

Abstract
Background
Improved knowledge of the distal triceps insertion is needed as a result of an increase in procedures involving this area, including distal triceps repair, posterior capsulectomy, and olecranon tip osteotomy for coronoid reconstruction.
Materials and methods
Five pair-matched upper limbs were dissected to study the morphology and dimension of the distal triceps tendon, triceps tendon insertion, capsular insertion on the olecranon, and triceps lateral retinaculum. Muscle origins of the triceps insertions were identified proximally.
Results
Three distinct insertional areas were found in the olecranon corresponding to the posterior capsular insertion, the deep muscular portion, and the superficial tendinous portion of the triceps with areas of 1.5, 1.2, and 2.8 cm2, respectively. The deep muscular head corresponded to the medial head of the triceps and the tendinous portion corresponded to the long and lateral heads and correlated with the height of the specimen. The triceps width at insertion was 2.6 ± 0.5 cm (standard deviation), and the triceps lateral retinaculum extended the tendon laterally for 2.5 ± 0.7 cm. The tendinous portion of the triceps tendon extended proximally 15.3 ± 1.4 cm. The triceps inserted at a mean of 1.1 cm from the tip of the olecranon.
Conclusions
The distinct insertional heads of the triceps provides additional knowledge that can aid in diagnosing and treating partial triceps tears. In addition, a safe zone for capsulectomy and olecranon tip osteotomy is described that can be used to increase the safety of these procedures.
Keywords: Triceps, Tendon, Muscle, Distal triceps, Triceps footprint, Anatomy
The triceps has historically been described as consisting of 3 muscular heads—the long head, the lateral head, and the medial head—that coalesce into a common and single insertion on the olecranon. The radial nerve innervates all 3 heads, but they originate from different anatomic sites at the glenoid and posterior aspect of the humeral shaft and are thought to insert at a distinct common insertion site.
Some authors have reported an isolated avulsion of the medial head of the triceps, but other anatomic studies have failed to find a distinct insertion pattern.2, 10, 12 The morphology of the injury may affect clinical presentation, imaging analysis, and surgical strategies. Furthermore, complications with triceps healing after total elbow arthroplasty have generated renewed interest in the adoption of “triceps-on” exposures and lateral and medial paraolecranon approaches that respect portions of the triceps insertion.1, 5, 16, 17
There are several clinical scenarios in which an exact knowledge of the insertional anatomy of the triceps to the olecranon might aid surgical treatment. Traumatic injuries to the triceps tendon, although relatively rare, require prompt diagnosis and oftentimes surgery. They are generally associated with a sudden event resulting in an eccentric load to a contracting triceps, usually with the arm in extension. It is uncommon that the whole triceps insertion is avulsed, and the lateral part of the tendinous insertion is typically left intact, which can delay diagnosis, but the recent recognition of the occurrence of partial tears requires additional anatomic knowledge.11
Apart from triceps tendon injuries, the propensity for surgical intervention involving the posterior aspect of the elbow, including exposures for distal humeral fracture internal fixation, elbow arthroplasty, and the use of portions of the olecranon as a graft for patients with persistent elbow instability, has fostered an interest in the anatomy of the distal tendon triceps tendon and its insertional footprint.1, 4, 7, 13, 15, 19 Recognition of a distinct footprint area would be of value in the diagnosis and repair of acute triceps ruptures, in designing effective surgical strategies for exposure to the elbow, and avoiding injury when performing operations involving the posterior olecranon.
The purpose of this study was to perform an anatomic study of the triceps insertion and its relationships to the 3 muscular origins with a special focus on the insertional footprint in the olecranon. We hypothesized that different portions of the triceps would have specific insertional footprint areas.
Materials and methods
Five paired-matched cadaveric upper limbs (total 10 limbs) including the shoulder, arm, elbow, forearm, wrist, and hand were obtained from the Mayo Clinic Institutional Department of Anatomy. Origins of the muscles were included to trace the relative contributions to the insertional footprint. No specimens had evidence of prior surgery or obvious injury to the elbow joint. The deceased donors (3 men and 2 women) were a mean (standard deviation) age of 72.4 ± 11.86 years (range, 56-86 years), a mean height of 169.3 ± 13.6 cm, and had a mean body mass index of 24.38 ± 2.39 kg/m2.
