

Abstract
Background
In Ethiopia uncomplicated severe acute malnutrition (SAM) is managed at health posts level through the outpatient therapeutic program (OTP). Yet, evidence on the treatment success rate of the program is scarce. This study determines the treatment outcomes and predictors of time-to-recovery among children 6–59 months of age with SAM managed at the health posts level in Shebedino district, Southern Ethiopia.
Methods
This was a prospective cohort study that enrolled 216 children with SAM identified through a campaign conducted in May 2015 and treated over eight weeks at 25 health posts of the district. The average time-to-recovery was estimated using Kaplan-Meier survival curve and the independent predictors of the recovery were determined using multivariable Cox-proportional hazard model. The outputs of the analyses are presented via adjusted hazard ratio with 95% confidence intervals (AHR, CI).
Results
At the end of the eight weeks of treatment 79.6% (95% CI: 74.2–85.0%) of cases recovered from SAM with a weight gain rate of 5.4 g/kg/day. The median time-to-recover was 36 days. The analysis indicated, maternal illiteracy (0.54, 0.38–0.78), severe household food insecurity (0.47, 0.28–0.79), walking for more than 1 h to receive the treatment (0.69, 0.50–0.96), diarrhoea co-morbidity (0.63, 0.42–0.91) and practicing sharing of ready to use therapeutic food (RUTF) (0.53, 0.32–0.88) were associated with slower propensity of recovery from SAM. Children who were enrolled with marasmus diagnosis showed lower recovery than children with kwashiorkor (0.30, 0.18–0.51).
Conclusion
The median time-to-recover was 36 days. Discouraging sharing of RUTF, appropriate management of diarrhoea in SAM cases and improving access to OTP sites can help to improve the treatment outcome for SAM.
Electronic supplementary material
The online version of this article (10.1186/s12887-019-1407-9) contains supplementary material, which is available to authorized users.
Keywords: Severe acute malnutrition, Outpatient therapeutic program, Treatment outcome, Time-to-recovery, Diarrhoea, Ethiopia
Background
Childhood undernutrition remains a major public health problem in the world. Undernutrition is considered as an the underlying cause for nearly half of the global childhood deaths – 3.1 million deaths annually [1, 2]. Despite the significant strides made in promoting child survival in the last two decades, Ethiopia remains one of the countries with highest burden of undernutrition [1, 3]. According to the recent demographic and health survey (DHS), in Ethiopia 38% of the children under the age of five years are stunted; further, 24 and 10% are underweight and wasted, respectively [3].
Severe acute malnutrition (SAM) – the most severe form of malnutrition – is defined as weight-for-height z-score below minus three standard deviations, or middle upper arm circumferences (MUAC) less than 110 mm or the presence of first or second degree bilateral pitting oedema [4]. As of 2016, globally SAM affects 17 million children, of which 98% are either from Asia or Africa [5]. Every year SAM approximately contributes to one million childhood deaths [6]. In Ethiopia, the prevalence of severe wasting is estimated to be 3% [3]. As of 2016, nearly half a million children in the country were in need of treatment for SAM [7].
SAM is a life threatening condition that requires urgent medical attention. The degree of wasting has dose-effect relationship with the risk of death and the risk of mortality is approximately 5–20 folds higher among SAM cases compared to well-nourished children [2]. Furthermore, surviving cases are susceptible to infections and may develop long-lasting physical and cognitive consequences [2].
With timely detection and improved access to standardized treatment, case-fatality rates from SAM can substancially be reduced to less than 5% [8, 9]. Consequently, many countries including Ethiopia have adopted a community- based strategy for scaling up and bringing the treatment closer to the grassroots level [9]. According to the World Health Organization (WHO) and the national guideline, children who have passed an appetite test and are judged to be clinically well should be treated on outpatient bases through the Outpatient Therapeutic Program (OTP). Nevertheless, children with medical complications, severe oedema or poor appetite should be managed as inpatients [4, 10].
In Ethiopia, since 2008 the treatment of uncomplicated SAM had been decentralized to the lowest primary health care unit and shifted to the outpatient setting [10, 11]. Nevertheless, limited information exists regarding the outcome of SAM treatment provided through this decentralized approach. The available few studies employed retrospective design and were reliant on secondary data extracted from medical records [11–16]. Consequently, they might not have captured key variables and can be liable to systematic errors.
Accordingly, this prospective cohort study was conducted to determine level and predictors of time-to-recovery from SAM in children 6–59 months of age managed through the OTP in Shebedino, Southern Ethiopia.
Methods
Study setting
The study was conducted from June to August 2015 in Shebedino district of Sidama zone, Southern Ethiopia. The district is located in the Great Rift Valley area, about 300 kms South of Addis Ababa, the capital of Ethiopia. Shebedino is administratively subdivided into 35 kebeles (32 rural and 3 urban). A kebele is the smallest administrative unit in Ethiopia comprising approximately 1000 households. In 2015, Shebedino had an estimated population of 294,214; of these 14% were infants and children 6–59 months of age.
Shebedino is affected by recurrent and chronic food insecurity. In the district, the average farmland ownership by a household is around 0.5 ha. Crop cultivation and livestock rearing are the major livelihood activities in the rural areas. Maize and Enset (false banana) are the major staple foods.
