

Abstract
Purpose:
CTLA-4 was the first inhibitory immune checkpoint to be identified. Two monoclonal antibodies, ipilimumab (IgG1) and tremelimumab (IgG2), which block the function of CTLA-4, have demonstrated durable clinical activity in a subset of patients with advanced solid malignancies by augmenting effector T cell-mediated immune responses. Studies in mice suggest that anti–CTLA-4 monoclonal antibodies may also selectively deplete intratumoral FOXP3+ regulatory T cells via an Fc-dependent mechanism. However, it is unclear whether the depletion of FOXP3+ cells occurs in cancer patients treated with anti-CTLA-4 therapies.
Experimental Design:
Quantitative immunohistochemistry was used to evaluate the densities of intratumoral CD4+, CD8+ and FOXP3+ cells in stage-matched melanoma (N=19), prostate cancer (N=17) and bladder cancer (N=9) samples treated with ipilimumab and in paired melanoma tumors (N=18) treated with tremelimumab. These findings were corroborated with multiparametric mass cytometry analysis of tumor infiltrating cells from paired fresh melanoma tumors (N=5) treated with ipilimumab.
Results:
Both ipilimumab and tremelimumab increase infiltration of intratumoral CD4+ and CD8+ cells without significantly changing or depleting FOXP3+ cells within the tumor microenvironment.
Conclusions:
Anti–CTLA-4 immunotherapy does not deplete FOXP3+ cells in human tumors, which suggests that their efficacy could be enhanced by modifying the Fc portions of the monoclonal antibodies to enhance Fc-mediated depletion of intratumoral regulatory T cells.
Keywords: FOXP3 Tregs, anti-CTLA-4, human tumors
Introduction
Cytotoxic T lymphocyte-associated protein 4 (CTLA-4) is an inhibitory immune checkpoint receptor that plays a crucial role in modulating T cell responses (1, 2). In preclinical studies, transient blockade of CTLA-4 resulted in tumor eradication and durable anti-tumor immunity (3). These findings translated into the clinical development of fully human monoclonal antibodies (mAbs) against CTLA-4, including ipilimumab and tremelimumab; an approach termed immune checkpoint blockade that has proven to be a paradigm shift in cancer therapy (4).
Initial preclinical studies primarily implicated effector T (Teff) cells in mediating the therapeutic activity of CTLA-4 blockade (1, 3); however, later studies demonstrated the contribution of both the effector and regulatory T cell compartments in promoting anti-tumor responses (5–10). Regulatory T cells (Tregs) maintain immune cell homeostasis and suppress anti-tumor immune responses. They express CD4, CD25 and forkhead box protein P3 (FOXP3), a transcription factor required for their function. In addition, Tregs constitutively express high levels of CTLA-4 on their surface (11–13), and FOXP3 is known to direct CTLA-4 transcription (14, 15), which led to the hypotheses that CTLA-4 blockade may impair the suppressive activity of Tregs or directly deplete Tregs via antibody-dependent cell-mediated cytotoxicity (ADCC) (16, 17).
More recent preclinical murine studies demonstrated that the therapeutic activity of anti-CTLA-4 mAbs (clones 9D9, 9H10 and 4F10) was dependent upon selective depletion of intratumoral Tregs via ADCC. In these studies, tumor regression was associated with an increase in the intratumoral Teff to Treg cell ratio, due to the preferential expansion of Teff cells and the selective depletion of Tregs (5, 7). Treg depletion was attributed to tumor-infiltrating macrophages expressing the Fc-receptor, FcγRIV (5). A murine anti-CTLA-4 mAb containing an IgG2a (clone 9D9) constant region was shown to exhibit enhanced ADCC-dependent intratumoral Treg depletion when compared to IgG2b and IgG1 murine anti-CTLA-4 mAbs (7).
Ipilimumab, the first fully human IgG1 mAb against CTLA-4, demonstrated durable clinical activity and prolonged survival in patients with advanced melanoma (18, 19). It has also been tested in other cancer types including non-small-cell lung cancer, renal cell carcinoma, urothelial carcinoma and prostate cancer (4). Similarly tremelimumab, an anti-CTLA-4 IgG2 mAb, has also been clinically studied across several tumor types (20). The humanized IgG1 mAb isotype binds to most human Fc receptors, and it has the ability to induce ADCC; whereas, the IgG2 isotype is known to have less ADCC activity (21). Clinical studies have been unclear in defining the role of IgG1 ipilimumab and IgG2 tremelimumab in depleting intratumoral Tregs in human cancers (9, 22).