The specimens were thawed at room temperature 24 hours before dissection, which was done using a midline posterior skin incision exposing the brachial and antebrachial fascia with the elbow in 90° of flexion. The superficial fascia was removed to expose the triceps muscle and tendon while protecting the ulnar nerve that had been previously isolated.
The triceps proximal muscular origins were isolated and followed distally. Gross measurements of the triceps tendinous portion and the lateral retinaculum to its insertion were performed. The triceps muscle was divided just proximal to the most proximal part of the superficial tendon and dissected distally toward the insertion separating it from the medial and lateral septum and the posterior aspect of the humerus. Laterally, the triceps was dissected from the brachioradialis and wrist extensors to facilitate exposure of the deep side of the triceps muscle and tendon along with the fat pad and capsule. The lateral side of the tendon was identified from the deep portion of the triceps, as the fibers were seen inserting into the olecranon and separate from the lateral retinaculum. The distal insertion of the retinaculum into the forearm fascia and the lateral extension of the retinaculum at the level of the triceps insertion were also measured.
The width of the triceps tendon was measured at the insertion and at 3 and 6 cm proximally. The capsule was released from the deep portion of the tendon and was released from proximal to distal to reveal its insertion on the olecranon. After the capsule was completely released, an attempt to distinguish discrete deep and superficial layers of the tendon at the insertion was performed. Finally, progressive release of the tendon insertion was performed, and footprint measurements were recorded. The footprint area was calculated using the methodology described by Yeh et al.20
All measurements were performed using a digital sliding caliper with precision to 0.1 mm (SE 784EC; Electronix Express, Rahway, NJ, USA) and were taken twice by a single surgeon with an interval of approximately 1 hour. The mean ± standard deviation (range) of these measurements was recorded. This was not possible for some measurements that required excision of the structure. Descriptive statistical analysis was performed with IBM SPSS Statistics for Windows 20.0 software (IBM, Armonk, NY, USA). Statistical significance was defined as the likelihood of differences to have occurred by chance to be <.05.
Results
Triceps muscle dissection
The triceps tendon had a distinct medial border extending proximally further than the lateral side, with the tendinous portion having a pennate aspect at mean distance from the olecranon of 15.25 ± 1.4 cm (range, 13.5-17.7 cm; Fig. S1). The superficial fascia of the triceps tendon had a direct relationship medially with the ulnar nerve and had fibers that extended into the posteromedial gutter, contributing to the floor of the ulnar nerve.
The tendinous portion extended laterally past the lateral border of the olecranon for a mean of 3 ± 0.7 mm (range, 1.5-3.8 mm; Table I). On visual inspection, delineating a discrete borderline between the lateral border of the triceps tendon and the lateral retinaculum was difficult. The dimensions of the triceps tendon were considered to include those fibers that connected to the olecranon on the deep side of the insertion, but this distinction was hard to make on the superficial side, especially on the lateral side of the tendon, which was hard to distinguish from the lateral retinaculum. Distally, the fibers of the lateral retinaculum blended with fibers of the forearm fascia covering the anconeus muscle and inserting into the ulna, with the most distal fibers at a mean distance of 8 ± 0.8 cm (range, 7-9 cm; Fig. S2). With extension of the elbow, these divergent fibers aligned with the rest of the triceps extensor mechanism. Morphologic aspects of the lateral retinaculum are reported as Supplementary Material.
Table I.
Measurements of the triceps length and lateral retinaculum dimensions*
| Specimen | Triceps length | Triceps width | Lateral retinaculum | ||||
|---|---|---|---|---|---|---|---|
| At insertion | At 3 cm† | At 6 cm† | Proximal expansion | Width | Length | ||
| 1 | 149.37 | 39.92 | 37.22 | 35.48 | 35.65 | 16.44 | 76.92 |
| 2 | 151 | 26.36 | 36.02 | 35.37 | 34.3 | 15.28 | 74.98 |
| 3 | 151.28 | 27.72 | 32.39 | 36 | 46.71 | 27.16 | 83.45 |
| 4 | 174.1 | 27 | 32.93 | 37.22 | 38.33 | 29.08 | 88.24 |
| 5 | 143.6 | 19.9 | 27.3 | 36.34 | 42.44 | 24.74 | 70.7 |
| 6 | 154.14 | 21.33 | 31.44 | 40.68 | 38.59 | 22.28 | 70.1 |
| 7 | 134.3 | 23.62 | 35.27 | 43.89 | 43.91 | 25.86 | 83.8 |
| 8 | 134.83 | 24.42 | 37.29 | 38.46 | 44.62 | 19.46 | 70.59 |
| 9 | 155.31 | 23.04 | 41.12 | 46.04 | 45.05 | 35.68 | 88.39 |
| 10 | 176.78 | 25.65 | 31.03 | 43.82 | 49.89 | 37.56 | 89.16 |
See Fig. 2. All measurements are in mm.
