

Abstract
Digital health interventions (DHIs) have been emerging in the last decade. Due to their interdisciplinary nature, DHIs are guided and influenced by theories (eg, behavioral theories, behavior change technologies, and persuasive technology) from different research communities. However, DHIs are always coded using various taxonomies and reported in insufficient perspectives. This inconsistency and incomprehensiveness will cause difficulty in conducting systematic reviews and sharing contributions among communities. Therefore, based on existing related work, we propose a holistic framework that embeds behavioral theories, behavior change technique taxonomy, and persuasive system design principles. Including four development steps, two toolboxes, and one workflow, our framework aims to guide DHI developers to design, evaluate, and report their work in a formative and comprehensive way.
Keywords: behavior change technique, behavior change technique taxonomy, digital health interventions, persuasive technology, persuasive system design
Introduction
According to the County Health Rankings [1], variation in health can be accounted for by health behaviors (30%), clinical care (20%), social and economic factors (40%), and physical environment (10%). Increasing evidence shows that lifestyle-related behaviors such as diet, exercise, sleeping, emotion, and smoking play an essential role in people’s health. Chronic diseases caused by unhealthy behaviors and habits are among the leading causes of mortality [2]. Some of the chronic diseases, for example, type 2 diabetes, could be lifelong and bring a heavy burden to the patients and their family. The only way to prevent many chronic diseases is to change unhealthy lifestyles, for example, diet and physical activity.
With the potential for low cost and high scalability for chronic disease prevention, in the past decade, digital health interventions (DHIs) have been widely discussed by government stakeholders, clinicians, and researchers [3]. Designing and deploying DHIs are challenging due to the complexity of human behavior, which could be affected by individuals’ motivation, emotion, ability, social environment, and physical environment. Therefore, DHI design could accordingly require theories and practice from several disciplines, including phycology, public health, behavioral science, human-computer interaction, and so on. The interdisciplinary nature of DHIs calls for a comprehensive framework to guide the development, evaluation, and report.
As DHIs are expected to change human behavior, behavioral theories can serve as the development foundation. It has been shown that theory-based behavior change interventions are more effective than others [4,5]. Nevertheless, behavioral theories could also be ignored [6] or misused [7]. Although behavioral theories allow the explanation and prediction of behavior, they lack the guidance for translating into operational techniques.
The behavior change technique (BCT) taxonomy [8] and persuasive system design (PSD) principles [9] are two widely used taxonomies in DHI research [10-13]. These taxonomies not only inform DHI design but also enable precise reporting, which is favored by systematic reviewers. Although derived from different philosophies, BCTs and PSDs have some common elements. However, they are used separately in many DHI studies. To benefit from both, we combined the BCT taxonomy and PSD principles into a more comprehensive taxonomy in the light of the behavioral intervention technology (BIT) model [14].
In this paper, we aim to put the puzzles together and build a holistic framework to aid DHI researchers to design, evaluate, and report their studies. In short, our contributions include the following:
We provide a holistic framework that allows DHI developers to design, evaluate, and report their work in a formative and comprehensive way.
We propose the DHI taxonomy including the strategy part and the characteristic part. Our DHI taxonomy enables more comprehensive description of DHIs.
We classify PSD principles into two parts: strategies and characteristics. We then combine the BCT taxonomy and PSD principles (strategies related) into our DHI taxonomy (the strategy part).
We integrate the intervention characteristics from the BIT model with the ones we extract from PSD principles (characteristic related) as the characteristic part of the DHI taxonomy.
Related Work
Summary
As this paper is for DHI developers from different communities, it is necessary to clarify the terms and our scope before we present the related work. Digital health or electronic health (eHealth) is the umbrella concept referring to the use of information and communication technologies for health [15]. According to the World Health Organization, DHIs cover systematic functionalities to support clients, health care providers, health system or resource managers, and data services [3]. In this paper, however, we limit our scope to the DHIs aiming to change users’ lifestyle behavior (eg, food intake, physical activity, and smoking) using digital technology to prevent or manage health problems.