The district has one primary hospital, nine health centers and thirty two health posts, making the potential health service coverage 98%. According to the health care system of Ethiopia, every kebele is expected to have a health post whereby at least two health extension workers (HEWs) are deployed to provide a package of preventive and essential curative services including the management of uncomplicated SAM in children. HEWs identify SAM cases from their catchment area through multiple modalities including periodical growth monitoring and promotion, enhanced outreach strategy (EOS)/community health day (CHD) campaigns, and static service provided at the health post.
Study design
A prospective cohort study was conducted among children aged 6–59 months with uncomplicated SAM enrolled at the OTP sites of the district following a CHD campaign conducted in late May 2015. The cases were followed for the maximum eight weeks through weekly visits starting from June 01, 2015. However, children who recovered earlier were only followed until recovery. Screening of the children and administration of the treatment were made by the frontline health workers according to the national protocol without any direct involvement of the research team.
Study participants
All children 6–59 months of age who were newly diagnosed with uncomplicated SAM during the CHD campaign and got enrolled in the OTP program were eligible for the study. According to the national protocol, uncomplicated SAM cases are diagnosed as children with good appetite and no major medical complication having MUAC of less than 110 mm and/or first or second degree bilateral pitting oedema [4].
According to the national protocol patients fulfilling the admission criteria are enrolled and given a weekly Plumpy’Nut ration – trade name of a peanut-based ready-to-use therapeutic food (RUTF). Each week, their weight is taken until they achieve a target weight stated in the protocol. On each visit the children are expected to receive a medical assessment and caregivers should be given nutrition education [4]. As the study employed an observational design, the research team was not involved in any aspect of the treatment of the children.
Sampling approach
An optimal sample size of 219 children with SAM was determined using Stata 11.0 program based on formula designed for survival analysis. The inputs for the computation were: 95% confidence level, 80% power, 1.5 adjusted hazard ratio to be detected as significant (equivalence of medium effect size) for time-to-recovery outcome variable and 15% compensation for possible non-response. Further, based on the sample size calculation formula for estimating a population average, the sample size (n = 219) was considered adequate for determining the median time-to-recovery.
From the total 32 rural health posts found in the district, 25 were selected purposively based on the availability of new SAM cases recruited for OTP during the CHD screening. The total sample size 219 was distributed to health posts proportionally to their newly recruited SAM cases and ultimately the study subjects were selected using quota sampling technique (Fig. 1).
Fig. 1.
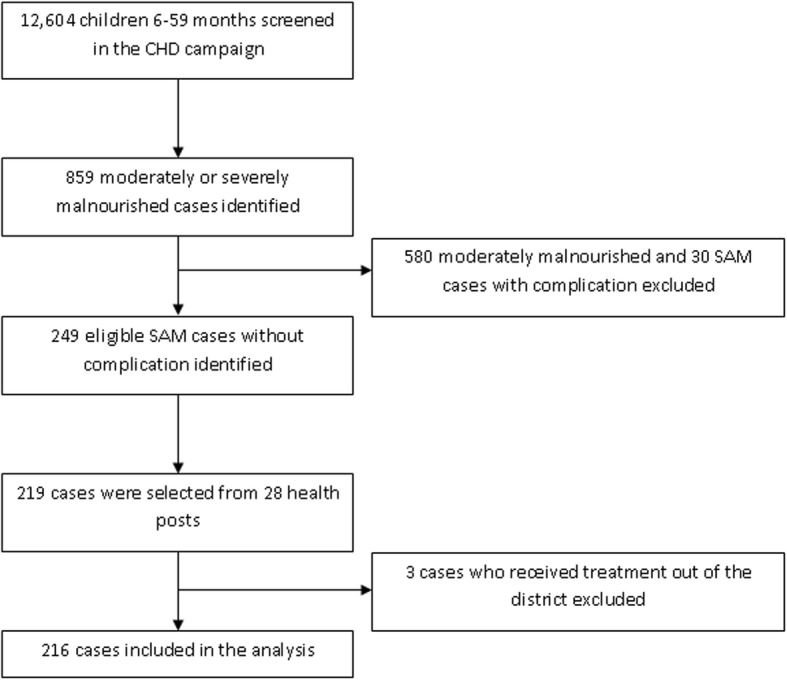
Flowchart of the study
At the end of the CHD camping 219 malnourished children were recruited for the study. Nevertheless, at the first follow-up 3 children were excluded as they were receiving the treatment from health posts found outside Shebedino district. The remaining 216 children were followed for a maximum duration of eight weeks and hence included in the analysis.
Data collection procedure
Data were gathered by eleven trained enumerators and supervisors using a structured and pretested questionnaire. Baseline data were collected at enrolment and follow-up measurements were made on weekly bases for a maximum of eight weeks.
