

Abstract
Background:
Considerable research links threat-related attention biases to anxiety symptoms in adults, whereas extant findings on threat biases in youth are limited and mixed. Inconsistent findings may arise due to substantial methodological variability and limited sample sizes, emphasizing the need for systematic research on large samples. The aim of this report is to examine the association between threat bias and pediatric anxiety symptoms using standardized measures in a large, international, multi-site youth sample.
Methods:
A total of 1,291 children and adolescents from seven research sites worldwide completed standardized attention bias assessment task (dot-probe task) and child anxiety symptoms measure (Screen for Child Anxiety Related Emotional Disorders). Using a dimensional approach to symptomatology, we conducted regression analyses predicting overall, and disorder-specific, anxiety symptoms severity, based on threat bias scores.
Results:
Threat bias correlated positively with overall anxiety symptoms severity (ß = 0.078, P = .004). Furthermore, threat bias was positively associated specifically with social anxiety (ß = 0.072, P = .008) and school phobia (ß = 0.076, P = .006) symptoms severity, but not with panic, generalized anxiety, or separation anxiety symptoms. These associations were not moderated by age or gender.
Conclusions:
These findings indicate associations between threat bias and pediatric anxiety symptoms, and suggest that vigilance to external threats manifests more prominently in symptoms of social anxiety and school phobia, regardless of age and gender. These findings point to the role of attention bias to threat in anxiety, with implications for translational clinical research. The significance of applying standardized methods in multi-site collaborations for overcoming challenges inherent to clinical research is discussed.
Keywords: anxiety/anxiety disorders, biological markers, child/adolescent, computer/internet technology, GAD/generalized anxiety disorder, international, phobia/phobic disorders, SAD/social anxiety disorder/social phobia, separation anxiety
1. INTRODUCTION
Pediatric anxiety disorders are common and associated with negative outcomes, including adult anxiety, clinical comorbidity, and compromised daily functioning (Bittner et al., 2007; Rapee, Schniering, & Hudson, 2009). Identifying cognitive correlates of pediatric anxiety may inform diagnosis and treatment (Pine & Fox, 2015; Pine, Helfinstein, Bar-Haim, Nelson, & Fox, 2009). In adults, considerable research links threat-related attention biases to anxiety, with some evidence suggesting their role in causing and maintaining anxiety (Armstrong & Olatunji, 2012; Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg, & van IJzendoorn, 2007; MacLeod & Mathews, 2012). Although anxiety typically emerges in youth (Kessler, Chiu, Demler, Merikangas, & Walters, 2005), threat biases in this age group have been studied less extensively. The limited extant findings suggest the presence of threat bias in anxious youth, but to a lesser extent than in anxious adults, and with results often being inconsistent (Bar-Haim et al., 2007; Dudeney, Sharpe, & Hunt, 2015).
Inconsistent findings regarding associations between threat bias and pediatric anxiety symptoms may be due to methodological inconsistencies across studies, such as large variability in bias measurement paradigms and task parameters (Bantin, Stevens, Gerlach, & Hermann, 2016; Bar-Haim et al., 2007; Dudeney et al., 2015). Such variability limits comparability between studies and reduces statistical power to reveal expected effects, particularly such that may be subtle, thereby emphasizing the need for standardizing tasks across samples and studying large participant pools. Here, we applied a standardized, multi-site approach by aggregating data from different research sites that employed identical measures, for the purpose of examining the association between attention bias to threat and pediatric anxiety symptoms in a large, international youth sample.
Studies based on large, heterogeneous samples may also identify factors that moderate the association between threat bias and pediatric anxiety symptoms. Some evidence indicates that the expression of threat bias may change with age, possibly reflecting a developmental trajectory in threat-related information processing biases in anxiety (Beesdo, Knappe, & Pine, 2009; Dudeney et al., 2015; Field & Lester, 2010). Thus, threat bias-anxiety findings from studies sampling only a specific age range may not necessarily translate to other ages. Similarly, there is some evidence to suggest gender differences in the expression of attention bias to threat, although extant results are mixed (Dudeney et al., 2015; Pintzinger, Pfabigan, Pfau, Kryspin-Exner, & Lamm, 2017; Sass et al., 2010). In addition, clinical features may moderate the findings, though few studies have tested this possibility (Pergamin-Hight, Naim, Bakermans-Kranenburg, van IJzendoorn, & Bar-Haim, 2015). Specifically, most studies examining threat bias in anxiety recruit participants with mixed anxiety features, but use stimuli which may be perceived as threatening to only specific anxiety categories (Dudeney et al., 2015; Pergamin-Hight et al., 2015; Salum et al., 2013; Waters, Bradley, & Mogg, 2014). For example, threat bias may emerge among individuals with social anxiety only in response to socially-meaningful stimuli, such as facial expressions. Large samples may facilitate elucidating such specificity. Finally, large sample sizes increase replicability and generalizability of findings, and confidence in reported outcomes (e.g., Asendorpf et al., 2013). Thus, there is a need to examine the association between threat bias and pediatric anxiety symptoms in large samples.
The aim of the current study is to complement and extend previous research by establishing associations between pediatric anxiety symptoms and attention bias to threat-related social stimuli. To this end, we analyzed data aggregated from seven international research sites taking part in the Tel Aviv University-National Institute of Mental Health Attention Bias Modification (TAU-NIMH ABM) Initiative, a collaborative effort aiming to increase standardization and comparability of attention bias research across laboratories (Abend, Pine, & Bar-Haim, 2014). Our large participant pool (N = 1291) represents a mixed, heterogeneous sample of youth aged 6–18 years reporting a wide range of anxiety symptoms. As part of the TAU-NIMH ABM Initiative, all participants completed an identical variant of a dot-probe task (featuring angry and neutral face stimuli presented for 500 ms) for assessment of threat bias in early attention orienting (Bar-Haim et al., 2007; Cisler & Koster, 2010). We thus used the most often-applied attention bias paradigm using stimuli appropriate for youth participants across ages. Across all participants, anxiety symptoms were assessed using the Screen for Child Anxiety Related Emotional Disorders (SCARED; Birmaher et al., 1999), which captures overall anxiety symptoms as well as symptoms of specific subtypes of anxiety (panic, generalized anxiety, social anxiety, separation anxiety, and school phobia). Following a dimensional approach to data analysis, we examined continuous associations between threat bias and symptom severity for the different anxiety sub-categories across the sample as a whole (Cuthbert, 2015; Cuthbert & Insel, 2013), as well as potential demographic moderators of these associations (Beesdo et al., 2009). We hypothesized that threat bias scores would be positively associated with overall anxiety symptom severity, as well as specifically with social anxiety severity (due to the use of social threat stimuli).
2. METHODS
The results reported here are based on data aggregated from several international research sites taking part in the TAU-NIMH ABM Initiative (Abend et al., 2014). Although each site may have tested specific hypotheses and collected specific measures of interest, core measures collected were consistent across sites. These included participant age and gender, the dot-probe threat bias task, and the SCARED questionnaire to assess anxiety symptoms, all used in the analyses described below.
