.02±5.02 | |||
| Total | 154 | 17.16±5.88 | |||
| ICON Scoring | Treatment need: Yes | ≥43 | 100 | 65 | 67.20±14.88 |
| Treatment need: No | <43 | 54 | 35 | 29.22±9.54 | |
| Complexity Grade | Easy (0–28) | 20 | 12.98 | 19.10±7.28 | |
| Mild (29–50) | 54 | 35.06 | 39.03±6.13 | ||
| Moderate (51–63) | 15 | 9.74 | 55.53±3.44 | ||
| Difficult (64–77) | 34 | 22.07 | 69.35±3.88 | ||
| Very difficult (77–100) | 31 | 20.12 | 83.67±5.92 |
Table 4.
ICON scores, age, and sex distributions of patients between the two universities
| Number | Percentage (%) | Mean Deviation±SD | |||
|---|---|---|---|---|---|
| Age | Female | 16.74±3.77 | 17.81±4.21 | 0.016 | |
| Male | 16.36±4.01 | 16.02±5.02 | 0.569 | ||
| Total | 16.58±3.99 | 17.16±5.88 | 0.141 | ||
| Sex | Female | 392 57.90% | 94 61.04 | 0.534 | |
| Male | 285 42.10% | 60 38.96 | |||
| ICON Scoring | Treatment need | ≥43 Yes | 488 72.08% | 100 64.94 | 0.096 |
| <43 No | 189 27.92% | 54 35.06 | |||
| Treatment need (Mean Deviation) | ≥43 Yes | 65.42±16.70 | 67.20±14.88 | 0.323 | |
| <43 No | 32.44±7.73 | 29.22±9.54 | 0.011 | ||
| Complexity Grade | Easy (0–28) | 54 7.98% | 20 12.99 | 0.032 | |
| Mild (29–50) | 252 37.22% | 54 35.06 | |||
| Moderate (51–63) | 124 18.32% | 15 9.74 | |||
| Difficult (64–77) | 137 20.24% | 34 22.08 | |||
| Very difficult (77–100) | 110 16.25% | 31 20.13 | |||
| Complexity Grade (Mean Deviation) | Easy (0–28) | 22.44±5.08 | 19.10±7.28 | 0.029 | |
| Mild (29–50) | 40.98±5.96 | 39.03±6.13 | 0.031 | ||
| Moderate (51–63) | 56.62±3.74 | 55.53±3.44 | 0.284 | ||
| Difficult (64–77) | 70.38±3.60 | 69.35±3.88 | 0.143 | ||
| Very difficult (77–100) | 89.04±11.14 | 83.67±5.92 | 0.011 |
When the level of compliance between the first and second measurement results of both universities was evaluated, a positive correlation with all values and between the total values was observed, with a statistically significant level of 98.8% (p<0.01) (table 5).
Table 5.
Level of coherence between the researcher’s ICON scores
| Intraclass correlation coefficient (ICC) | 95% CI | p | ||
|---|---|---|---|---|
| Aesthetic component | 0.984 | 0.979 | 0.988 | 0.000** |
| Upper arch crowding/spacing | 0.992 | 0.989 | 0.994 | 0.000** |
| Crossbite | 0.986 | 0.981 | 0.990 | 0.000** |
| Overbite/openbite | 0.971 | 0.961 | 0.979 | 0.000** |
| Right buccal antero-posterior | 0.951 | 0.934 | 0.964 | 0.000** |
| Left buccal antero-posterior | 0.912 | 0.881 | 0.935 | 0.000** |
| Total | 0.988 | 0.983 | 0.991 | 0.000** |
ICC: Intraclass correlation coefficient 95% CI: 95% confidence interval
p<0.01
DISCUSSION
In this study, orthodontic models of patients that applied for treatment at state and foundation universities were scored by the same investigator according to the ICON index. The level of compliance with the first and second measurements (ICC: 0.988) was high, indicating that the ICON index is highly reproducible. The ICON index has been applied by the same researcher or by different researchers to obtain compatible results (9–12).
