

Abstract
Treatment of chronic Monteggia fracture-dislocations remains controversial in skeletally immature patients. The present study aimed to review the clinical outcomes of surgical treatment with an Ilizarov mini-fixator for chronic Monteggia fracture-dislocations in children. From April 2003 to March 2014, 5 pediatric patients (4 males, 1 female) with chronic Monteggia fracture-dislocation were treated with an Ilizarov mini-fixator at our institution. The median age at the time of surgery was 9 years (range 5–14 years), median duration from injury to surgery was 31 months (range 2–125 months), and median duration of follow-up was 12 months (range 11 months–10 years). All patients underwent opening wedge osteotomy of the proximal ulna followed by the application of an Ilizarov mini-fixator. Although closed reduction was attempted after ulnar osteotomy and application of the Ilizarov mini-fixator, open reduction of the radial head was required in all patients. In 4 patients, dense scar tissue in the radiocapitellar joint was excised to enable reduction of the radial head; the remaining patient had traumatic radioulnar synostosis, and underwent separation of the synostosis followed by anconeus interposition arthroplasty. No patient received bone grafting at the ulnar osteotomy site, repair or reconstruction of the annular ligament, or temporary fixation of the radial head with transarticular wire. The median period of external fixation was 10 weeks (range 8–13 weeks). Although there were no severe complications such as deep infection and neurovascular disturbance, asymptomatic radial head subluxation occurred in 2 patients. The patient with traumatic synostosis had residual posterior subluxation with limitation of forearm rotation, and another patient with radial head enlargement had residual anterior subluxation. The median postoperative ranges of motion in pronation, supination, extension, and flexion were 90°, 90°, 0°, and 140°, respectively. The median Kim's elbow performance score was 65 (range 50–75) preoperatively, which improved to 94 (range 80–100) at final follow-up. The outcome was rated as excellent in 4 cases, and good in 1. In pediatric chronic Monteggia fracture-dislocations, ulnar osteotomy followed by the application of an Ilizarov mini-fixator is a viable option that is less invasive than plate fixation.
Keywords: chronic Monteggia fracture-dislocation, Ilizarov mini-fixator, malunion, opening wedge osteotomy, radial head dislocation
1. Introduction
Chronic Monteggia fracture-dislocations involve persistent plastic deformation or malunion of the ulna with concomitant unreduced dislocation of the radial head,[1–17] which are uncommon injuries in children. Chronic Monteggia fracture-dislocations are usually defined as those that are present more than 4 weeks after injury,[1,16] and this delay after injury makes the treatment challenging.[1,10] The treatment of persistent unreduced dislocation of the radial head in skeletally immature patients is still controversial.[1–3,5,7–10,14–23] As there is limited conflicting evidence regarding the treatment of these injuries, a non-surgical approach was advocated in the past.[24] However, some reports indicate that the injuries occasionally result in marked disability, including residual pain, stiffness of the elbow joint, neurological compromise, deformity of the elbow, osteoarthritis, and even instability of the distal radioulnar joint.[1,4,15,25] Treatment of chronic Monteggia fracture-dislocation via watchful waiting has not been recommended in recent studies.[1,4,10,15]
Surgical treatment of chronic Monteggia fracture-dislocations poses several challenges. Restoration of the alignment of the radiocapitellar joint is important for satisfactory long-term functional outcome.[6,10,23,26,27] Many authors have described various operative procedures for the treatment of chronic Monteggia fracture-dislocations, including only open reduction of the radial head dislocation, open reduction of the dislocation combined with opening wedge osteotomy of the ulna, and a combination of open reduction and ulnar osteotomy with or without annular ligament reconstruction;[1–3,5,7–10,14–23] however, the optimal treatment remains unclear. Furthermore, there are 2 main procedures used for the fixation of the osteotomy of the ulna: plate fixation[6,7,14,15,17,27–32] and application of external fixation.[23,33,34] These fixation procedures both have advantages and disadvantages. Plate fixation obtains rigid fixation, but is more invasive than external fixation, while external fixation can result in pin tract infection.[23,34]
In our institution, an Ilizarov mini-fixator (Ito Medical Instrument, Tokyo, Japan) has been used for chronic Monteggia fracture-dislocations in children since 2003. The mini-fixator enables correction of the angular and rotational deformity of the ulna, which allows controlled reduction of the radial head. The purpose of the present study was to present the clinical outcomes of opening wedge osteotomy of the ulna combined with the application of an Ilizarov mini-fixator for chronic Monteggia fracture-dislocations in children.
