

Abstract
Background and Aim:
Treatment outcomes in bipolar disorder are highly variable, and several sociodemographic, clinical characteristics, and comorbidities play an important role. Early recognition of these factors will help the physicians to implement individualized treatment and a better clinical outcome. The present study was aimed at identifying the factors affecting treatment outcomes in bipolar disorder.
Materials and Methods:
All patients diagnosed with bipolar disorder as per diagnostic and statistical manual-IV criteria were included in the study. Patients were followed for 6 months from the day of enrollment. Patient demography, age at bipolar disorder was diagnosed, age at treatment was started, social habits, signs and symptoms, comorbidities, symptoms, treatment pattern, and compliance to treatment were recorded in case record form. Based on the changes in young mania rating scale and Hamilton Depression Rating Scale (HAM-D) score from baseline to last follow-up, the patients were classified as remission and non-remission. Multiple logistic regression was used to identify risk factors associated nonremission in bipolar disorder patients and calculation of odds ratio (OR).
Results:
The mean age of the study population was 37.6 ± 14.1 years. Out of the 121 patients, 68 (56.2%) were female. At the end of the follow-up period, 41 (33.9%) had remission, and 80 (66.1%) had nonremission. Early onset (OR: 9.77; confidence intervals [CI]: 1.77–86.01), treatment delay (OR: 6.48; CI: 1.27–32.92), treatment noncompliance (OR: 4.64; CI: 1.37–15.64), and single living (OR: 4.26; CI: 1.56–11.66) were independently associated with nonremission in bipolar disorder patients.
Conclusions:
Early-onset bipolar disorder, delay in treatment, treatment non-compliance, and single living adversely affect remission in bipolar disorder.
Keywords: Bipolar disorder, early onset, Hamilton Depression Rating Scale, remission, young mania rating scale
INTRODUCTION
Bipolar disorder is one of the most common psychiatric illnesses with cyclic changes in mood from mania or hypomania to depression or vice versa. In bipolar disorder, the patient's cognitive and behavioral abilities are affected, at work or school as well as daily chores in the household.[1] The symptoms, course, severity, and response to treatment vary among individual patients.
Alcohol and substance abuse is common among patients with bipolar disorder and can have a significant impact on the age of onset, course of the illness, and response to treatment.[2] Bipolar disorder is highly misdiagnosed at times, which leads to comorbid conditions and delayed treatment of the same. Due to this, bipolar disorder is often hard to treat and leaves the patient with prolonging disabilities such as unemployment and mental retardation. If left untreated, there is an increased risk of suicide, morbidity, and mortality.[1] Furthermore, the treatment outcomes in bipolar disorder are highly variable, and the treatment must be individualized as the clinical presentation, severity, and frequency of episodes vary widely among each patient. Early recognition of the factors affecting the treatment outcome will help the treating physicians to early implementation of individualized treatment and a better clinical outcome.
In the present study, demographics, treatment pattern, clinical characteristics, comorbidities, bipolar disorder severity scores, and treatment outcomes were assessed to identify the factors affecting treatment outcome in bipolar disorder patients.
MATERIALS AND METHODS
Participants
A prospective cohort study was conducted between August 2016 and February 2017 in a tertiary care teaching hospital located in Manipal, India. The Institutional Ethics Committee approval was obtained before the study. All newly diagnosed bipolar disorder patients as per diagnostic and statistical manual-IV criteria or previously diagnosed bipolar disorder patients but not on treatment and who are willing to participate in the study were enrolled. The patients were followed for 6 months from the day of enrollment. Patients who are not willing to undergo treatment, without clear treatment outcome as remission or nonremission and patients who lost the follow-up were excluded from the study. Patient demography, age at bipolar disorder was diagnosed, age at treatment was started, social habits, signs and symptoms, medical and psychiatric comorbidities, treatment paten, and compliance to treatment were recorded in predesigned case record form.