Socio-demographic and economic variables were gathered at baseline using standard questions extracted from the DHS questionnaire [17]. Dietary Diversity (DD) of the children was assessed at baseline and consecutive weekly follow-up visits by asking the caregivers whether the child had taken from the standard seven food groups recommended by the WHO in the preceding day of the study without setting a minimum intake restriction [18]. The seven food groups were: (i) grains, roots and tubers; (ii) legumes and nuts; (iii) milk and milk products excluding breast milk; (iv) flesh foods; (v) eggs; (vi) vitamin A-rich fruits and vegetables; and (vii) others fruits and vegetables [18]. Household food security was measured at baseline using the Household Food Insecurity Access Scale (HFIAS) by asking about the occurrence and frequency of occurrence of nine food insecurity related events in the preceding four weeks of the survey. Ultimately the food security situation was classified into four ordinal categories: secure, and mild, moderate and severe insecurity [19]. Recent illness history of the child was assessed by asking the caregiver whether the child had fever, cough and diarrhoea in the preceding two weeks of the interview. The questionnaire used for collecting the data is provided as a supporting file with this manuscript (Additional file 1).
Anthropometric measurements – height, weight and MUAC – of the children were taken at baseline and on successive weekly visits using calibrated equipments following standardized procedures. Height and weight were measured without shoes and wearing light clothes using portable stadiometer and Salter spring scales. Height and weight were measured to the nearest 0.1 cm and 100 g, respectively. MUAC was measured at the middle point of the left arm to the nearest 0.1 cm using MUAC tape. Bilateral pitting oedema was assessed by applying normal thumb pressure for 3 s to the both feet.
Variables of the study
The dependent variable of the study is time-to-recover from SAM (i.e. the event of interest is recovery and that the response variable is rate of recovery). The independent variables considered are: age and sex of the child, maternal and paternal educational status, level of household food insecurity, household wealth index, distance from the OTP sites, perceived severity of SAM by the caregivers, perceived benefit of SAM treatment, type of malnutrition (Marasmus or Kwashiorkor), dietary diversity and clinical symptoms (diarrhoea, cough and fever). As described in the following conceptual framework, the independent variables were grouped into distal and proximal factors (Fig. 2).
Fig. 2.

Conceptual framework of the study describing the distal and proximal determinants of time-to-recovery from SAM
Statistical methods
Data were entered, cleaned, and analyzed using SPSS for windows, version 20. Data were described using frequencies, percentages and proper measure of central tendency and dispersion.
During enrollment and follow-ups, dietary diversity scores (DDSs) were determined weekly by summing up the number of unique food groups the child received in the preceding day of the assessment. Ultimately a grand DDS was computed by averaging all the available weekly scores by the number of observations. A grand score of 4 or more was considered as optimal DDS [18].
The treatment outcomes were classified as recovered, non-responder and defaulter in line with the national protocol for the management of SAM [4] and the effectiveness of the program is judged by the Global SPHERE standards [20]. Recovery was defined based on the criteria used to diagnose SAM upon enrollment. For children admitted to OTP based on low MUAC, MUAC greater than 110 mm at two consecutive weeks and/or achieving target weight gain within the maximum stay of 8 weeks in the OTP were used to define recovery. For children admitted based on edema, recovery was resolution of edema at two consecutive weeks. Conversely, children who fail to achieve the aforementioned recovery criteria within the maximum eight weeks treatment were considered as non-responders. Children who missed appointments for two consecutive weeks while being confirmed that they are alive were considered as defaulters.
The time-to-recover from SAM was determined by calculating the differences (in day) from the start of treatment until the child were declared recovered. The average time-to-recover in days was estimated using Kaplan-Meier survival analysis.
Predictors of time-to-recovery were identified using bivariable and multivariable Cox-proportional hazard models (CPHM). All independent variables that had p-value less than 0.25 in bivariable model were considered as candidate variables for the multivariable model. In order to avoid over adjustment bias, proximal and distal variables were fitted in separate models in accordance with the conceptual framework of the study. The output of the multivariable CPHM is presented using adjusted hazard ratios (AHR) with the respective 95% confidence intervals (CI). The proportional hazard assumption of the model was assessed on the basis of Schoenfeld residuals. Multicolinearity was checked using variance inflation factor.
For the distal CPHM model a total of eight variables were considered. These were: sex and age of the index child, maternal and paternal educational status, agro-ecology of the kebele, household food insecurity status, household wealth index, two-way travelling distance to the health post, and home visit by HEWs during the follow-up period. In the bivariable analyses, five variables (age of the child, maternal literacy, agro-ecological zone, food insecurity and distance to health post) had p-values less than 0.25 and hence considered for the multivariable model.
For the proximal CPHM a total of nine variables were considered. The variables were DDS, type of nutritional diagnosis at baseline, occurrence of diarrhoea, fever and cough, RUTF sharing and selling practices, breastfeeding status and maternal perception on severity of SAM. After the bivariable analyses, all of the variables except breastfeeding status were found eligible (p-value < 0.25) for the multivariable analysis.
Household wealth index was computed using Principal Component Analysis (PCA) as an indicator of household wealth status. A total of fifteen variables related to ownership of selected household assets, size of agricultural land, quantity of livestock, materials used for housing construction, and ownership of improved water and sanitation facilities were considered. Ultimately the generated score was divided into quintiles: poorest, poorer, middle, richer, and richest.