2.1. Participants
The current report is based on data of 1,291 participants aged 6–18 years (M = 13.5 years, SD = 2.3; 725 females) from seven international sites. All sites tested the clinical efficacy of an Attention Bias Modification (ABM) procedure for anxiety (Abend et al., 2014), and collected attention bias and SCARED data at baseline before treatment initiated. Generally, all participants had to satisfy the following criteria to be included in the aggregated sample: (i) have complete attention bias score data; (ii) have complete SCARED (total and subscale scores) data; and (iii) be between 6 to 18 years of age. Overall, sampling included non-selected youth, high trait anxiety youth, and treatment-seeking anxiety patients, ensuring a broad range of anxiety symptoms severity (see below). Specific inclusion/exclusion criteria for each site, as well as additional information, are detailed in the supplementary material. Some of the sites have previously published the attention bias and anxiety severity data for some of their respective participants as pre-treatment mean threat bias and anxiety scores, and as correlations between these two measures (de Voogd et al., 2016; Fitzgerald, Rawdon, & Dooley, 2016; Morales, Taber-Thomas, & Pérez-Edgar, 2017; White, Britton et al., 2016; White, Sequeira et al., 2017).
The sites differed in terms of age, F(6,1284) = 451.83, P < .001, gender, 𝜒2(6) = 22.70, P < .001, and baseline SCARED scores (total and all subscale scores), Fs(6,1284) > 13.48, Ps < .001, and thus sites were entered as covariates in analyses (described below). Mean attention bias scores did not differ across sites, F(6,1284) = 0.33, P = .92. In each site, the study was performed in compliance with the Code of Ethics of the World Medical Association (Declaration of Helsinki), approved by the local Institutional Review Board, and, prior to participation, informed consent and assent were obtained from parents and youth, respectively.
2.2. Attention bias assessment
Attention bias to threat was assessed at all sites using the same variant of the visual dot-probe task (Abend et al., 2014; MacLeod, Mathews, & Tata, 1986) similar to the paradigm used in previous studies of pediatric anxiety (Pergamin-Hight, Pine, Fox, & Bar-Haim, 2016). Each trial in the task (Figure 1) began with a fixation cross displayed for 500 ms presented at the center of the screen. Next, a pair of faces, one angry and one neutral, were presented (500 ms), followed by a target probe (< or >) that appeared at the location vacated by one of the faces and presented until response. Using a button-press, participants were instructed to identify the probe type as quickly as possible without compromising accuracy. A new trial began after a 500-ms inter-trial interval.
FIGURE 1.
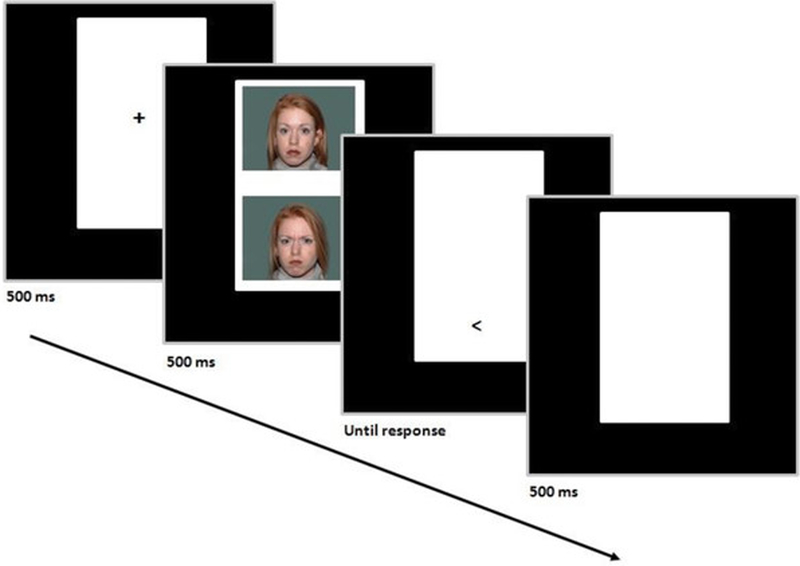
Sequence of events in a single dot-probe task trial; in this case, an angry–neutral trial in which the probe replaces the angry face (angry trial)
Note: ms = millisecond.
A total of 120 trials were used in the task. Of those, 80 trials included angry–neutral face pairs (AN) and 40 trials included neutral– neutral (NN) face pairs. The locations of the angry face and the probe were counterbalanced throughout the experiment. This number of trials was chosen in order to strike a balance between task length and stability, particularly among children, who may find it difficult to adequately sustain attention over time. The task was programmed using either E-Prime (Psychology Software Tools, Sharpsburg, PA) or Adobe Flash (ActionScript 3.0) software.
The cue stimuli in the task were face photographs of 20 different actors (10 male, 10 female) taken from the NimStim stimulus set (Tottenham et al., 2009). Two different pictures of each actor were selected, depicting angry and neutral expressions. The task used face stimuli, as these are deemed suitable across ages. Each face was placed on a greenish background subtending 45 mm in width and 34 mm in height. Participants were presented with pairs of faces of the same actor (AN or NN). The face photographs were presented with equal distance to the top and bottom of the fixation cross, with a distance of 14 mm between them. The top photograph was positioned about 20 mm from the top edge of the screen. Throughout the session trials, the screen background was black, whereas the photographs were surrounded by a single 58 mm wide by 94 mm tall white rectangle denoting the general area of the screen on which to focus.
A common method for data preparation was used in all sites (Abend et al., 2014). Prior to bias scores calculation, and in accord with common practice for tasks relying on reaction time (RT) data, all trials in which participants appeared not to adhere to standard task requirements were removed. Specifically, trials with incorrect responses or trials in which RT was very short (<150 ms, reflecting anticipatory response) or long (>2,000 ms, reflecting possible lapses in task performance) were excluded. Then, outlier trials in which RT was outside ±2.5 standard deviations of the participant’s mean were also excluded. Attention bias scores were computed by subtracting the mean RT in trials where probes replaced angry faces from the mean RT in trials where probes replaced neutral faces. Positive bias scores reflect a bias toward threat; negative scores reflect a bias away from threat. To maximize the signal in detecting threat biases in the context of clinical ABMT trials for anxiety, the attention bias assessment variant used by the participating sites did not include positive stimuli.