Measurements of the triceps width, 3 and 6 cm proximal to the tip of the olecranon.
The triceps tendon and lateral retinaculum were dissected laterally in the interval between the brachioradialis and the triceps, elevating the muscle from the posterior aspect of the humerus and lateral column until the capsule was seen. The ulnar nerve was dissected free from the superficial fascia on the medial side, and the medial head of the triceps was elevated from the posterior aspect of the humerus and the medial intermuscular septum until the capsule was seen. The triceps muscle was divided at the level of the musculotendinous junction and flipped forward to continue the dissection of the capsule and the overlying muscle.
Capsule and capsular footprint
The capsule and muscle fibers blended close to the insertion but were easily dissected unto the bony insertion. On 2 specimens, some distinct muscle fibers attached directly to the posterior capsule. The capsule extended from the medial to the lateral column and from the insertion in the olecranon to the margin of the olecranon fossa. The capsule was measured and dissected proximally while maintaining the insertion on the olecranon to determine the area of insertion and the distance of the tip of the olecranon to the capsule insertion (Table II). The insertion area of the posterior capsule was broader at the center of the olecranon and thinned towards both sides of the olecranon (Fig. 1).
Table II.
Measurements of the capsular insertion dimensions and footprint of the deep (muscular) and superficial (tendinous) insertions of the distal triceps*
| Specimen | Capsule footprint | Olecranon tip-capsule distance | Deep triceps insertion | Superficial triceps insertion | |||
|---|---|---|---|---|---|---|---|
| Width | Height | Width | Height | Width | Height | ||
| 1 | 21.31 | 4.6 | 3.7 | 22.07 | 2.9 | 20.86 | 14.26 |
| 2 | 21.73 | 4.1 | 7.75 | 16.15 | 7.55 | 23.1 | 16.89 |
| 3 | 24 | 5.25 | 6.21 | 14.83 | 6.85 | 23.05 | 11.73 |
| 4 | 23.76 | 5.63 | 7.77 | 21.8 | 4.26 | 22.3 | 15.6 |
| 5 | 25.62 | 7 | 3 | 17.15 | 3.72 | 17.49 | 7.49 |
| 6 | 25.58 | 6.43 | 2.7 | 16.76 | 3.24 | 20.24 | 5.78 |
| 7 | 21.64 | 7.35 | 3.14 | 21.77 | 7.15 | 23.45 | 14.18 |
| 8 | 18.82 | 8.32 | 2.93 | 18.56 | 8.72 | 22.19 | 14.44 |
| 9 | 19.49 | 9.46 | 3.11 | 21.66 | 6.8 | 22.16 | 10.29 |
| 10 | 17.26 | 9.72 | 4.63 | 23.27 | 11.62 | 26.36 | 13.04 |
All measurements are in mm.
Figure 1.

Posterior view of a right elbow with the triceps muscle reflected backwards. (A) The posterior capsule of the elbow has been released proximally and from the medial and lateral column and is being held by the forceps. (B) The capsule is broadest at the midpart of the olecranon and may insert very close to the olecranon tip. (C) After resection of the capsule, a distinct capsular insertional area becomes evident.
Distal triceps and insertional footprint
After the posterior capsule was resected, the triceps tendon insertion was noticed to have a deep bulky muscular insertion and a superficial tendinous insertion. Close inspection showed the deep muscular portion of the triceps had a tendinous insertion, but the length of the tendon at this point was inconsistent or too small to measure (Fig. 2). The distal aspect of the triceps muscle and tendon were studied to analyze the distinct insertion sites of the medial, long, and lateral heads of the complex. The dissection began at the distal medial border of the triceps tendon, and as it continued proximally the muscle fibers were observed to assume a 90° orientation with respect to the central tendon. Proximally, the deep muscular insertion originated from the medial head, and the tendinous superficial insertion originated from the long and lateral heads of the triceps (Fig. 3).
Figure 2.

The deep muscular insertion of the triceps has a bulky muscular tendinous insertion that shows a millimetric tendinous insertion on close insepction.