2. Materials and methods
The present case series was treated at our institution. Patient demographic characteristics, medical history, imaging findings, and follow-up data were retrospectively extracted from the medical records.
2.1. Patients
A total of 6 elbows in 6 patients aged less than 15 years with chronic Monteggia fracture-dislocations underwent opening wedge osteotomy of the proximal ulna[6] followed by the application of an Ilizarov mini-fixator between April 2003 and March 2014. One patient who was followed-up for less than 6 months postoperatively was excluded from the present study. A final total of 5 chronic Monteggia fracture-dislocations in 5 patients (4 males and 1 female) were evaluated by direct examination. The preoperative statuses of the 5 patients with chronic Monteggia fracture-dislocations are shown in Table 1. The median age at the time of injury was 5 years and 2 months (range 2.7–10.4 years), median age at the time of surgery was 9 years (range 5.2–14.2 years), median duration between initial injury and surgery was 31 months (range 2 to more than 125 months), and median follow-up period was 12 months (range 11 months to 9.6 years). According to the classification of Bado,[35] all 5 patients had type I fractures. Preoperatively, 1 patient had a traumatic radioulnar synostosis, and 1 other patient had radial head enlargement.
Table 1.
Preoperative status of five pediatric patients with chronic Monteggia fracture-dislocation.

2.2. Surgical techniques
All surgeries were performed by a hand surgeon (TS), with the patients under general anesthesia and a tourniquet applied. An external fixator (the Ilizarov mini-fixator developed by the Russian Ilizarov Scientific Center) was first applied to the ulna to provide external fixation (Fig. 1). The mini-fixator is able to link with all other units 3-dimensionally by combining the rod, hinge, and posts; it can also be used for bone elongation. Briefly, the dedicated pins (1.5 mm diameter) were inserted into the proximal and distal parts of the presumptive site of the ulnar osteotomy, and were attached to the Ilizarov mini-fixator units (Fig. 2A). Ulnar osteotomy was performed through a 1 cm skin incision at the proximal third of the ulna, or at the fracture site (Fig. 2B). After osteotomy of the ulna, each of the fixator units was held, and the proximal ulna was angulated to enable closed reduction of the radial head (Fig. 2C). When anatomical reduction of the radial head was unable to be obtained, open reduction was performed using the Boyd approach.[24] An incision was started approximately 2.5 cm proximal to the elbow joint just lateral to the triceps tendon, and extended distally over the lateral side of the elbow tip to the olecranon on the medial side. The anconeus and extensor carpi ulnaris on the lateral side were then separated from the ulna. After the anconeus muscle was elevated from the bone and reflected radially, the dislocated radial head was reduced by manipulation under direct visualization.
Figure 1.
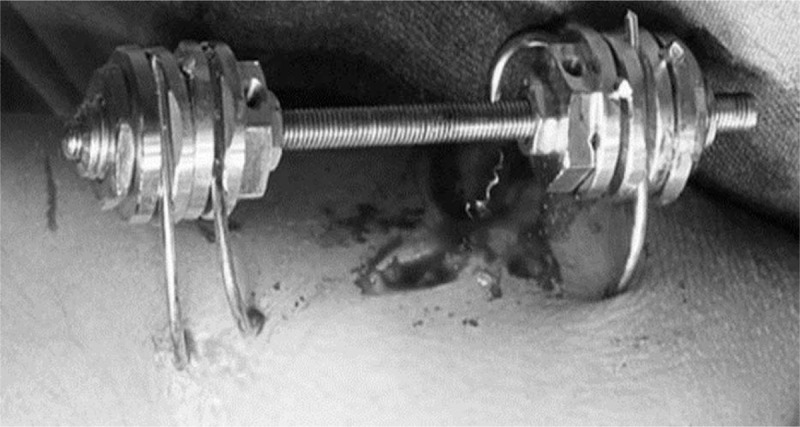
The Ilizarov mini-fixator, developed for external fixation by the Russian Ilizarov Scientific Center.