2.3. Anxiety symptoms
Youth anxiety symptoms were assessed using the SCARED, a self-rating of pediatric anxiety symptoms found to be valid and reliable in clinical and nonclinical populations (Birmaher et al., 1999; Muris, Merckelbach, Ollendick, King, & Bogie, 2002). The SCARED is composed of 41 items, and participants rate the extent to which each item is true using a 3-point scale (from 0 = “never true” to 2 = “very true or often true”). Total SCARED scores were calculated by summing all item-level scores; higher scores reflect higher overall anxiety symptom severity. The range of SCARED scores in this sample was 0–78 points (out of 82 points), indicating that virtually the entire span of the scale was covered. In addition, different SCARED items were also summed to comprise five anxiety subscales: panic, generalized anxiety, social anxiety, separation anxiety, and school phobia (Birmaher et al., 1999). All subscales were significantly correlated (see Supporting Information Table S1). The parent-report version of the SCARED was not administered in some sites to minimize participant burden. The SCARED has been adequately translated and back-translated before being administered in each site.
2.4. Data analysis
We performed two primary types of analyses. First, we tested whether attention bias to threat predicted overall anxiety symptoms severity, beyond age and gender as well as in interaction with these two factors. To this end, we conducted a hierarchical multiple regression analysis using total SCARED scores as the dependent variable. The first step included age and gender as predictors, the second step added attention bias score, the third step added the Age x bias and Gender x bias interaction terms, and a fourth step added the Age x Gender x bias term. A significance level of 𝛼= 0.05 was used to detect effects. All tests were two-tailed.
Second, we examined whether attention bias to threat specifically predicted different anxiety subtypes. To this end, we conducted five separate hierarchical multiple regression analysis, each predicting one of the five SCARED subscales (panic, generalized anxiety, social anxiety, separation anxiety, and school phobia), using the same hierarchical structure described above for the total score. To correct for potential type I error inflation in these analyses, a significance level of 𝛼/5 = 0.01 was used to detect effects.
Due to differences in age, gender and anxiety symptoms between the seven sites providing data, a series of six binary (dummy) variables coding for site was created. The above analyses were repeated with these variables added to the first step of the models, to adjust for the effect of specific sites on the results. The addition of these variables did not change the significance of any of the models tested.
As supplementary analyses, the effects above were also examined using linear mixed-effects multilevel analyses in which site was treated as a random-effects variable (rather than a fixed-effects variable), to more comprehensively account for potential site differences. This was performed using the ‘nlme’ package (Pinheiro & Bates, 2000) from R software (R Core Team, 2014).
For comparability with previous reports examining differences in threat bias between anxious and non-anxious groups, participants were also divided into three tertile groups based on total SCARED scores. Mean threat bias scores were then compared in this complementary analysis between these low-, moderate-, and high-symptom groups using a one-way analysis of variance (ANOVA).
Finally, in light of the notion that differences in mean RT between NN trials and threat and neutral trials may reflect vigilance to threat or difficulty disengaging from it, respectively (Koster, Crombez, Verschuere, & De Houwer, 2004), the primary analyses were repeated with these two components of the bias scores (NN-threat, NN-neutral) in place of the traditional bias score. In addition, differences between the symptom severity groups were examined using these measures.
3. RESULTS
See Table 1 for demographic information, mean measures of the dot-probe task, and SCARED scores for each site, and supplementary material for results pertaining to general task performance.
TABLE 1.
Age, gender, mean (and SD) measures of the dot-probetask, and SCARED scores (total and subscales), for each of the sites providing data
| Dot-probe task |
SCAREDscores |
||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Site | n | Age (Years) |
Gender (%females) |
Accuracy: all trials(%) |
RT: all trials(ms) |
RT: NN trials(ms) |
RT: neutral trials(ms) |
RT: threat trials(ms) |
Attentionbias score(ms) |
Total | Panic | Generalized anxiety |
Social anxiety |
Separation anxiety |
School phobia |
| UvA | 673 | 14.4(1.2) | 59.0 | 96 (5) | 524 (67) | 523 (69) | 525 (68) | 524 (69) | 1 (27) | 18.8 (12) | 3.3 (3.5) | 5.8 (4.3) | 2.7 (2.5) | 5.6 (3.6) | 1.5 (1.5) |
| PSU | 200 | 10.9(1.0) | 54.7 | 90 (12) | 604 (79) | 603 (79) | 606 (82) | 603 (83) | 3 (24) | 16.6 (12.2) | 3.2 (3.6) | 4.1 (3.6) | 3.9 (3.4) | 4.4 (3.6) | 1.1 (1.3) |
| UCD | 127 | 15.9(0.5) | 57.5 | 93 (8) | 501 (90) | 502 (91) | 502 (95) | 499 (89) | 3 (29) | 37.9 (13.1) | 8.5 (5.6) | 12.4 (3.9) | 4.4 (3.4) | 10.2 (2.7) | 2.4 (2.2) |
| NIMH | 122 | 12.9 (2.6) | 45.2 | 95 (6) | 591 (93) | 590 (91) | 591 (92) | 591 (94) | 0 (17) | 15.6 (14.1) | 2.9 (3.8) | 4.5 (4.9) | 2.8 (3.3) | 4.3 (4.2) | 1.2 (1.7) |
| UFRGS | 72 | 8.9 (1.6) | 53.2 | 87 (17) | 940 (261) | 936 (264) | 947 (262) | 944 (263) | 3 (60) | 32.6 (12.5) | 6.3 (4.6) | 8.7 (4.5) | 8.8 (3.3) | 6.9 (3.6) | 1.9 (1.9) |
| ZJU | 61 | 16.0 (0.0) | 68.9 | 97 (3) | 439 (44) | 437 (46) | 440 (43) | 440 (45) | 0 (18) | 37.2 (8.5) | 9.0 (4.0) | 11.3 (3.3) | 5.8 (3.3) | 8.7 (3) | 2.4 (1.8) |
| FIU | 36 | 11.2 (2.2) | 34.1 | 95 (4) | 696 (204) | 700 (196) | 708 (195) | 707 (208) | 1 (39) | 21.8 (14.9) | 4.6 (4.6) | 5.1 (4.5) | 5.2 (4.1) | 5.5 (3.7) | 1.3 (1.5) |
| Total | 13.4 (2.4) | 56.2 | 94 (8) | 566 (145) | 565 (145) | 568 (146) | 566 (147) | 2 (29) | 21.8 (14.4) | 4.2 (4.4) | 6.4 (4.8) | 3.6 (3.3) | 5.9 (3.9) | 1.5 (1.7) | |
Note: RT = reaction time; ms = millisecond; NN = neutral–neutral trials; neutral trials = neutral–angry trials in which the probe followed the neutral face; threat trials = neutral–angry trials in which the probe followed the angry face; UvA = University of Amsterdam, Netherlands; PSU = Pennsylvania State University, USA; UCD = University College Dublin, Ireland; NIMH = National Institute of Mental Health, USA; URFGS = Universidade Federal do Rio Grande do Sul,Brazil; ZJU = Zhejiang University, China; FIU = Florida International University, USA; SCARED = Screen for Child Anxiety Related Emotional Disorders.
