

Abstract
Purpose:
An appropriate vault after implantation of a posterior chamber phakic intraocular lens with a central hole (ICL KS-AP) is important for successful long-term outcomes. In the present study, we used anterior segment optical coherence tomography (AS-OCT) to examine dynamic pupil and vault changes under photopic and scotopic conditions and during accommodation in eyes with ICL KS-AP.
Methods:
This retrospective study included patients at an outpatient ophthalmology clinic who underwent ICL KS-AP implantation >1 month before enrollment. All patients underwent dynamic AS-OCT imaging under photopic and scotopic conditions. Patients aged <40 years also underwent imaging in the accommodative and nonaccommodative states. Primary outcome measures were the pupil size and vault at the maximum and minimum pupil sizes.
Results:
This study included 91 eyes of 47 patients (35.5 ± 8.6 years, 21 men). Accommodation was examined in 51 eyes of 26 patients (28.9 ± 5.0 years, 10 men) younger than 40 years. The pupil size was significantly smaller under photopic conditions (3.64 ± 0.77 mm) than under scotopic conditions (4.91 ± 0.75 mm, P < 0.001) and during accommodation (3.88 ± 0.64 vs. 4.10 ± 0.61 mm, P < 0.001). Vault was also significantly lower under photopic conditions (476.1 ± 219.6 μm) than under scotopic conditions (521.1 ± 220.4 μm, P < 0.001) and during accommodation (454.8 ± 224.9 vs. 481.6 ± 219.1 μm, P < 0.001).
Conclusions:
Vault can be significantly lowered by light-induced pupil constriction and accommodation in eyes with ICL KS-AP.
Key Words: pupil size, vault, implantable collamer lens, accommodation
The implantable collamer lens (ICL) is often the first choice for surgical correction of high myopia. However, the number of ICLs implanted to treat low-to-moderate myopia is increasing.1–5 The posterior chamber phakic intraocular lens with a central hole (KS-AP; STAAR Surgical, Monrovia, CA), invented by Shimizu et al,6 has a central artificial hole with a 0.36-mm diameter, and it was approved for use in Japan by the Ministry of Health, Labour and Welfare in 2010. ICL KS-AP has been reported to be safe and effective for correcting refractive errors, and it provides predictable, stable, and good visual outcomes.6,7 Introduction of ICL KS-AP was a marked improvement over the Visian ICL V4, which has been associated with cataract and increased intraocular pressure caused by postoperative complications. The central hole in ICL KS-AP improves aqueous humor circulation, preventing many of these complications.8 The use of ICL V4 necessitates peripheral iridectomy, but because the hole in ICL KS-AP keeps the aqueous humor circulating, peripheral iridectomy is unnecessary.6
An appropriate vault (distance between the posterior ICL surface and anterior crystalline lens surface) after ICL implantation is generally 0.5 to 1.5 times the corneal thickness (CT, 250–750 μm). Patients with a low vault before V4 ICL implantation are at an increased risk of postoperative cataract progression, whereas those with a high vault before ICL implantation are at an increased risk of postoperative intraocular pressure elevation. Previous studies have revealed that the pupil size can influence vault measurements, but the dynamic vault changes associated with dynamic pupil changes have not been examined in eyes with ICLs. The current study used anterior segment swept-source optical coherence tomography (AS-OCT) to simultaneously evaluate the dynamic pupil size and vault changes in eyes with ICL KS-AP. Measurements were made under photopic and scotopic conditions and in the accommodative and nonaccommodative states.
MATERIALS AND METHODS
This study was reviewed and approved by the Institutional Review Board at Sanno Hospital (Tokyo, Japan). All patients provided informed consent to participate in the study, and all study procedures adhered to the tenets of the Declaration of Helsinki.
All patients had undergone ICL KS-AP implantation at the Sanno Hospital Eye Center at least 1 month before study enrollment. All patients were included in study group A and underwent study measurements under both photopic and scotopic conditions. Study group B comprised younger patients (aged <40 years) with emmetropia after ICL implantation. These patients also underwent measurements in both the accommodative and nonaccommodative states. All measurements were obtained at 1 month after surgery.
All patients underwent AS-OCT in the “Lens Movie” mode, which was programmed to obtain 10-second video clips (CASIA2; TOMEY, Nagoya, Japan). The image capture rate was 10 images/s. A video was obtained for the patients in group A under scotopic conditions (background illumination = 4 lx) for the first 5 seconds and photopic conditions (background illumination = 400 lx) for the next 5 seconds. The patients fixated on an internal target during video capture. An additional video was obtained for patients in group B under photopic conditions. The patients fixated on an internal target while looking through a 0.00-diopter (D) lens for the first 5 seconds and a 3.00-D lens for the next 5 seconds. The patients were asked to specifically focus on the internal fixation target to achieve an accommodative state.
