

Abstract
Objectives:
To describe beverages purchased in restaurants among a nationally representative sample of U.S. households.
Methods:
Data were obtained from the U.S. Department of Agriculture National Food Acquisition and Purchase Survey, 2012–2013. Survey-weighted multiple regressions assessed correlates of purchasing a sugar-sweetened beverage (SSB), low-calorie beverage, and per capita beverage calories and grams of sugar among purchases from U.S. restaurants (n=14,669).
Results:
Dining at a top fast food chain (OR =1.9 [95% CI=1.6, 2.3] vs. small chain or independent restaurants) and ordering a combination meal (2.8 [1.3, 3.3]) or from the kids’ menu (2.1 [1.2, 3.4]) were positively associated with purchasing a SSB. Age (young adult and adolescent vs. older adult; 0.7 [0.5, 0.9] and 0.4 [0.3, 0.7], respectively), race (White vs. Black; 0.4 [0.3, 0.6]), ethnicity (Non-Hispanic vs. Hispanic; 0.8 [0.6, 0.9]), and household food security (high vs. very low; 0.7 [0.5, 0.8]) were associated with purchasing a low-calorie beverage. Caloric beverage purchases contained the most calories and grams of sugar per capita when purchased by Hispanic and Non-Hispanic Black adolescents.
Conclusions:
U.S. households purchase a considerable amount of SSBs from the nation’s largest chain restaurants, particularly when combination meals or kids’ menu items are ordered, and there are disparities by age, race/ethnicity, and household food security.
Keywords: Sugar-sweetened beverage, public health, public policy
Introduction
Sugar-sweetened beverage (SSB) consumption is a stubborn public health problem that contributes to persistent socioeconomic and racial disparities in obesity and diet-related diseases.1–3 While consumption has declined over the last decade, it remains high, and there are persistent disparities by race, ethnicity, income, and education.4–6 On a typical day, half of all adults and two-thirds of children consume SSBs.4 Among children, SSB consumption is associated with increased risk of overweight and dental caries.7 High SSB consumption in adulthood has been linked to higher risk of developing diabetes, hypertension, and cardiovascular disease.8 SSBs contribute no nutritive value and may not be as satiating as solid food, contributing to overconsumption of calories.9 The prevalence and consequences of consumption make it an important policy target. It is considered by many to be a key “low hanging fruit” – one of the most obvious opportunities for addressing obesity and diet-related disease.
Increasingly, beverages are consumed in restaurants, where roughly 40% of U.S. food dollars are spent, and where SSBs are widely available and heavily promoted.10 Nearly one-quarter of adult calories and more than 10% of child and adolescent calories from SSBs are consumed in this setting.11,12 In 2017, beverages in the 90 top-earning chain restaurants in the U.S. contained an average of 281 kcals and 46 grams of total sugar/item, with 80% of beverages containing over 100 kcals/item (menustat.org). In recent years, chain restaurants have introduced new, lower calorie food items and dropped higher calorie foods from their menus, but availability of high calorie beverages has not significantly changed.13,14 Similarly, foods listed and advertised on fast food menu boards have become healthier and lower in calories over time, while the opposite patterns have been observed for beverages.15
Many public health policy efforts aiming to reduce SSB consumption are relevant to restaurant settings, where substituting a SSB with plain water or other unsweetened beverage may reduce total energy consumption.16 Menu labeling policies, which require chain restaurants to provide calorie information on menu boards alongside price, could influence both consumer selection and industry reformulation of beverages, although evidence to date has been mixed.13,14,17–20 Several U.S. cities have imposed beverage taxes, which raise the price of SSBs sold in restaurants and appear to be reducing purchases and consumption.21–23 Many jurisdictions have introduced bills that would require warning labels on the front of SSB packages or advertisements, although these efforts have been largely unsuccessful. Policies requiring healthier default beverage options -- offering water or milk instead of a SSB with combination meals in chain restaurants -- have become popular strategies for promoting healthy beverages with kids’ meals and could, in principle, be applied to combination meals promoted to adults on the regular menu board. Understanding the potential impact of these policies on health behaviors will require better monitoring of chain restaurant beverage purchases at the national level.
Research using the National Health and Nutrition Examination Surveys (NHANES) has examined national trends in restaurant beverage consumption,16, 24, 25 but few studies have assessed restaurant beverage purchases.26–28 While the NHANES is useful for describing prevalence of consumption and characteristics of consumers, it is less useful for targeting interventions aimed at reducing SSB consumption or for modeling the potential effects of proposed programs and policies. This is because the NHANES provides little information about the context in which SSBs are obtained. For example, over a dozen cities, counties, and states have implemented policies requiring chain restaurants to offer healthy beverages instead of SSBs as the default option with children’s meals. National data on the proportion of kids dining at chain restaurants, the proportion of kids purchasing children’s meals, and characteristics of beverages purchased on these occasions would be useful for estimating policy reach and impact, but these data are unavailable in the NHANES. The U.S Department of Agriculture’s (USDA) National Household Food Acquisition and Purchase Survey (FoodAPS) collects information on foods and beverages acquired by a nationally representative sample of households and is the first dataset to record detailed information about the context in which beverages are obtained, including information about the purchaser and specific details about the restaurant. In this study, we describe beverages purchased from U.S. restaurants, using data from FoodAPS. Findings will be useful for monitoring trends in restaurant purchases over time, for targeting SSB reduction strategies in restaurants, and for estimating potential effects of proposed public policies.
Methods
Data
We obtained data from the U.S. Department of Agriculture’s (USDA) National Household Food Acquisition and Purchase Survey (FoodAPS), which collected detailed information on foods and beverages acquired by a nationally representative sample of households over seven consecutive days (n=4,826) between April 2012 and January 2013. Households were sampled using a multistage sampling design, which oversampled households participating in the Supplemental Nutrition Assistance Program (SNAP) and low-income households.29 All adults and older children (11 years and older) in the household tracked foods purchased or acquired “at home” (e.g., supermarkets, convenience stores) and “away-from-home” (e.g., restaurants) using food records, scanned barcodes on foods, and receipts. The household primary respondent also reported on household resources and sociodemographic characteristics of individuals in the household in two in-person interviews. Additional details of food acquisitions were reported by the primary respondent in up to three telephone interviews.