The current study herein was conducted to gain insight on the effect of anti–CTLA-4 immunotherapy on the density of intratumoral FOXP3+ Tregs across several human cancer types, including melanoma, bladder cancer and prostate cancer. Our data provide evidence that CTLA-4 blockade does not decrease the density of FOXP3+ Tregs in human tumors.
Materials and Methods
Patient material
Formalin-fixed, paraffin-embedded (FFPE) tumor samples were collected from a cohort of stage-matched untreated and ipilimumab-treated primary prostate cancer patients (N=17), primary bladder cancer patients (N=9) and metastatic melanoma patients (N=19). The median time of tumor biopsy collection following last treatment with ipilimumab was 8 weeks for prostate and bladder tumors (post-dose 2 treatments) and 18 weeks for melanoma (post-dose 2–3 treatments). For the mass cytometry or CyTOF assay, tumor infiltrating cells were obtained from paired fresh melanoma tumors pre- and post-ipilimumab treatment (N=5). The tumor samples were retrieved from the MD Anderson Cancer Center Department of Pathology and Institutional Tumor Bank. All patients provided informed consent on The University of Texas MD Anderson Cancer Center institutional-approved laboratory protocol, PA13–0291. FFPE tumor samples from a cohort of paired metastatic melanoma patients (N=18) treated with tremelimumab were obtained from the Department of Hematology and Oncology, University of California Los Angeles institutional–approved protocol, 11–003254-AM-00019. The median time of post-treatment biopsy collection was 5 weeks following treatment with tremelimumab (post-dose 1 treatment). The institutional review boards of The University of Texas MD Anderson Cancer Center and University of California Los Angeles specifically approved these studies. All patients signed the informed consent forms and were given a unique code, thus protecting their identity.
Immunohistochemistry
Immunohistochemistry (IHC) was performed on FFPE tumor tissue sections. The tumor tissues were fixed in 10% formalin, embedded in paraffin, and transversely sectioned. Four μm sections were used for the IHC analyses. The sections were stained with mouse anti-human monoclonal antibodies against CD4 (Novocastra, CD4–368-L-A), CD8 (Thermo Scientific, MS-457-S), FOXP3 (Abcam, ab96048–206D) and CD68 (Dako, M0876). All sections were counterstained with hematoxylin, dehydrated, mounted, and processed with peroxidase-conjugated avidin/biotin and 3’−3-diaminobenzidine (DAB) substrate (Leica Microsystem). The IHC slides were scanned and digitalized using the scanscope system from Scanscope XT, Aperio/Leica Technologies. The IHC analysis was solely performed in the center of the tumor (CT) region across all tumor types.
Quantitative analysis of IHC staining was conducted using the image analysis software- ImageScope-Aperio/Leica. Five random areas (1 mm2 each) were selected using a customized algorithm for each marker to determine the number of positive cells per high power field (20X magnification), and the average of the five fields was taken. The pathologists in our team carefully reviewed the data generated by the automated image analysis Aperio software, and the data were expressed as a density score (total number of positive cells per 1 mm2 area). IHC staining was interpreted in conjunction with H&E stained sections, which facilitated the identification of malignant cells and thus directed IHC quantification.
CyTOF
Tumor infiltrating cells from paired fresh melanoma tumors pre- and post-ipilimumab treatment (N=5) were used for the CyTOF analysis. The tumor sample was dissociated with GentleMACS system (Miltenyi Biotec; Bergisch Gladbach, Germany) as per the manufacturer’s instructions and cultured overnight in a 96 well plate with RPMI 1640 medium; supplemented with 10% human AB Serum, 10 mM Hepes, 50 μM β-ME, penicillin/streptomycin/l-glutamine and 50 U/ml human IL-2. The cells were then collected and analyzed for seven analytes including CD45 (Fluidigm, HI30), CD3 (Fluidigm, UCTH1), CD4 (Fluidigm, RPA-T4), CD8 (Fluidigm, RPA-T8), CD56 (Fluidigm, NCAM16.2), FOXP3 (Fluidigm, PCH101), and CTLA-4 (Fluidigm, 14D3). The data was analyzed by gating on CD45+ live singlets using ViSNE (23) and FlowJo.
Statistical analysis
The statistical analysis for each immune subset between the untreated versus treated cohorts was performed using Mann-Whitney unpaired t-test for the unpaired tumor sections and Wilcoxon paired t-test for the paired tumor sections (P value; Graphpad-Prism). Statistical significance was defined as P < 0.05.
