

Abstract
This study aims to evaluate the clinic value of ultrasound, computed tomography (CT) and serological testing in the differentiation between hepatic Cystic Echinococcosis (CE) types 1 and simple hepatic cysts.
Totally 50 patients with CE Types 1 and 50 patients with simple hepatic cysts were included. All patients examined by ultrasound, CT and serological testing respectively. The receiver operating characteristic (ROC) curve of diagnosis methods was drawn and their sensitivity, specificity, Youden index, positive likelihood ratio, negative likelihood ratio, positive predictive value and negative predictive value were compared. Pathology result was used as golden standard.
The area under ROC curve of ultrasound was 0.97 and of CT and serological testing was 0.79 and 0.71 respectively. The sensitivity of ultrasound in the diagnosis of CE Types 1 was 96.00%, specificity was 98.00%, the positive likelihood ratio was 48.00, and negative likelihood ratio was 0.04. Disease prevalence was 50%, positive predictive value was 97.96%, and negative predictive value was 96.08%. The sensitivity of CT was 80.00%, specificity was 62.00%, positive likelihood ratio was 2.11, and negative likelihood ratio was 0.32. Disease prevalence was 50%, positive predictive value was 67.80%, and negative predictive value was 75.61%. The sensitivity of immunological test was 86.00%, specificity was 72.00%, positive likelihood ratio was 3.07, and negative likelihood ratio was 0.19. Disease prevalence was 50%, positive predictive value was 75.44%, and negative predictive value was 83.72%. Combined ultrasound and immunological test, the sensitivity and the specificity was 82% and 100% respectively. Combined CT and immunological test, the sensitivity the specificity was 70% and 82% respectively.
In the differentiate diagnosis of CE Types 1 and simple hepatic cyst, ultrasound is better than CT with high sensitivity and specificity, therefore recommended. Immunological examination is an important complement to the imaging examination.
Keywords: differentiation, hepatic cystic echinococcosis, simple hepatic cysts
1. Introduction
Cystic hydatid disease is an important parasitic zoonosis caused by the larval cyst stage of the dog tapeworm Echinococcus granulosus which impacts on both population health and animal production in hyper endemic areas in Central Asia, the Mediterranean countries and South America.[1] Surgery has been considered as the only definitive and curative method.[2] Simple hepatic cyst is also known as congenital hepatic cyst, a condition that may be related to congenital biliary developmental aberrations.[3] Simple hepatic cysts grow slowly and usually require no specific treatment except in cases of complications, such as intracystic hemorrhage, infection, cyst rupture, jaundice, or portal hypertension.[4] The clinical manifestations and laboratory and imaging findings are similar and are particularly difficult to differentiate between Hepatic Cystic Echinococcosis (CE) Type 1 and simple hepatic cysts.[5–7] However, wrong diagnosis may lead to severe clinical outcome.[8,9] For example, if CE Types 1 misdiagnosed as simple hepatic cysts, surgery will be performed, leading to cyst fluid overflow spread in abdominal cavity or even anaphylactic shock; therefore, a clear diagnosis is very important. Ultrasound, CT and serological testing are important methods for disease differentiation.[10] Therefore, a retrospective analysis was conducted and the diagnostic value of each combined detection method was evaluated.
2. Materials and methods
2.1. Patients
A total of 50 patients with CE type 1 and 50 patients with simple hepatic cysts were enrolled, and they were diagnosed by pathology. All patients underwent ultrasound, CT and serological testing before surgery. This study was approved by the Ethical Committees of The First Affiliated Hospital of Xinjiang Medical University
2.2. Ultrasound
Ultrasound was performed using the Siemens G60 color Doppler ultrasound imaging instrument and convex array probe with the frequency of 3.5 to 5.0 MHz. Patients were in supine or lateral position. Parenchymal echo and lesions, cyst size, number and its relationship with the surrounding blood vessels were recorded.
2.3. CT detection
The scanning parameters include layer thickness of 5 mm, layer space of 5 mm, tube voltage of 120 KV, tube current of 300 mA and automatic milliampomy. The ROI was selected according to the contour of the lesion. The CT value (mean and standard deviation (SD)) of the ROI was recorded.
2.4. Immunological tests
The dot immunogold filtration assay was used to detect the antibodies of EgCF, EgP, EgB, and Em2. All patients underwent immunological tests before surgery.