Figure 3.

Progressive disection of the distal triceps. (A) After the triceps muscle is flipped back, the true triceps tendon can be seen superficial to the deep muscular part. (B) Dissection on the medial side can easily identify a plane of cleavage between the deep and superficial parts of the tendon. (C) A view from the lateral side of the elbow shows the relationship between the deep portion (1), the superficial portion (2), and the lateral retinaculum (3), which overlies the anconeus muscle. (D) When the triceps is flipped back, the triceps tendon proper can be seen to form a sturdy tendinous structure perpendicular to the superficial triceps tendon. (E and F) After resection of the distal insertion, one can observe the long tendinous insertion of the superfical portion of the triceps and the short tendinous insertion of the deep portion of the triceps.
Near the insertion, all the specimens revealed a plane of cleavage between the deep muscular and the more superficial tendinous insertion, which continued to discrete insertion sites at the footprint on the olecranon. The superficial tendinous portion was observed to originate from the long and lateral heads of the triceps, whereas the deep muscular portion originated from the medial head of the triceps. The superficial insertion of the triceps tendon formed a “W”-type shape with the medial “V” inserting slightly more distal than the lateral “V” (Fig. 4). Finally, the tendinous portion of the insertion was sharply released from the insertion site, and footprint analysis of the superficial tendinous portion was performed.
Figure 4.

The tendinous portion inserts onto the olecranon, forming a “W.” The medial fibers insert most typically distal than the lateral fibers.
We were able to characterize 3 distinct contributions to the footprint corresponding to the capsule, the deep portion of the triceps, and the common tendinous insertion sites (Fig. 5). The posterior capsule has a mean footprint insertion of 1.5 ± 0.3 cm2, the superficial triceps tendon insertion averaged 2.8 ± 1 cm2, and the deep triceps insertion averaged 1.2 ± 0.6 cm2. The mean distance from the olecranon tip to the beginning of the capsular insertion was 0.4 ± 0.2 cm (Table II). The distinct medial head of the triceps width and height positively correlated with the height of the specimens at 0.49 (P = .14) and 0.59 (P = .07), respectively. The mean distance from the tip of the olecranon to the triceps tendon was 1.1 cm, with all except 1 specimen having a safe distance of 1 cm. A safe zone for performing an olecranon tip osteotomy without violating the triceps insertion was defined at 1 cm from the tip of the olecranon (Fig. 6).
Figure 5.

After resection of the complete triceps insertion and posterior capsule, the bare olecranon shows 3 insertional areas corresponding to the posterior capsular insertion (1), the deep muscular head of the triceps (2), and the superficial tendinous head of the triceps (3).
Figure 6.
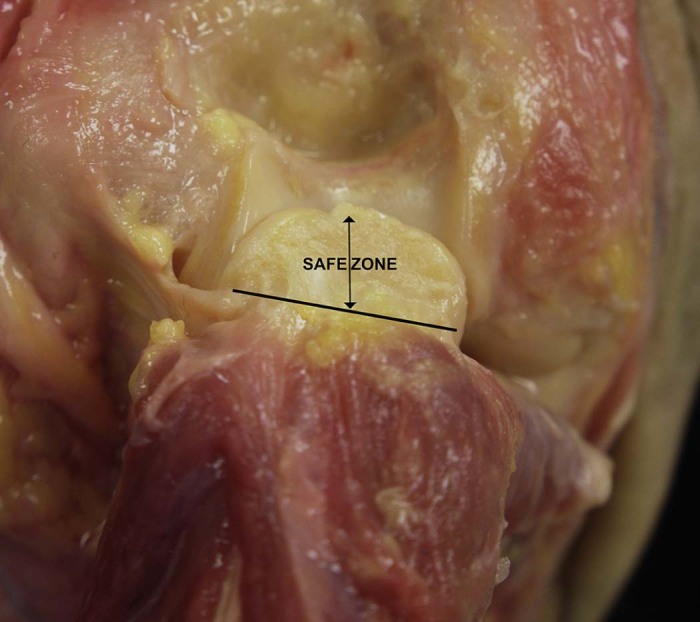
A safe zone described for olecranon osteotomy includes the distance from the tip of the olecranon to the muscular insertion of the deep head of the triceps.