Results
Anti-CTLA-4 immunotherapy increases the density of intratumoral CD4+ and CD8+ cells.
Preclinical and early clinical studies suggest that CTLA-4 blockade promotes anti-tumor activity by increasing the frequency of intratumoral Teff cells (5, 7, 8, 10, 24, 25). To confirm these findings using tissues obtained from patients treated with two different anti-CTLA-4 mAbs, we examined the immune profile of melanoma tumors by immunohistochemistry (IHC). Our data demonstrate that both ipilimumab (Fig. 1A and Supplementary Fig. S1A) and tremelimumab (Fig. 1B) significantly increased the intratumoral densities of both CD4+ and CD8+ cells. Similar results have been reported in human melanoma upon treatment with tremelimumab (26). Consistent with these findings, we observed increased densities of intratumoral CD4+ and CD8+ cells in bladder and prostate tumors obtained from patients treated with ipilimumab (Supplementary Fig. S2A and S2B).
Figure 1: CTLA-4 blockade expands CD4+ and CD8+ cells.
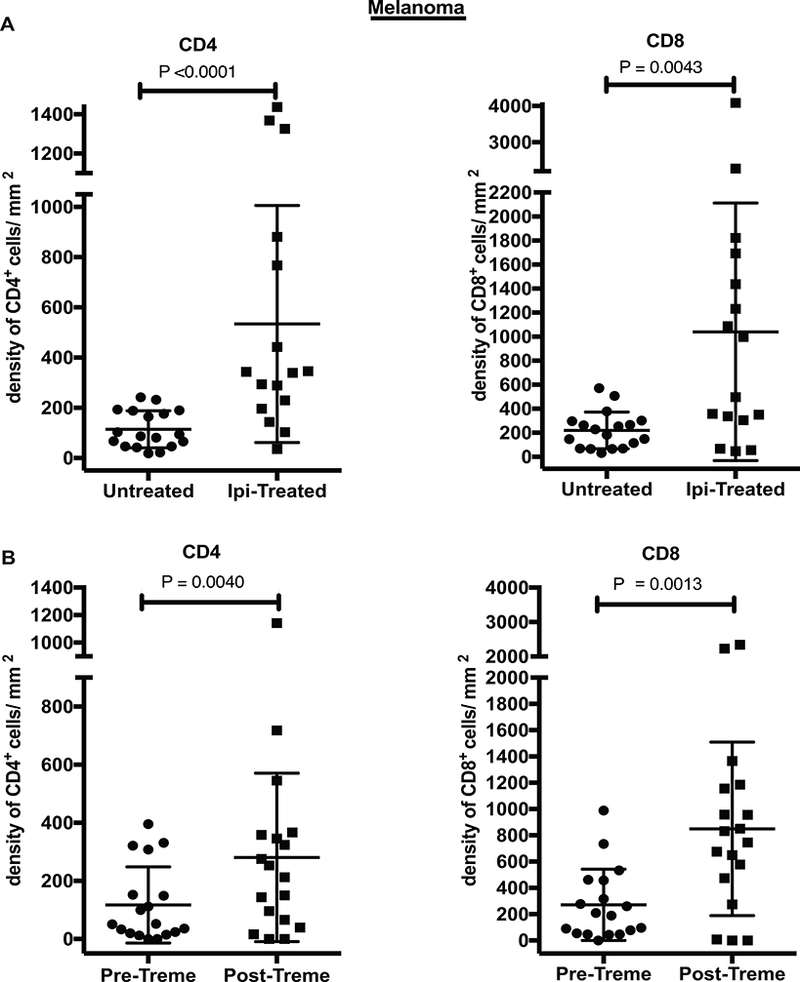
A) Stage-matched untreated (N=18) and ipilimumab (Ipi)-treated (N=16) metastatic melanoma tumor samples, and B) metastatic melanoma tumor samples (N=18) pre- and post-tremelimumab (Treme) treatment were analyzed by IHC for the presence of CD4+ and CD8+ cells. Each plot shows mean with standard deviation (SD), and each symbol represents an individual patient. Statistical significance is defined as P < 0.05.
Anti–CTLA-4 immunotherapy does not deplete intratumoral FOXP3+ cells in human cancers.