The AS-OCT images obtained while the pupil was at its minimum and maximum sizes were identified under each measurement condition, and each anterior segment parameter was manually measured on these images. The examined parameters included the pupil size, vault, the anterior chamber depth (ACD), and the lens thickness (LT). Two measurements were obtained for the ACD. ACD-lens was defined as the distance between the posterior corneal surface and the anterior lens surface, whereas ACD-ICL was defined as the distance between the posterior corneal surface and the anterior ICL surface.
Data are presented as mean values ± SDs where applicable. Wilcoxon signed-rank tests were used to compare the parameters measured under scotopic and photopic conditions and those measured during accommodative and nonaccommodative states. Spearman rank correlation coefficients were used to examine correlations between the measured parameters and the pupil size and vault. All statistical analyses were performed using spreadsheet software (Excel; Microsoft Corporation, Redmond, WA). Statistical significance was defined as P < 0.05.
RESULTS
Group A included 91 eyes (47 patients, 35.5 ± 8.6 years, 21 men) and group B included 51 eyes (26 patients, 28.9 ± 5.0 years, 10 men). Table 1 summarizes the patient and ocular characteristics before ICL KS-AP implantation surgery. Table 2 summarizes the scotopic and photopic anterior chamber measurements after ICL KS-AP implantation. Briefly, the pupil size was significantly smaller, and vault was significantly lower under photopic conditions than under scotopic conditions (both P <0.001). LT (P = 0.154) and ACD-lens (P = 0.129) were not significantly different between scotopic and photopic conditions. However, vault was significantly lower, and ACD-ICL was significantly larger during photopic conditions (both P < 0.001). Representative AS-OCT images taken under scotopic and photopic conditions are shown in Figure 1.
TABLE 1.
Patient and Ocular Characteristics Before Implantation of a Posterior Chamber Phakic Intraocular Lens With a Central Hole

TABLE 2.
Effect of Lighting Conditions on Anterior Chamber Measurements for Eyes With a Posterior Chamber Phakic Intraocular Lens With a Central Hole

FIGURE 1.
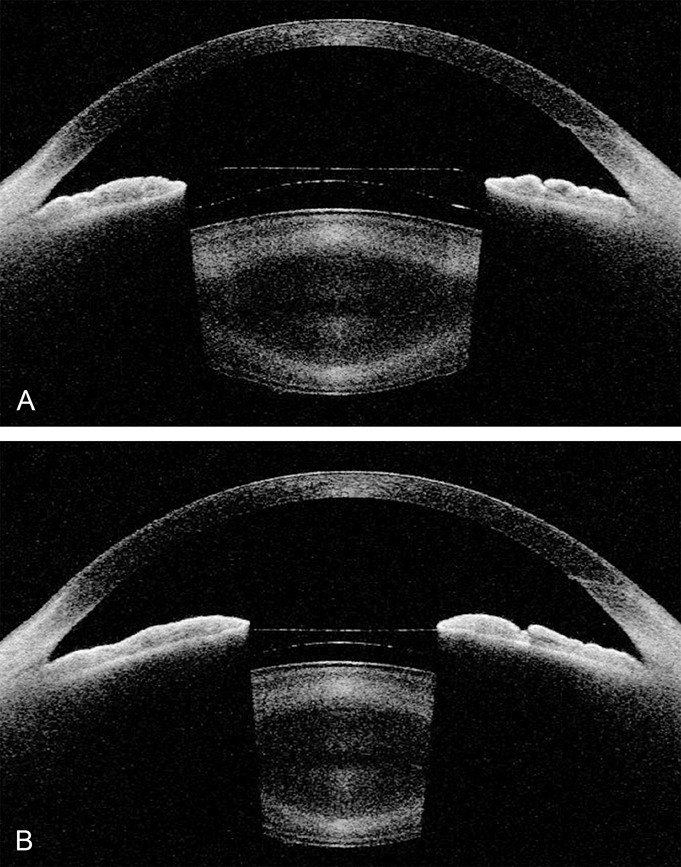
Representative anterior segment optical coherence tomography images for the left eye of a 27-year-old man who underwent implantation of a posterior chamber phakic intraocular lens with a central hole. Images obtained under scotopic conditions (A) show a vault of 570 μm and a pupil size of 5.9 mm. Images obtained under photopic conditions (B) show a vault of 386 μm and a pupil size of 3.8 mm.