Of the 4,826 sampled households, 4,739 recorded acquisitions and purchases (n=55,118 acquisitions and purchases) during the study period (Figure 1). For this study, we created a subpopulation that excluded food-at-home purchases (FAH; n=15,998) and food-away-from home (FAFH) purchases from sources other than restaurants (n=23,251). FAFH purchases from restaurants (n=15,869) accounted for 41% of all FAFH and 29% of total purchases and acquisitions. We excluded from our subpopulation observations in which acquisitions were recorded but lacked item information (n=226) and observations missing data on timing of the meal (n=622) or other covariates (n=352). The final analytic sample included 14,669 restaurant purchases. Of these, 8,335 included a caloric beverage.
Figure 1.
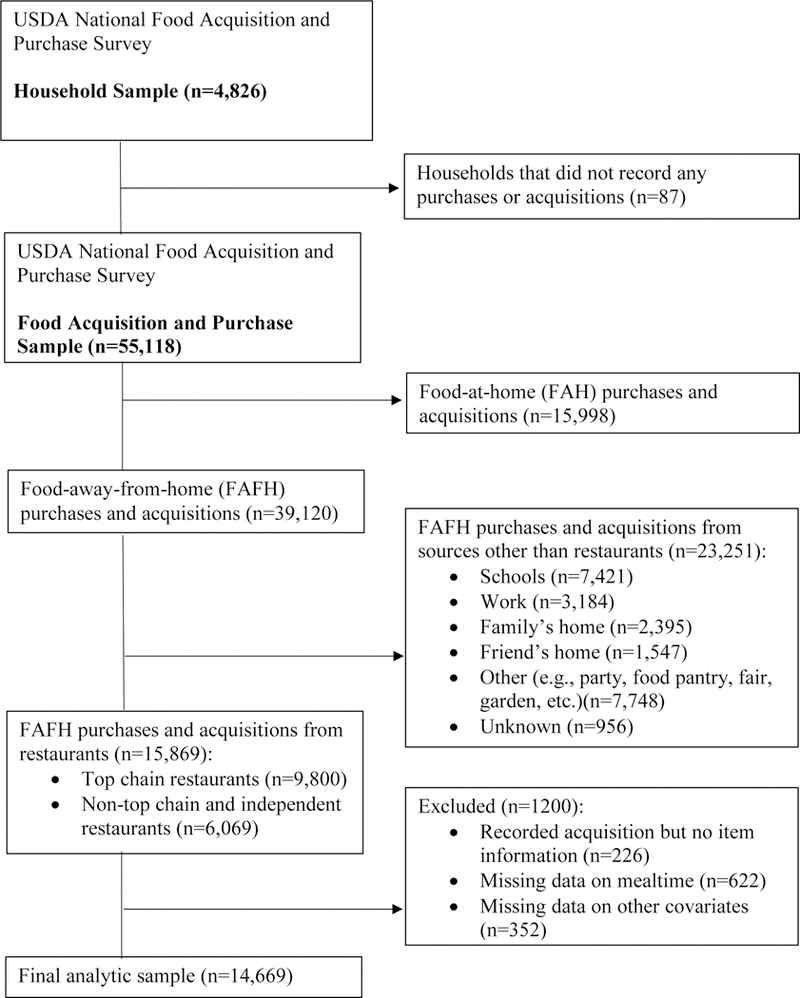
Sample Selection Flow Chart
Measures
The primary units of observation were restaurant purchases. Individual and household characteristics were obtained from interviews with the primary respondent and included the age (child <12 years, adolescent 12–19 years, young adult 20–39 years, or older adult 40+ years), sex (male or female), race (White, Black, or other race), ethnicity (Hispanic or non-Hispanic), and BMI (not overweight, overweight, obese) of the person acquiring the purchase; number and age group of people sharing the purchase; and household participation in SNAP (yes/no) or the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) (yes/no), food security status assessed using the 18-item U.S. Household Food Security Survey Module (food secure, marginal, low, or very low food security), and poverty status (<100% federal poverty level – FPL, 100%−184% FPL, ≥185% FPL) of the household, and educational attainment (<high school, high school graduate, > high school) of the household primary respondent. A purchase was defined as “shared” if more than one person consumed the purchase. FoodAPS provides the number of people who shared the purchase and the ID of each person in the household who shared but does not describe how much was consumed or which items within the purchase were consumed by each person. Thus, a single purchase may be shared by multiple people of different ages in the household. Current participation in SNAP or WIC were ascertained primarily through administrative matching (SNAP) or self-report (WIC). Racial and ethnic groups were selected based on high consumption of SSBs among Black and Hispanic compared to White adults.4
Information about each purchase included the timing of the meal (breakfast, lunch, dinner, snack, multiple meals); the number of items included in the purchase; and whether items were purchased from the kids’ menu (defined as the item unit or relative size containing the word “kids”), as part of a combination meal, or from a buffet. Beverages were coded by researchers as “sugar-sweetened beverages” (soft drinks, sport/energy drinks, fruit drinks, sweetened tea, sweetened flavored water) or “low-calorie beverages” (unsweetened coffee or tea, diet beverages, water, or seltzer) based on USDA food codes and prior analyses using the NHANES.4,5 Nutrients (calories, sugar) and weight (g) were matched to beverage descriptions and sizes from the Food and Nutrient Database for Dietary Studies in FoodAPS. For each purchase, researchers calculated per capita beverage grams, calories, and sugar by dividing total beverage weight and nutrients by the number of people who shared the meal.
FoodAPS respondents recorded the name and location of all FAFH purchases and acquisitions. To protect participant privacy, purchase locations were grouped into broader categories (e.g., school, work, restaurant) by the FoodAPS team. Specific restaurant names were available for acquisitions from the 78 “top” chain restaurants. This list of 78 restaurants was compiled based on the following characteristics: (1) restaurant is included in Menustat, a database with nutrient information for the top restaurants by U.S. sales based on a list from Nation’s Restaurant News in 2012 (n=66) or (2) restaurant is not included in Menustat but included on a list of the top 30 fast food and casual dining restaurants ranked by Quick Service Restaurant and Restaurant Institutions in 2009 (n=12). For these top restaurants, we coded each as fast-food (e.g., McDonald’s), fast-casual (e.g., Panera Bread), or full-service (e.g., Chili’s), based on a coding scheme developed for prior studies.13,14 All other unnamed restaurants were grouped together as “small chain or independent restaurants.” All restaurants were coded by FoodAPS into a restaurant type (e.g., burger, Italian) based on classifications from InfoUSA, We made small changes to these classifications so that purchases from the same restaurant chain fell into the same category. For example, a McDonald’s located in an airport was recoded from “airport” to “burger.”