2.5. Statistical analysis
All data were analyzed using SPSS version 22.0. Comparison between the 2 groups was performed by the Student's t test for continuous variables and the Chi-squared test for categorical variables. P value less than .05 was considered as statistically significant.
3. Results
3.1. Patient characteristics
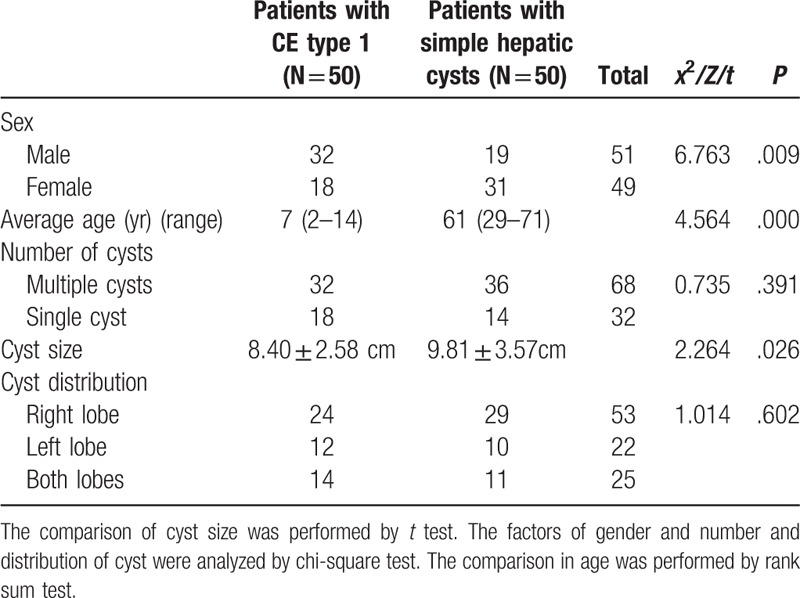
The clinical data of patients were shown in Table 1. Among 50 patients with CE type 1, 32 cases were male, and 18 cases were female. Patients aged 2 to 14 years old and the median age was 7. A total of 32 cases had multiple cysts, and 18 cases had single cyst. The cysts were located in the right lobe in 24 patients, in the left lobe in 12 patients, and in both lobes in 14 patients. The mean cyst size was 8.40 ± 2.58 cm (range 5–14 cm) in diameter. Among 50 patients with simple hepatic cysts, 19 were males and 31 females. Patients aged 29 to 71 years with the median age of 61 years. A total of 36 cases had multiple cysts, and 14 cases had single cyst. The cysts were located in the right lobe in 29 patients, in the left lobe in 10 patients, and in both lobes in 11 patients. The mean cyst size was 9.81 ± 3.57 cm (range 7–13 cm) in diameter. One patient in CE group developed hydrothorax at 5 days post-operation and was treated by thoracocentesis. Other patients recovered well after surgery. Patients were followed up for 1 to 3 years without recurrence.
Table 1.
The characteristics of patients.
3.2. Ultrasound
Diagnosis of CE types 1 was considered positive, and simple hepatic cystic was considered negative. All diagnoses were based on pathological diagnosis. Ultrasound was performed for detection of diagnostic value. The comparison value was shown in Figure 1. The sensitivity of the ultrasound is 96.00%, specificity was 98.00%, positive likelihood ratio was 48.00, negative likelihood ratio was 0.04, disease prevalence was 50%, positive predictive value was 97.96%, and negative predictive value was 96.08%.
Figure 1.
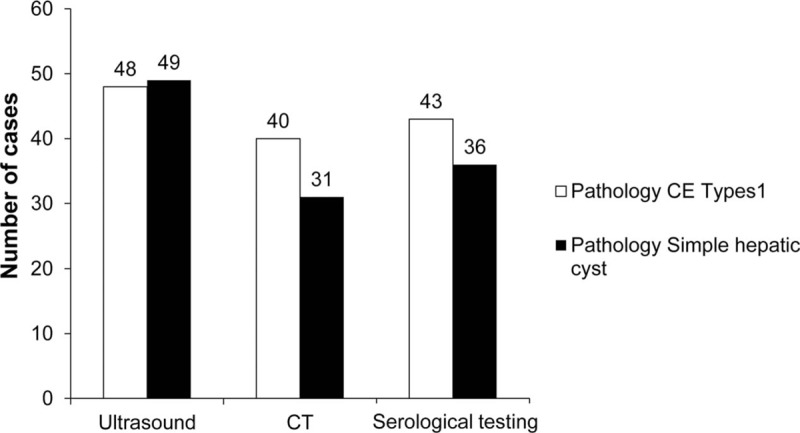
The diagnostic value of ultrasound, CT, and serological testing in liver cystic lesions. CT = computed tomography.