Table 2 presents the results of the primary analyses: the multiple regression analysis predicting total SCARED scores and the five anxiety subscales scores. Significant models are presented in boldface, using 𝛼= 0.01 for subscales analyses. For ease, the presented results are for the analyses which did not include the binary variables coding for site. The addition of the third step (Age x bias and Gender x bias interaction terms) and the fourth step (Age x Gender x bias term) were not significant in any of the analyses, all R2< 0.01, Fs(2,1279) < 3.87, Ps > .02 (uncorrected), and thus the results of these models are not presented in the table.
TABLE 2.
Results of multiple regression analysis predicting total SCARED scores and scores for each of the five SCARED subscales. Significant models and predictors (𝛼≤ 0.01) are presented in boldface. Model 1 included participant age and gender as predictors; Model 2 added attention bias score as predictor; Model 3 added Age x bias and Gender x bias interaction terms; Model 4 added Age x Gender x bias; since in all analyses the addition of the third and fourth steps did not significantly explain more variance, these models are not presented here
| Total |
Panic |
Generalized anxiety |
||||
|---|---|---|---|---|---|---|
| Statistic | P-value | Statistic | P-value | Statistic | P-value | |
| Model 1 | F(2,1288) = 25.93 | <.001 | F(2,1288) = 22.20 | <.001 | F(2,1288) = 63.92 | <.001 |
| Age | ß = 0.113 | <.001 | ß = 0.106 | <.001 | ß = 0.247 | <.001 |
| Gender | ß =−0.151 | <.001 | ß =−0.139 | <.001 | ß =−0.149 | <.001 |
| Model 2 | F(3,1287) = 20.15 | <.001 | F(3,1287) = 16.55 | <.001 | F(3,1287) = 44.17 | <.001 |
| ΔR2= 0.01, F(1,1287) = 8.27 | .004 | ΔR2< 0.01, F(1,1287) = 5.12 | .024 | ΔR2< 0.01, F(1,1287) = 4.34 | .037 | |
| Age | ß = 0.113 | <.001 | ß = 0.016 | <.001 | ß = 0.247 | <.001 |
| Gender | ß = −0.150 | <.001 | ß = −0.138 | <.001 | ß = −0.149 | <.001 |
| Bias | ß = 0.078 | .004 | ß = 0.062 | .024 | ß = 0.052 | .037 |
|
Social anxiety |
Separation anxiety |
School phobia |
||||
| Statistic | P-value | Statistic | P-value | Statistic | P-value | |
| Model 1 | F(2,1288) = 35.55 | <.001 | F(2,1288) = 52.88 | <.001 | F(2,1288) = 18.77 | <.001 |
| Age | ß = 0.197 | <.001 | ß =−0.258 | <.001 | ß = 0.112 | <.001 |
| Gender | ß =−0.099 | <.001 | ß =−0.124 | <.001 | ß =−0.115 | <.001 |
| Model 2 | F(3,1287) = 26.19 | <.001 | F(3,1287) = 36.91 | <.001 | F(3,1287) = 15.16 | <.001 |
| ΔR2= 0.01, F(1,1287) = 7.13 | .008 | ΔR2< 0.01, F(1,1287) = 4.67 | .031 | ΔR2= 0.01, F(1,1287) = 7.78 | .006 | |
| Age | ß = 0.197 | <.001 | ß =−0.258 | <.001 | ß = 0.112 | <.001 |
| Gender | ß =−0.098 | <.001 | ß =−0.123 | <.001 | ß =−0.114 | <.001 |
| Bias | ß = 0.072 | .008 | ß = 0.058 | .024 | ß = 0.076 | .006 |
Note: SCARED = Screen for Childhood Anxiety Related Emotional Disorders.
When predicting total SCARED scores, the first model was significant. Likewise, all first models predicting anxiety subscales scores were significant. In all cases, age was positively associated with symptom severity, except for separation anxiety scores which were negatively associated with age; females reported greater symptom severity than males. The models adding attention bias scores remained significant in all analyses. However, the addition of this second step significantly explained more variance only when predicting total SCARED scores, and the social anxiety and school phobia subscales scores. In these models, attention bias was positively correlated with symptom severity. See Figure 2 for depiction of partial correlations between age, gender, and threat bias, and total SCARED scores. As noted, in all analyses, the addition of the third and fourth steps was not significant, suggesting that age and gender did not interact with attention bias when predicting any overall or category-specific anxiety symptoms.
FIGURE 2.
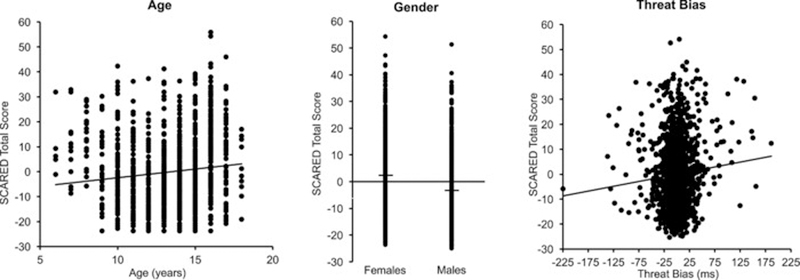
Scatterplots depicting the unique association between age, gender and threat bias, and total SCARED scores, based on the regression model predicting the latter variable. In each plot, SCARED scores are presented as residuals, controlling for the effects of the other predictors.
Note: SCARED= Screen for childhood Anxiety Relational Disorders.
For comparability with previous studies examining direct relations between threat bias and anxiety symptoms, we also calculated the zero-order correlations between bias scores and total and subscales scores of the SCARED, across the entire sample. Threat bias correlated positively and significantly with total SCARED scores, r = 0.080, P = .004, and with social anxiety, r = 0.073, P = .009, and school phobia, r = 0.078, P = .005, subscale scores. Correlations with other subscale scores were not significant, rs < 0.057, Ps > .022 (𝛼= 0.01 for multiple comparisons).
Multilevel analyses using site as a random effect replicated the primary results, showing that threat bias was significantly associated only with total SCARED scores, P = .004, social anxiety subscale scores, P = .008, and school phobia subscale scores, P = .006, whereas adjusting for age and gender. This indicates that the observed associations are present even when adjusting for the specific means and variance structures of each specific site, further attesting to the generalizability of the findings.
Next, we divided the current sample into three tertile anxiety-severity groups based on total SCARED scores: low (score ≤ 13), moderate (14–24), and high symptom-severity (≥25). SCARED scores of 22 and 25 have been suggested as sensitive and specific cutoffs for the detection of an anxiety disorder (Canals, Hernandez-Martinez, Cosi, & Domenech, 2012; Desousa, Salum, Isolan, & Manfro, 2013); thus, participants in the high severity group had scores that are considered clinically indicative of an anxiety disorder. See Supporting Information Table S2 in supplementary material for accuracy and RT information per group. One-way ANOVA on threat bias scores with Group (low, moderate, high severity) as a between-subjects factor revealed a significant main effect of Group, F(2,1288) = 3.46, P = .03, 𝜂p2= 0.01. Post hoc analysis showed that the high severity group had a significantly greater mean bias score (M = 4.4 ms) relative to the moderate (M = 0.6 ms), P = .05, and the low (M =−0.3 ms), P = .01, symptom severity groups. The two latter groups did not differ in mean bias scores, P = .68. One-sample t-tests revealed that the mean bias score in the high severity group was significantly greater than zero, t(485) = 2.86, P = .004; mean bias scores in the other groups did not differ from zero, Ps > .71.