As it is postulated that human IgG1 mAbs promote ADCC to a greater extent than IgG2 (21), we evaluated the potential differential effects of ipilimumab (IgG1) and tremelimumab (IgG2) on the densities of FOXP3+ cells in tumor tissues from patients with advanced melanoma. Surprisingly, both ipilimumab (Fig. 2A and Supplementary Fig. S3) and tremelimumab (Fig. 2B) did not deplete, but instead significantly increased the density of FOXP3+ cells within the tumor microenvironment. Of note, pre-treatment biopsies from two patients with melanoma, which were negative for FOXP3+ cells, showed FOXP3+ cellular infiltration post-tremelimumab treatment (Fig. 2B).
Figure 2: Effect of CTLA-4 blockade on FOXP3+ cells in human melanoma.
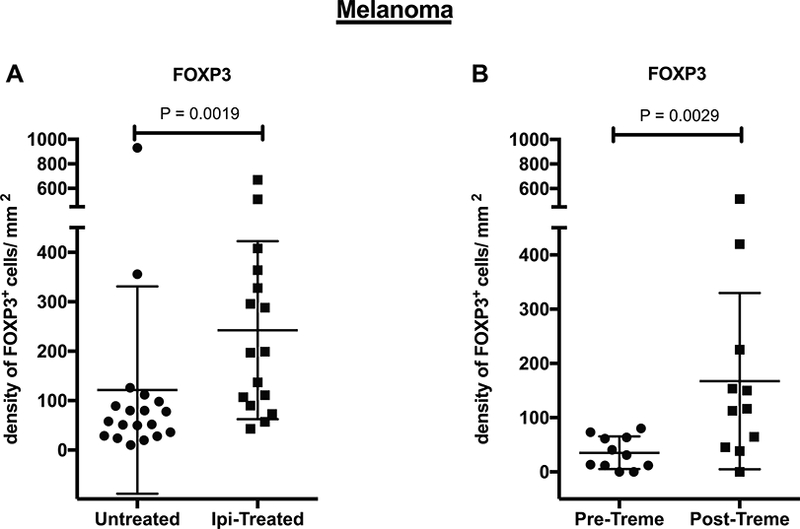
A) Stage-matched untreated (N=19) Ipi-treated (N=16) metastatic melanoma tumor samples, and B) metastatic melanoma tumor samples pre- and post-Treme treatment (N=11) were analyzed by IHC for the presence of FOXP3+ cells. Each plot shows mean with SD, and each symbol represents an individual patient. Statistical significance is defined as P < 0.05.
Furthermore, in bladder and prostate tumors obtained from patients treated with ipilimumab, there was no reduction in intratumoral FOXP3+ cells (Fig. 3 and Supplementary Fig. S3). Taken together, the data demonstrate that both ipilimumab and tremelimumab, despite having two different IgG isotypes with potentially different mechanisms of action, similarly augment the densities of intratumoral CD4+ and CD8+ cells, but do not deplete FOXP3+ cells.
Figure 3: Effect of CTLA-4 blockade on FOXP3+ cells in bladder and prostate tumors.
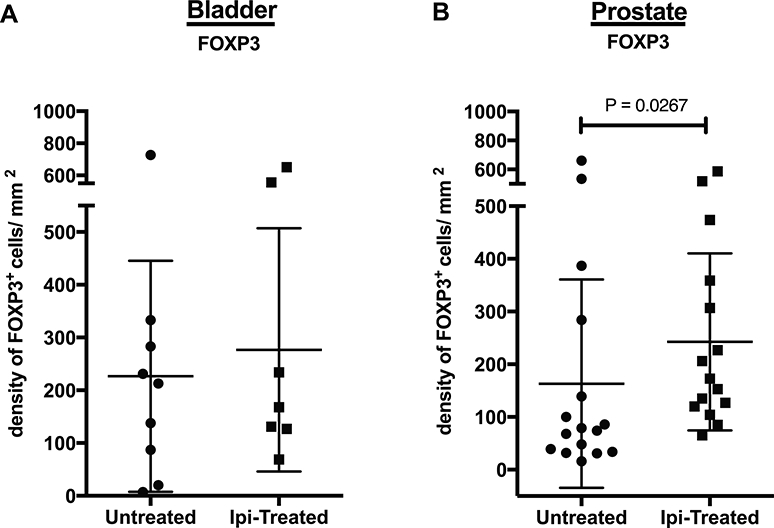
A) Stage-matched untreated and Ipi-treated bladder tumors (N=9), and B) prostate tumors (N=16) were analyzed by IHC for the presence of FOXP3+ cells. Each plot shows mean with SD, and each symbol represents an individual patient. Statistical significance is defined as P < 0.05.