3.3. CT performance
CT scan was performed for detection of diagnostic value. The comparison value was shown in Figure 1. The sensitivity of CT was 80.00%, specificity was 62.00%, positive likelihood ratio was 2.11, negative likelihood ratio was 0.32, disease prevalence was 50%, positive predictive value was 67.80%, and negative predictive value was 75.61%.
3.4. Serological testing
Serological testing was performed for detection of diagnostic value. The comparison value was shown in Figure 1. The sensitivity of the immunological test was 86%, specificity was 72.00%, positive likelihood ratio was 3.07, negative likelihood ratio was 0.19, disease prevalence was 50%, positive predictive value was 75.44%, and negative predictive value was 83.72%.
3.5. Analysis ROC curve area
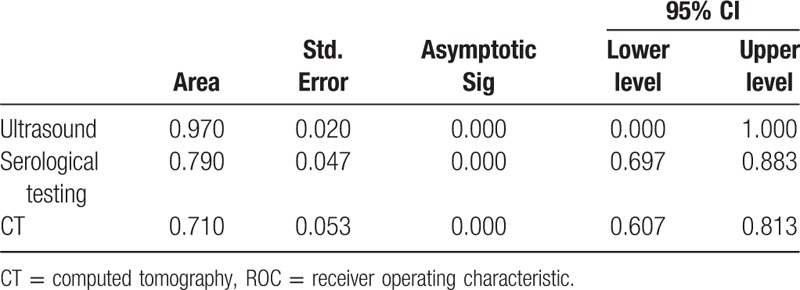
ROC was drawn to compare the diagnostic value of the ultrasound, CT and serological testing (Fig. 2). The larger the area under the ROC curve, the greater the value of differential diagnosis. The comparison value was shown in Table 2. The area under ROC curve of ultrasound was 0.97, CT and serological testing was 0.79 and 0.71 respectively. It showed that ultrasound is a preferred differential diagnosis tool.
Figure 2.
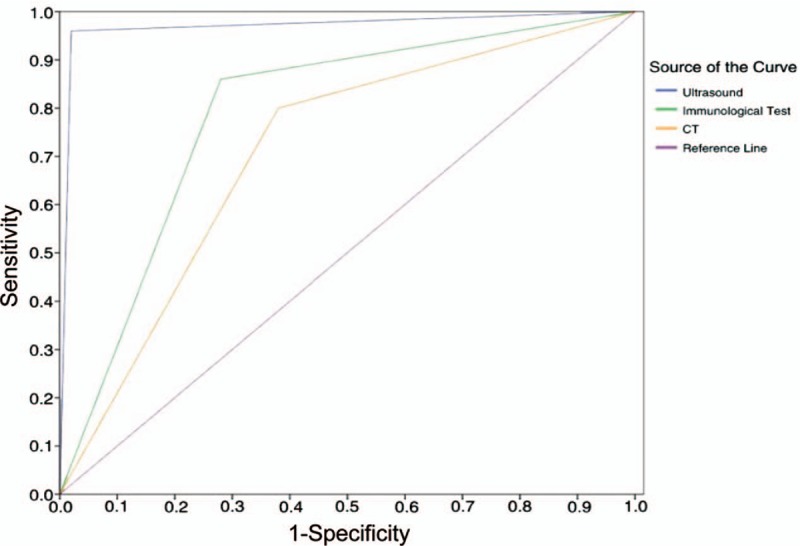
ROC analysis. ROC was used to compare the diagnostic value of the ultrasound, CT and serological testing. The area under ROC curve of ultrasound, CT and serological testing was 0.97, 0.79, and 0.71, respectively. CT = computed tomography, ROC = receiver operating characteristic.
Table 2.
The area under ROC curve of ultrasonography, CT and laboratory tests.