Additional analyses exploring variations of the bias measures or the regression models are reported in supplementary material.
4. DISCUSSION
We examined the association between attention bias to social threat cues and overall and specific anxiety symptoms in a large, heterogeneous sample of youth performing a standardized threat-bias paradigm. The key findings are that threat bias positively and significantly correlated with severity of overall anxiety symptoms, with some evidence indicating hypervigilance to threat (as opposed to difficulty in disengaging from it). Specifically, bias-symptoms associations appeared to emerge more prominently for social anxiety and school phobia symptoms. In addition, threat bias did not interact with age or gender to predict any of the reported anxiety symptoms.
Overall, our findings of bias-anxiety associations are in accord with several previous studies examining group differences in threat bias between healthy and anxious groups (Dudeney et al., 2015; Salum et al., 2013; Waters et al., 2014). Our results extend previous findings in terms of both generalizability and specificity (Asendorpf et al., 2013). In terms of generalizability, our findings are based on a large, inclusive, and multi-cultural sample which may offer greater heterogeneity than smaller and more restrictive samples (although the different sites still applied some limiting inclusion/exclusion criteria, see supplementary material). Furthermore, the observed bias-anxiety associations were not moderated by age or gender, suggesting that they are further generalizable across these factors. Finally, our findings capture bias-anxiety associations across the full, continuous range of anxiety symptom severity (as well as differences in bias scores between high- and low-anxiety groups), complementing previous work relying only on extreme or diagnosis-based groups which may limit generalizability and dimension-based research (Cuthbert & Insel, 2013; Hoertel et al., 2014).
Our results also suggest greater specificity of threat bias to symptoms of pediatric social anxiety and school phobia when measured with a faces-based dot-probe task. This extends extant literature which to date has been limited in robustly identifying associations between threat bias and symptoms of specific anxiety subtypes (Dudeney et al., 2015; Waters et al., 2014). Specifically, social anxiety has been hypothesized to relate to an attentional bias to threat-related facial expressions since this information may inform about negative evaluation by others (Pergamin-Hight et al., 2015; Rapee & Heimberg, 1997; Staugaard, 2010). However, to date, studies comparing threat bias between groups differing in social anxiety levels yielded mixed results (Bantin et al., 2016). The current data suggest a direct association between threat bias to angry faces and symptoms of pediatric social anxiety.
This is also the first report of association between threat bias and symptoms of school phobia, a correlation which has not been addressed in previous research. School phobia often occurs with other anxiety symptoms, and may confer risk for development of adult psychiatric disorders (Fremont, 2003; Tyrrell, 2005). The common association with threat bias demonstrated in this study suggests that social anxiety and school phobia may involve some common attentional elements (e.g., fear of school-related social situations), which manifest as vigilance to potential social threat cues (Vuilleumier, 2002).
Childhood and adolescence have been established as core risk phases for the development of anxiety symptoms, with different anxiety disorders following distinct developmental trajectories (Beesdo et al., 2009; Hale, Raaijmakers, Muris, van Hoof, & Meeus, 2008; Kessler et al., 2005). Whether attention biases to threat also follow a specific developmental trajectory has been a matter of debate (Field & Lester, 2010; Hadwin & Field, 2010). Our results indicate that the severity of anxiety symptoms changes with age, but do not show evidence for a moderating role for age in the association between anxiety and threat bias, suggesting that these associations do not markedly change with child development (Dudeney et al., 2015; Field & Lester, 2010). In fact, similar correlations between bias scores and symptom severity were obtained when first removing or maintaining variance in bias explained by age, further suggesting an independence between threat bias and age. Of note, this finding differs from the moderating effect of age reported in a meta-analysis by Dudeney et al. (2015), although this discrepancy may arise due to greater variability in methodology, such as task parameters that depend on linguistic ability which develops with age. Future longitudinal research following children over time and using different, complementary methodologies could allow for a systematic and comprehensive analysis of the development of attentional bias across age.
In addition to elucidating the association between threat bias and pediatric anxiety symptoms, the current findings may have translational clinical implications. ABM is a novel computerized therapeutic approach to anxiety disorders aimed at rectifying attentional biases to threat stimuli (Bar-Haim, 2010; MacLeod & Clarke, 2015). The specificity of social anxiety and school phobia symptoms to a bias to threatening faces lends validity to the use of face stimuli in ABM procedures targeting such symptoms, whereas patients suffering from other types of anxiety may benefit more from training using stimuli that are more specifically relevant to their symptoms. The stability of bias-anxiety relations across age also suggests that ABM targeting threat bias may potentially be applied early in development for anxiety in children as young as 6 years of age, although it is not yet clear whether the cognitive and psychomotor capacities required for effective ABM application are sufficiently mature in such younger patients (Mogoase, David, & Koster, 2014; Pergamin-Hight et al., 2016). Additional research is needed to empirically test the translation of the current findings into treatment efficacy. Of particular importance is the application of reliable measures of threat bias (see limitations section) that will allow for tracking of the effect of ABM over the training protocol.
It should also be noted that although threat bias was significantly associated with anxiety symptoms severity, the magnitude of the revealed associations is fairly weak. Moreover, when the sample was divided into tertiles, only the high symptom severity group evidenced mean bias score that was significantly different from zero. This may suggest that the relative role of an attention bias to threat in pediatric anxiety symptoms is indeed minor, and may explain previous inconsistencies and the moderate effect size of ABM efficacy for pediatric anxiety (Dudeney et al., 2015; Linetzky, Pergamin-Hight, Pine, & Bar-Haim, 2015; Mogoase et al., 2014). Alternatively, stronger bias-symptoms relations could be uncovered as more potent, reliable, and sensitive measures of threat bias patterns are developed and applied (De Voogd, Wiers, Prins, & Salemink, 2014; Lazarov, Abend, & Bar-Haim, 2016; Naim et al., 2015; Price et al., 2015). Continued research on improved threat bias assessment is warranted to further consolidate the association between bias and anxiety symptoms.
Nevertheless, the current findings underscore the utility and value of a standardized, multi-site collaborative approach to psychopathology research (Arad & Bar-Haim, 2017). Multi-site studies are being increasingly used to study various conditions, including anxiety and its treatment (e.g., Allen et al., 2010; Mennin et al., 2002). Such collaborative efforts can significantly advance research by enabling the aggregation of large, heterogeneous samples which are key for increasing statistical power to reveal effects as well as generalizability of findings (e.g., Asendorpf et al., 2013). Furthermore, they can facilitate research on dimensions of psychopathology by increasing the variability along the sampled dimension and focusing on individual differences (Cuthbert & Insel, 2013). An important aspect of multi-site collaboration is the convergence and standardization of tasks and measures used in the research field; a case in point is the attention bias field which features a broad range of paradigms and task parameters (Dudeney et al., 2015; Priceetal., 2015;Puliafico&Kendall,2006). Inthisstudy,suchmethodology enabled us to uncover weak but specific bias-symptoms associations, and test relevant moderators, across a large and diverse sample.