Accommodation significantly changed several anterior chamber measurements (Table 3), resulting in a decreased pupil size (constriction), an increased LT, a decreased vault, and a decreased ACD-lens and ACD-ICL (all P < 0.001). A decrease in ACD-ICL indicates forward movement of the ICL.
TABLE 3.
Effect of Accommodation on Anterior Chamber Measurements for Eyes With a Posterior Chamber Phakic Intraocular Lens With a Central Hole

The influence of the pupil size on vault was examined by calculating the change in the pupil size and vault. The vault change was positively correlated with the light-related pupil size change [Spearman rank correlation coefficient (r) = 0.509, P < 0.001]. In contrast, the accommodation-related pupil size change was not correlated with the vault change (r = 0.204, P = 0.151).
DISCUSSION
The present study simultaneously examined the pupil size and vault under photopic and scotopic conditions and in the accommodative and nonaccommodative states. In both cases, pupillary constriction resulted in a lower vault. This study's main strength was that it used video AS-OCT to dynamically evaluate the vault changes associated with dynamic pupil changes. Because of hippus, the accurate maximum and minimum pupil sizes could not be obtained by static measurement. The dynamic method used in this study can measure the maximum and minimum pupil sizes for 5 seconds, thereby providing a more accurate and stable value than that obtained by static measurement. However, this study does not compare static and dynamic imaging.
Our study also has some limitations. First, our sample size was relatively small, and the effects of light and accommodation on ICL KS-AP should be examined in a larger group of patients. Second, this study performed assessments only under 2 lighting conditions and 1 accommodation power. Future studies should include various light and accommodation levels to better understand the anatomical position of ICL KS-AP in all conditions.
The results of the present study are consistent with those of Petternel et al,9 who compared the pupil size and vault under photopic and mesopic conditions in eyes with a V3 or V4 ICL. Measurements were made using partial coherence interferometry, with a penlight shining on the fellow eye to induce photopic conditions. They did not find a significant light-induced change in ACD-lens, but ACD-ICL was significantly increased by 0.10 mm, whereas vault was significantly decreased by 73 μm. Lee et al10 also examined the anterior chamber anatomy under photopic and mesopic conditions in eyes with a V4c ICL using the Visante OCT. As observed in the study by Petternel et al,9 mesopic conditions were induced by shining a penlight (2 lx) on the fellow eye. Light induced a significant decrease in both pupil size (2.32 mm under photopic conditions) and vault (change of 147.5 μm); however, ACD-lens did not significantly change. Lindland et al11 examined the anterior chamber anatomy during mesopic (2 lx) and photopic (257 lx) conditions using the Visante OCT. The change from the mesopic to the photopic condition induced a decrease in the pupil size (by 1.8 mm), a decrease in ACD-lens, an increase in ACD-ICL, and a decrease in vault (by 35 μm). Their study did not find a significant difference between myopic and toric ICLs. Both Petternel et al9 and Lee et al10 observed a vault change larger than that observed in the present study, probably because of differences in lighting techniques. Their studies used a penlight to induce photopic conditions, whereas our study used background light.
Previous studies have examined the vault changes induced by accommodation. Both Petternel et al9 and Lindland et al12 found that ACD-lens, ACD-ICL, and vault did not significantly change with accommodation in eyes with a V3 (Ref. 9) or V4 (Refs. 9,12) ICL. Furthermore, Lee et al13 used the Visante OCT to examine the effect of accommodation on the anterior chamber anatomy in eyes with a V4c ICL. The pupil size, ACD-lens, and ACD-ICL decreased by 0.8, 0.2, and 0.2 mm, respectively, in the presence of an accommodation of 16 D. Vault did not significantly change. We speculated that changes in vault were not observed because these previous studies used static imaging modalities. However, our results, obtained with dynamic imaging (10-second video recording used to ensure measurements taken during accommodation), are in agreement with those of previous static imaging studies.
Kojima et al reported that the vault of ICL V4 decreased until 3 months postoperatively but remained stable from 3 months to 1 year postoperatively.14 Yan et al15 reported that there was no long-term change in vault over a period of 2 years after surgery. Based on these reports, we believed that the hole would not affect the vault in our study. Furthermore, when ACD is used for ICL size selection, the value does not differ between photopic and scotopic conditions, but the ACD becomes shallow with accommodation. Therefore, whether using ACD or other parameters, it is better to measure illuminance and accommodation under the same condition.