3.6. Combined analysis of ultrasound with serological testing
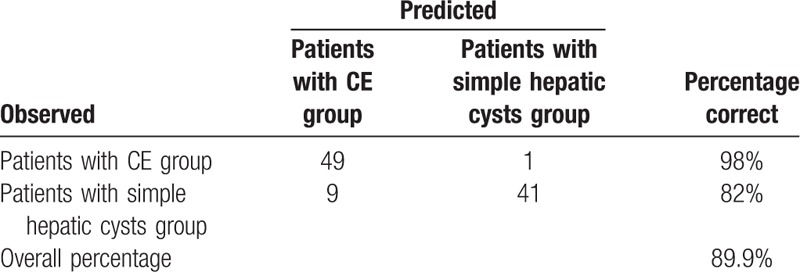
Combined diagnostic value of ultrasound with serological testing was evaluated. The combination was considered positive if both techniques were positive, and negative if both negative. The comparison value was shown in Table 3. The diagnostic sensitivity of this combination was 82%, and the specificity was 100%. Then we integrated the serological testing results and ultrasound into a diagnostic model, and performed logistic analysis (Table 4). The result showed that both ultrasound and serological testing were positive, which can increase 5.39 units in logistic P. And, the accuracy of positive results was 218-fold higher than that of negative ones. This result confirmed the validity of the model. And we evaluated the diagnostic value of the model through the misjudgment matrix of this model. It showed that in 50 patients with simple hepatic cysts, 49 patients were predicted correctly and the accuracy rate was 98%. And, in 50 patients with hepatic cystic echinococcosis types 1, 41 patients were predicted correctly with accuracy rate of 82%. The overall prediction rate of the model was 89.9% (Table 5). It showed that ultrasound combined with serological testing were the most reliable method for differential diagnosis of CE type1 and simple hepatic cyst.
Table 3.
The diagnostic value of combined test in liver cystic lesions.
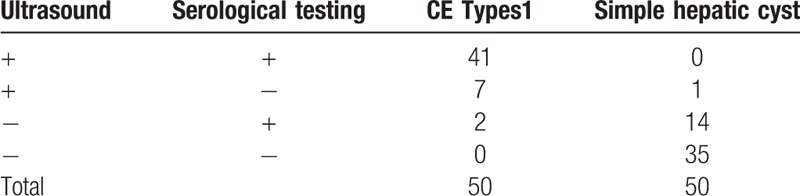
Table 4.
The results of logistic analysis of combined tests.

Table 5.
The diagnostic value of the model.
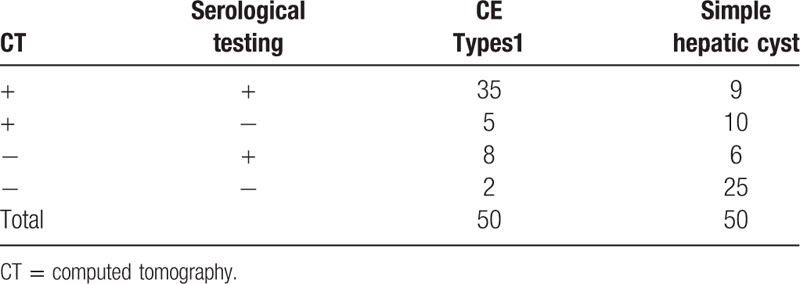
3.7. Combined analysis of CT with immunological test
Combined diagnostic value of CT with serological testing was evaluated. The combination was considered positive if both techniques were positive, and negative if both negative. The diagnostic sensitivity of this combination was 70%, and the specificity was 82%, as shown in Table 6.
Table 6.
The diagnostic value of combined test in liver cystic lesions.
4. Discussion
Echinococcosis is a zoonosis caused by the larval (metacestode) stages of cestodes (flat worms) belonging to the genus Echinococcus and the family Taeniidae.[11] The most common location for the development of hydatid cysts is the liver (50–70%).[12] According WHO-Informal Working Group Classification on Echinococcus (IWGE), Liver hydatid cyst were categorized into 5 types[13] and CE type 1 was an early stage. It showed unilocular cystic lesion with anechoic content, similar as the simple liver cysts. However, due to the significantly different treatments for these 2 diseases, a new diagnosis model is warranted to distinguish CE type1 and simple hepatic cyst preoperatively.