Ethical considerations
The research protocol was reviewed and approved by the institutional review board (IRB) of College of Medicine and Health Science, Hawassa University. Data were collected after securing informed verbal consent from the caregivers of the children. Verbal consent, instead of written consent, was preferred because most of the study respondents were not literate. The same was approved by the IRB that reviewed the protocol of the study. Confidentiality was maintained while handling participants’ information. Nutrition education was given to the entire caregivers.
Results
Socio-demographic characteristics
Among 216 study subjects enrolled in the study, the boys-to-girls ratio was 1.08 and at enrolment 36.1% were younger than 24 months of age. The mean (±SD) age of the caregivers was 30.1 (±7.0) years and 87.5% were married. More than two-thirds (72.2%) didn’t attend any formal education and about three-fourths (76.4%) were housewives. Nearly two-thirds (65.7%) of the children were sampled from midland areas (1750 to 2300 m above sea level) (Table 1).
Table 1.
Socio-demographic and economic characteristics of the study participants
| Variables (n = 216) | Frequency | Percent |
|---|---|---|
| Sex of the child | ||
| Male | 104 | 48.1 |
| Female | 112 | 51.9 |
| Age of children (months) | ||
| 6–11 | 44 | 20.4 |
| 12–23 | 34 | 15.7 |
| 24–35 | 29 | 13.4 |
| 36–47 | 46 | 21.3 |
| 48–59 | 63 | 29.2 |
| Maternal education | ||
| No formal education | 156 | 72.8 |
| Primary school | 60 | 27.2 |
| Paternal education | ||
| No formal education | 151 | 69.9 |
| Primary school | 65 | 30.1 |
| Mother’s occupation | ||
| Housewife | 165 | 76.4 |
| Others | 51 | 23.6 |
| Agro-ecological zone | ||
| Highland | 74 | 34.3 |
| Midland | 142 | 65.7 |
Nutritional and related characteristics of children at OTP enrollment
Household food insecurity assessment at baseline indicated that all of the households had experienced food insecurity with different degrees of severity in the preceding four weeks of the survey. Nearly half of the respondents (45.4%) had to walk for more than an hour to receive the OTP service from the nearby health post.
At baseline 68.1% of the cases were Marasmic (MUAC< 110 mm) while the remaining 31.9% had Kwashiorkor (presence of bilateral pitting oedema irrespective of anthropometric status). Study participants enrolled in the study with an average weight (±SD) of 8.5 (±2.6) kgs. On admission the vast majority (91.2%) of the children had suboptimal DDS. But nearly half (47.7%) of them were still breastfeeding. Regarding the occurrence of common childhood ailments, 12.5, 42.4 and 45.1% of the children, had cough, diarrhea and fever in the reference two weeks, respectively.
During the first follow-up visit carried out a week after OTP enrolment, the RUTF utilization pattern was assessed. It was found that RUTF sharing (35.2%) and selling (20.8%) practices were not rare. Nearly quarters (24.5%) of the respondents were aware that RUTF is both food and medicine to children with severe malnutrition (Table 2).
Table 2.
Nutritional and related characteristics of children with SAM enrolled in OTP
| Variables (n = 216) | Frequency | Percent |
|---|---|---|
| Household food security status | ||
| Secure | 0 | 0.0 |
| Mild | 22 | 10.2 |
| Moderate | 53 | 24.5 |
| Severe | 141 | 65.3 |
| Two-way walking distance to the OTP | ||
| Less than an hour | 118 | 54.6 |
| More than an hour | 98 | 45.4 |
| Visited at home by HEWs during the treatment | ||
| Yes | 67 | 31.0 |
| No | 149 | 69.0 |
| Receiving nutrition education during the treatment | ||
| Yes | 147 | 68.1 |
| No | 69 | 31.9 |
| Nutritional diagnosis at admission | ||
| Marasmus | 147 | 68.1 |
| Kwashiorkor | 69 | 31.9 |
| Ailment in the past 2 weeks | ||
| Diarrhoea | 115 | 42.4 |
| Cough | 34 | 12.5 |
| Fever | 122 | 45.1 |
| Breastfeeding status at admission | ||
| Still breastfeeding | 103 | 47.7 |
| Stopped breastfeeding | 113 | 52.3 |
| Dietary diversity score at admission | ||
| Suboptimal (< 4) | 197 | 91.2 |
| Optimal (≥4) | 19 | 8.8 |
| RUTF sharing at first follow-up | ||
| Yes | 76 | 35.2 |
| No | 140 | 64.8 |
| RUTF selling during the first week | ||
| Yes | 45 | 20.8 |
| No | 171 | 79.2 |
| Caregivers perception on RUTF | ||
| Food and medicine | 87 | 40.3 |
| Food for SAM child | 53 | 24.5 |
| Medicine for SAM child | 76 | 35.2 |
Time-to-recovery and treatment outcomes of children with SAM
From the total study subjects, 79.6% (95% CI: 74.2–85.0%) successfully recovered from SAM within the first eight weeks of treatment. Conversely, nearly one-fifth (20.4%) were censored. Reasons for censoring were: failure to respond to the treatment (11.1%), defaulting from the treatment (3.7%) and transferred out (5.6%).
The median time-to-recovery as determined by the Kaplan-Meier survival analysis, was 5 weeks (95% CI: 4.67–5.33) or 36.0 days (95% CI: 34.3–37.7). The overall mean (±SD) daily weight gain rate was 5.4 (2.6) gm/kg/day for the recovered children.