Figure 2.
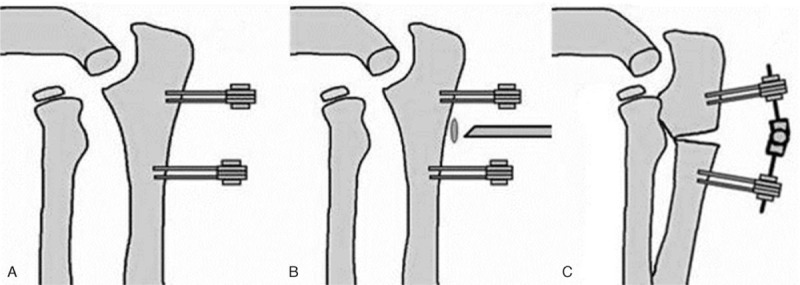
Illustrations demonstrating the application of the Ilizarov mini-fixator. A. The dedicated pins (1.5 mm diameter) are inserted into the proximal and distal parts of the presumptive site of the ulnar osteotomy, and attached to the Ilizarov mini-fixator units. B. Ulnar osteotomy is performed through a 1 cm skin incision at the proximal third of the ulna or at the fracture site. C. Each fixator unit is held and the proximal ulna is angulated to attempt closed reduction of the radial head.
In the patient with a post-traumatic radioulnar synostosis, the synostosis was exposed and separated while care was taken to protect the vascular and nervous structures. After the separation of the synostosis, the anconeus muscle was interposed around the ulna and anchored to the radial tuberosity.[36,37] Briefly, the proximal anconeus muscle was elevated as a full-thickness myofascial flap, which was then raised subperiosteally off the proximal ulna to its origin on the lateral epicondyle. The proximal attachment of the anconeus muscle was left intact at the lateral aspect of the olecranon to preserve the vascular pedicle. The forearm was pronated, and the distal tip of the flap was sutured to the periosteum of the radial tuberosity.
After the osteotomized ulna was angulated and the radial head was reduced, the Ilizarov mini-fixator units were fixed. No patient underwent bone grafting at the osteotomized site of the ulna, repair or reconstruction of the annular ligament, or temporary fixation of the radial head with a transarticular wire. A representative case is shown in Fig. 3. Active range of motion (ROM) exercise was encouraged immediately after surgery.
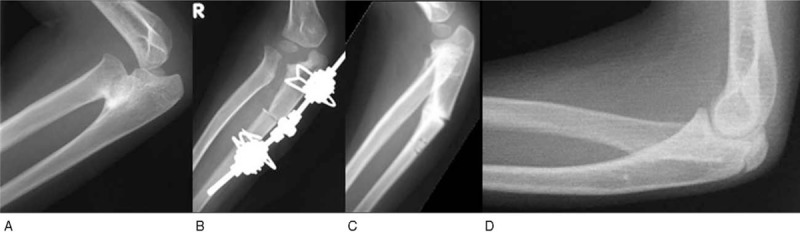
Figure 3.
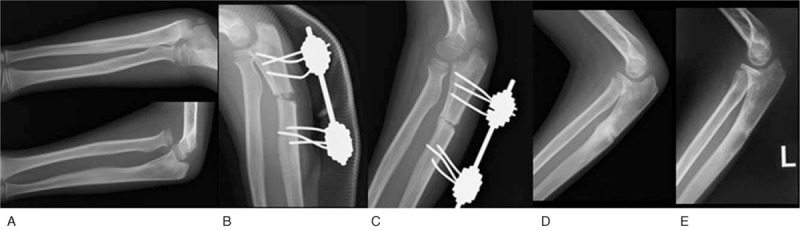
Radiographs from case 3: a 5-year-old male. A. Preoperative anteroposterior and lateral views. B. Postoperative lateral view. C. Four months after surgery. D. Two months after surgery. E. Twelve months after surgery.