Ultrasound has become a widely used diagnostic technique for CE detection. The diagnostic criteria of ultrasound for CE are thick walled cystic lesions with 2 lines along the wall. These cysts usually have fine internal echoes.[14] In this study, the sensitivity and the specificity of ultrasound was 96% and 98% respectively, and it has higher value when compared with CT and serological testing. However, the results are dependent on user's technique and experience. For example, when patients are overweight or have intestinal gas accumulation, ultrasound may miss some of the lesions. In this study, only 2 patients with CE type 1 were misdiagnosed as simple hepatic cyst, and only 1 patient with simple hepatic cyst was misdiagnosed as CE type 1. If ultrasound combined with serological testing, the specificity can reach 100%. Based on our study, ultrasound is considered as a feasible, simple, fast, and cheap method for differential diagnosis of CE type1 and simple hepatic cyst.
The typical CT findings of hepatic cystic echinococcosis are water-like density of cystic lesions, calcification of the cyst wall, daughter cyst or collapsed inner cyst. Liver CE type 1 always showed a sharply defined homogeneous hypodense lesion with a CT value of 14 to 20 HU.[15] Differential diagnosis of CE type 1 from simple hepatic cyst using CT is difficult. CT can diagnose or differentially diagnose them based on CT values.[16] When compared the CT values of hepatic hydatid cyst and hepatic cysts, there was no significant difference. Therefore, CT staff can only identify the 2 diseases based on past experience; this objective determination brought great confusion and challenges to clinical work. In this study, among 50 patients with simple hepatic cyst, only 31 cases were successfully diagnosed by CT, and the rest 19 cases cannot be differentiated from the CE type 1. In the 50 cases of CE type 1, 40 cases were successfully diagnosed by CT, and the rest 10 cases cannot be differentiated from the hepatic cyst. Therefore, CT can only provide a reference for clarifying the size and position of cysts for the surgical approach, but cannot assist the future surgeries.
Serological testing are useful to confirm with imaging diagnosis and is an important tool in differential diagnosis.[17] The sensitivity of serological testing is dependent on the echinococcal antigen levels and its cross-reactivity with antigens of other diseases.[18,19] In this study, the dot immunogold filtration assay was used to detect antibody response to parasite. It showed among 50 patients with simple hepatic cyst, there were 14 cases positive and among 50 patients with CE type1, 43 cases were positive. The sensitivity and the specificity was 86.00% and 72.00% respectively, which was similar to Fu Yan large sample research (sensitivity of 92.61%).[20] For uncertain cases, for example in patients whose hepatic cysts cannot be differentiated from simple liver cyst using ultrasound or CT, combination with serological testing can get higher diagnostic value. In our study, it showed the specificity of combination of serological testing and ultrasound can reach 100%.
Currently, clinical diagnosis of hepatic hydatid cyst is mainly based on medical history, clinical symptoms, imaging and serological testing.[21] However, imaging examinations can be difficult to differentiate between CE cyst and hepatic cyst. Serological testing can help supplement imaging examinations to further diagnosis. Combination of imaging examinations and serological testing can provide a more reliable diagnosis.
This study has several limitations. First, this is a retrospective study from a single-institution experience. The number of patients enrolled may be not sufficient. Second, all the data were collected through the medical records and selection bias possibly exists. Therefore, randomized controlled researches with large sample size are expected in the future.
In conclusion, ultrasound is a considerably helpful technique for differentiating hydatid cyst from simple hepatic cyst. Serological test can be an important supplement to ultrasound.
Author contributions
Data curation: Tuerganaili Aji, Abuduaini Abulizi, Yusfu Yimiti, Hao Wen.
Formal analysis: Tuerganaili Aji, Tieming Jiang, Yusfu Yimiti.
Funding acquisition: Yingmei Shao.
Methodology: Bo Ran, Tieming Jiang, Ruiqing Zhang, Qiang Guo, Abuduaini Abulizi.
Resources: Ruiqing Zhang, Qiang Guo, Abuduaini Abulizi, Yusfu Yimiti.
Supervision: Yingmei Shao.
Validation: Yingmei Shao.
Visualization: Yingmei Shao.
Writing – original draft: Bo Ran, Ruiqing Zhang, Hao Wen.
Footnotes
Abbreviations: CE = cystic echinococcosis, CT = computed tomography, ROC = receiver operating characteristic curve.
This work was financially supported by National Science Foundation of China (No. 81560098) and Xinjiang Autonomous Regional Science Foundation of China (No. 2017D01C322).
The authors declared no conflict of interest.
