

Abstract
Candida infection of the gastrointestinal (GI) tract is rare in the immunocompetent individual. In immunocompromised patients, it frequently involves the oesophagus, but extra-oesophageal involvement is uncommon. We report a case of primary and isolated gastroduodenal candidiasis. Upper GI endoscopy with biopsy of gastric mucosa was crucial for making the diagnosis. The patient showed transient improvement after therapy with fluconazole.
LEARNING POINTS
Gastroduodenal candidiasis is rarely documented in the literature.
Old age is an independent risk factor for fungal infection of the gastrointestinal tract.
In this case, fungal gastroduodenitis was associated with gastroparesis.
Keywords: Gastroduodenitis, Fungal infection, Candida spp
INTRODUCTION
Fungal infection of the stomach may be seen in patients with underlying malignancy, who have undergone surgery for peptic ulcer or are immunosuppressed, but is infrequent in immunocompetent individuals[1]. Gastric involvement usually occurs as a secondary infiltration of benign or malignant ulceration, being rarely described as a primary infection of the mucosa[2]. We report a case of primary gastroduodenal candidiasis in an elderly patient without underlying disease or receiving immunosuppressive treatment.
CASE DESCRIPTION
A 91-year-old woman presented to the emergency room (ER) with vomiting and fever. She had a history of dementia and dyslipidaemia. Her usual medication included an anti-dementia drug, an anti-depressive and a statin. There was no history of recent surgery or other medication usage including antibiotics and immunosuppressive drugs.
On physical examination in the ER, the patient had hypotension, tachycardia and prostration with signs of poor peripheral perfusion. Initial laboratory investigations showed elevation of the white cell count with a raised neutrophilic count, renal dysfunction (urea 110 and serum creatinine 2.69 mg/dl), hypernatremia and elevation of transaminases.
Computed tomography (CT) of the abdomen showed marked dilation of the gastric cavity and duodenum which were filled with liquid and gas (Fig. 1), with a transition to normal calibre in the third portion of the duodenum. A nasogastric tube was placed and revealed faecaloid content. The patient was evaluated by general surgery personnel, who suggested that CT alterations could be secondary to a proliferative lesion, but that surgery was not indicated due to the patient’s overall condition. The patient was administered fluid therapy and prokinetic agents (metoclopramide and erythromycin) and was nil by mouth, as palliative measures. A high quantity of drainage (about 1,000–2,000 ml per day) through the nasogastric tube was maintained. Four days after hospital admission, the patient was clinically stabilized in order to perform an upper GI endoscopy, which revealed greyish-looking gastric and duodenal mucosa (Fig. 2), without alterations of the oesophagus. Gastric peristalsis was not observed during endoscopy and the greyish-looking mucosa remained the same after gastric wash. Because of the greyish-looking mucosa and the age of the patient, ischaemic gastroduodenitis was suggested. This hypothesis was later excluded after CT angiography of the abdomen was performed, which indicated permeability of the vascular axes of the gastrointestinal tract. However, histological examination showed numerous fungi and non-branched and septate hyphae (Figs. 3 and 4), which were microscopically compatible with Candida spp. (although microbiological examination was not performed to confirm this). Blood cultures were negative. The patient started parenteral nutrition and antifungal therapy with 400 mg intravenous fluconazole daily for 21 days. She showed gradual clinical improvement and within a few days the nasogastric drainage stopped. The patient was started on enteric nutrition and then oral feeding, with good tolerance. Upper GI endoscopy was repeated, but the gastric mucosa had the same greyish-looking appearance. A biopsy was not attempted because the gastric mucosa was too friable. After discontinuation of antifungal therapy, there was gradual clinical worsening, with vomiting and the need for nasogastric tube replacement, again with high drainage. The fluconazole was reintroduced, but the patient died.
Figure 1.