Outcome measures
The Young mania rating scale (YMRS) and Hamilton Depression Rating Scale (HAM-D) scores were used to measure the severity of manic episodes and depression, respectively, in the study population, at baseline, and at last follow-up. YMRS and HAM-D were assessed by expert psychiatrists in the presence of the investigator. Based on the changes in YMRS and HAM-D scores from baseline to the last follow-up, the patients were classified into remission and nonremission.
Definitions
Early onset is defined as bipolar disorder diagnosed before 18 years of age.[3]
Remission is described as that clinical stage wherein the patient does not exhibit any symptoms of mania or depression with a YMRS ≤12 and HAM-D score of seven or less.[4,5]
Nonremission is that clinical stage where the patient exhibits signs and symptoms of mania or depression irrespective of being on prescribed medication.[6]
Low-income group is defined, as total annual household income is between 1 and 2 lakh.[7]
The single living is defined as unmarried, widowed or divorced condition and living separately.
Treatment delay is defined as when the interval between the onset of bipolar disorder and its first treatment is >6 years.[8]
Statistical analyses
Nominal data were described and expressed in frequency and percentage. Parametric data were expressed as the mean ± standard deviation (SD). Comparison of YMRS/HAM-D scores at baseline and last follow-up was done using paired t-test. Multiple logistic regression was used to identify risk factors associated with nonremission in bipolar disorder patients and calculation of odds ratio (OR). In multiple logistic regression, factors were selected based on published literatures and clinical relevance as judged by expert clinicians. Factors having less than adequate number of events (<10) per independent variable were not included in the multiple logistic regression analysis. P <0.05 was considered as statistically significant for all analyses. Data entry and statistical analysis were done using IIBM SPSS version 20.0 (IBM Corp. IBM SPSS Statistics for Windows, Armonk, NY).
RESULTS
Study population characteristics
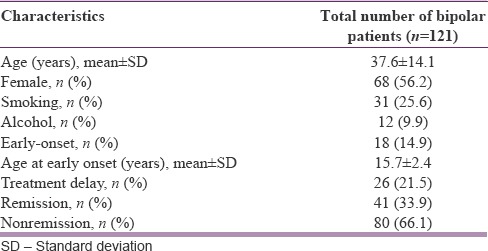
During the study period, 121 bipolar disorder patients were enrolled in the study based inclusion criteria. Patient demography, age at onset, treatment outcome, and other details are summarized in Table 1. The average age of the study population was 37.6 ± 14.1 years (mean ± SD), and 56.2% (n = 68) of the patients were female. Early-onset bipolar disorder was seen in 14.9%, (n = 18) and the mean age at early-onset bipolar disease was 15.7 ± 2.4 (mean ± SD) years. Treatment delay was observed in 21.5% (n = 26) of patients. At the end of the follow-up period, 33.9% (n = 41) had remission and 66.1% (n = 80) had nonremission.
Table 1.
Demography, clinical characteristics and outcome of bipolar patients
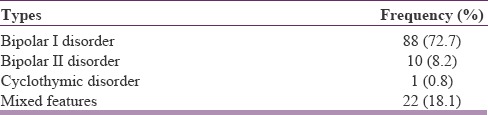
Subtypes of bipolar disorder based on specific mood episodes are summarized in Table 2, majority of the patients (72.7%, n = 88) were diagnosed with Bipolar I disorder, followed by Bipolar II disorder (8.2%, n = 10), cyclothymic disorder (0.8%, n = 1), and mixed features (18.1%, n = 22).
Table 2.
Types of bipolar disorder
Severity scores in study population
Mean YMRS and HAM-D scores among remission and nonremission group at the last follow-up are shown in Table 3. There was a statistically significant (at P < 0.01), 67.5% reduction in YMRS and 70.0% reduction HAM-D score compared to baseline whereas in nonremission group, reduction in YMRS and HAM-D score was not significant.
Table 3.