Presence of tumor-associated macrophages in baseline and ipilimumab-treated biopsies
In humans, ADCC is primarily mediated by FcγRIIIA (CD16a) (27), which is expressed on macrophages and natural killer (NK) cells. The lack of intratumoral Treg depletion following treatment with ipilimumab could be attributable to a paucity of macrophages or NK cells and/or FcγRIIIA expression within the tumor microenvironment. Therefore, we sought to evaluate the effect of ipilimumab on intratumoral CD68+ macrophages in advanced melanoma patients. Compared to intratumoral CD4+ and CD8+ cell densities, there was considerable infiltration of CD68+ macrophage in the untreated tumor samples, which did not significantly change following treatment with ipilimumab (Fig. 4).
Figure 4: Effect of CTLA-4 blockade on CD68+ cells.
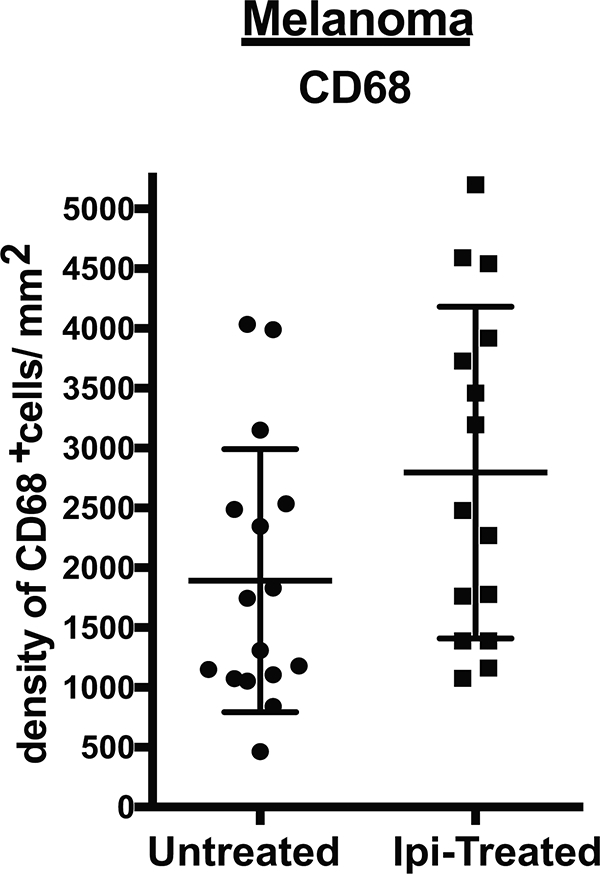
Stage-matched untreated and Ipi-treated (N=16) metastatic melanoma samples were analyzed by IHC for the presence of CD68+ cells. Each plot shows mean with SD, and each symbol represents an individual patient. Statistical significance is defined as P < 0.05.
Discussion
Anti–CTLA-4 immunotherapy has demonstrated significant anti-tumor activity in preclinical and clinical studies (3, 6, 18, 19, 28), and it has emerged as a paradigm shift in cancer therapy. Although the effect of CTLA-4 blockade on Teff cells has been well established, its effect on human FOXP3+ Tregs within the tumor microenvironment remains unclear. While some studies report a decrease in the frequency of circulating or intratumoral Tregs (5, 7, 9, 29, 30), other studies did not result in Treg depletion following anti-CTLA-4 treatment (11, 25, 26, 31, 32). The current study has been undertaken to gain a better understanding of the effect of anti-CTLA-4 therapy on intratumoral FOXP3+ Tregs in human cancers.
Preclinical studies have reported that CTLA-4 blockade results in an increase in the Teff to Treg ratio (5–7). Multiple studies have been conducted to evaluate Tregs in human tumors following anti-CTLA-4 therapy (24–26, 28, 32). However, most of these studies relied on the evaluation of intratumoral Tregs by flow cytometry with the calculation of FOXP3+ Tregs as a percentage of total cells. In previous studies, FOXP3+ Tregs were evaluated in bladder tumor tissues pre- and post-ipilimumab treatment. We observed an increase in the number of total T cells, but a decrease in frequency of FOXP3+ Tregs, which was measured as a percent of total cells (24, 25). Since the total number of T cells increased in post-treatment tumor tissues, our calculation of FOXP3+ Tregs as a percent of the total T cells led to data indicating a decrease in frequency of FOXP3+ Tregs, even though the absolute number of FOXP3+ cells may not have changed.