A 0.03-mm shift in an intraocular lens translates into a 0.05-D refraction change.16 The present study showed that photopic conditions induced a 0.04-mm increase in ACD-ICL and that accommodation induced a 0.05-mm decrease in ACD-ICL. This translates into 0.03- and 0.04-D refraction changes, respectively. Therefore, vault changes that occur during miosis and accommodation have almost no effect on the refractive error. Furthermore, we found that vault was significantly lower under photopic conditions than scotopic conditions, with no difference in ACD-lens. These findings suggest that light-induced vault changes result from physical changes in the iris and not in the ICL position. In addition, the increase in LT and decrease in ACD-lens during accommodation suggest anterior ICL movement during accommodation. However, an increase in LT would induce a decrease in vault. Therefore, it is essential to keep illumination and, consequently, the pupil size, constant during examination of the effects of accommodation.
Footnotes
K. Shimizu is a consultant to STAAR Surgical. The remaining authors have no funding or conflicts of interest to disclose.
REFERENCES
- 1.Kamiya K, Igarashi A, Shimizu K, et al. Visual performance after posterior chamber phakic intraocular lens implantation and wavefront-guided laser in situ keratomileusis for low to moderate myopia. Am J Ophthalmol. 2013;153:1178–1186. [DOI] [PubMed] [Google Scholar]
- 2.Igarashi A, Kamiya K, Shimizu K, et al. Visual performance after implantable collamer lens implantation and wavefront-guided laser in situ keratomileusis for high myopia. Am J Ophthalmol. 2009;148:164–170. [DOI] [PubMed] [Google Scholar]
- 3.Dougherty PJ, Priver T. Refractive outcomes and safety of the implantable collamer lens in young low-to-moderate myopes. Clin Ophthalmol. 2017;11:273–277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kobashi H, Kamiya K, Igarashi A, et al. Long-term quality of life after posterior chamber phakic intraocular lens implantation and after wavefront-guided laser in situ keratomileusis for myopia. J Cataract Refract Surg. 2014;40:2019–2024. [DOI] [PubMed] [Google Scholar]
- 5.Igarashi A, Shimizu K, Kamiya K. Eight-year follow-up of posterior chamber phakic intraocular lens implantation for moderate to high myopia. Am J Ophthalmol. 2014;157:532–539. [DOI] [PubMed] [Google Scholar]
- 6.Shimizu K, Kamiya K, Igarashi A, et al. Early clinical outcomes of implantation of posterior chamber phakic intraocular lens with a central hole (Hole ICL) for moderate to high myopia. Br J Ophthalmol. 2012;96:409–412. [DOI] [PubMed] [Google Scholar]
- 7.Kamiya K, Shimizu K, Igarashi A, et al. Posterior chamber phakic intraocular lens implantation: comparative, multicentre study in 351 eyes with low-to-moderate or high myopia. Br J Ophthalmol. 2018;102:177–181. [DOI] [PubMed] [Google Scholar]
- 8.Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol. 2016;10:1059–1077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Petternel V, Köppl CM, Dejaco-Ruhswurm I, et al. Effect of accommodation and pupil size on the movement of a posterior chamber lens in the phakic eye. Ophthalmology. 2004;111:325–331. [DOI] [PubMed] [Google Scholar]
- 10.Lee H, Kang SY, Seo KY, et al. Dynamic vaulting changes in V4c versus V4 posterior chamber phakic lenses under differing lighting conditions. Am J Ophthalmol. 2014;158:1199–1204. [DOI] [PubMed] [Google Scholar]
- 11.Lindland A, Heger H, Kugelberg M, et al. Changes in vaulting of myopic and toric implantable collamer lenses in different lighting conditions. Acta Ophthalmol. 2012;90:788–791. [DOI] [PubMed] [Google Scholar]
- 12.Lindland A, Heger H, Kugelberg M, et al. Vaulting of myopic and toric implantable collamer lenses during accommodation measured with Visante optical coherence tomography. Ophthalmology. 2010;117:1245–1250. [DOI] [PubMed] [Google Scholar]
- 13.Lee H, Kang DS, Ha BJ, et al. Effect of accommodation on vaulting and movement of posterior chamber phakic lenses in eyes with implantable collamer lenses. Am J Ophthalmol. 2015;160:710–716. [DOI] [PubMed] [Google Scholar]
- 14.Kojimia T, Maeda M, Yoshida Y, et al. Posterior chamber phakic implantable collamer lens: changes in vault during 1 year. J Refract Surg. 2010;26:327–332. [DOI] [PubMed] [Google Scholar]
- 15.Yan Z, Miao H, Zhao F, et al. Two-year outcomes of Visian implantable collamer lens with a central hole for correcting high myopia. J Ophthalmol. 2018:1–9, Article ID 8678352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Klijn S, Sicam VA, Reus NJ. Long-term changes in intraocular lens position and corneal curvature after cataract surgery and their effect on refraction. J Cataract Refract Surg. 2016;42:35–43. [DOI] [PubMed] [Google Scholar]