References
- [1].Salamatin R, Kowal J, Nosal P, et al. Cystic echinococcosis in Poland: genetic variability and the first record of Echinococcus granulosus sensu stricto (G1 genotype) in the country. Parasitol Res 2017;116:3077–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Dziri C, Haouet K, Fingerhut A, et al. Management of cystic echinococcosis complications and dissemination: where is the evidence? World J Surg 2009;33:1266–73. [DOI] [PubMed] [Google Scholar]
- [3].Celebi S, Kutluk G, Bestas CB, et al. Current diagnosis and management of simple hepatic cysts detected prenatally and postnatally. Pediatr Surg Int 2014;30:599–604. [DOI] [PubMed] [Google Scholar]
- [4].Simon T, Bakker IS, Penninga L, et al. Haemorrhagic rupture of hepatic simple cysts. BMJ Case Rep 2015;2015: [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Giri S, Parija SC. A review on diagnostic and preventive aspects of cystic echinococcosis and human cysticercosis. Trop Parasitol 2012;2:99–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Sbihi Y, Rmiqui A, Rodriguez-Cabezas MN, et al. Comparative sensitivity of six serological tests and diagnostic value of ELISA using purified antigen in hydatidosis. J Clin Lab Anal 2001;15:14–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Zaman K, Mewara A, Kumar S, et al. Seroprevalence of human cystic echinococcosis from North India (2004-2015). Trop Parasitol 2017;7:103–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Doussot A, Gluskin J, Groot-Koerkamp B, et al. The accuracy of pre-operative imaging in the management of hepatic cysts. HPB (Oxford) 2015;17:889–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Mihmanli M, Idiz UO, Kaya C, et al. Current status of diagnosis and treatment of hepatic echinococcosis. World J Hepatol 2016;8:1169–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Pakala T, Molina M, Wu GY. Hepatic echinococcal cysts: a review. J Clin Transl Hepatol 2016;4:39–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Knapp J, Nakao M, Yanagida T, et al. Phylogenetic relationships within Echinococcus and Taenia tapeworms (Cestoda: Taeniidae): an inference from nuclear protein-coding genes. Mol Phylogenet Evol 2011;61:628–38. [DOI] [PubMed] [Google Scholar]
- [12].Patkowski W, Krasnodebski M, Grat M, et al. Surgical treatment of hepatic Echinococcus granulosus. Prz Gastroenterol 2017;12:199–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Gharbi HA, Hassine W, Brauner MW, et al. Ultrasound examination of the hydatic liver. Radiology 1981;139:459–63. [DOI] [PubMed] [Google Scholar]
- [14].Han S, Chen R, Fang W, et al. Investigation of the use of serology and ultrasonography to detect hepatic cystic echinococcosis in Heilongjiang, China, using a Bayesian framework. Acta Trop 2016;162:212–7. [DOI] [PubMed] [Google Scholar]
- [15].Yan C, Hamit M, Li L, et al. The comparison of algorithms on the CT image retrieval of Xinjiang local liver hydatid disease. J Biomed Eng (Shengwu yixue gongchengxue zazhi) 2013;30:942–5. [PubMed] [Google Scholar]
- [16].Stojkovic M, Rosenberger K, Kauczor HU, et al. Diagnosing and staging of cystic echinococcosis: how do CT and MRI perform in comparison to ultrasound? PLoS Negl Trop Dis 2012;6:e1880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Niscigorska J, Sluzar T, Marczewska M, et al. Parasitic cysts of the liver - practical approach to diagnosis and differentiation. Med Sci Monit 2001;7:737–41. [PubMed] [Google Scholar]
- [18].Wuestenberg J, Gruener B, Oeztuerk S, et al. Diagnostics in cystic echinococcosis: serology versus ultrasonography. Turk J Gastroenterol 2014;25:398–404. [DOI] [PubMed] [Google Scholar]
- [19].Pektas B, Altintas N, Akpolat N, et al. Evaluation of the diagnostic value of the ELISA tests developed by using EgHF, Em2 and EmII/3-10 antigens in the serological diagnosis of alveolar echinococcosis. Mikrobiyol Bul 2014;48:461–8. [DOI] [PubMed] [Google Scholar]
- [20].Fu Y, Feng XH, Wen H, et al. Preliminary observation on the clinical application of immunological diagnosis of echinococcosis. J Xinjiang MedUniv 2000;3:242–3. [Google Scholar]
- [21].Kern P, Menezes da Silva A, Akhan O, et al. The echinococcoses: diagnosis, clinical management and burden of disease. Adv Parasitol 2017;96:259–369. [DOI] [PubMed] [Google Scholar]