Bipolar disorder severity scores among remission and nonremission group

Drug treatment pattern among the study population is shown in Table 4. Antipsychotics (62.8%, n = 76) were the most the most commonly prescribed agents followed by antidepressant (55.4%, n = 67). However, remission (41.3%, n = 19) was more in patient who were treated with mood stabilizers (lithium salts) compared to anticonvulsants (31.8%, n = 21) and antipsychotics (30.3%, n = 23).
Table 4.
Different type of treatment in bipolar disorder patients

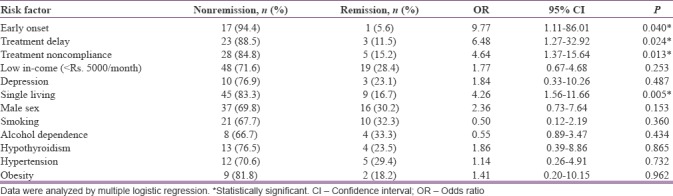
The results of multiple logistic regression are summarized in Table 5. Twelve variables were analyzed to identify the possible association with nonremission in the study population. Early onset (OR: 9.77; confidence intervals [CI]: 1.11–86.01), treatment delay (OR: 6.48; CI: 1.27–32.92) treatment noncompliance (OR: 4.64; CI: 1.37–15.64), and single living (OR: 4.26; CI: 1.56–11.66) were independently associated with nonremission in bipolar disorder patients. Other variables, namely low income, depression, male sex, hypothyroidism, hypertension, and obesity also had OR >1; however, they were not statistically significant. Smoking and alcoholism shown to favor remission but again results were statistically nonsignificant.
Table 5.
Identification of factors associated nonremission in bipolar disorder patients
DISCUSSION
In this study, 121 bipolar disorder patients were followed for 6 months from the day of enrollment into the study. As per our knowledge and literature search, it is the first study attempted to identify the factors leading to nonremission in bipolar disorder patients.
The mean age of our study population was 37.6 ± 14.1 years with female predominance; (56.2%) these observations were similar to the results published in a study conducted by Perry et al., in that study, the mean age was 43 ± 15 years with female patients being 68%.[9] The incidence of bipolar disorder is more in female gender may be due to their lifestyle or physiological effects. A study conducted by Leibenluft showed that women are more prone to suffering from bipolar disorder as compared to men.[10]
In our study population, 14.9% had the early-onset bipolar disorder and mean age at early onset was 15.7 ± 2.4. Early-onset bipolar disorder is most common, in a study conducted by Post et al. 50% of the patient had early-onset disease.[11] According to the American Psychiatric Association and according to Wells et al., the average age of the onset of first manic episode is about 21 years, our results also showed a similar pattern.[1]
According to a study conducted by McGlashan, it showed that with the passing of adolescence, the disorder becomes less penetrating with respect to virulence. Conversely, late-developing mania or late onset of illness, even if it is mild, may be devastating to someone with established rigid, defensive styles and less adaptive flexibility.[12]
Treatment delay and implications: According to Post et al., treatment delay occurs when the patient starts his/her medication much after the disorder is diagnosed. This can cause resistance to drugs and positive outcome with the treatment would be affected.[11]
In our study, bipolar disorder Type I has found to be more common although there is no substantial literature support. This may be due to the smaller sample size of our study. Although studies have suggested that bipolar disorder Type I is more severe and acute when compared to the other types while bipolar Type II patients have a more chronic course of treatment, significantly more depressive episodes, and shorter periods of being well between episodes than patients with bipolar disorder I, also there is a high risk for suicide.[13]