Determinants of recovery from SAM
Predictors of recovery were identified using Cox-proportional hazard model fitted separately to the distal and proximal factors in line with the conceptual framework of the study. In the distal multivariable model, maternal education status, agro-ecological zone of the kebele, household food insecurity status, and distance from the OTP site turned out to be significant predictors of recovery from SAM. Children having caregivers with no formal education had 46% reduced chance of recovery than their counterparts. Children from the highlands showed 43% lower probability of recovery as compared to those from the midlands. Those from severely food insecure household were 53% less likely to recover than cases from mildly food insecure households. Children who reside more than an hour walking distance from the OTP site had 31% reduced chance of recovery than their counterparts (Table 3).
Table 3.
Outputs of the Cox-proportional hazard model analyses on the distal and proximate predictors of time-to-recovery from severe acute malnutrition
| Independent variables (n = 216) | CHR (95% CI) | AHR (95% CI) |
|---|---|---|
| Age group of child | ||
| Younger than 24 months | 1r | 1r |
| Older than 24 months | 1.58 (1.47–2.17)* | 1.17 (0.82–1.66) |
| Sex of child | ||
| Male | 1r | – |
| Female | 0.86 (0.89–1.18) | – |
| Maternal education | ||
| Primary school | 1r | 1r |
| No education | 0.51 (0.37–0.72)* | 0.54 (0.38–0.78)* |
| Paternal education | ||
| Primary school | 1r | – |
| No education | 0.34 (0.95–1.88) | – |
| Ecological zone | ||
| Midland | 1r | 1r |
| Highland | 0.62 (0.44–0.86)* | 0.57 (0.41–0.81)* |
| Household food security status | ||
| Mild insecurity | 1r | 1r |
| Moderate insecurity | 0.77 (0.45–1.32) | 0.68 (0.39–1.71) |
| Severe insecurity | 0.43 (0.26–.71)* | 0.47(0.28–0.79)* |
| Household wealth index | ||
| Richest | 1r | |
| Richer | 0.92 (0.56–1.51) | – |
| Middle | 0.89 (0.54–1.47) | – |
| Poorer | 1.02 (0.63–1.67) | – |
| Poorest | 0.80 (0.50–1.32) | – |
| Two-way distance from health post | ||
| More than an hour | 0.59(0.43–0.81)* | 0.69 (0.50–0.96)* |
| Less than an hour | 1r | 1r |
| Dietary diversity score | ||
| Optimal | 1r | – |
| Suboptimal | 0.86 (0.50–1.50) | – |
| Nutritional diagnosis at admission | ||
| Marasmus | 0.18 (0.12–0.27)* | 0.30 (0.18–0.51)* |
| Kwashiorkor | 1r | 1r |
| Diarrhea during admission or follow-up | ||
| Yes | 0.40 (0.29–0.55)* | 0.63 (0.42–0.91)* |
| No | 1r | 1r |
| Cough during admission or follow-up | ||
| Yes | 1r | 1r |
| No | 0.55 (0.35–0.86)* | 0.65 (0.41–1.03) |
| Fever during admission or follow-up | ||
| Yes | 1r | – |
| No | 0.90 (0.66–1.21) | – |
| RUTF sharing practice | ||
| Yes | 0.56 (0.40–0.77)* | 0.53 (0.32–0.88)* |
| No | 1r | 1r |
| RUTF selling practice | ||
| Yes | 0.56 (0.38–0.85)* | 0.61 (0.29–8.33) |
| No | 1r | 1r |
| Maternal perceived on the severity of SAM | ||
| Not aware of any consequences | 1r | 1r |
| Death and disability | 1.42 (0.82–2.49) | 1.17 (0.66–2.08) |
| Disability | 1.11(0.63–1.55) | 1.03 (0.58–1.84) |
| Death | 4.10 (2.32–6.87)* | 2.45 (1.35–4.46)* |
* Significant association at p-value of 0.05
1r Set as a reference group
CHR crude hazard ratio, AHR adjusted hazard ratio, CI confidence interval
In the proximate model six variables emerged statistically significant. SAM cases who were admitted on the basis of low MUAC were less likely to recover than those admitted based on presence of edema. Children who had diarrhoea at baseline or during follow-up had 37% reduced probability of recovery than their counterparts. The chance of recovery was almost reduced by half among children whose RUTF was shared with other household members. Furthermore, among children whose caregivers were aware that SAM can be fatal, the chance of recovery was nearly two times higher (Table 3).
Discussion
This study assessed the recovery rate of severely malnourished infants and children aged 6–59 months managed on outpatient basis for a maximum duration of eight weeks. The recovery rate was about 80%. Time-to-recovery was negatively affected by manifold factors including maternal illiteracy, severe household food insecurity, inaccessibility of OTP sites, diarrhoea co-morbidity, practice of RUTF sharing within the household and being diagnosed with Marasmus on admission.