2.3. Postoperative evaluation
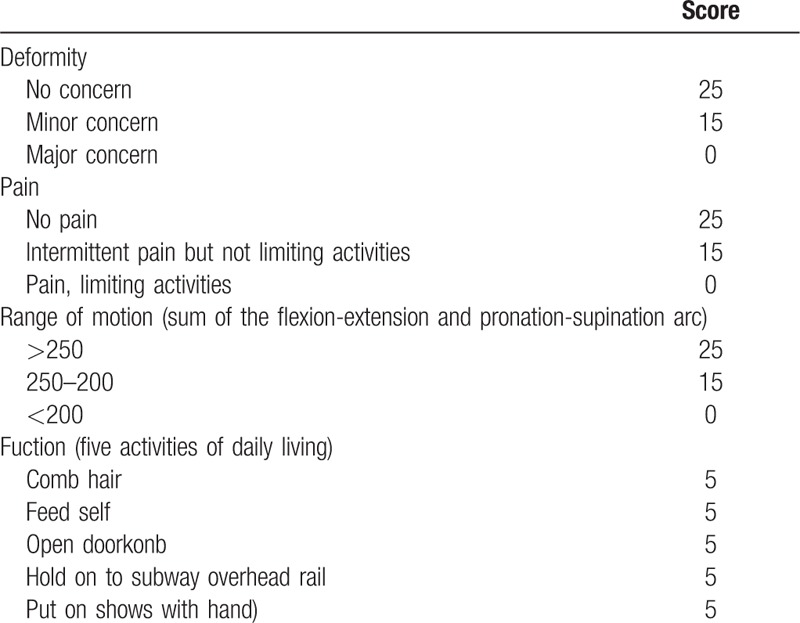
The median duration of external fixation was investigated. When open reduction of the radial head was required, the perioperative factors inhibiting reduction of the radial head were investigated. Postoperative complications were evaluated, including pin infection or neurovascular lesion. Clinical outcomes (including pain or discomfort of the elbow joint), pre- and postoperative ROM for forearm pronation/supination and elbow extension/flexion, and Kim's elbow performance scores (Table 2)[15] were evaluated. Anteroposterior and lateral radiographs were used to evaluate the congruency of the radiocapitellar joint and the presence of any deformity or arthritic changes.
Table 2.
Kim's elbow performance scoring system[15].
3. Results
The postoperative outcomes of the 5 pediatric patients with chronic Monteggia fracture-dislocations are shown in Table 3. The median duration of external fixation was 10 weeks (range 8–13 weeks). The patient with post-traumatic radioulnar synostosis (case 1) required open reduction of the radial head after separation of the synostosis. Four patients (cases 2–5) initially underwent attempted closed reduction of the radial head after application of the mini-fixator and opening wedge osteotomy of the ulna; however, anatomical reduction of the radial head was not obtained. As a result, open reduction of radial head was required. The annular ligament was not identifiable in all patients. The dense fibrous tissue surrounding the dislocated radial head seemed to be fibrous scar tissue and the remnants of the annular ligament; this was interposed between the radiocapitellar joint, and inhibited the anatomical reduction.
Table 3.
Postoperative outcome of 5 pediatric patients with chronic Monteggia fracture-dislocation.

There were no severe complications, such as pin infection or neurovascular disturbance. Bone union of the ulna was obtained in all patients. Although the alignment of the radial head was restored in 3 of 5 patients, 2 patients had residual subluxation of the radial head. One patient (case 1) who had post-traumatic radioulnar synostosis had posterior subluxation of the radial head (Fig. 4). Another patient with radial head enlargement preoperatively (case 5) had residual anterior subluxation of the radial head on radiography at final follow-up (Fig. 5).
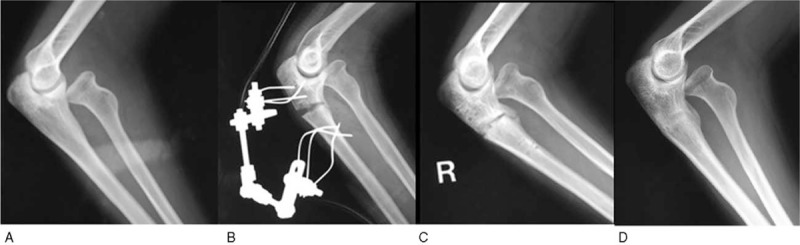
Figure 4.