Statistical Analysis
Survey procedures were used in all analyses to account for the complex sampling design (clusters, strata, and household weights). Survey-weighted means and frequencies were calculated to describe characteristics of restaurant purchases overall and by age of the consumer. To estimate the odds of purchasing a SSB or low-calorie beverage, these variables (binary measures for whether SSBs and low-calorie beverages were purchased or not) were regressed on characteristics of the person acquiring the purchase (age group, sex, race, ethnicity, BMI), characteristics of the household (poverty status, food security status, participation in SNAP or WIC, educational attainment of the primary respondent), and characteristics of the purchase (timing of purchase, whether it was intended for multiple meals, restaurant type – top chain fast food, top chain fast casual, top chain full-service, other restaurant, combination meal, number of items purchased, whether the purchase was shared, kids’ menu, or buffet). After examining the odds of purchasing a SSB, we examined correlates of per capita beverage calories and sugar when a caloric beverage was purchased. We regressed per capita beverage calories and sugar on the independent variables listed above (except variables indicating whether a meal was shared and the number of items purchased), and predicted means were estimated holding covariates at their means or references groups. Stratified analyses by age of the consumer, household poverty, race and ethnicity were also conducted. Analyses were weighted to be representative of the U.S. population, and robust variance was estimated using Taylor linearization, which accounts for correlation of residuals between purchases within the same individual and household. Significance was assessed at p<0.05. Analyses were conducted in Stata Version 14 (College Station, TX) in 2018.
Results
More than half of restaurant purchases came from top chain restaurants (58%), with 45% from top fast food chains (Table 1). Most adult purchases were consumed alone, while the majority of child (94%) and adolescent (69%) purchases were shared with others. Overall, most purchases were acquired by an adult (93%), except among adolescents, who acquired about half of purchases they consumed. The most popular cuisines were burger restaurants (29% of purchases), followed by American restaurants among children and adolescents and coffee/bakery among adults. On average, purchases contained 93 kcals, and 20 grams of sugar from beverages per capita. Nearly two-thirds (64%) of purchases contained a beverage. On average, one-third (34%) of purchases contained a SSB, which were more prevalent in purchases consumed by younger vs. older consumers (48% of child and adolescent purchases, 38% of young adult purchases, and 30% of older adult purchases).
Table 1.
Characteristics of restaurant purchases in 2012–2013, overall and by age of consumer. Values are representative of the national population (n=14,669).
| Variable | Age of consumer | ||||
|---|---|---|---|---|---|
| Overall | Children <12 years | Adolescents 12–19 years | Adults 20–39 years | Adults 40+ years | |
| % (SE) | % (SE) | % (SE) | % (SE) | % (SE) | |
| Age of person in household who acquired purchase | |||||
| Child (<12 years) | 0.6 (0.1) | 5.8 (0.9) | 0.2 (0.1) | 0.1 (0.1) | 0.1 (0.05) |
| Adolescent (12–19 years) | 5.9 (0.6) | 5.0 (4.0) | 50.1 (2.7) | 0.3 (0.1) | 0.1 (0.04) |
| Adult (20–39 years) | 36.3 (1.6) | 58.4 (3.4) | 16.5 (2.7) | 91.8 (0.8) | 3.0 (0.3) |
| Adult (40+ years) | 57.1 (1.3) | 30.7 (2.8) | 33.2 (3.4) | 7.8 (0.8) | 96.8 (0.3) |
| How the purchase was consumed | |||||
| Intended for multiple meals | 0.6 (0.1) | 0.7 (0.3) | 1.0 (0.3) | 0.6 (0.2) | 0.6 (0.1) |
| Consumed solely by one person | 54.5 (0.9) | 5.8 (0.7) | 31.0 (2.4) | 52.2 (1.7) | 51.4 (1.2) |
| Shared with other people | 45.4 (0.9) | 94.2 (0.7) | 69.0 (2.4) | 47.8 (1.7) | 48.6 (1.2) |
| Number of people who shared, mean (SE) | 1.7 (0.02) | 3.2 (0.1) | 2.3 (0.1) | 1.8 (0.04) | 1.7 (0.02) |
| Timing of purchase | |||||
| Breakfast | 14.6 (1.0) | 10.2 (1.2) | 7.9 (1.2) | 12.8 (1.1) | 16.6 (1.0) |
| Lunch | 38.3 (0.8) | 31.5 (2.0) | 34.7 (3.0) | 38.1 (1.0) | 37.3 (1.2) |
| Dinner | 33.4 (0.6) | 47.6 (1.6) | 46.1 (2.3) | 36.3 (1.1) | 32.1 (0.9) |
| Snack | 14.4 (0.5) | 11.5 (1.3) | 12.5 (1.4) | 13.4 (1.0) | 14.6 (0.8) |
| Purchase location | |||||
| Non-top chain or independent restaurant | 42.5 (2.1) | 36.2 (3.8) | 33.5 (3.3) | 40.8 (2.6) | 45.1 (2.2) |