CeHRes Roadmap
In 2011, a holistic framework (ie, the CeHRes Roadmap) was proposed to improve the uptake and impact of eHealth technology. The CeHRes Roadmap was built upon 16 existing frameworks via a systematic review and emphasized the importance of holism [16]. Human characteristics, socioeconomic and cultural environments, and technology are closely connected to affect human behavior. Therefore, developers should always keep these holistic factors in mind when building eHealth technologies. Within this framework, the CeHRes Roadmap was illustrated as a practical guideline to help plan, coordinate, and execute the participatory development process of eHealth technologies. The CeHRes Roadmap consists of five steps, namely, contextual inquiry, value specification, design, operationalization, and summative evaluation, which integrate persuasive technology design, human-centered design, and business modeling. Although the CeHRes Roadmap integrates behavioral theories as its foundation, it does not explicitly show how to apply them in the intervention design. Besides, the CeHRes Roadmap does not adopt any persuasive technology taxonomy.
Behavioral Intervention Technology Model
In 2014, Mohr and colleagues proposed the BIT model, aiming to support the translation of treatment and intervention aims into an implementable treatment model [14]. The BIT model includes a theoretical phase followed by an instantiation phase. The theoretical phase consists of the intervention aims and behavior change strategies, whereas the instantiation level consists of intervention elements, characteristics, and workflow. Thus, the BIT model can serve as a supplement to the CeHRes Roadmap. However, the BIT model only provides some examples in each component. For example, behavior change strategies include education, goal setting, monitoring, feedback, and motivation enhancement. As the author mentioned, the BIT model is a simplification and should be modified and elaborated to fit users’ needs [14]. In this paper, we will adjust and elaborate the BIT model to fit into our holistic framework.
Integrate, Design, Assess, and Share Framework
In 2016, Mummah et al proposed IDEAS (Integrate, Design, Assess, and Share) as a framework and toolkit of strategies for the development of DHIs [17]. IDEAS was built on three essential components: behavioral theory, design thinking, and evaluation and dissemination. The IDEAS framework emphasizes the importance of behavioral theories and introduces the taxonomy of BCTs. However, the BCT taxonomy is regarded as an alternative to using behavioral theories to identify target constructs in interventions. In our holistic framework, we suggest using both of them as two necessary steps because they correspond to the intervention aims and strategies, respectively.
Behavioral Theories
All the three reviewed works above mention behavioral theories, but only IDEAS explicitly integrates behavioral theories into the steps of the development process. Behavioral theories refer to the social-psychological theories of behavior change, which explain and predict human behavior. As depicted by Sutton [18], each of the behavioral theories specifies a small number of cognitive and affective factors as the proximal determinants of behavior (see Figure 1). These factors are called constructs in behavioral science [7]. We will use this term to refer to the fundamental components of behavioral theories in the rest of the paper.
Figure 1.
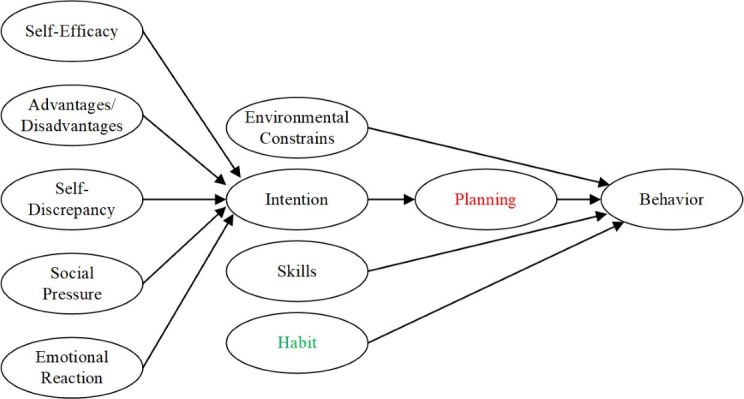
Our hypothesized continuum model of behavior change.