The level of recovery reported in this study is above the minimum 75% threshold set by the SPHERE standard [20]. Previous studies in Ethiopia that evaluated the recovery rate in the OTP program provided at health center and/or health post levels came up with assorted figures. Studies that evaluated OTP provided at health post level in North Western Ethiopia and Wolita determined 78 and 65% recovery rates, respectively [11, 20]. Studies in Jimma (45%), South Wollo (82%) and Southern Ethiopia (87%) that evaluated health center level OTP care reported varying recovery rates [12, 16, 21]. Studies in Tigray region (62%) and Kemba district (68%) based on combination of cases treated at health center and health post levels reported relatively lower success rates [14, 15]. The observed discrepancies could be due to diverse reasons including variation in timing and season in which the studies were conducted, level of maturity of the OTP program in the study settings and dissimilarity in the underlying determinants of malnutrition across the localities.
The mean weight gain rate of 5.4 g/kg/day observed was less than the expected rate based on the SPHERE standard which recommends weight gain rate greater than 8 g/kg/day [20]. Many studies conducted in Ethiopia [11, 13, 21] and in East Africa [22, 23] consistently documented substandard rate of weight gain among SAM cases managed through the OTP. A study in Southern Ethiopia found 4.5 and 3.5 g/kg/day weight gain in Kwashiorkor and Marasmic cases, respectively [11]. Another study from Wolaita zone, Southern Ethiopia determined 4.2 g/kg/day rate [13].
Overall the median time-to-recovery was about 5 weeks (36 days). It is within the range of the acceptable minimum international standard (< 6 weeks) [24] and it is well within the Ethiopian protocol for management of SAM which allows children to stay under treatment up to 8 weeks [4, 8]. Previous studies in Ethiopia reported comparable figures. In a study based on OTP care provided at health post level in Wolita zone, the time to recovery was 35 days for children with kwashiorkor and 49 days for children with marasmus [13]. A similar study North Western Ethiopia reported 48 days [11]. According to a study in Jimma that evaluated health center level OTP care, the median time to recovery was 38 days [16]. In a similar study in Southern Ethiopia the time ranged from 21to 25 days depending on the type of malnutrition [12]. In studies conducted in Tigray region and Kemba district the time to recovery was approximately 49 days [14, 15].
In the current study, maternal literacy is identified as a significant predictor of recovery of children from SAM. Previous studies which were based on secondary medical records review have not explored such relationship as socio-demographic information is not registered in the standard OTP cards. However, the finding is plausible and anticipatable as maternal literacy is likely to be associated with better child feeding and caring practice, adoption of nutritional advices and superior household economic status.
The study found that children from severely food insecure households showed lesser propensity of recovery from SAM. Better household food security level is likely to promote the recovery of children through enabling caregivers to adhere to the nutritional advices provided by health workers. Household food insecurity may also prompt mothers to share RUTF with other members of the household.
Conversely, the study did not witness significant association between household wealth index and time-to-recovery from SAM. The unexpected finding can be due to the fact that wealth was quantified using a relative scale as measurement based on actual household income was not feasible. Relative scale might not have adequate discriminating power to disaggregate a population with homogeneous economic status. The adjustment of household food insecurity for household wealth index might have also caused underestimation of the association as the two variables are likely to be correlated to each other.
In the study area the majority of the caregivers travelled for less than an hour walking distance to receive the OTP service. The finding is compatible with the standard of CMAM programs which aims to provide services within 3 h walking distance [20]. However, significantly lower time-to-recovery rate was observed among caregivers who travel more than one hour to receive the service. Caregivers who have limited access to OTP sites may only decide to bring their child to treatment when the malnutrition gets severe and this may compromise the treatment success rate. The finding may also indicate that making the OTP service even more accessible to the community may help to improve the treatment outcome.
Cases with oedematous malnutrition demonstrated a better propensity of recovery than severely wasted children. This is parallel to the findings of the two studies conducted in Ethiopia [11, 12]. A study from North Western Ethiopia concluded that the median time-to-recovery was 35 days for children with Kwashiorkor and 49 days for children with Marasmus [11]. While the study in Southern Ethiopia reported 25 and 21 days average length of stay in the treatment respectively for the two groups [12]. A study that evaluated the outcome of inpatient SAM cases concluded the same [25]. The observed variation can likely be due to differences in the severity of wasting between the two groups on enrolment. Further, Kwash cases, unlike Marasmic children, are discharged from the OTP upon the resolution of oedema regardless of their weight gain progress [15].
We observed that diarrhoea complicates SAM almost in two-fifth of the children. Further, diarrhoea while on treatment is a negative predictor of time-to-recovery from SAM. Diarrhoea is known to be more frequent in SAM cases due to the systematic immune-suppression effect and loss of the intestinal mucosal barrier due to malnutrition [26]. A study conducted in Tigray Northern Ethiopia also found slower recovery rates among children who had diarrhoea during the course of SAM [15]. Diarrhoea may retard weight gain during treatment through compromising absorption and increasing biological demand for nutrients. Other co-symptoms like anorexia and vomiting may also limit recovery from SAM.
Nearly one-in-three of the caregivers with SAM children reported the practice of sharing RUTF with other members of the household. Even the figure is likely to be underestimated due to social desirability bias. Our study also found that the practice as a significant negative predictor of time-to-recovery from SAM. Previous studies have also concluded the same [16, 24, 27, 28].