In this study, 72.1% of patients at the first clinic and 65% of those at the second clinic were scored as ≥43 and were thus, evaluated as “treatment needed” according to the ICON. Onyeaso and Be Gole (10) have reported treatment needs according to the ICON in 86% of 100 patients, Kamak et al. (13) in 58% of 154 patients, Utomi and Onyeaso (14) in 38% of 150 patients, and Lopez et al. (15) in 37% of 162 patients. Rates observed when evaluating treatment needs vary according to factors such as race, number of patients, and age distribution. The number of patients evaluated in our study was considerably higher than that in other studies in the literature. Furthermore, patients in our study comprised those who had applied for orthodontic treatment, instead of randomly selected members of the normal population. The higher ICON scores of our study can be attributed to this.
In terms of treatment difficulties, results showed that in the first clinic, 7.97% of patients were evaluated as “easy,” 37.2% were evaluated as “mild,” 18.3% were evaluated as “moderate,” 20.2% were evaluated as “difficult,” and 16.2% were evaluated as “very difficult.” In the second clinic, 12.98% of patients were evaluated as “easy,” 35.06% were evaluated as “mild,” 9.74% were evaluated as “moderate,” 22.07% were evaluated as “difficult,” and 20.12% were evaluated as “very difficult.” Richmond et al. (16) have reported that 36% of 100 patients they examined were evaluated as “very difficult,” whereas Kamak et al. (17) have reported that 56.4% of 500 patients they examined were evaluated as “difficult” or “very difficult” and Onyeaso (18) has reported the same for 10% of 274 patients examined.
In our country, treatment fees for patients aged <18 years applying for orthodontic treatment are covered by the government if they score ≥43 on the ICON index. With this rule of force since 2013, its aim is to increase treatment quality by providing orthodontic treatment to patients who need treatment and whose treatment difficulty is high. In our study, an average of one-third of patients who applied to both universities scored <43 and was thus, ineligible for treatment. This practice ensures that the health budget is rationally used by directing resources to patients of most need of treatment, instead of to purely aesthetic patients.
The limitation of our study was the difference between the number of patients at the two clinics. In our study, patients referred to both state and foundation universities during the same period were examined. Therefore, the number of patients at these two clinics was variable because of the high concentration of patients at the state university.
CONCLUSION
In our study, the distribution of orthodontic treatment services funded by the SSI for individuals with treatment needs according to the ICON index was examined at both state and foundation universities. The number of patients who applied for treatment during the same period was three times higher in the state university than in the foundation university, whereas the rates of treatment needs of patients were similar in both universities. At both universities, nearly one-third of patients were evaluated as “no treatment needed.” The ICON index was found to be a reliable index in terms of reproducibility.
Footnotes
Ethics Committee Approval: Ethics committee approval was received for this study from the Istanbul University School of Dentistry’s Clinical Research Ethics Committee (2016/25).
Informed Consent: Written informed consent was obtained from the patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - M.K., A.S.Y.; Design - M.K., A.S.Y.; Supervision - M.K., A.S.Y.; Data Collection and/or Processing - M.K., A.S.Y.; Analysis and/or Interpretation - M.K., A.S.Y.; Writing Manuscript - M.K., A.S.Y.; Critical Reviews - M.K., A.S.Y.