| Top fast food chain restaurant | 44.7 (2.0) | 52.3 (3.1) | 55.8 (2.6) | 45.6 (2.3) | 41.8 (2.1) |
| Top fast casual chain restaurant | 6.1 (0.5) | 3.7 (0.9) | 3.5 (0.8) | 7.1 (0.7) | 5.6 (0.6) |
| Top full-service chain restaurant | 6.8 (0.5) | 7.8 (1.0) | 7.2 (1.2) | 6.5 (0.5) | 7.4 (0.6) |
| Restaurant type | |||||
| Sandwich | 7.8 (0.4) | 4.3 (0.7) | 8.0 (0.7) | 8.1 (0.4) | 7.3 (0.7) |
| Steak House | 1.3 (0.2) | 2.3 (1.3) | 1.8 (1.1) | 1.1 (0.3) | 1.2 (0.2) |
| Seafood | 1.6 (0.3) | 0.9 (0.4) | 1.6 (0.5) | 1.7 (0.6) | 1.6 (0.2) |
| Mexican | 8.4 (0.4) | 7.8 (1.1) | 8.3 (1.0) | 10.6 (0.8) | 7.4 (0.5) |
| Asian | 4.2 (0.4) | 3.5 (0.7) | 4.5 (0.8) | 5.5 (0.5) | 4.0 (0.6) |
| American | 12.4 (1.0) | 11.0 (2.7) | 10.4 (2.4) | 10.1 (0.6) | 14.0 (1.3) |
| European | 2.2 (0.3) | 1.4 (0.3) | 1.5 (0.5) | 2.0 (0.4) | 2.6 (0.4) |
| Pizza | 6.6 (0.4) | 12.5 (1.4) | 10.3 (1.4) | 7.9 (0.6) | 5.9 (0.5) |
| Chicken | 5.1 (0.5) | 6.0 (0.8) | 6.6 (1.0) | 5.6 (0.6) | 4.7 (0.6) |
| Burger | 28.6 (1.2) | 34.8 (2.2) | 34.8 (2.1) | 27.0 (1.4) | 27.9 (1.3) |
| Buffet | 0.9 (0.2) | 1.0 (0.3) | 1.2 (0.4) | 0.6 (0.1) | 1.2 (0.3) |
| Coffee/Bakery | 13.8 (1.1) | 8.8 (0.9) | 5.6 (0.9) | 14.0 (0.1) | 14.2 (1.3) |
| Othera | 7.1 (0.6) | 5.6 (0.9) | 5.3 (1.3) | 5.8 (0.6) | 8.0 (0.9) |
| Menu type | |||||
| Combination meal | 16.7 (0.9) | 25.6 (1.7) | 22.8 (1.5) | 17.3 (1.2) | 15.7 (1.1) |
| Kids’ menu | 1.6 (0.3) | 5.9 (1.0) | 1.2 (0.3) | 1.8 (0.3) | 1.6 (0.4) |
| Purchase includes a beverage | 64.4 (1.2) | 65.6 (2.3) | 62.8 (2.8) | 62.8 (0.8) | 65.2 (1.6) |
| Beverage typeb | |||||
| Sugar-sweetened beverage | 33.7 (1.1) | 48.0 (2.3) | 48.0 (3.1) | 38.3 (1.4) | 29.6 (1.6) |
| Soft drink | 21.5 (1.0) | 37.1 (2.4) | 35.1 (3.9) | 25.1 (1.4) | 18.1 (1.0) |
| Fruit drink | 4.8 (0.3) | 7.9 (1.1) | 8.1 (0.8) | 5.8 (0.5) | 3.9 (0.5) |
| Sport / energy drink | 0.4 (0.1) | 0.6 (0.2) | 0.9 (0.4) | 0.6 (0.2) | 0.3 (0.1) |
| Sweetened tea | 9.6 (0.7) | 11.2 (1.7) | 11.3 (1.6) | 9.7 (0.7) | 9.8 (1.0) |
| Flavored milk | 0.5 (0.1) | 3.4 (0.7) | 0.5 (0.2) | 0.9 (0.2) | 0.3 (0.1) |
| Milkshake | 2.2 (0.2) | 3.6 (0.7) | 4.3 (0.7) | 1.8 (0.2) | 2.2 (0.3) |
| Sweetened coffee or coffee drink | 2.0 (0.2) | 1.3 (0.4) | 1.5 (0.4) | 2.9 (0.5) | 1.4 (0.2) |
| Unsweetened coffee and tea | 16.1 (1.1) | 6.4 (0.8) | 5.0 (1.1) | 11.0 (0.9) | 20.9 (1.7) |
| Water or seltzer | 9.6 (0.6) | 7.9 (0.8) | 8.1 (1.3) | 9.6 (1.0) | 10.0 (0.9) |
| Plain milk | 0.8 (0.1) | 2.8 (0.7) | 0.8 (0.4) | 0.5 (0.1) | 0.9 (0.2) |
| 100% juice | 2.0 (0.2) | 6.1 (1.1) | 2.1 (0.4) | 2.2 (0.2) | 1.9 (0.3) |
| Beverage amount per capita, mean (SE) | |||||
| Weight (g) | 370.3 (9.4) | 267.8 (12.9) | 359.1 (18.1) | 378.0 (10.7) | 356.2 (11.7) |
| Calories (kcals) | 92.5 (3.7) | 86.5 (4.9) | 115.1 (6.9) | 107.9 (5.0) | 76.1 (4.6) |
| Sugar (g) | 20.1 (0.8) | 19.3 (1.2) | 26.1 (1.6) | 23.2 (1.1) | 16.7 (1.0) |
Note: Standard errors account for sampling design.
Includes specialty top restaurants (e.g., Jamba Juice) and restaurants of unspecified type.
Percentages do not add to 100 because purchases could contain more than one beverage and more than one sugar-sweetened beverage.
In adjusted models, the strongest correlates of purchasing a SSB or a low-calorie beverage were the age, race and ethnicity of the individual acquiring the purchase, household food security status, and the characteristics of the restaurant (Table 2). Compared to older adults, young adults and adolescents were more likely to purchase SSBs (OR=1.5 [95% CI=1.2, 1.8] and 2.6 [1.6, 4.4], respectively), and the odds of purchasing a low-calorie beverage decreased with age (0.1 [0.0, 0.3] comparing children to older adults). Purchases were half as likely to include a lowcalorie beverage (0.4 [0.3, 0.6]) when acquired by a Black person compared to a White person, and 20% less likely to include a low-calorie beverage when acquired by a Hispanic vs. NonHispanic person (0.8 [0.6, 0.9]. Compared to food secure households, the odds of purchasing a SSB were higher in households with marginal and low food security (1.3 [1.0, 1.6] and 1.5 [1.1, 2.1], respectively) and the odds of purchasing a low-calorie beverage were lower in households with very low food security (0.7 [0.5, 0.8]). Purchases at top fast food chains were 1.9 times more likely to include a SSB (1.9 [1.6, 2.3]) and less likely to include a low-calorie beverage (0.6 [0.5, 0.8]) than purchases from small chain or independent restaurants. When purchases included a combination meal or kids’ menu items they were more than twice as likely to include a SSB (2.8 [1.3, 3.3] and 2.1 [1.2, 3.4], respectively).