In the current study, we evaluated immune subsets including CD4+, CD8+ and FOXP3+ cells in tumor tissues obtained from patients treated with anti-CTLA-4 mAbs by quantitative IHC. We measured the density of T cell subsets in stage-matched human tumor tissues and found that anti-CTLA-4 therapy increases the density of intratumoral CD4+ and CD8+ cells, but without significant change or depletion of FOXP3+ cells. In addition, evaluation of paired pre-treatment and post-ipilimumab treatment melanoma tissues revealed higher densities of intratumoral CD8+ cells (Supplementary Fig. S1B) and FOXP3+ cells (Supplementary Fig. S1C).
Importantly, the timing of biopsy collection post-anti-CTLA-4 therapy (ipilimumab and tremelimumab) did not impact the infiltration of immune subsets (Supplementary Fig. S4). Consistent with this, an IHC study evaluating melanoma tumor samples (N=19) demonstrated higher infiltrates of FOXP3+ cells in the responding lesions following treatment with tremelimumab (26). Taken together, these results indicate that IHC may be a more reliable tool to examine treatment-related changes in immune subsets within the tumor, as it provides a more direct measure of the absolute numbers of cells in a given surface area.
The limitation of single stain IHC is that an individual marker may be expressed on more than one cellular population. For example, single staining for CD8 can represent both T cells and NK cells; likewise, staining for FOXP3 alone can represent Teff and Treg cells. To address this, we collaborated our IHC results with multiparametric CyTOF analysis of tumor infiltrating cells from paired pre- and post-ipilimumab-treated melanoma tissues. We found that greater than 95% of the CD8+ population were T cells (CD3+CD8+); whereas less than 5% of these were NK cells (CD3-CD8+CD56+). More importantly, ipilimumab significantly increased the frequency of CD8+ T cells but not CD8+CD56+ NK cells (Supplementary Fig. S5). Similarly, to differentiate between Teff and Treg cells, we evaluated coexpression of FOXP3, CD3, CD4 and CTLA-4. The data demonstrated ipilimumab increases the frequency of CD3+CD4+FOXP3+CTLA-4+ T cells (Tregs), but not CD3+CD4+FOXP3-CTLA-4+ and CD3+CD4+FOXP3-CTLA-4- T cells (Supplementary Fig. S6).
It has been reported that antibody-mediated depletion can occur via complement-mediated lysis (33) or ADCC (5). In mouse models, the anti-CTLA-4 therapy-mediated depletion of FOXP3+ Treg cells was dependent on the presence of intratumoral FcγRIV-expressing macrophages (5). In patients, ADCC is essentially mediated through an equivalent FcγR, namely FcγRIIIA (CD16) that is expressed on macrophages and NK cells (27), which may account for the discrepancy between the preclinical and clinical data. Our findings did not demonstrate significant changes in the intratumoral density of CD68+ macrophages after anti-CTLA-4 therapy; however, we did not evaluate FcγRIIIA expression in these human tumor samples.
In conclusion, our data illustrate that the IgG1 ipilimumab and IgG2 tremelimumab mAbs with distinct FcγR-mediated mechanisms do not deplete intratumoral FOXP3+ cells in human cancers.
Supplementary Material
Statement of translational relevance.
In preclinical murine models, anti-CTLA-4 monoclonal antibodies promote cancer regression by increasing the frequency of effector T cells within the tumor microenvironment and selectively depleting intratumoral regulatory T cells via an Fc-dependent mechanism. However, it is unclear whether this occurs in cancer patients treated with anti-CTLA-4 therapies. Herein, we show that treatment with IgG1 ipilimumab and IgG2 tremelimumab monoclonal antibodies, which have distinct FcγR-mediated mechanisms, increase the density of intratumoral CD4 and CD8 T cells, and do not deplete FOXP3+ Tregs across different human tumors. These data suggest that there is an opportunity to improve the clinical efficacy of anti-CTLA-4 immunotherapies by modifying the monoclonal antibodies to promote the depletion of intratumoral regulatory T cells.
Acknowledgements
Immune monitoring studies were performed at the Immunotherapy Platform, The University of Texas MD Anderson Cancer Center with funding from NIH/NCI R01 CA1633793 (P.S.) and a Prostate Cancer Foundation 2014 young investigator award (S.K.S.). Drs. Sharma, Allison, and Wargo are members of the Parker Institute for Cancer Immunotherapy at MD Anderson Cancer Center and Dr. Ribas is a member of Parker Institute for Cancer Immunotherapy at University of California Los Angeles.
We would like to thank Ashura Khan, Sheila Duncan and Marla Polk for administrative support; Maria Higa for technical support and Spencer Wei for scientific discussions.