Although this report highlights the importance of standardizing and aggregating data across multiple sites, such methodology may also bring about some challenges resulting in limitations, as in the current report. First, the single common symptoms measure across sites was the child-report version of the SCARED; furthermore, clinical diagnosis of anxiety was not required in all sites. The use of multiple measures of anxiety and other psychopathology symptoms by multiple informants, including clinical diagnosis, would have enabled us to more comprehensively assess the clinical correlates of attention bias (Schniering, Hudson, & Rapee, 2000; Silverman & Ollendick, 2005). Second, and relating to the previous limitation, the different sites collected different demographic information, limiting our ability to fully control for confounding factors (Beesdo et al., 2009), and did not apply identical inclusion and exclusion criteria, which may have led to additional heterogeneity in the sample. Such limitations stem from differences in study aims between the different sites. Nevertheless, future collaborative efforts could strive to maximize the number of common measures applied across sites such that more specific or comprehensive research questions may be addressed. Third, we examined attention biases only to social threat cues (angry faces). Although this allowed us to establish specificity to specific anxiety categories, the use of other types of stimuli would have enabled us to potentially test for specificity to other categories as well. Finally, all sites, as part of the TAU-NIMH Initiative, employed the dot-probe task to assess threat bias. Although it is one of the most widely used threat bias paradigms, studies suggest that bias assessment using the dot-probe task is characterized by inadequate reliability (Price et al., 2015; Schmukle, 2005). As such, future studies may wish to assess threat bias via multiple, complementary methods (e.g., combining behavioral and eye-tracking methods) or over several measurement sessions, as well as extend the traditional, single threat bias score to novel and more stable measures which aim to capture the dynamic aspects of threat bias across time (Iacoviello et al., 2014; Price et al., 2015; Zvielli, Bernstein, & Koster, 2015).
5. CONCLUSION
In conclusion, extant research on relations between attention bias to threat and pediatric anxiety symptoms may be limited by methodological constraints. To overcome some of these constraints, we utilized standardized measures and a multi-site approach to create a large youth sample, and reveal associations between threat bias and anxiety symptoms. Our findings inform about the role of attentional threat bias in specific anxiety symptom categories as well as bear practical clinical implications.
Supplementary Material
ACKNOWLEDGMENTS
We would like to thank G. G. Manfro, P. Pan, Y. Maman, A. Omri, and B. Lily for their valuable input. This research was supported (in part) by the NIMH Intramural Research Program (ZIAMH00278115, NCT00018057; R.A., L.K.W., D.S.P.), by National Institutes of Health (R01 MH094633, K.P-E.; UH2 MH101470, J.W.P., W.K.S.; R34 MH097931, J.W.P, W.K.S.), by the United States – Israel Binational Science Foundation (2013349; Y.B-H.), and by the Irish Research Council Project Starter Grant (A.F.).
Funding information
Grant sponsor: NIMH Intramural Research Program; Contract grant numbers: ZIAMH002781–15 and NCT00018057 (to R.A., L.K.W., D.S.P.); Grant sponsor: National Institutes of Health; Contract grant numbers: R01 MH094633 (to K.P-E.), UH2 MH101470 (to J.W.P., W.K.S.), and R34 MH097931 (to J.W.P., W.K.S.); Grant sponsor: United States - Israel Binational Science Foundation; Contract grant number: 2013349 (to Y.B-H.); Grant sponsor: Irish Research Council Project Starter Grant (to A.F.).
Footnotes
CONFLICT OF INTEREST
All authors declare that they have no conflict of interest.
REFERENCES
- Abend R, Pine DS, & Bar-Haim Y (2014). The TAU-NIMH attention bias measurement toolbox Retrieved from https://people.socsci.tau.ac.il/mu/anxietytrauma/research/
- Allen LB, White KS, Barlow DH, Shear MK, Gorman JM, & Woods SW (2010). Cognitive-Behavior Therapy (CBT) for panic disorder: Relationship of anxiety and depression comorbidity with treatment outcome. Journal of Psychopathology and Behavioral Assessment, 32(2), 185–192. 10.1007/s10862-009-9151-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arad G, & Bar-Haim Y (2017). Commentary: Information-processing in anxiety and depression: Novel targets for translational research – a reflection on Lau and Waters (2017). Journal of Child Psychology and Psychiatry, 58(4), 408–410. 10.1111/jcpp.12717 [DOI] [PubMed] [Google Scholar]
- Armstrong T, & Olatunji BO (2012). Eye tracking of attention in the affective disorders: A meta-analytic review and synthesis. Clinical Psychology Review, 32(8), 704–723. 10.1016/j.cpr.2012.09.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asendorpf JB, Conner M, De Fruyt F, De Houwer J, Denissen JJA, Fiedler K, … Wicherts JM (2013). Recommendations for increasing replicability in psychology. European Journal of Personality, 27(2), 108–119. 10.1002/per.1919 [DOI] [Google Scholar]
- Bantin T, Stevens S, Gerlach AL, & Hermann C (2016). What does the facial dot-probe task tell us about attentional processes in social anxiety? A systematic review. Journal of Behavior Therapy and Experimental Psychiatry, 50, 40–51. 10.1016/j.jbtep.2015.04.009 [DOI] [PubMed] [Google Scholar]
- Bar-Haim Y (2010). Research review: Attention bias modification (ABM): A novel treatment for anxiety disorders. Journal of Child Psychology and Psychiatry, 51(8), 859–870. 10.1111/j.1469-7610.2010.02251.x [DOI] [PubMed] [Google Scholar]
- Bar-Haim Y, Lamy D, Pergamin L, Bakermans-Kranenburg MJ, & van IJzendoorn MH (2007). Threat-related attentional bias in anxious and nonanxious individuals: A meta-analytic study. Psychological Bulletin, 133(1), 1–24. 10.1037/0033-2909.133.1.1 [DOI] [PubMed] [Google Scholar]
- Beesdo K, Knappe S, & Pine DS (2009). Anxiety and anxiety disorders in children and adolescents: Developmental issues and implications for DSM-V. Psychiatric Clinics of North America, 32(3), 483–524. 10.1016/j.psc.2009.06.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, & Baugher M (1999). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38(10), 1230–1236. 10.1097/00004583-199910000-00011 [DOI] [PubMed] [Google Scholar]