Radiographs from case 1: a 2-year-old male with post-traumatic radioulnar synostosis. A. Preoperative lateral view. B. Postoperative lateral view. C. Two months after surgery. D. Posterior subluxation of the radial head was present 9 years postoperatively.
Figure 5.
Radiographs from case 5: a 14-year-old female with preoperative radial head enlargement. A. Preoperative lateral view. B. Postoperative lateral view. C. Two months after surgery. D. Anterior subluxation of the radial head was present 12 months postoperatively.
The pre- and postoperative ROM and the arcs of the forearm and elbow joint are shown in Table 4. The median postoperative ROM in pronation, supination, extension, and flexion were 90°, 90°, 0°, and 140°, respectively. At final follow-up, the median pronation-supination arc was 180° (range 110–180°) and the median extension-flexion arc was 135° (range 130–150°); the median increases in the pronation-supination arc and the extension-flexion arc were 0° and 15°, respectively. The median preoperative Kim's elbow performance score was 65 (range 50–75), which improved to 100 (range 80–100) at final follow-up. Four outcomes were rated as excellent, and 1 as good (Table 5).
Table 4.
Pre- and postoperative ranges of motion and arcs of the forearm and elbow joint.

Table 5.
Pre- and postoperative Kim's elbow performance scores[15].

4. Discussion
The treatment of Monteggia fracture-dislocations that have been present for more than 4 weeks poses several challenges.[16] Although closed reduction of the dislocated radial head should initially be attempted, it is rarely successful.[1] In our case series, closed reduction of the radial head was blocked by the presence of dense fibrous scar tissue, which was the remnant of the annular ligament. Lädermann et al[21] reported that open reduction may only be required in cases in which anatomical reduction of the radial head cannot be obtained by closed reduction after ulnar osteotomy. However, dense fibrous scar tissue between the radial head and the radiocapitellar joint is the most common finding in cases in which open reduction is performed[1,6,8,28,29,33,38]; the presence of this scar tissue in chronic Monteggia fracture-dislocations means that open reduction is inevitable.[1,10]
The necessity of reconstruction of the annular ligament remains controversial.[1–3,5,7–10,14–23] Some authors have reported that opening wedge osteotomy of the ulna followed by open reduction is sufficient to maintain the alignment of the radiocapitellar joint and radial head.[29,33,39] In our case series, anatomical reduction of the radial head was obtained without reconstruction of the annular ligament in 3 of 4 patients, excluding the patient with post-traumatic radioulnar synostosis. One patient had residual anterior subluxation of the radial head; this was caused by the enlargement of the radial head, which resulted in malalignment of the radiocapitellar joint head and residual subluxation. Thus, congruence of the radiocapitellar joint is essential for the anatomical reduction of the radial head.[6,10,23,26,27] The patient with the synostosis had instability of the radial head after the separation of the synostosis. However, anchoring the interposed anconeus muscle to the radial tuberosity tethered and stabilized the radial neck. Thus, reconstruction of annular ligament was not needed. Hirayama et al[6] reported that hyperangulation and lengthening of the ulna stabilized the radial head due to the interosseous membrane, which is the stabilizer of the radial head in the absence of the annular ligament. Moreover, annular ligament reconstruction frequently results in restriction of forearm rotation (especially pronation).[1,7,8,27,38,39] Thus, annular ligament reconstruction is not necessarily appropriate.