Footnotes
Conflict of interest
Drs. Sharma an Allison are founders of Jounce Therapeutics. Dr. Sharma also serves as a consultant for Bristol-Myers Squibb (BMS), Amgen, Constellation Pharmaceuticals, Jounce Therapeutics, Kite Pharma, Evelo, Neon Therapeutics, EMD Serono, Astellas Pharma, AstraZeneca, BioAtla, Pieris Pharmaceuticals, Oncolytics Biotech, Merck Sharp & Dohme. Dr. Allison is an inventor and recipient of royalty from intellectual property licensed to BMS and Merck and is also a consultant for Jounce Therapeutics, Neon Therapeutics, Amgen and Kite Pharma. All other authors have no relevant conflicts of interest to disclose
References
- 1.Walunas TL, Lenschow DJ, Bakker CY, Linsley PS, Freeman GJ, Green JM, et al. CTLA-4 can function as a negative regulator of T cell activation. Immunity. 1994;1(5):405–13. [DOI] [PubMed] [Google Scholar]
- 2.Krummel MF, and Allison JP. CD28 and CTLA-4 have opposing effects on the response of T cells to stimulation. The Journal of experimental medicine. 1995;182(2):459–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Leach DR, Krummel MF, and Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science. 1996;271(5256):1734–6. [DOI] [PubMed] [Google Scholar]
- 4.Sharma P, and Allison JP. The future of immune checkpoint therapy. Science. 2015;348(6230):56–61. [DOI] [PubMed] [Google Scholar]
- 5.Simpson TR, Li F, Montalvo-Ortiz W, Sepulveda MA, Bergerhoff K, Arce F, et al. Fc-dependent depletion of tumor-infiltrating regulatory T cells co-defines the efficacy of anti-CTLA-4 therapy against melanoma. The Journal of experimental medicine. 2013;210(9):1695–710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Quezada SA, Peggs KS, Curran MA, and Allison JP. CTLA4 blockade and GM-CSF combination immunotherapy alters the intratumor balance of effector and regulatory T cells. J Clin Invest. 2006;116(7):1935–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Selby MJ, Engelhardt JJ, Quigley M, Henning KA, Chen T, Srinivasan M, et al. Anti-CTLA-4 antibodies of IgG2a isotype enhance antitumor activity through reduction of intratumoral regulatory T cells. Cancer Immunol Res. 2013;1(1):32–42. [DOI] [PubMed] [Google Scholar]
- 8.Peggs KS, Quezada SA, Chambers CA, Korman AJ, and Allison JP. Blockade of CTLA-4 on both effector and regulatory T cell compartments contributes to the antitumor activity of anti-CTLA-4 antibodies. The Journal of experimental medicine. 2009;206(8):1717–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Romano E, Kusio-Kobialka M, Foukas PG, Baumgaertner P, Meyer C, Ballabeni P, et al. Ipilimumab-dependent cell-mediated cytotoxicity of regulatory T cells ex vivo by nonclassical monocytes in melanoma patients. Proceedings of the National Academy of Sciences of the United States of America. 2015;112(19):6140–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wada S, Jackson CM, Yoshimura K, Yen HR, Getnet D, Harris TJ, et al. Sequencing CTLA-4 blockade with cell-based immunotherapy for prostate cancer. J Transl Med. 2013;11:89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kavanagh B, O’Brien S, Lee D, Hou Y, Weinberg V, Rini B, et al. CTLA4 blockade expands FoxP3+ regulatory and activated effector CD4+ T cells in a dose-dependent fashion. Blood. 2008;112(4):1175–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Takahashi T, Tagami T, Yamazaki S, Uede T, Shimizu J, Sakaguchi N, et al. Immunologic self-tolerance maintained by CD25(+)CD4(+) regulatory T cells constitutively expressing cytotoxic T lymphocyte-associated antigen 4. The Journal of experimental medicine. 2000;192(2):303–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zheng Y, and Rudensky AY. Foxp3 in control of the regulatory T cell lineage. Nature immunology. 2007;8(5):457–62. [DOI] [PubMed] [Google Scholar]
- 14.Jain N, Nguyen H, Chambers C, and Kang J. Dual function of CTLA-4 in regulatory T cells and conventional T cells to prevent multiorgan autoimmunity. Proceedings of the National Academy of Sciences of the United States of America. 2010;107(4):1524–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wu Y, Borde M, Heissmeyer V, Feuerer M, Lapan AD, Stroud JC, et al. FOXP3 controls regulatory T cell function through cooperation with NFAT. Cell. 2006;126(2):375–87. [DOI] [PubMed] [Google Scholar]