- Bittner A, Egger HL, Erkanli A, Jane Costello E, Foley DL, & Angold A (2007). What do childhood anxiety disorders predict? Journal of Child Psychology and Psychiatry, and Allied Disciplines, 48(12), 1174–1183. [DOI] [PubMed] [Google Scholar]
- Canals J, Hernandez-Martinez C, Cosi S, & Domenech E (2012). Examination of a cutoff score for the Screen for Child Anxiety Related Emotional Disorders (SCARED) in a non-clinical Spanish population. Journal of Anxiety Disorders, 26(8), 785–791. 10.1016/j.janxdis.2012.07.008 [DOI] [PubMed] [Google Scholar]
- Cisler JM, & Koster EH (2010). Mechanisms of attentional biases towards threat in anxiety disorders: An integrative review. Clinical Psychology Review, 30(2), 203–216. 10.1016/j.cpr.2009.11.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuthbert BN (2015). Research domain criteria: Toward future psychiatric nosologies. Dialogues in Clinical Neuroscience, 17(1), 89–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuthbert BN, & Insel TR (2013). Toward the future of psychiatric diagnosis: The seven pillars of RDoC. BMC Medicine, 11, 126 10.1186/1741-7015-11-126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Voogd EL, Wiers RW, Prins PJ, de Jong PJ, Boendermaker WJ, Zwitser RJ, & Salemink E (2016). Online attentional bias modification training targeting anxiety and depression in unselected adolescents: Short- and long-term effects of a randomized controlled trial. Behaviour Research and Therapy, 87, 11–22. 10.1016/j.brat.2016.08.018 [DOI] [PubMed] [Google Scholar]
- De Voogd EL, Wiers RW, Prins PJ, & Salemink E (2014). Visual search attentional bias modification reduced social phobia in adolescents. Journal of Behavior Therapy and Experimental Psychiatry, 45(2), 252–259. 10.1016/j.jbtep.2013.11.006 [DOI] [PubMed] [Google Scholar]
- Desousa DA, Salum GA, Isolan LR, & Manfro GG (2013). Sensitivity and specificity of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A community-based study. Child Psychiatry & Human Development, 44(3), 391–399. 10.1007/s10578-012-0333-y [DOI] [PubMed] [Google Scholar]
- Dudeney J, Sharpe L, & Hunt C (2015). Attentional bias towards threatening stimuli in children with anxiety: A meta-analysis. Clinical Psychology Review, 40, 66–75. 10.1016/j.cpr.2015.05.007 [DOI] [PubMed] [Google Scholar]
- Field AP, & Lester KJ (2010). Is there room for ‘development’ in developmental models of information processing biases to threat in children and adolescents? Clinical Child and Family Psychology Review, 13(4), 315–332. 10.1007/s10567-010-0078-8 [DOI] [PubMed] [Google Scholar]
- Fitzgerald A, Rawdon C, & Dooley B (2016). A randomized controlled trial of attention bias modification training for socially anxious adolescents. Behaviour Research and Therapy, 84, 1–8. 10.1016/j.brat.2016.06.003 [DOI] [PubMed] [Google Scholar]
- Fremont WP (2003). School refusal in children and adolescents. American Family Physician, 68(8), 1555–1560. [PubMed] [Google Scholar]
- Hadwin JA, & Field AP (2010). Theoretical and methodological issues in researching information processing biases in anxious children and adolescents. In Hadwin JA & Field AP (Eds.), Information processing biases and anxiety: A developmental perspective (pp. 1–17). Chichester, England: Wiley-Blackwell. [Google Scholar]
- Hale WW 3rd, Raaijmakers Q, Muris P, van Hoof A, & Meeus W (2008). Developmental trajectories of adolescent anxiety disorder symptoms: A 5-year prospective community study. Journal of the American Academy of Child and Adolescent Psychiatry, 47(5), 556–564. 10.1097/CHI.0b013e3181676583 [DOI] [PubMed] [Google Scholar]
- Hoertel N, de Maricourt P, Katz J, Doukhan R, Lavaud P, Peyre H, & Limosin F (2014). Are participants in pharmacological and psychotherapy treatment trials for social anxiety disorder representative of patients in real-life settings? Journal of Clinical Psychopharmacology, 34(6), 697–703. 10.1097/JCP.0000000000000204 [DOI] [PubMed] [Google Scholar]
- Iacoviello BM, Wu G, Abend R, Murrough JW, Feder A, Fruchter E, … Charney DS (2014). Attention bias variability and symptoms of posttraumatic stress disorder. Journal of Traumatic Stress, 27(2), 232–239. 10.1002/jts.21899 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Chiu WT, Demler O, Merikangas KR, & Walters EE (2005). Prevalence, severity, and comorbidity of 12month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 617–627. 10.1001/archpsyc.62.6.617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koster EH, Crombez G, Verschuere B, & De Houwer J (2004). Selective attention to threat in the dot probe paradigm: Differentiating vigilance and difficulty to disengage. Behaviour Research and Therapy, 42(10), 1183–1192. 10.1016/j.brat.2003.08.001 [DOI] [PubMed] [Google Scholar]
- Lazarov A, Abend R, & Bar-Haim Y (2016). Social anxiety is related to increased dwell time on socially threatening faces. Journal of Affective Disorders, 193, 282–288. 10.1016/j.jad.2016.01.007 [DOI] [PubMed] [Google Scholar]
- Linetzky M, Pergamin-Hight L, Pine DS, & Bar-Haim Y (2015). Quantitative evaluation of the clinical efficacy of attention bias modification treatment for anxiety disorders. Depression and Anxiety, 32(6), 383–391. 10.1002/da.22344 [DOI] [PubMed] [Google Scholar]
- MacLeod C, & Clarke PJ (2015). The attentional bias modification approach to anxiety intervention. Clinical Psychological Science, 3(1), 58–78. 10.1177/2167702614560749 [DOI] [Google Scholar]
- MacLeod C, & Mathews A (2012). Cognitive bias modification approaches to anxiety. Annual Review of Clinical Psychology, 8, 189–217. 10.1146/annurev-clinpsy-032511-143052 [DOI] [PubMed] [Google Scholar]
- MacLeod C, Mathews A, & Tata P (1986). Attentional bias in emotional disorders. Journal of Abnormal Psychology, 95(1), 15–20. [DOI] [PubMed] [Google Scholar]
- Mennin DS, Fresco DM, Heimberg RG, Schneier FR, Davies SO, & Liebowitz MR (2002). Screening for social anxiety disorder in the clinical setting: Using the Liebowitz Social Anxiety Scale. Journal of Anxiety Disorders, 16(6), 661–673. [DOI] [PubMed] [Google Scholar]
- Mogoase C, David D, & Koster EH (2014). Clinical efficacy of attentional bias modification procedures: An updated meta-analysis. Journal of Clinical Psychology, 70(12), 1133–1157. 10.1002/jclp.22081 [DOI] [PubMed] [Google Scholar]