The findings of the study have to be interpreted inconsideration of its strength and limitation. Unlike most of the earlier studies that evaluated OTP programs, our study employed a prospective cohort design and used primary data. Accordingly we have been able to evaluate the significance of many socio-demographic, economic and nutritional factors which are otherwise unavailable in medical records.
Conversely, we could have underestimated the significance of the OTP program as the study was conducted during the lean season of the locality. As dietary diversity and household food insecurity were assessed retrospectively, recall errors cannot be fully excluded. Further, responses related to RUTF sharing and selling behaviours might have been underestimated due to social desirability bias. In addition, baseline wasting status, which can be an important predictor of the treatment outcome in children with non-oedematous malnutrition was not statistically adjusted, and this may have limited the comprehensiveness of the model and caused residual bias in the analysis. Due to the observational design of the study, confounding from unmeasured variables (e.g. vaccination history, birth weight) cannot be entirely excluded.
Conclusion
The OTP program in Shebedino exceeds the international minimum standard for recovery in most of the indicators. The median time-to-recover from SAM was 36 days. Factors that prolong time-to-recovery include maternal illiteracy, severe household food insecurity, practice of RUTF sharing within the household, lack of access to the OTP sites, being Marasmic at enrolment and diarrhoea co-morbidity during admission or follow-up.
The CMAM program in the district or in other similar settings can enhance treatment outcome by improving access to OTP sites, discouraging of RUTF sharing behaviour and giving close follow-up to children with diarrhoea co-morbidity.
Additional file
Questionnaire used for data collection. (DOCX 31 kb)
Acknowledgements
We are grateful to the Hawassa University for funding the study. We also like to sincerely acknowledge the mothers/caregivers of the children, the data collectors, the health extension workers and the district health offices.
Funding
The financial support for this study came from Hawassa University, Ethiopia.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AHR
Adjusted Hazard Ratio
- CHD
Community Health Day
- CI
Confidence Intervals
- CPHM
Cox Proportional Hazard Model
- DD
Dietary Diversity
- DHS
Demographic and Health Survey
- EOS
Enhanced Outreach Strategy
- HEWs
Health Extension Workers
- HFIAS
Household Food Insecurity Access Scale
- IQR
Inter Quartile Range
- IRB
Institutional Review Board
- MUAC
Middle-upper Arm Circumference
- OTP
Outpatient Therapeutic Program
- RUTF
Ready-to-use Therapeutic Food
- SAM
Severe Acute Malnutrition
- SD
Standard Deviation
- SPSS
Statistical Package for Social Sciences
- WHO
World Health Organization
Authors’ contributions
GT conceived and designed the study; collected analysed and interpreted the data; and drafted the manuscript. SG and TB participated in the designing of the study and supervised of the fieldwork and the data analysis. All the authors critically reviewed the manuscript for intellectual content and approved the final draft.
Ethics approval and consent to participate
Ethical clearance was obtained from the Institutional Review Board (IRB) of Hawassa University, College of Medicine and Health Sciences. Data were collected after securing informed verbal consent from the caregivers of the children. Verbal consent, instead of written consent, was preferred because most of the study respondents were not literate. The same was approved by the IRB that reviewed the protocol of the study.
Consent for publication
Consent to publish the data was taken from the parents of the study participants.
Competing interests
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Genene Teshome, Phone: +251910827762, Email: teshomegenene2008@gmail.com.
Tafese Bosha, Phone: +251931529578, Email: tafese.bosha@gmail.com.
Samson Gebremedhin, Phone: +251916822815, Email: samsongmgs@yahoo.com.
References
- 1.Development Initiatives. Development Initiatives Global nutrition report 2017: nourishing the SDGs. Bristol, UK: development Initiatives; 2017.
- 2.Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–451. doi: 10.1016/S0140-6736(13)60937-X. [DOI] [PubMed] [Google Scholar]
- 3.Central Statistical Agency [Ethiopia] and the DHS Program Ethiopia: Demographic and health survey 2016. Rockville, Maryland and Addis Ababa: CSA and ICF; 2017.
- 4.Federal Ministry of Health [Ethiopia] Protocol for the management of severe acute malnutrition. Addis Ababa: MoH; 2007. [Google Scholar]
- 5.UNICEF, WHO and World Bank. Levels and trends in child malnutrition: UNICEF/WHO/World Bank Group joint child malnutrition estimates, 2017. Accessed from: http://www.who.int/nutgrowthdb/jme_brochoure2017.pdf?ua=1. Accessed: 17 Dec 2017.
- 6.ACF International. Taking action nutrition for survival, growth and development, 2010. Accessed from: https://reliefweb.int/report/ethiopia/unicef-ethiopia-humanitarian-situation-report-7-reporting-period-november-december. Accessed 17 Dec 2017.
- 7.UNICEF. UNICEF Ethiopia humanitarian situation report #7 – reporting period: November–December 2015. Accessed from: http://www.who.int/pmnch/topics/child/acf_whitepaper.pdf. Accessed 17 Dec 2017.
- 8.WHO, WFP, UNSCN, UNICEF. Community-based management of severe acute malnutrition: A joint statement Accessed from: https://www.unscn.org/files/Statements/Community_Based__Management_of_Severe_Acute_Malnutrition.pdf. Accessed 17 Dec 2017.