Table 2.
Correlates of purchasing a sugar-sweetened beverage or noncaloric beverage at a restaurant, U.S. households 2012–2013 (n=14,669).
| Variable | Sugar-sweetened beveragea | Low-calorie beverageb |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| Characteristics of person acquiring the purchase | ||
| Age | ||
| Adult (40+ years) | ref | Ref |
| Adult (20–39 years) | 1.5 (1.2, 1.8)*** | 0.7 (0.5, 0.9)** |
| Adolescent (12–19 years) | 2.6 (1.6, 4.4)** | 0.4 (0.3, 0.7)** |
| Child (<12 years) | 1.8 (0.7, 4.9) | 0.1 (0.0, 0.3)*** |
| Sex | ||
| Male | ref | Ref |
| Female | 0.9 (0.7, 1.0) | 1.1 (0.9, 1.4) |
| Race | ||
| White | ref | ref |
| Black | 1.1 (0.9, 1.3) | 0.4 (0.3, 0.6)*** |
| Other race | 0.8 (0.7, 0.9)** | 0.9 (0.7, 1.1) |
| Hispanic | ||
| No | ref | ref |
| Yes | 1.1 (0.9, 1.3) | 0.8 (0.6, 0.9)** |
| BMI category | ||
| Not overweight | ref | ref |
| Overweight | 1.0 (0.8, 1.2) | 1.2 (1.0, 1.5) |
| Obese | 1.1 (0.9, 1.4) | 1.1 (0.9, 1.4) |
| Characteristics of the household | ||
| Educational attainment | ||
| <High School | ref | ref |
| High School Grad | 1.0 (0.7, 1.3) | 1.2 (0.8, 1.7) |
| >High School | 0.8 (0.7, 1.1) | 1.0 (0.7, 1.5) |
| Poverty status | ||
| 185%+ FPL | ref | ref |
| 100%−184% FPL | 1.1 (0.9, 1.4) | 0.9 (0.6, 1.2) |
| <100% FPL | 1.0 (0.7, 1.3) | 0.9 (0.7, 1.2) |
| Food security status | ||
| Food secure | ref | ref |
| Marginal food security | 1.3 (1.0, 1.6)* | 0.7 (0.5, 1.0) |
| Low food security | 1.5 (1.1, 2.1)* | 0.8 (0.5, 1.3) |
| Very low food security | 1.2 (0.9, 1.5) | 0.7 (0.5, 0.8)** |
| Food assistance participation | ||
| SNAP | ||
| No | ref | ref |
| Yes | 1.0 (0.8, 1.2) | 0.7 (0.6, 0.8)** |
| WIC participant | ||
| No | ref | ref |
| Yes | 1.3 (0.9, 1.8) | 0.8 (0.6, 1.1) |
| Characteristics of the purchase | ||
| Restaurant type | ||
| Small chain or independent restaurant | ref | ref |
| Top fast food chain | 1.9 (1.6, 2.3)*** | 0.6 (0.5, 0.8)*** |
| Top fast casual chain | 1.0 (0.8, 1.4) | 1.5 (1.1, 2.1)* |
| Top full-service chain | 1.1 (0.8, 1.4) | 1.2 (0.9, 1.7) |
| Combination meal | ||
| No | ref | ref |
| Yes | 2.8 (1.3, 3.3)*** | 1.0 (0.8, 1.2) |
| Kids’ menu | ||
| No | ref | ref |
| Yes | 2.1 (1.2, 3.4)** | 0.8 (0.5, 1.3) |
Note: Logistic regression additionally controlled for the number of items purchased, whether the purchase was shared with other people, the timing of the purchase (breakfast, lunch dinner, or snack) whether the beverage came from a buffet, and whether or not the purchase was intended for multiple meals. Standard errors account for the sampling design.
“Sugar-sweetened beverages” include fruit drinks, sports and energy drinks, Vitamin water, and sweetened tea.
“Low-calorie beverages” include water, seltzer, diet beverages, and unsweetened coffee or tea. Boldface indicates statistically significant difference from reference group.
p<0.05
p<0.01
p<0.001
Caloric beverages purchased by adolescents and young adults contained significantly more calories (214 and 188 vs. 137, respectively) and grams of sugar (47 and 40 vs. 30, respectively) than those purchased by older adults (Table 3). Caloric beverages purchased by Black people contained significantly more calories (195 vs. 158) and grams of sugar (45 vs. 34) than those purchased by White people, and purchases by Hispanic people contained more calories (176 vs. 158) and grams of sugar (38 vs. 34) than those by Non-Hispanic people. Compared to food secure households, households with marginal and very low food security purchased more beverage calories (172 and 179 vs. 154, respectively). Purchases were highest in beverage calories when purchased from a top fast food or fast casual chain compared to a small chain or independent restaurant (191 and 173 vs. 121, respectively), and were lower in calories when items were ordered from the kids’ menu (129 vs. 161).
Table 3.