Discussion
The insertional footprint has been variably reported in earlier reports.10, 11 The acknowledgement of distinct insertional areas of the triceps may have implications in our understanding of partial ruptures of the triceps and may help to avoid complications related to surgical approaches involving the posterior part of the olecranon and the distal triceps.2, 5, 8, 12, 13, 16
We have identified three distinct insertion areas corresponding to the posterior capsular insertion, a deep muscular insertion and a common tendinous insertion of the triceps. The posterior capsule and the deep head of the triceps, to the best of our knowledge, have not yet been described as having a distinct and independent insertion site on the olecranon.
Yeh et al20 performed an anatomic study of the distal triceps insertion and included the capsular insertion as part of the global tendinous insertional footprint. Some authors have described triceps injuries affecting only the deep muscular insertion, which corresponds to the medial head of the triceps but did not recognize a distinct insertional footprint.2, 12 Athwal et al2 found a discrete insertional area for the medial head of the triceps in 8 of 15 specimens. Although the tendinous fibers of both the superficial and deep portions of the triceps tendon coalesce and insert as a single unit on visual inspection, blunt dissection carried toward the insertion can identify consistently a separate insertional area.
Recently, there have been several reports on the isolated partial superficial tears of the distal triceps tendon attachment.6, 9, 11, 18 Downey et al6 reported a retrospective ultrasound analysis of 5 partial ruptures of the superficial tendinous portion with integrity of the deep portion as assessed by magnetic resonance imaging or confirmed in surgery, although outcomes of the procedures were not reported. Interestingly, all cases were associated with an avulsed osseous fragment evident on radiographs and ultrasound imaging. Advanced imaging techniques may be essential in detecting these injuries with increased precision and designing a surgical strategy.
There has also been some lack of clarity regarding which components of the complex contribute to various elements of the insertion site. The deep portion of the triceps has been recognized to originate from the medial head of the triceps and it is muscular almost to the point of insertion, with more tendinous fibers in the superficial part of this deep portion.3, 12 The superficial distal triceps tendon originates from the long and lateral heads of the triceps and has a distinct and well-structured tendinous insertion on the posterior aspect of the olecranon.
The insertional footprint has been variably reported in earlier reports as ranging from 280 to 646 mm2.10, 11 Our findings are in the middle of this range, and this variability most likely results from the definition of what constitutes the footprint, because some authors, such as Keener et al,10 have only included the superficial tendinous attachment in this definition. Including the deep muscular portion of the triceps in the definition of what constitutes the footprint would seem logical.3, 20
The anatomic arrangement of the distal triceps footprint insertion may have functional implications. Confluence of the capsule with the muscle close to the insertion and the findings of direct muscle fibers insertion into the posterior capsule suggest a possible role in proprioception. Further clinical relevance might include limiting the amount of olecranon that can be removed before violating the insertional footprint. A study by Moritomo et al13 described the use of an osteochondral autograft of the ipsilateral posterior olecranon to reconstruct coronoid-deficient elbows. We have described that limiting the osteotomy to 1 cm distal to the tip of the olecranon will be safe in 9 of 10 cases.
The occurrence of partial triceps ruptures may be explained by the fact that the deep portion of the triceps is centrally located on the olecranon and is smaller than the superficial tendinous portion.2, 8, 12 Differential strength at different positions of elbow flexion may also be explained by the specific portion and location of the insertion that is involved and can be related to the different length/tension relationship of each head at different flexion angles. The mechanical advantage for each portion of the triceps may change with elbow position and may influence the location of the injury depending on the position of the arm when the injury occurs.14 A study by Madsen et al12 described a triceps rupture in a weightlifter corresponding to the medial head of the triceps that resulted in profound weakness from full to 90° of flexion but with nearly normal strength in terminal extension. This deficiency resolved with repair. Athwal et al2 reported 2 patients with partial ruptures of the deep portion. Clinically, they complained of pain against elbow extension without a palpable defect, 1 of them without weakness.2
The limitations of this study include the absence of advanced imaging or histologic analysis that could help differentiate the component parts of the triceps, but careful dissection tracing the origins of the muscles was performed and may obviate the need for additional imaging. Also, the average age of the specimens being 72 years might have influenced some of the morphologic characteristics we have described, but all elbows were analyzed for the presence of osteoarthritis, which was an exclusion criterion. We believe, however, that these limitations do not affect the findings of the study.