A wide range of medical comorbidities have been observed in various studies on bipolar population. According to Kupfer, the most common being cardiovascular disease, obesity, and diabetes mellitus.[14] Literature by Fagiolini et al. showed that 49% suffered from abdominal obesity, suggesting that metabolic disorders are risky and very high in the prevalence of bipolar patients.[15] F, according to McElroy et al., obesity in bipolar disorder may be due to factors such as age, gender, binge eating problems, income level, psychotropic drugs that cause weight gain, geographical location, and health habits.[16]
There was a statistically significant (at P < 0.01), 67.5% reduction in YMRS and 70.0% reduction HAM-D score compared to baseline, A study conducted by Kauer-Sant’Anna et al. reported 34% functionality recovery in 6 months, in patients with a first psychotic episode, 33% of those had functional recovery after 3 years of follow-up.[17]
Medications prescribed for bipolar disorder, in our study, showed that 76 (62.8%) patients prescribed with atypical antipsychotics, 67 (55.4%) patients were given antidepressants. Surprisingly, antipsychotic agents were used more frequently than mood stabilizers. A study conducted by Blanco et al. showed that there had been a decrease in the use of mood stabilizers and an increase in the use of atypical antipsychotics and anticonvulsants particularly valproates. Antipsychotics are being prescribed more often now for manic and mixed type of episodes. They have lesser side effects and do not produce extrapyramidal syndrome. Antidepressants are commonly prescribed in the absence of mood stabilizers.[18]
Risk factors associated nonremission found to have a significant effect were early onset, treatment delay, noncompliance, and single living. Noncompliance is seen in all age groups. The reason for this is polypharmacy, forgetfulness, and lack of education regarding the illness. According to Colom et al. noncompliance leads to increase the risk of relapse, decrease in quality of life, increase in symptoms, and more suicidal attempts. About 20%–60% of bipolar patients are noncompliant. One-third of the bipolar patients do not consume 70% of their medication. This leads to increase relapse rates causing the poor outcome.[19]
Another significant risk factor found in our study was marital status, more specifically the unmarried, separated and widowed patients. According to Yoshimasu et al. and Krishnan, this may be because of lack of family support leading to depression, substance abuse, suicide attempts. Unmarried, separated, and widowed patients socially isolate themselves. A lack of family and social support leads to an increase in suicidal attempts.[20,21]
CONCLUSIONS
It is known that the outcome of bipolar disorder treatment is highly variable and several patients and environmental-related factors may affect the outcome. The identified factors may be used as a clinical decision supporting tool and addressing these factors in the early phase of treatment may reduce the chances of nonremission in bipolar disorder patients and improve their quality of life.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Manipal College of Pharmaceutical Sciences, Kasturba Hospital and Manipal Academy of Higher Education for supporting this study.
REFERENCES
- 1.Wells B, Dipiro J, Schwinghammer T, Dipiro C. Pharmacotherapy Handbook. 9th ed. New York: McGraw-Hill Education; 2015. [Google Scholar]
- 2.Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord. 2000;2:269–80. doi: 10.1034/j.1399-5618.2000.20308.x. [DOI] [PubMed] [Google Scholar]
- 3.James J. Early-onset bipolar disorder. In: Skuse D, Bruce H, Dowdney L, Mrazek D, editors. Child Psychology and Psychiatry. 2nd ed. London (UK): Wiley-Blackwell; 2011. pp. 223–16. [Google Scholar]
- 4.Patel NC, Patrick DM, Youngstrom EA, Strakowski SM, Delbello MP. Response and remission in adolescent mania: Signal detection analyses of the young mania rating scale. J Am Acad Child Adolesc Psychiatry. 2007;46:628–35. doi: 10.1097/chi.0b013e3180335ae4. [DOI] [PubMed] [Google Scholar]