Predicted mean per capita beverage calories and sugar and 95% confidence intervals (CI) from purchases containing a caloric beverage, U.S. households 2012–2013 (n=8,335)
| Variable | Calories (kcals) per capita per purchase | Sugar (g) per capita per purchase |
|---|---|---|
| Predicted mean (95% CI) | Predicted mean (95% CI) | |
| Characteristics of person acquiring the purchase | ||
| Age | ||
| Adult (40+ years) (ref) | 137 (125, 150) | 30 (28, 33) |
| Adult (20–39 years) | 188 (175, 201)*** | 40 (38, 43)*** |
| Adolescent (12–19 years) | 214 (205, 224)*** | 47 (38, 43)*** |
| Child (<12 years) | 172 (134, 210) | 36 (26, 46) |
| Sex | ||
| Male (ref) | 161 (150, 172) | 36 (33, 38) |
| Female | 159 (148, 171) | 34 (32, 37) |
| Race | ||
| White (ref) | 158 (149, 168) | 34 (32, 36) |
| Black | 195 (176, 214)*** | 45 (41, 49)*** |
| Other race | 142 (126, 159)* | 32 (28, 36) |
| Hispanic | ||
| No (ref) | 158 (149, 167) | 34 (32, 36) |
| Yes | 176 (158, 194)* | 38 (35, 41)* |
| BMI category | ||
| Not overweight (ref) | 164 (150, 178) | 36 (33, 39) |
| Overweight | 156 (140, 172) | 34 (30, 38) |
| Obese | 160 (145, 176) | 34 (31, 37) |
| Characteristics of the household | ||
| Educational attainment | ||
| <High School (ref) | 157 (131, 183) | 35 (29, 41) |
| High School Grad | 160 (147, 174) | 35 (32, 38) |
| >High School | 160 (150, 171) | 35 (32, 37) |
| Poverty status | ||
| 185%+ FPL (ref) | 159 (148, 170) | 34 (32, 37) |
| 100%−184% FPL | 164 (149, 179) | 37 (33, 41) |
| <100% FPL | 165 (147, 183) | 37 (32, 41) |
| Food security status | ||
| Food secure (ref) | 154 (142, 166) | 34 (31, 36) |
| Marginal food security | 172 (159, 185)* | 37 (34, 40) |
| Low food security | 188 (154, 222) | 38 (35, 41) |
| Very low food security | 179 (160, 198)* | 40 (35, 44)* |
| Food assistance participation | ||
| SNAP | ||
| No (ref) | 160 (150, 169) | 35 (33, 37) |
| Yes | 168 (151, 184) | 37 (34, 41) |
| WIC participant | ||
| No (ref) | 160 (151, 169) | 35 (33, 37) |
| Yes | 161 (138, 184) | 36 (31, 42) |
| Characteristics of the purchase | ||
| Restaurant type | ||
| Non-top chain (ref) | 121 (108, 134) | 26 (23, 29) |
| Top fast food chain | 191 (177, 205)*** | 43 (39, 46)*** |
| Top fast casual chain | 173 (134, 211)* | 32 (26, 37) |
| Top full-service chain | 143 (117, 169) | 32 (27, 38)* |
| Combination meal | ||
| No (ref) | 158 (148, 168) | 34 (32, 37) |
| Yes | 166 (149, 182) | 36 (33, 39) |
| Kids’ menu | ||
| No (ref) | 161 (152, 170) | 35 (33, 37) |
| Yes | 129 (96, 161)* | 28 (20, 36) |
Note: Limited to purchases including a caloric beverage. Regressions additionally controlled for the number of items purchased, whether the purchase was shared with other people, the timing of the purchase (breakfast, lunch dinner, or snack) whether the beverage came from a buffet, and whether or not the purchase was intended for multiple meals. Standard errors account for the sampling design. Boldface indicates statistically significant difference from reference group.
p<0.05
p<0.001
In subgroup analyses, there were no meaningful differences in the effect of the restaurant (e.g., restaurant type) on beverage choice across income, age of consumer, race or ethnicity, but there were marked differences across race and ethnicity by age (Figure 2). The highest amount of beverage calories (261 kcals) per capita were purchased by Non-Hispanic Black adolescents, who purchased significantly more than Non-Hispanic Black children (132 kcals) and NonHispanic White adolescents (206 kcals).
Figure 2.
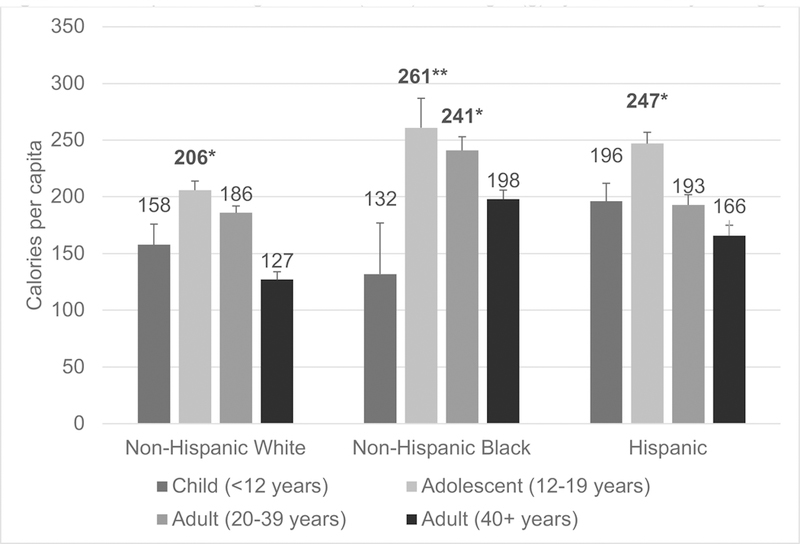
Per capita beverage calories (kcals) and sugar (g) by race/ethnicity and age
Figure shows mean (SE) per capita beverage calories (kcals) from restaurant purchases containing a caloric beverage, U.S. households, 2012–2013 (n=8,333). Data are from linear regressions controlling for the BMI of the person acquiring the purchase, household educational attainment, food security status, poverty status, federal food assistance participation (SNAP and WIC), restaurant type, whether a combination meal or kids’ meal was ordered, whether the beverage came from a buffet, the timing of the purchase, whether the purchase was shared, the number of items purchased, and whether the purchase was intended for multiple meals. Standard errors account for sampling design, so values are representative of the national population. Boldface indicates statistically significant difference from the reference group (children). *p<0.05, **p<0.01
Discussion
Households included in this study purchased large amounts of calories and sugar from beverages in U.S. restaurants, with marked differences by race, ethnicity, household food security and restaurant type. More than one-third of purchases consumed by adults and half of those consumed by children included a SSB. Restaurant purchases contained an average of 93 calories and 20 grams of sugar from beverages per capita -- approximately the amount of calories and sugar in an 8-ounce can of soda. Consistent with the most recent literature on SSB consumption, Black and Hispanic individuals purchased more beverage calories and grams of sugar per capita than White individuals, with the highest amounts of calories and sugar purchased by NonHispanic Black adolescents and young adults.4 Very food insecure households purchased more beverage calories and grams of sugar than food secure households -- findings that align with prior studies showing a correlation between food security and diet quality.30 These disparities are particularly notable given the disproportionately higher risk of obesity and chronic disease among food insecure, Black, and Hispanic adults.31–34
Another important finding was the strong correlation between aspects of the restaurant and SSB purchases. Purchases from top chain fast food restaurants (compared to smaller chain or independent restaurants) were nearly twice as likely to include a SSB and half as likely to include a low-calorie beverage. Further, per capita beverage calories and sugar were highest among purchases from top chain fast food restaurants compared to other restaurant types. Promotions within the restaurant also influenced beverage choice. Specifically, purchasing a combination meal increased the odds of selecting a SSB by 2.8 times, and purchasing items from the kids’ menu doubled the odds of selecting a SSB. These results are similar to those from a study of adults dining at fast-food restaurants in New York and New Jersey, which found that ordering a combination meal was associated with both a higher risk of ordering a SSB and with purchasing more beverage calories per order.27
There are some notable limitations to this study. First, in shared meals, beverages could not be linked to the individual who consumed them. For purchases intended for one person only, it is unknown whether the entire beverage or only a portion was consumed. Second, although product barcodes were scanned for food-at-home purchases, reporting of chain restaurant purchases largely relied on self-report, which is subject to recall bias. Third, although this study is based on the most recently released FoodAPS data, these data were collected in 2012–2013, which could make findings outdated if consumer dining patterns have undergone a significant shift over the past five years. Lastly, this is a cross-sectional study, so we cannot determine the direction of associations, i.e., whether attributes of top chain fast food restaurants influence consumer beverage choices, or whether people go to top chain fast food restaurants because they intend to purchase a SSB. Strengths of this study include a nationally representative weighted sample of households and detailed information about the restaurant and purchase. To our knowledge, this is the first study to describe household restaurant purchases on a national scale.