Conclusion
There is increasing evidence of the presence of distinct footprint areas in the olecranon for the posterior elbow capsule, the medial head of the triceps, and the common tendon of the long and lateral head of the triceps. The medial head of the triceps is separated from the rest of the triceps by a distinct plane of cleavage and represents the deep attachment of the complex. The morphologic features and numeric values reported in our study can be of help in the surgical repair of partial and complete distal triceps tendon ruptures as well as when designing procedures that require partial or complete detachment of the triceps or removal of portions of the olecranon.
Disclaimer
The authors, their immediate families, and any research foundation with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Acknowledgements
We acknowledge our gratitude to the people who donated their bodies that were used in this study.
Footnotes
A specific proposal from the Biospecimens Committee for this study was approved by the Mayo Clinic Institutional Review Board (10429.006).
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.jses.2017.05.002.
Appendix. Supplementary data
The following are the supplementary data to this article:
Other anatomic measurements are considered. The width and height and distal extension of the lateral retinaculum were measured as follows (Fig. S1): The height was considered as the distance from the posterolateral corner of the olecranon to the point where it blended with the triceps. The width was considered as the distance from the posterolateral corner of the olecranon to the most lateral aspect of the lateral retinaculum with 90° of elbow flexion. The fibers of the distal extension of the lateral retinaculum were blended with the forearm fascia but were considered as extending over the anconeus to its insertion in the ulna (Table I).
Posterior approach to the elbow with exposed triceps extensor mechanism. Superficially, the fibers of the medial head of the triceps appear to insert obliquely into the most medial aspect of the triceps tendon. The lateral expansion of the triceps can extend laterally significantly.
Lateral view of a right elbow. The lateral reticnaculum of the triceps is seen merging its fibers proximally with the triceps tendon proper and distally with fibers of the extensor carpi ulnaris. The lateral retinaculum has been released according to a Kocher approach to the lateral elbow. The width, length, and proximal extension were considered as shown in the photograph before any release.
References
- 1.Alonso-Llames M. Bilaterotricipital approach to the elbow. Its application in the osteosynthesis of supracondylar fractures of the humerus in children. Acta Orthop Scand. 1972;43:479–490. doi: 10.3109/17453677208991270. [DOI] [PubMed] [Google Scholar]
- 2.Athwal G.S., McGill R.J., Rispoli D.M. Isolated avulsion of the medial head of the triceps tendon: an anatomic study and arthroscopic repair in 2 cases. Arthroscopy. 2009;25:983–988. doi: 10.1016/j.arthro.2009.02.020. [DOI] [PubMed] [Google Scholar]
- 3.Belentani C., Pastore D., Wangwinyuvirat M., Dirim B., Trudell D.J., Haghighi P. Triceps brachii tendon: anatomic-MR imaging study in cadavers with histologic correlation. Skeletal Radiol. 2009;38:171–175. doi: 10.1007/s00256-008-0605-6. [DOI] [PubMed] [Google Scholar]
- 4.Bryan R.S., Morrey B.F. Extensive posterior exposure of the elbow. A triceps-sparing approach. Clin Orthop Relat Res. 1982;166:188–192. [PubMed] [Google Scholar]
- 5.Celli A., Arash A., Adams R.A., Morrey B.F. Triceps insufficiency following total elbow arthroplasty. J Bone Joint Surg Am. 2005;87:1957–1964. doi: 10.2106/JBJS.D.02423. [DOI] [PubMed] [Google Scholar]
- 6.Downey R., Jacobson J.A., Fessell D.P., Tran N., Morag Y., Kim S.M. Sonography of partial-thickness tears of the distal triceps brachii tendon. J Ultrasound Med. 2011;30:1351–1356. doi: 10.7863/jum.2011.30.10.1351. [DOI] [PubMed] [Google Scholar]
- 7.Eygendaal D. Ligamentous reconstruction around the elbow using triceps tendon. Acta Orthop Scand. 2004;75:516–523. doi: 10.1080/00016470410001367-1. [DOI] [PubMed] [Google Scholar]