- Morales S, Taber-Thomas BC, & Pérez-Edgar K (2017). Patterns of attention to threat across tasks in behaviorally inhibited children at risk for anxiety. Developmental Science, 20(2). 10.1111/desc.12391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muris P, Merckelbach H, Ollendick T, King N, & Bogie N (2002). Three traditional and three new childhood anxiety questionnaires: Their reliability and validity in a normal adolescent sample. Behaviour Research and Therapy, 40(7), 753–772. [DOI] [PubMed] [Google Scholar]
- Naim R, Abend R, Wald I, Eldar S, Levi O, Fruchter E, … Bar-Haim Y (2015). Threat-related attention bias variability and posttraumatic stress. American Journal of Psychiatry 10.1176/appi.ajp.2015.14121579 [DOI] [PMC free article] [PubMed]
- Pergamin-Hight L, Naim R, Bakermans-Kranenburg MJ, van IJzendoorn MH, & Bar-Haim Y (2015). Content specificity of attention bias to threat in anxiety disorders: A meta-analysis. Clinical Psychology Review, 35, 10–18. 10.1016/j.cpr.2014.10.005 [DOI] [PubMed] [Google Scholar]
- Pergamin-Hight L, Pine DS, Fox NA, & Bar-Haim Y (2016). Attention bias modification for youth with social anxiety disorder. Journal of Child Psychology and Psychiatry, 57(11), 1317–1325. 10.1111/jcpp.12599 [DOI] [PubMed] [Google Scholar]
- Pine DS, & Fox NA (2015). Childhood antecedents and risk for adult mental disorders. Annual Review of Psychology, 66, 459–485. 10.1146/annurev-psych-010814-015038 [DOI] [PubMed] [Google Scholar]
- Pine DS, Helfinstein SM, Bar-Haim Y, Nelson E, & Fox NA (2009). Challenges in developing novel treatments for childhood disorders: Lessons from research on anxiety. Neuropsychopharmacology, 34(1), 213–228. 10.1038/npp.2008.113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinheiro JC, & Bates DM (2000). Mixed-effects models in S and S-PLUS New York, NY: Springer-Verlag. [Google Scholar]
- Pintzinger NM, Pfabigan DM, Pfau L, Kryspin-Exner I, & Lamm C (2017). Temperament differentially influences early information processing in men and women: Preliminary electrophysiological evidence of attentional biases in healthy individuals. Biological Psychology, 122, 69–79. 10.1016/j.biopsycho.2016.07.007 [DOI] [PubMed] [Google Scholar]
- Price RB, Kuckertz JM, Siegle GJ, Ladouceur CD, Silk JS, Ryan ND, … Amir N (2015). Empirical recommendations for improving the stability of the dot-probe task in clinical research. Psychological Assessment, 27(2), 365–376. 10.1037/pas0000036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puliafico AC, & Kendall PC (2006). Threat-related attentional bias in anxious youth: A review. Clinical Child and Family Psychology Review, 9(3–4), 162–180. 10.1007/s10567-006-0009-x [DOI] [PubMed] [Google Scholar]
- R Core Team. (2014). R: A language and environment for statistical computing Vienna, Austria: R Foundation for Statistical Computing; Retrieved from https://www.r-project.org/. [Google Scholar]
- Rapee RM, & Heimberg RG (1997). A cognitive-behavioral model of anxiety in social phobia. Behaviour Research and Therapy, 35(8), 741–756. https://doi:S0005-7967(97)00022-3 [DOI] [PubMed] [Google Scholar]
- Rapee RM, Schniering CA, & Hudson JL (2009). Anxiety disorders during childhood and adolescence: Origins and treatment. Annual Review of Clinical Psychology, 5, 311–341. 10.1146/annurev.clinpsy.032408.153628 [DOI] [PubMed] [Google Scholar]
- Salum GA, Mogg K, Bradley BP, Gadelha A, Pan P, Tamanaha AC, … Pine DS (2013). Threat bias in attention orienting: Evidence of specificity in a large community-based study. Psychological Medicine, 43(4), 733–745. 10.1017/S0033291712001651 [DOI] [PubMed] [Google Scholar]
- Sass SM, Heller W, Stewart JL, Silton RL, Edgar JC, Fisher JE, & Miller GA (2010). Time course of attentional bias in anxiety: Emotion and gender specificity. Psychophysiology, 47(2), 247–259. 10.1111/j.1469-8986.2009.00926.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmukle SC (2005). Unreliability of the dot probe task. European Journal of Personality, 19(7), 595–605. 10.1002/Per.554 [DOI] [Google Scholar]
- Schniering CA, Hudson JL, & Rapee RM (2000). Issues in the diagnosis and assessment of anxiety disorders in children and adolescents. Clinical Psychology Review, 20(4), 453–478. [DOI] [PubMed] [Google Scholar]
- Silverman WK, & Ollendick TH (2005). Evidence-based assessment of anxiety and its disorders in children and adolescents. Journal of Clinical Child and Adolescent Psychology, 34(3), 380–411. 10.1207/s15374424jccp3403_2 [DOI] [PubMed] [Google Scholar]
- Staugaard SR (2010). Threatening faces and social anxiety: A literature review. Clinical Psychology Review, 30(6), 669–690. 10.1016/j.cpr.2010.05.001 [DOI] [PubMed] [Google Scholar]
- Tottenham N, Tanaka JW, Leon AC, McCarry T, Nurse M, Hare TA, … Nelson C (2009). The NimStim set of facial expressions: Judgments from untrained research participants. Psychiatry Research, 168(3), 242–249. 10.1016/j.psychres.2008.05.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tyrrell M (2005). School phobia. Journal of School Nursing, 21(3), 147–151. [DOI] [PubMed] [Google Scholar]
- Vuilleumier P (2002). Facial expression and selective attention. Current Opinion in Psychiatry, 15(3), 291–300. [Google Scholar]
- Waters AM, Bradley BP, & Mogg K (2014). Biased attention to threat in paediatric anxiety disorders (generalized anxiety disorder, social phobia, specific phobia, separation anxiety disorder) as a function of ‘distress’ versus ‘fear’ diagnostic categorization. Psychological Medicine, 44(3), 607–616. 10.1017/S0033291713000779 [DOI] [PubMed] [Google Scholar]
- White LK, Britton JC, Sequeira S, Ronkin EG, Chen G, BarHaim Y, … Pine DS (2016). Behavioral and neural stability of attention bias to threat in healthy adolescents. Neuroimage, 136, 84–93. 10.1016/j.neuroimage.2016.04.058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- White LK, Sequeira S, Britton JC, Brotman MA, Gold AL, Berman E, … Pine DS (2017). Complementary features of attention bias modification therapy and cognitive-behavioral therapy in pediatric anxiety disorders. American Journal of Psychiatry 10.1176/appi.ajp.2017.16070847 [DOI] [PMC free article] [PubMed]
- Zvielli A, Bernstein A, & Koster EH (2015). Temporal dynamics of attentional bias. Clinical Psychological Science, 3(5), 772–788. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.