Glanz et al [19] illustrated the most frequently used behavioral theories published before 2010: the social cognitive theory (SCT) [20], the transtheoretical model of behavior change (TTM) [21], the health belief model (HBM) [22], and the theory of planned behavior (TPB) [23]. Davis et al [24] also identified 82 behavioral theories, among which the most frequently used theories are TTM, TPB, SCT, the information- motivation-behavioral skills model, HBM, the self-determination theory [25], the health action process approach (HAPA) [26], and the social learning theory [27]. Based on different assumptions of human behavior, these behavioral theories can be grouped into continuum theories and stage theories [28].
Continuum theories assume people’s behavior is caused by a set of variables, for example, intention and skills. Except for TTM, all other mentioned theories fall into this group. Based on the behavioral model integrating several existing ones [28], we present a hypothesized continuum model as shown in Figure 1. The constructs in black are borrowed from the integrated behavioral model in [28]. Planning (shown in red in Figure 1) is specified as a mediator of the intention-behavior relationship in HAPA [26,29,30]. The habit (shown in green in Figure 1) has been found to moderate the effects of planning on behavior change [31].
Stage theories assume people change their behavior in a process including several stages. The factors pushing people from one stage to the next are believed to be different. Therefore, the strategies at each state should be adapted accordingly. For example, Figure 2 shows the stages and strategies of TTM, which is adapted from [32]. This model divides the behavior change process into five stages, namely precontemplation, contemplation, preparation, action, and maintenance and relapse prevention. Depending on the stage of change, different strategies could be applied accordingly to make the intervention effective.
Figure 2.
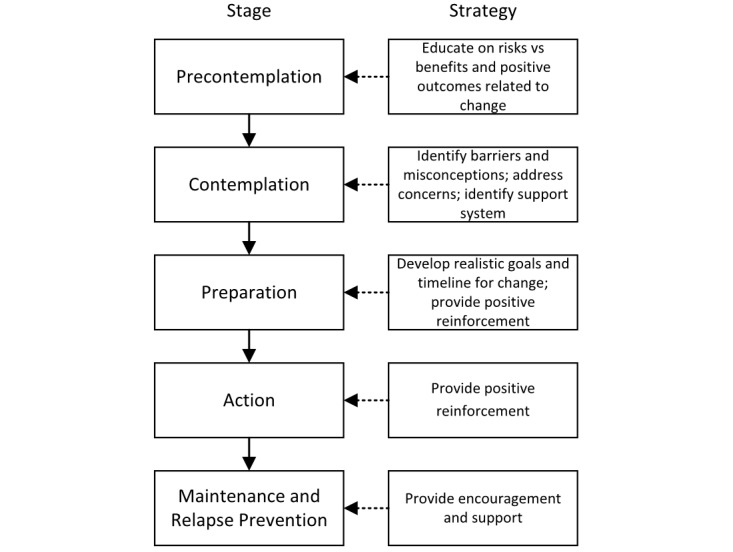
The transtheoretical model of behavior change.
Behavioral theories provide a toolbox to understand human behavior and explain the rationale behind interventions. However, their shortcomings should be noted before they are used. Hekler and colleagues [7] have pointed out three shortcomings of behavioral theories: (1) most behavioral theories explain only a small portion of variance in the outcomes they are trying to account for, (2) many behavioral theories, in their current form, are not falsifiable, and (3) there is a fragmentation and an overabundance of different theories. Therefore, DHI developers should not be limited to behavioral theories. With the emergence of DHIs, the existing behavioral theories can be further evaluated and improved [33]. Here we list some guidelines when using specific behavioral theories: [34] and [35] for the SCT, [36] for the HBM, [37] for the TPB, and [38] for the HAPA.
Digital Health Intervention Taxonomy
While behavioral theories can predict and explain human behavior, there is a gap between theories and operational interventions. Will self-monitoring increase self-efficacy for promoting physical activity? Will information about health consequences affect perceived advantages or disadvantages? Due to the high complexity of human behavior and health, one DHI may involve several techniques. The lack of a consistent taxonomy of DHIs will lead to poor replicability and low comparability of the results from related studies. Although there exists taxonomies to bridge the theory-intervention gap, the use of different taxonomies still hinders the understanding and contribution among communities. Therefore, we present the DHI taxonomy, a unified taxonomy taking advantage of two widely used taxonomies (the BCT taxonomy and PSD principles) in light of the BIT model.