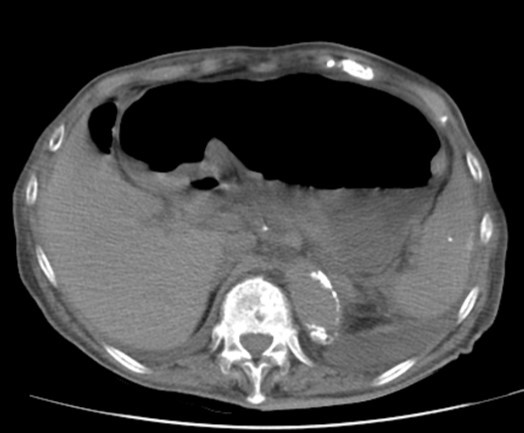
Abdominal CT revealing marked dilation of the gastric cavity filled with liquid and gas
Figure 2.
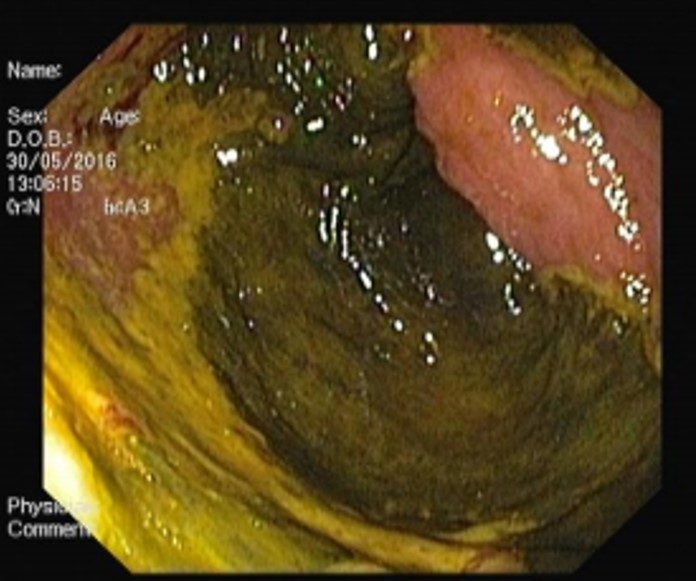
Upper gastrointestinal endoscopy showing the greyish appearance of the antrum mucosa
Figure 3.
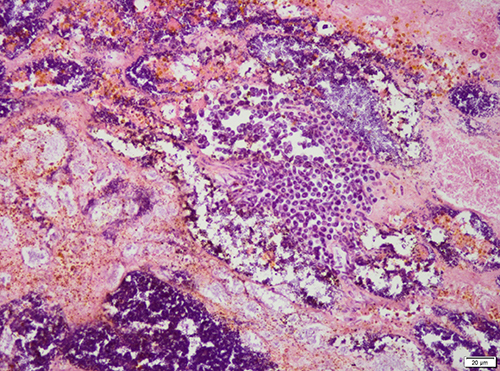
Histological examination: haematoxylin and eosin staining (400×) demonstrating spores and hyphae
Figure 4.
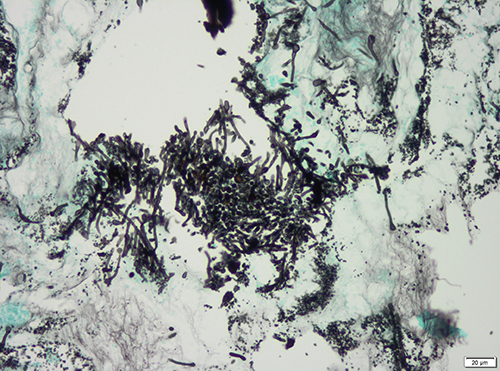
Histological examination: Grocott staining (400×) revealed non-branched and septate hyphae
DISCUSSION
This case report describes an unusual primary fungal infection, very likely candidiasis, in a rare location of the gastrointestinal tract. Candida is normally present in small amounts in the normal human GI tract[3]. Fungal overgrowth and colonization of the GI tract is mostly seen in the oesophagus and oral cavity, being less frequent in the stomach and rare in the duodenum. In our patient, there was evidence of gastroduodenal involvement but no oesophageal involvement.