The most common mode of treatment for chronic Monteggia fracture-dislocation is opening wedge osteotomy of the ulna followed by open reduction of radial dislocation.[1] After performing ulnar osteotomy to enable the reduction of the radial head, there are 2 main choices for the fixation of the osteotomized ulna: plate fixation[6,7,14,15,17,27–32] or application of an external fixator.[22,23,33,34]
Plate fixation has the advantage of more rigid and stable fixation of the osteotomized ulna than external fixation. However, plate fixation is invasive and disrupts the blood supply of the ulnar periosteum. In addition, plate removal in children requires general anaesthesia. Application of an external fixator is less invasive than plate fixation. Furthermore, the fixator enables correction of both angular and rotational deformity of the ulna, which enables controlled reduction of the radial head. Removal of the fixator can be done without anesthesia in an ambulatory care faculty. However, external fixation can occasionally cause pin tract infection.[23,34]
Although both plate fixation and external fixation obtain stable fixation of the osteotomized ulna, the Ilizarov-mini fixator has primarily been used in our institution since 2003. The application of a unilateral external fixator has been proposed for ulnar correction.[22,23] Exner[22] reported the technique of gradual lengthening and angulation of the ulna using callotasis in 2 cases of chronic Monteggia fracture-dislocation; however, this requires additional angulation and lengthening of the ulna under general anesthesia or sedation.[22] Kawoosa et al[19] firstly reported the treatment of 2 chronic Monteggia fracture-dislocations using the Ilizarov technique with an Ilizarov 2-ring frame in the English literature, but the ring frame would be problematic in children. Also, the presence of the superimposing proximal steel ring makes it difficult to determine reduction of the radial head on intraoperative radiography.[19]
The present study is the first report that proposed the Ilizarov-mini fixator for chronic Monteggia fracture-dislocations in children. The Ilizarov mini-fixator enables 3-dimensional insertion of the 3 dedicated pins (1.5 mm diameter) into each fragment of the proximal and distal ulna, which provides stable fixation. Thus, the Ilizarov mini-fixator results in stable fixation, which maintains the function of the arm after the application of the fixator, and allows patients to perform intensive hand therapy. Moreover, anesthesia is not required for postoperative angle adjustment and bone elongation after osteotomy without bone grafts.
We performed angulated ulnar osteotomy after the application of the Ilizarov mini-fixator in 5 cases of chronic Monteggia fracture-dislocation in children. The clinical results were good in 3 of 5 patients. Although the other 2 patients had residual subluxation of the radial head, acceptable results were obtained without substantial complications due to the fixator. The Ilizarov Mini-fixator is less invasive than plate fixation, and is a good option for treatment of chronic Monteggia fracture-dislocations in children.
The major limitations of the present study include the small sample size and the short follow-up periods. Long-term observation of additional patients is needed to evaluate the development of osteoarthritis of the radiocapitellar joint after treatment of chronic Monteggia fracture-dislocations.
5. Conclusion
We performed angulated ulnar osteotomy after the application of an Ilizarov mini-fixator in 5 children suffering from chronic Monteggia fracture-dislocation. The Ilizarov mini-fixator is less invasive than plate fixation, and is a good option for the treatment of chronic Monteggia fracture-dislocations in children.
Acknowledgment
We thank Kelly Zammit, BVSc, from Edanz Group (www.edanzediting.com/ac), for editing a draft of this manuscript.
Author contributions
Conceptualization: Yuji Tomori.
Data curation: Yuji Tomori.
Investigation: Masaki Take, Yuji Tomori.
Project administration: Takuya Sawaizumi, Yuji Tomori.
Supervision: Shinro Takai and Takuya Sawaizumi.
Writing – original draft: Masaki Take and Yuji Tomori.
Writing – review & editing: Yuji Tomori, Tokifumi Majima, Mitsuhiko Nanno, and Shinro Takai.
Footnotes
Abbreviation: ROM = range of motion.
Takuya Sawaizumi deceased 5 May 2015.
This study was not supported by any funding source.
The present study was a retrospective, human, non-interventional study. According to public health law in Japan, institutional review board approval is not required for human non-interventional studies. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. Informed consent was obtained from the guardians of all patients for surgery and for case publication.
Informed consent was obtained from all individual participants included in the study.
The authors declare no conflicts of interest.