BCTs are defined as observable, replicable, and irreducible components of an intervention designed to change behavior [8,39], for example, self-monitoring or goal setting. Abraham and Michie developed a taxonomy of BCTs that identified 22 BCTs and 4 BCT packages [8] and was later extended to a taxonomy containing 93 BCTs in 16 groups, called BCT taxonomy (v1) [39]. The BCT taxonomy has been used for informing intervention development and report [40,41] and identifying the effectiveness of BCTs [13,42-44]. It also provides a means to evaluate health and fitness apps [12,45-47] and wearables [48]. From the official website of the BCT taxonomy [49], we found a collection of 405 intervention studies with BCT coding. We show the word cloud of BCTs based on this collection in Multimedia Appendix 1. The top five used or tested BCTs are goal setting (behavior), instruction on how to perform a behavior, problem solving, information about health consequences, and action planning.
In related work, we have introduced the BIT model [14]. In terms of the intervention strategies in the BIT model, only some examples (ie, education, goal setting, monitoring, feedback, and motivation enhancement) were provided. We think the BCT taxonomy can serve as a strategy pool for the BIT model.
Aiming to create a conceptual framework that can be directly applied to persuasive system development, the PSD model describes 28 principles in four categories (supporting primary task, computer-human dialogue, system credibility, and social) as an extension of Fogg’s work on persuasive technology [50]. Table 1 describes the details of PSD principles. We found 16 principles that have the same or similar definitions with counterparts from the BCT taxonomy. For example, self-monitoring appears both in PSD principles and the BCT taxonomy. Tunneling (1.2) in PSD principles has the same meaning as the BCT “4.1 structure on how to perform the behavior” (refer to Multimedia Appendix 2 for more details). There are three PSD principles (ie, cooperation, competition, and recognition) whose counterparts could not be found from the BCT taxonomy; these can serve as a supplement to the BCT taxonomy.
Table 1.
Persuasive system design principles.
| Persuasive system design principlea | Definition | |
| Primary task support | ||
|
|
Reduction (1.1) | System should reduce steps users take when performing target behavior. |
|
|
Tunneling (1.2) | System should guide users in attitude or behavior change process by providing means for action. |
|
|
Tailoring (1.3)b | System should provide tailored info for user groups. |
|
|
Personalization (1.4)b | System should offer personalized content and services for individual users. |
|
|
Self-monitoring (1.5) | System should provide means for users to track their performance or status. |
|
|
Simulation (1.6) | System should provide means for observing link between cause & effect with regard to users’ behavior. |
|
|
Rehearsal (1.7) | System should provide means for rehearsing target behavior. |
| Dialogue support | ||
|
|
Praise (2.1) | System should use praise to provide user feedback based on behaviors. |
|
|
Rewards (2.2) | System should provide virtual rewards for users to give credit for performing target behavior. |
|
|
Reminders (2.3) | System should remind users of their target behavior while using the system. |
|
|
Suggestion (2.4) | System should suggest users carry out behaviors while using the system. |
|
|
Similarity (2.5)b | System should imitate its users in some specific way. |
|
|
Liking (2.6)b | System should have a look & feel that appeals to users. |
|
|
Social role (2.7)b | System should adopt a social role. |
| System credibility support | ||
|
|
Trustworthiness (3.1)b | System should provide info that is truthful, fair & unbiased. |
|
|
Expertise (3.2) | System should provide info showing knowledge, experience & competence. |
|
|
Surface credibility (3.3)b | System should have competent and truthful look & feel. |
|
|
Real-world feel (3.4) | System should provide info of the organization or actual people behind it content & services. |
|
|
Authority (3.5) | System should refer to people in the role of authority. |
|
|
Third-party endorsements (3.6) | System should provide endorsements from external sources. |
|
|
Verifiability (3.7) | System should provide means to verify accuracy of site content via outside sources. |
| Social support | ||
|
|
Social learning (4.1) | System should provide means to observe others performing their target behaviors. |
|
|
Social comparison (4.2) | System should provide means for comparing performance with the performance of others. |
|
|
Normative influence (4.3) | System should provide means for gathering people who have same goal & make them feel norms. |
|
|
Social facilitation (4.4) | System should provide means for discerning others who are performing the behavior. |
|
|
Cooperation (4.5)c | System should provide means for cooperation. |
|
|
Competition (4.6)c | System should provide means for competing with others. |
|
|
Recognition (4.7)c | System should provide public recognition for users who perform their target behavior. |
aThe rest principles have counterparts with the same or similar definitions in the behavior change technique taxonomy.
bThe principles are interventions characteristics.
cThe principles have no counterparts in the behavior change technique taxonomy but can also be regarded as intervention strategies.