- 5.Israel JA. Remission in depression: Definition and initial treatment approaches. J Psychopharmacol. 2006;20:5–10. doi: 10.1177/1359786806064306. [DOI] [PubMed] [Google Scholar]
- 6.Bulloch AG, Patten SB. Non-remission of depression in the general population as assessed by the HAMD-7 scale. Depress Anxiety. 2008;25:393–7. doi: 10.1002/da.20396. [DOI] [PubMed] [Google Scholar]
- 7.Economically Weaker Sections. New Delhi: Arthapedia; 2016. [Last accessed on 2018 Jul 23]. Available from: http://www.arthapedia.in/index.php?title=Economically_Weaker_Sections_(EWS) [Google Scholar]
- 8.Dagani J, Signorini G, Nielssen O, Bani M, Pastore A, Girolamo G, et al. Meta-analysis of the interval between the onset and management of bipolar disorder. Can J Psychiatry. 2017;62:247–58. doi: 10.1177/0706743716656607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Perry A, Tarrier N, Morriss R, McCarthy E, Limb K. Randomised controlled trial of efficacy of teaching patients with bipolar disorder to identify early symptoms of relapse and obtain treatment. BMJ. 1999;318:149–53. doi: 10.1136/bmj.318.7177.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leibenluft E. Women with bipolar illness: Clinical and research issues. Am J Psychiatry. 1996;153:163–73. doi: 10.1176/ajp.153.2.163. [DOI] [PubMed] [Google Scholar]
- 11.Post RM, Leverich GS, Kupka RW, Keck PE, Jr, McElroy SL, Altshuler LL, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71:864–72. doi: 10.4088/JCP.08m04994yel. [DOI] [PubMed] [Google Scholar]
- 12.McGlashan TH. Adolescent versus adult onset of mania. Am J Psychiatry. 1988;145:221–3. doi: 10.1176/ajp.145.2.221. [DOI] [PubMed] [Google Scholar]
- 13.Berger F. Bipolar Disorder. Baltimore, MD: University of Maryland Medical Center; 2017. [Last accessed on 2018 Jul 21]. Avaialble from: https://www.umms.org/ummc/patients-visitors/health-library/in-depth-patient-education-reports/articles/bipolar-disorder . [Google Scholar]
- 14.Kupfer DJ. The increasing medical burden in bipolar disorder. JAMA. 2005;293:2528–30. doi: 10.1001/jama.293.20.2528. [DOI] [PubMed] [Google Scholar]
- 15.Fagiolini A, Frank E, Scott JA, Turkin S, Kupfer DJ. Metabolic syndrome in bipolar disorder: Findings from the bipolar disorder center for pennsylvanians. Bipolar Disord. 2005;7:424–30. doi: 10.1111/j.1399-5618.2005.00234.x. [DOI] [PubMed] [Google Scholar]
- 16.McElroy SL, Frye MA, Suppes T, Dhavale D, Keck PE, Jr, Leverich GS, et al. Correlates of overweight and obesity in 644 patients with bipolar disorder. J Clin Psychiatry. 2002;63:207–13. doi: 10.4088/jcp.v63n0306. [DOI] [PubMed] [Google Scholar]
- 17.Kauer-Sant’Anna M, Bond DJ, Lam RW, Yatham LN. Functional outcomes in first-episode patients with bipolar disorder: A prospective study from the systematic treatment optimization program for early mania project. Compr Psychiatry. 2009;50:1–8. doi: 10.1016/j.comppsych.2008.05.013. [DOI] [PubMed] [Google Scholar]
- 18.Blanco C, Laje G, Olfson M, Marcus SC, Pincus HA. Trends in the treatment of bipolar disorder by outpatient psychiatrists. Am J Psychiatry. 2002;159:1005–10. doi: 10.1176/appi.ajp.159.6.1005. [DOI] [PubMed] [Google Scholar]
- 19.Colom F, Vieta E, Tacchi MJ, Sánchez-Moreno J, Scott J. Identifying and improving non-adherence in bipolar disorders. Bipolar Disord. 2005;7(Suppl 5):24–31. doi: 10.1111/j.1399-5618.2005.00248.x. [DOI] [PubMed] [Google Scholar]
- 20.Yoshimasu K, Kiyohara C, Miyashita K Stress Research Group of the Japanese Society for Hygiene. Suicidal risk factors and completed suicide: Meta-analyses based on psychological autopsy studies. Environ Health Prev Med. 2008;13:243–56. doi: 10.1007/s12199-008-0037-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Krishnan KR. Psychiatric and medical comorbidities of bipolar disorder. Psychosom Med. 2005;67:1–8. doi: 10.1097/01.psy.0000151489.36347.18. [DOI] [PubMed] [Google Scholar]