- 16.Wing K, Onishi Y, Prieto-Martin P, Yamaguchi T, Miyara M, Fehervari Z, et al. CTLA-4 control over Foxp3+ regulatory T cell function. Science. 2008;322(5899):271–5. [DOI] [PubMed] [Google Scholar]
- 17.Read S, Greenwald R, Izcue A, Robinson N, Mandelbrot D, Francisco L, et al. Blockade of CTLA-4 on CD4+CD25+ regulatory T cells abrogates their function in vivo. Journal of immunology (Baltimore, Md : 1950). 2006;177(7):4376–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Robert C, Thomas L, Bondarenko I, O’Day S, Weber J, Garbe C, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364(26):2517–26. [DOI] [PubMed] [Google Scholar]
- 20.Ribas A Clinical development of the anti-CTLA-4 antibody tremelimumab. Seminars in oncology. 2010;37(5):450–4. [DOI] [PubMed] [Google Scholar]
- 21.Beers SA, Glennie MJ, and White AL. Influence of immunoglobulin isotype on therapeutic antibody function. Blood. 2016;127(9):1097–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Smyth MJ, Ngiow SF, Ribas A, and Teng MW. Combination cancer immunotherapies tailored to the tumour microenvironment. Nat Rev Clin Oncol. 2016;13(3):143–58. [DOI] [PubMed] [Google Scholar]
- 23.Amir el AD, Davis KL, Tadmor MD, Simonds EF, Levine JH, Bendall SC, et al. viSNE enables visualization of high dimensional single-cell data and reveals phenotypic heterogeneity of leukemia. Nat Biotechnol. 2013;31(6):545–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Liakou CI, Kamat A, Tang DN, Chen H, Sun J, Troncoso P, et al. CTLA-4 blockade increases IFNgamma-producing CD4+ICOShi cells to shift the ratio of effector to regulatory T cells in cancer patients. Proceedings of the National Academy of Sciences of the United States of America. 2008;105(39):14987–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Carthon BC, Wolchok JD, Yuan J, Kamat A, Ng Tang DS, Sun J, et al. Preoperative CTLA-4 blockade: tolerability and immune monitoring in the setting of a presurgical clinical trial. Clin Cancer Res. 2010;16(10):2861–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Huang RR, Jalil J, Economou JS, Chmielowski B, Koya RC, Mok S, et al. CTLA4 blockade induces frequent tumor infiltration by activated lymphocytes regardless of clinical responses in humans. Clin Cancer Res. 2011;17(12):4101–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Yeap WH, Wong KL, Shimasaki N, Teo EC, Quek JK, Yong HX, et al. CD16 is indispensable for antibody-dependent cellular cytotoxicity by human monocytes. Sci Rep. 2016;6:34310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hodi FS, Butler M, Oble DA, Seiden MV, Haluska FG, Kruse A, et al. Immunologic and clinical effects of antibody blockade of cytotoxic T lymphocyte-associated antigen 4 in previously vaccinated cancer patients. Proceedings of the National Academy of Sciences of the United States of America. 2008;105(8):3005–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Du X, Tang F, Liu M, Su J, Zhang Y, Wu W, et al. A reappraisal of CTLA-4 checkpoint blockade in cancer immunotherapy. Cell research. 2018;28(4):416–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Arce Vargas F, Furness AJS, Litchfield K, Joshi K, Rosenthal R, Ghorani E, et al. Fc Effector Function Contributes to the Activity of Human Anti-CTLA-4 Antibodies. Cancer cell. 2018;33(4):649–63.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Retseck J, VanderWeele R, Lin HM, Lin Y, Butterfield LH, and Tarhini AA. Phenotypic and functional testing of circulating regulatory T cells in advanced melanoma patients treated with neoadjuvant ipilimumab. Journal for immunotherapy of cancer. 2016;4:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ribas A, Comin-Anduix B, Economou JS, Donahue TR, de la Rocha P, Morris LF, et al. Intratumoral immune cell infiltrates, FoxP3, and indoleamine 2,3-dioxygenase in patients with melanoma undergoing CTLA4 blockade. Clin Cancer Res. 2009;15(1):390–9. [DOI] [PubMed] [Google Scholar]
- 33.Reff ME, Carner K, Chambers KS, Chinn PC, Leonard JE, Raab R, et al. Depletion of B cells in vivo by a chimeric mouse human monoclonal antibody to CD20. Blood. 1994;83(2):435–45. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.