References
- [1].Goyal T, Arora SS, Banerjee S, et al. Neglected Monteggia fracture dislocations in children: a systematic review. J Pediatr Orthop B 2015;24:191–9. [DOI] [PubMed] [Google Scholar]
- [2].Bhaskar A. Missed Monteggia fracture in children: Is annular ligament reconstruction always required? Indian J Orthop 2009;43:389–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Delpont M, Jouve JL, Sales de Gauzy J, et al. Proximal ulnar osteotomy in the treatment of neglected childhood Monteggia lesion. Orthop Traumatol Surg Res 2014;100:803–7. [DOI] [PubMed] [Google Scholar]
- [4].Freedman L, Luk K, Leong JC. Radial head reduction after a missed Monteggia fracture: brief report. J Bone Joint Surg Br 1988;70:846–7. [DOI] [PubMed] [Google Scholar]
- [5].Gyr BM, Stevens PM, Smith JT. Chronic Monteggia fractures in children: outcome after treatment with the Bell-Tawse procedure. J Pediatr Orthop B 2004;13:402–6. [DOI] [PubMed] [Google Scholar]
- [6].Hirayama T, Takemitsu Y, Yagihara K, et al. Operation for chronic dislocation of the radial head in children. Reduction by osteotomy of the ulna. J Bone Joint Surg Br 1987;69:639–42. [DOI] [PubMed] [Google Scholar]
- [7].Horii E, Nakamura R, Koh S, et al. Surgical treatment for chronic radial head dislocation. J Bone Joint Surg Am 2002;84-A:1183–8. [DOI] [PubMed] [Google Scholar]
- [8].Hui JH, Sulaiman AR, Lee HC, et al. Open reduction and annular ligament reconstruction with fascia of the forearm in chronic monteggia lesions in children. J Pediatr Orthop 2005;25:501–6. [DOI] [PubMed] [Google Scholar]
- [9].Hurst LC, Dubrow EN. Surgical treatment of symptomatic chronic radial head dislocation: a neglected Monteggia fracture. J Pediatr Orthop 1983;3:227–30. [DOI] [PubMed] [Google Scholar]
- [10].Kim HT, Conjares JN, Suh JT, et al. Chronic radial head dislocation in children, Part 1: pathologic changes preventing stable reduction and surgical correction. J Pediatr Orthop 2002;22:583–90. [PubMed] [Google Scholar]
- [11].Lu X, Yan G, Wang Y, et al. Repositioning of the annular ligament in the management of missed Monteggia fracture. J Pediatr Orthop 2017;37:20–2. [DOI] [PubMed] [Google Scholar]
- [12].Park H, Park KW, Park KB, et al. Impact of open reduction on surgical strategies for missed Monteggia fracture in children. Yonsei Med J 2017;58:829–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Song KS, Ramnani K, Bae KC, et al. Indirect reduction of the radial head in children with chronic Monteggia lesions. J Orthop Trauma 2012;26:597–601. [DOI] [PubMed] [Google Scholar]
- [14].Wang MN, Chang WN. Chronic posttraumatic anterior dislocation of the radial head in children: thirteen cases treated by open reduction, ulnar osteotomy, and annular ligament reconstruction through a Boyd incision. J Orthop Trauma 2006;20:1–5. [DOI] [PubMed] [Google Scholar]
- [15].Kim HT, Park BG, Suh JT, et al. Chronic radial head dislocation in children, Part 2: results of open treatment and factors affecting final outcome. J Pediatr Orthop 2002;22:591–7. [PubMed] [Google Scholar]
- [16].Rodgers WB, Waters PM, Hall JE. Chronic Monteggia lesions in children. Complications and results of reconstruction. J Bone Joint Surg Am 1996;78:1322–9. [DOI] [PubMed] [Google Scholar]
- [17].Tajima T, Yoshizu T. Treatment of long-standing dislocation of the radial head in neglected Monteggia fractures. J Hand Surg Am 1995;20(3 Pt 2):S91–94. [DOI] [PubMed] [Google Scholar]
- [18].Datta T, Chatterjee N, Pal AK, et al. Evaluation of outcome of corrective ulnar osteotomy with bone grafting and annular ligament reconstruction in neglected monteggia fracture dislocation in children. J Clin Diagn Res 2014;8:LC10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Kawoosa AA, Dhar SA, Butt MF, et al. Stable relocation of the radial head without annular ligament reconstruction using the Ilizarov technique to treat neglected Monteggia fracture: two case reports. J Med Case Rep 2010;4:344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Koslowsky TC, Mader K, Wulke AP, et al. Operative treatment of chronic Monteggia lesion in younger children: a report of three cases. J Shoulder Elbow Surg 2006;15:119–21. [DOI] [PubMed] [Google Scholar]