Public Health Implications
Results from this study can help target policy changes and voluntary programs aimed at reducing disparities in SSB consumption in the restaurant setting. For example, this study found higher purchases of beverage calories and sugar among food insecure households. There is growing momentum around beverage taxes, which may increase the price of SSB calories in restaurants and reduce SSB purchases, particularly among low-income adults (while income is not perfectly correlated with food insecurity, the two are closely related). Evidence from Mexico (1 peso/liter tax) found a 7.6% decline in SSB purchases after two years with larger reductions among the lowest income households,35 and evidence from Berkeley, CA (one-cent-per ounce tax) found a 21% reduction in SSB consumption in low-income neighborhoods 4 months after implementation.22 Second, in this study, SSBs were more likely to be purchased with combination meals, likely because SSBs are offered with these meals as the default option, are heavily advertised on menu boards, and are value priced to encourage larger portions. These findings suggest that policies requiring restaurants to offer only healthy beverages as the default option in combination meals instead of SSBs may encourage no calorie or low-calorie choices. This hypothesis is supported by behavioral research, which shows that consumers strongly favor the status quo and will tend to select the default or automatic option.36,37 Third, results showed substantially higher purchases of beverage calories and sugar among non-Hispanic Black adolescents; restaurants could voluntarily adopt public health messaging campaigns tailored towards this population. For example, one study providing caloric information in terms of physical activity equivalents was more effective than absolute calories at reducing purchases of SSBs among low-income Black adolescents.38
Future research is needed to understand the causal relationship between the restaurant environment and beverage choice, and recent changes to local policy offer opportunities for natural experiments to study the influence of price changes and healthy defaults on restaurant beverage selection. For example, beverage taxes apply to beverages served in chain restaurants, but real-world studies of the effect of these taxes on restaurant pricing and consumer selection are lacking. As a second example, more than ten cities and counties have adopted healthy default beverage ordinances, but it is unclear how such ordinances influence child drink selection and consumption. In the meantime, findings from this study can help to estimate the potential public health impact of popular policy options, and highlights aspects of the restaurant environment, such as combination meals and kids’ menus, that are ripe for policy action.
Conclusions
Adults purchase a considerable amount of SSB from the nation’s largest chain restaurants. This is particularly true in top chain fast food restaurants, when combination meals are ordered, when items are ordered from the kids’ menu, and for individuals who are racial/ethnic minorities or food insecure. Understanding how recent policy and programmatic efforts to reduce SSB consumption may influence purchases in the restaurant setting are a key area of future inquiry.
Study Importance Questions.
What is already known about this subject?
On a typical day, half of adults and two-thirds of children consume sugar-sweetened beverages, which are linked to higher risk of developing diabetes, hypertension, and cardiovascular disease.
Increasingly, sugar-sweetened beverages are consumed in restaurants -- the target of several recent public health efforts, including beverage taxes, menu labeling, and healthy beverage ordinances.
Understanding the impact of these policies will require better monitoring of restaurant sugar-sweetened beverage purchases on a national scale, but prior studies have been limited to a small number of chains or one geographic region.
What does your study add?
In a seven-day national survey of 14,669 restaurant purchases, age, race, ethnicity, household food insecurity, and characteristics of the restaurant were correlated with beverage choice.
Beverages from top National fast food chains contained more calories and grams of sugar per capita than purchases from non-top chain or independent restaurants.
Households ordering a combination meal or from the kids’ menu were more than twice as likely to include a sugar-sweetened beverage, but no more likely to include a lowcalorie beverage than purchases without combinations or kids’ items.
Acknowledgments
Funding: This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Ms. Moran was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under award number T32DK007703.
Footnotes
Disclosure: The authors declared no conflict of interest.
References
- 1.Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review. Am J Clin Nutr;84(2):274–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Malik VS, Pan A, Willett WC, Hu FB. Sugar-sweetened beverages and weight gain in children and adults: a systematic review and meta-analysis. Am J Clin Nutr 2013. October;98(4):1084–102. doi: 10.3945/ajcn.113.058362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Resolved: there is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes Rev 2014;14(8):606–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bleich SN, Vercammen KA, Koma JW, Li Z. Trends in beverage consumption among children and adults, 2003–2014. Obesity (Silver Spring) 2018. February;26(2):432–441. [DOI] [PubMed] [Google Scholar]
- 5.Han E, Powell LM. Consumption patterns of sugar-sweetened beverages in the United States. J Acad Nutr Diet 2013;113(1):43–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rehm CD, Penalvo JL, Afshin A, Mozaffarian D. Dietary intake among US adults, 1999–2012. JAMA 2016. June 21;315(23):2542–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bleich SN, Vercammen KA. The negative impact of sugar-sweetened beverages on children’s health: an update of the literature. BMC Obes 2018. February 20;5:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Schwingshackl L, Hoffman G, Lampousi AM, et al. Food groups and risk of type 2 diabetes mellitus: a systematic review and meta-analysis of prospective studies. Eur J Epidemiol 2017. May;32(5):363–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cassady BA, Considine RV, Mattes RD. Beverage consumption, appetite, and energy intake: what did you expect? Am J Clin Nutr 2012. March;95(3):587–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.U.S. Department of Agriculture. Food Expenditures. Last updated January 26, 2016 Available at https://www.ers.usda.gov/data-products/food-expenditures/foodexpenditures/#Food%20Expenditures. Accessed April 16, 2018.