- 9.Collins S. Treating severe acute malnutrition seriously. Arch Dis Child. 2007;92(5):453–461. doi: 10.1136/adc.2006.098327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.World Health Organization . Guideline: updates on the management of severe acute malnutrition in infants and children. Geneva: WHO; 2013. [PubMed] [Google Scholar]
- 11.Mengesha MM, Deyessa N, Tegegne SB, Dessie Y. Treatment outcome and factors affecting time to recovery in children with severe acute malnutrition treated at outpatient therapeutic care program. Glob Health Action. 2016;9. 10.3402/gha.v9.30704. [DOI] [PMC free article] [PubMed]
- 12.Teferi E, Lera M, Sita S, Bogale Z, Datiko DG, Yassin MA. Treatment outcome of children with severe acute malnutrition admitted to therapeutic feeding centers in southern region of Ethiopia. Ethiop J Health Dev. 2010;24(3):234–238. [Google Scholar]
- 13.Kabalo MY, Seifu CN. Treatment outcomes of severe acute malnutrition in children treated within outpatient therapeutic program (OTP) at Wolaita zone, southern Ethiopia: retrospective cross-sectional study. J Health Popul Nutr. 2017;36(7). 10.1186/s41043-017-0083-3.. [DOI] [PMC free article] [PubMed]
- 14.Shanka NA, Lemma S, Abyu DM. Recovery rate and determinants in treatment of children with severe acute malnutrition using outpatient therapeutic feeding program in Kamba District, South West Ethiopia. J Nutr Dis Ther. 2015;5:155. doi: 10.4172/2161-0509.1000155. [DOI] [Google Scholar]
- 15.Yebyo HG, Kendall C, Nigusse D, Lemma W. Outpatient therapeutic feeding program outcomes and determinants in treatment of severe acute malnutrition in Tigray, northern Ethiopia: a retrospective cohort study. PLoS One. 2013;8(6):e65840. doi: 10.1371/journal.pone.0065840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Eklund M, Girma T. Effectiveness of integrated outpatient care of severe acute malnutrition in Ethiopia, 2008. Field Exchange Issue. 34, October 2008. https://www.ennonline.net/fex/34/effectiveness. Accessed 23 Dec 2015.
- 17.The DHS Program. DHS model questionnaires Accessed from: https://dhsprogram.com/What-We-Do/Survey-Types/DHS-Questionnaires.cfm. Accessed 17 Dec 2017.
- 18.World Health Organization . Indicators for assessing infant and young child feeding practices: definitions. Geneva: WHO; 2008. [Google Scholar]
- 19.Coates J, Swindale A, Bilinsky P. Household food insecurity access scale (HFIAS) for measurement of food access: Indicator guide. New York: FANTA; 2007. [Google Scholar]
- 20.The SPHERE. Project. Humanitarian charter and minimum standards in disaster response. 3. Geneva: The SPHERE Project; 2004. [DOI] [PubMed] [Google Scholar]
- 21.Asres DT, Prasad RP, Ayele TA. Recovery time and associated factors of severe acute malnutrition among children in Bahir Dar city, Northwest Ethiopia: an institution based retrospective cohort study. BMC Nutrition. 2018;4:17. [DOI] [PMC free article] [PubMed]
- 22.Mbaya D, Bitok LK, Karani AK, Osano B, Habtu M. Outcomes of severely malnourished children aged 6-59 months on outpatient management program in Kitui County hospital, Kenya. Open J Pediatr. 2015;5:326–333. doi: 10.4236/ojped.2015.54049. [DOI] [Google Scholar]
- 23.Nalwa GM. Outcomes of Severely Malnourished Children Aged 6–60 months on Outpatient Management in Nairobi, Master’s Thesis, University of Nairobi, 2012.
- 24.Collins S, Dent N, Binns B, Bahwere P, Sadler K, Hallam A. Management of severe acute malnutrition in children. Lancet. 2006;368(9551):1992–2000. doi: 10.1016/S0140-6736(06)69443-9. [DOI] [PubMed] [Google Scholar]
- 25.Gebremichael DY. Predictors of nutritional recovery time and survival status among children with severe acute malnutrition who have been managed in therapeutic feeding centers, southern Ethiopia: retrospective cohort study. BMC Public Health. 2015;15:1267. doi: 10.1186/s12889-015-2593-5.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Talbert A, Thuo N, Karisa J, Chesaro C, Ohuma E, Ignas J, et al. Diarrhoea complicating severe acute malnutrition in Kenyan children: a prospective descriptive study of risk factors and outcome. PLoS One. 2012;7(6):e38321. doi: 10.1371/journal.pone.0038321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Collins S, Sadler K. Outpatient care for severely malnourished children in emergency relief program. A retrospective Cohort study. Lancet. 2002;360:24–30. doi: 10.1016/S0140-6736(02)11770-3. [DOI] [PubMed] [Google Scholar]
- 28.Manary MJ, Ndkeha M, Ashorn P, Maleta K, Briend A. Home based therapy for severe malnutrition with ready-to-use food. Arch Dis Child. 2004;89:55–56. doi: 10.1136/adc.2003.034306. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Questionnaire used for data collection. (DOCX 31 kb)
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.