- [21].Lädermann A, Ceroni D, Lefèvre Y, et al. Surgical treatment of missed Monteggia lesions in children. J Child Orthop 2007;1:237–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Exner GU. Missed chronic anterior Monteggia lesion. Closed reduction by gradual lengthening and angulation of the ulna. J Bone Joint Surg Br 2001;83:547–50. [DOI] [PubMed] [Google Scholar]
- [23].Hasler CC, Von Laer L, Hell AK. Open reduction, ulnar osteotomy and external fixation for chronic anterior dislocation of the head of the radius. J Bone Joint Surg Br 2005;87:88–94. [PubMed] [Google Scholar]
- [24].Boyd HB, Boals JC. The Monteggia lesion. A review of 159 cases. Clin Orthop Relat Res 1969;66:94–100. [PubMed] [Google Scholar]
- [25].Nishimura M, Itsubo T, Horii E, et al. Tardy ulnar nerve palsy caused by chronic radial head dislocation after Monteggia fracture: a report of two cases. J Pediatr Orthop B 2016;25:450–3. [DOI] [PubMed] [Google Scholar]
- [26].Inoue G, Shionoya K. Corrective ulnar osteotomy for malunited anterior Monteggia lesions in children. 12 patients followed for 1-12 years. Acta Orthop Scand 1998;69:73–6. [DOI] [PubMed] [Google Scholar]
- [27].Stoll TM, Willis RB, Paterson DC. Treatment of the missed Monteggia fracture in the child. J Bone Joint Surg Br 1992;74:436–40. [DOI] [PubMed] [Google Scholar]
- [28].Belangero WD, Livani B, Zogaib RK. Treatment of chronic radial head dislocations in children. Int Orthop 2007;31:151–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Degreef I, De Smet L. Missed radial head dislocations in children associated with ulnar deformation: treatment by open reduction and ulnar osteotomy. J Orthop Trauma 2004;18:375–8. [DOI] [PubMed] [Google Scholar]
- [30].Eygendaal D, Hillen RJ. Open reduction and corrective ulnar osteotomy for missed radial head dislocations in children. Strategies Trauma Limb Reconstr 2007;2:31–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Kemnitz S, De Schrijver F, De Smet L. Radial head dislocation with plastic deformation of the ulna in children. A rare and frequently missed condition. Acta Orthop Belg 2000;66:359–62. [PubMed] [Google Scholar]
- [32].Nakamura K, Hirachi K, Uchiyama S, et al. Long-term clinical and radiographic outcomes after open reduction for missed Monteggia fracture-dislocations in children. J Bone Joint Surg Am 2009;91:1394–404. [DOI] [PubMed] [Google Scholar]
- [33].Lu X, Kun Wang Y, Zhang J, et al. Management of missed Monteggia fractures with ulnar osteotomy, open reduction, and dual-socket external fixation. J Pediatr Orthop 2013;33:398–402. [DOI] [PubMed] [Google Scholar]
- [34].Bor N, Rubin G, Rozen N, et al. Chronic anterior Monteggia lesions in children: report of 4 cases treated with closed reduction by ulnar osteotomy and external fixation. J Pediatr Orthop 2015;35:7–10. [DOI] [PubMed] [Google Scholar]
- [35].Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50:71–86. [PubMed] [Google Scholar]
- [36].Daluiski A, Schreiber JJ, Paul S, et al. Outcomes of anconeus interposition for proximal radioulnar synostosis. J Shoulder Elbow Surg 2014;23:1882–7. [DOI] [PubMed] [Google Scholar]
- [37].Bell SN, Benger D. Management of radioulnar synostosis with mobilization, anconeus interposition, and a forearm rotation assist splint. J Shoulder Elbow Surg 1999;8:621–4. [DOI] [PubMed] [Google Scholar]
- [38].Seel MJ, Peterson HA. Management of chronic posttraumatic radial head dislocation in children. J Pediatr Orthop 1999;19:306–12. [PubMed] [Google Scholar]
- [39].Devnani AS. Missed Monteggia fracture dislocation in children. Injury 1997;28:131–3. [DOI] [PubMed] [Google Scholar]