The risk factors associated with fungal colonization of the gastric mucosa are old age, malnutrition, diabetes, trauma, burns, surgical operations, parenteral nutrition, intravascular or bladder catheterization, H2-blocker therapy, steroid therapy, immunosuppressive treatment and the use of wide-spectrum antibiotics[4]. Patients with three or more risk factors are considered to be vulnerable to infection, although there are some reports in the literature of gastric candidiasis in patients with one or even no risk factors. In 1976, Von Vitovec reported gastric candidiasis in two elderly patients with no associated underlying disease[5]. In 1979 Minoli et al. also reported two cases of primary and isolated gastroduodenal candidiasis without any underlying disease[6]. Our patient had only one of the risk factors cited above, namely old age.
Similarly to the cases reported by Minoli et al., the fungal infection in our patient was primary in nature and confined to the gastric and duodenal compartments.
GI endoscopy revealed no gastric peristalsis and no evidence of obstruction or suspicious lesions. Also, abdominal CT angiography showed no evidence of malignancy or suspicious lesions. Consequently, the authors believe that the gastric dilation was related to gastroparesis. There were no medication or other causes of gastroparesis in our patient and the gastroparesis only improved after antifungal therapy and not after prokinetic agents. Therefore, the authors assume the gastroparesis was due to the gastroduodenal fungal invasion.
There is a lack of literature on this topic, but a retrospective study of gastric candidiasis in 26 patients described three types of candidiasis seen on endoscopy: the thrush type, the nodular form and the ulcerated form[7]. The thrush type presents as a white or greenish-white membrane of variable location and extension, which is spread over inflamed mucosa but readily removed. The nodular form presents as nodular projections a few millimetres high overlaid with highly inflamed mucosa and mainly located in the antrum. The ulcerated type has no particular endoscopic features to distinguish it from other types of peptic ulcer[5]. We assume that our patient had the thrush type.
In most cases reported in the literature, patients were treated for 3 weeks (or less) with a variable antifungal drug, with good response and outcomes.
To conclude, the authors believe that advanced age, the extended period of hospitalization and being bedridden were important factors in the unfavourable outcome in this patient. We would like to stress that all medical decisions were carefully considered and discussed with the medical team and the patient’s family.
Ackowledgements
The authors would like to thank the Pathological Anatomy Department for providing the histological images and collaborating on this clinical case.
Footnotes
Conflicts of Interests: The Authors declare that there are no competing interests.
REFERENCES
- 1.Rai P, Chakraborty SB. Giant fungal gastric ulcer in an immunocompetent individual. Saudi J Gastroenterol. 2012;18:282–284. doi: 10.4103/1319-3767.98438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nelson RS, Bruni HC, Goldstein HM. Primary gastric candidiasis in uncompromised subjects. Gastrointest Endosc. 1975;22:92–94. doi: 10.1016/s0016-5107(75)73711-2. [DOI] [PubMed] [Google Scholar]
- 3.Sasaki K. Candida associated gastric ulcer relapsing in a different position with a different appearance. World J Gastroenterol. 2012;18:4450–4453. doi: 10.3748/wjg.v18.i32.4450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zwolińska-Wcisło M, Budak A, Bogdał J, Trojanowska D, Stachura J. Fungal colonization of gastric mucosa and its clinical relevance. Med Sci Monit. 2001;7:982–988. [PubMed] [Google Scholar]
- 5.Von Vitovec J. Kandidose des Magens. Fortschr Rontgenstr. 1976;124:289. [PubMed] [Google Scholar]
- 6.Minoli G, Terruzzi V, Rossini A. Gastroduodenal candidiasis occurring without underlying disease (primary gastroduodenal candidiasis). Report on two cases. Endoscopy. 1979;1:18–22. doi: 10.1055/s-0028-1098318. [DOI] [PubMed] [Google Scholar]
- 7.Minoli G, Terruzzi V, Butti G, Frigerio G, Rossini A. Gastric candidiasis: an endoscopic and histological study in 26 patients. Gastrointest Endosc. 1982;28:59–61. doi: 10.1016/s0016-5107(82)72998-0. [DOI] [PubMed] [Google Scholar]