Conflict of Interest: The authors have no conflict of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Templeton KM, Powell R, Moore MB, Williams AC, Sandy JR. Are the Peer Assessment Rating Index and the Index of Treatment Complexity, Outcome, and Need suitable measures for orthognathic outcomes? Eur J Orthod. 2006;28:462–6. doi: 10.1093/ejo/cji120. [DOI] [PubMed] [Google Scholar]
- 2.Daniels C, Richmond S. The development of the index of complexity, outcome and need (ICON) J Orthod. 2000;27:149–62. doi: 10.1093/ortho/27.2.149. [DOI] [PubMed] [Google Scholar]
- 3.Llewellyn SK, Hamdan AM, Rock WP. An index of orthodontic treatment complexity. Eur J Orthod. 2007;29:186–92. doi: 10.1093/ejo/cjl080. [DOI] [PubMed] [Google Scholar]
- 4.Richmond S, Shaw WC, O’brien KD, Buchanan IB, Jones R, Stephens CD, et al. The development of the PAR Index (Peer Assessment Rating): reliability and validity. Eur J Orthod. 1992;14:125–39. doi: 10.1093/ejo/14.2.125. [DOI] [PubMed] [Google Scholar]
- 5.Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11:309–20. doi: 10.1093/oxfordjournals.ejo.a035999. [DOI] [PubMed] [Google Scholar]
- 6.Draker HL. Handicapping labio-lingual deviations: a proposed index for public health purposes. Am J Orthod. 1960;46:295–305. doi: 10.1016/0002-9416(60)90197-4. [DOI] [Google Scholar]
- 7.http://www.resmigazete.gov.tr/eskiler/2012/01/20120121-4.htm
- 8.Ankara Valiliği İl Sağlık Müdürlüğü Tebligatı-Ortodonti tedavi gerekliliği indeksi. http://www.asm.gov.tr/UploadGenelDosyalar/SubeDosyalari/Dosyalar/31_08_2016_10_51_24.pdf.
- 9.Onyeaso CO, BeGole EA. Orthodontic treatment need in an accredited graduate orthodontic center in North America: a pilot study. J Contemp Dent Pract. 2006;7:87–94. [PubMed] [Google Scholar]
- 10.Onyeaso CO, BeGole EA. Orthodontic treatment standard in an accredited graduate orthodontic clinic in North America assessed using the Index of Complexity, Outcome and Need (ICON) Hell Orthod Rev. 2006;9:23–24. [Google Scholar]
- 11.Firestone AR, Beck FM, Beglin FM, Vig KW. Validity of the Index of Complexity, Outcome, and Need (ICON) in determining orthodontic treatment need. Angle Orthod. 2002;72:15–20. doi: 10.1043/0003-3219(2002)072<0015:VOTIOC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Torkan S, Pakshir HR, Fattahi HR, Oshagh M, Danaei SM, Salehi P, et al. An Analytical Study on an Orthodontic Index: Index of Complexity, Outcome and Need (ICON) J Dent. 2015;16:149. [PMC free article] [PubMed] [Google Scholar]
- 13.Kamak H, Çağlaroğlu M, Çatalbaş B, Keklik H. İç Anadolu Bölgesi Ortodontik Tedavi İhtiyacının ICON İndeksi Kullanılarak Değerlendirilmesi. J Dent fac Atatürk Uni. 2012;22:149–153. [Google Scholar]
- 14.Utomi IL, Onyeaso CO. Orthodontic treatment complexity and need in a Nigerian Teaching Hospital. Oral Health Dent Manag. 2014;13:562–7. [PubMed] [Google Scholar]
- 15.López MFC, Rojo MFG, Rojo JFG, García ARR. Comparison between the ICON index and the esthetic component of the IOTN to determine the need for orthodontic treatment. Revista Mexicana de Ortodoncia. 2017;5:e10–e13. doi: 10.1016/j.rmo.2017.03.029. [DOI] [Google Scholar]
- 16.Richmond S, Ikonomou C, Williams B, Ramel S, Rolfe B, Kurol J. Orthodontic treatment standards in a public group practice in Sweden. Swedish Dent J. 2001;25:137–44. [PubMed] [Google Scholar]
- 17.Kamak H. Doktora Tezi. Atatürk Üniversitesi, Sağlık Bilimleri Enstitüsü, Ortodonti Anabilim Dalı; Erzurum: 2010. ICON İndeksi Kullanılarak Tedavi Sonucunun Kabul Edilebilirliğinin, Tedavi Zorluğunun ve Tedavinin İyileşme Derecesinin Değerlendirilmesi. [Google Scholar]
- 18.Onyeaso CO. Relationship between Index of Complexity, Outcome and Need and Dental Aesthetic Index in the assessment of orthodontic treatment complexity and need of Nigerian adolescents. Pesqui Bras Odontopediatria Clin Integr. 2008;8:145–9. doi: 10.4034/1519.0501.2008.0082.0002. [DOI] [Google Scholar]