- 8.Ganeshan R.M., Keerthi N. Isolated medial head of triceps rupture. BMJ Case Rep. 2014;2014 doi: 10.1136/bcr-2014-205452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Heikenfeld R., Listringhaus R., Godolias G. Endoscopic repair of tears of the superficial layer of the distal triceps tendon. Arthroscopy. 2014;30:785–789. doi: 10.1016/j.arthro.2014.03.005. [DOI] [PubMed] [Google Scholar]
- 10.Keener J.D., Chafik D., Kim H.M., Galatz L.M., Yamaguchi K. Insertional anatomy of the triceps brachii tendon. J Shoulder Elbow Surg. 2010;19:399–405. doi: 10.1016/j.jse.2009.10.008. [DOI] [PubMed] [Google Scholar]
- 11.Khiami F., Tavassoli S., De Ridder Baeur L., Catonne Y., Sariali E. Distal partial ruptures of triceps brachii tendon in an athlete. Orthop Traumatol Surg Res. 2012;98:242–246. doi: 10.1016/j.otsr.2011.09.022. [DOI] [PubMed] [Google Scholar]
- 12.Madsen M., Marx R.G., Millett P.J., Rodeo S.A., Sperling J.W., Warren R.F. Surgical anatomy of the triceps brachii tendon: anatomical study and clinical correlation. Am J Sports Med. 2006;34:1839–1843. doi: 10.1177/0363546506288752. [DOI] [PubMed] [Google Scholar]
- 13.Moritomo H., Tada K., Yoshida T., Kawatsu N. Reconstruction of the coronoid for chronic dislocation of the elbow. Use of a graft from the olecranon in two cases. J Bone Joint Surg Br. 1998;80:490–492. doi: 10.1302/0301-620x.80b3.8328. [DOI] [PubMed] [Google Scholar]
- 14.Murray W.M., Delp S.L., Buchanan T.S. Variation of muscle moment arms with elbow and forearm position. J Biomech. 1995;28:513–525. doi: 10.1016/0021-9290(94)00114-j. [DOI] [PubMed] [Google Scholar]
- 15.O'Driscoll S.W. Arthroscopic treatment for osteoarthritis of the elbow. Orthop Clin North Am. 1995;26:691–706. [PubMed] [Google Scholar]
- 16.Shahane S.A., Stanley D. A posterior approach to the elbow joint. J Bone Joint Surg Br. 1999;81:1020–1022. doi: 10.1302/0301-620x.81b6.9696. [DOI] [PubMed] [Google Scholar]
- 17.Studer A., Athwal G.S., MacDermid J.C., Faber K.J., King G.J. The lateral para-olecranon approach for total elbow arthroplasty. J Hand Surg Am. 2013;38:2219–2226. doi: 10.1016/j.jhsa.2013.07.029. e2213. [DOI] [PubMed] [Google Scholar]
- 18.Tagliafico A., Gandolfo N., Michaud J., Perez M.M., Palmieri F., Martinoli C. Ultrasound demonstration of distal triceps tendon tears. Eur J Radiol. 2012;81:1207–1210. doi: 10.1016/j.ejrad.2011.03.012. [DOI] [PubMed] [Google Scholar]
- 19.van Riet R.P., Morrey B.F., Ho E., O'Driscoll S.W. Surgical treatment of distal triceps ruptures. J Bone Joint Surg Am. 2003;85-A:1961–1967. doi: 10.2106/00004623-200310000-00015. [DOI] [PubMed] [Google Scholar]
- 20.Yeh P.C., Stephens K.T., Solovyova O., Obopilwe E., Smart L.R., Mazzocca A.D. The distal triceps tendon footprint and a biomechanical analysis of 3 repair techniques. Am J Sports Med. 2010;38:1025–1033. doi: 10.1177/0363546509358319. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Other anatomic measurements are considered. The width and height and distal extension of the lateral retinaculum were measured as follows (Fig. S1): The height was considered as the distance from the posterolateral corner of the olecranon to the point where it blended with the triceps. The width was considered as the distance from the posterolateral corner of the olecranon to the most lateral aspect of the lateral retinaculum with 90° of elbow flexion. The fibers of the distal extension of the lateral retinaculum were blended with the forearm fascia but were considered as extending over the anconeus to its insertion in the ulna (Table I).
Posterior approach to the elbow with exposed triceps extensor mechanism. Superficially, the fibers of the medial head of the triceps appear to insert obliquely into the most medial aspect of the triceps tendon. The lateral expansion of the triceps can extend laterally significantly.
Lateral view of a right elbow. The lateral reticnaculum of the triceps is seen merging its fibers proximally with the triceps tendon proper and distally with fibers of the extensor carpi ulnaris. The lateral retinaculum has been released according to a Kocher approach to the lateral elbow. The width, length, and proximal extension were considered as shown in the photograph before any release.