- 11.An R, Maurer G. Consumption of sugar-sweetened beverages and discretionary foods among US adults by purchase location. Eur J Clin Nutr 2016. December;70(12):1396–1400. [DOI] [PubMed] [Google Scholar]
- 12.Poti JM, Slining MM, Popkin BM. Where are kids getting their empty calories? Stores, schools, and fast food restaurants each play an important role in empty calorie intake among US children in 2009–2010. J Acd Nutr Diet 2014;115(6):908–917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bleich SN, Wolfson JA, Jarlenski MP. Calorie changes in large chain restaurants: declines in new menu items but room for improvement. Am J Prev Med 2016. January;50(1):e1–e8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bleich SN, Moran AJ, Jarlenski MP, Wolfson JA. Higher-calorie menu items eliminated in large chain restaurants. Am J Prev Med 2018;54(2):214–220. [DOI] [PubMed] [Google Scholar]
- 15.Soo J, Harris JL, Davison KK, Williams DR, Roberto CA. Changes in the nutritional quality of fast-food items marketed at restaurants, 2010 v. 2013. Public Health Nutr 2018. March 27:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.An R Plain water and sugar-sweetened beverage consumption in relation to energy and nutrient intake at full-service restaurants. Nutrients 2016;8(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Long MW, Tobias DK, Cradock AL, Batchelder H, Gortmaker SL. Systematic review and meta-analysis of the impact of restaurant menu calorie labeling. Am J Public Health 2015;105(5):e11–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.VanEpps EM, Roberto CA, Park S, Economos CD, Bleich SN. Restaurant menu labeling policy: review of evidence and controversies. Curr Obes Rep 2016;5(1):72–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cantu-Jungles TM, McCormack LA, Slaven JE, Slebodnik M, Eicher-Miller HA. A meta-analysis to determine the impact of restaurant menu labeling on calories and nutrients (ordered or consumed) in U.S. adults. Nutrients 2017;9(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bleich SN, Economos CD, Spiker ML, et al. A systematic review of calorie labeling and modified calorie labeling interventions: impact on consumer and restaurant behavior. Obesity (Silver Spring) 2017;25(12):2018–2044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Colchero MA, Molina M, Guerrero-Lopez CM. After Mexico implemented a tax purchases of sugar-sweetened beverages decreased and water increased: difference by place of residence, household composition, and income level. J Nutr 2017. August;147(8):1552–1557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Falbe J, Thompson HR, Becker CM, Rojas N, McCulloch CE, Madsen KA. Impact of the Berkeley excise tax on sugar-sweetened beverage consumption. Am J Public Health 2016;106(10):1865–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhong Y, Auchincloss AH, Lee BK, Kanter GP. The short-term impacts of the Philadelphia beverage tax on beverage consumption. Am J Prev Med (in press) [DOI] [PubMed]
- 24.Powell LM, Nguyen BT. Fast-food and full-service restaurant consumption among children and adolescents: effect on energy, beverage, and nutrient intake. JAMA Pediatr 2013. January;167(1):14–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nguyen BT, Powell LM. Supplemental nutrition assistance program participation and sugar-sweetened beverage consumption, overall and by source. Prev Med 2015. December;81:82–6. [DOI] [PubMed] [Google Scholar]
- 26.Cantor J, Breck A, Elbel. Correlates of sugar-sweetened beverages purchased for children at fast-food restaurants. Am J Public Health 2016. November;106(11):2038–2041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Taksler GB, Kiszko K, Abrams C, Elbel B. Adults who order sugar-sweetened beverages: sociodemographics and meal patterns at fast food chains. Am J Prev Med 2016. December;51(6):890–897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dumanovsky T, Nonas CA, Huang CY, Silver LD, Bassett MT. What people buy from fast-food restaurants: caloric content and menu item selection, New York City 2007. Obesity (Silver Spring) 2009;17(7):1369–74. [DOI] [PubMed] [Google Scholar]
- 29.Economic Research Service (ERS), U.S. Department of Agriculture (USDA). National Household Food Acquisition and Purchase Survey (Foodaps) http://www.ers.usda.gov/foodaps.
- 30.Laraia BA, Leak TM, Tester JM, Leung CM. Biobehavioral factors that shape nutrition in low-income populations: a narrative review. Am J Prev Med 2017. February;52(2S2):S118–S126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Laraia BA. Food insecurity and chronic disease. Adv Nutr 2013. March 1;4(2):203–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dhurandhar EJ. The food-insecurity obesity-paradox: a resource scarcity hypothesis. Physiol Behav 2016. August 1;162:88–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014;311:806–814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zhang Q, Wang Y, Huang ES. Changes in racial/ethnic disparities in the prevalence of Type 2 diabetes by obesity level among US adults. Ethn Health 2009;14:439–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Colchero MA, Rivera-Dommarco J, Popkin BM, Ng SW. In Mexico, evidence of sustained consumer response two years after implementing a sugar-sweetened beverage tax. Health Aff (Millwood) 2017. March 1;36(3):564–571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Roberto CA, Kawachi I. Use of psychology and behavioral economics to promote healthy eating. Am J Prev Med 2014. December;47(6):832–7. [DOI] [PubMed] [Google Scholar]
- 37.Anzman-Frasca S, Mueller MP, Lynskey VM, Harelick L, Economos CD. Orders of healthier children’s items remain high more than two years after menu changes at a regional restaurant chain. Health Aff(Millwood) 2015. Nov;34(11):1885–92. [DOI] [PubMed] [Google Scholar]
- 38.Bleich SN, Herring BJ, Flagg DD, Gary-Webb TL. Reduction in purchases of sugarsweetened beverage among low-income Black adolescents after exposure to caloric information. Am J Public Health 2012. February;102(2):329–35. [DOI] [PMC free article] [PubMed] [Google Scholar]