Next, we present the diagram of our DHI taxonomy (see Figure 3). The blue part is the strategy part, whereas the green part is the characteristic part. We have just shown its strategy part, which includes 93 (the BCTs from the BCT taxonomy) plus 3 (cooperation, competition, and recognition from PSD principles) strategies. The other part of our DHI taxonomy corresponds to the characteristics. The BIT model described four characteristics (medium, complexity, aesthetics, and personalization). Inspired by the characteristics-related PSD principles (Table 1), we included social role and trustiness, in addition to the mentioned four from the BIT model, into the characteristic part of the DHI taxonomy.
Figure 3.
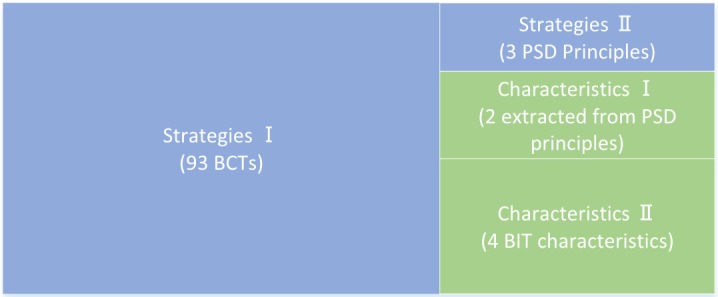
Diagram of our digital health intervention taxonomy. BCT: behavior change technique; BIT: behavioral intervention technology; PSD: persuasive system design.
We divided the PSD principles into two groups. The ones fitting the definition of the BCT were placed in the strategies group, while the others fell into the characteristics group. Personalization is one of the characteristics in the BIT model. We found that tailoring has a very close meaning to personalization according to their definitions in the PSD principles [51], whereas similarity and liking are also in line with the definition of personalization. Therefore, we regard tailoring, similarity and liking the same as personalization. Likewise, trustworthiness, surface credibility, real-world feel, and verifiability were merged to one characteristic as trustiness. By dividing the PSD principles and merging the overlapping principles, we hope our new taxonomy can reduce the confusion and difficulty of coding DHIs [6,10] (see Multimedia Appendix 3 for the complete list of elements in our DHI taxonomy).
The Holistic Framework
The Framework Structure
The proposed holistic framework (see Figure 4) is called TUDER (Targeting, Understanding, Designing, Evaluating and Refining), which consists of four steps, two toolboxes (behavioral theories and the DHIs taxonomy), and a workflow. In each step, going back and updating corresponding information is allowed.
Figure 4.
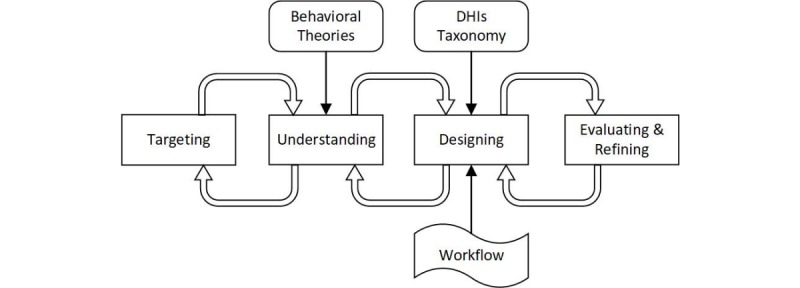
TUDER (Targeting, Understanding, Designing, Evaluating and Refining) diagram. DHI: digital health intervention.
Targeting the User Group, the Health Problem, and the Behavior
The target group, health problem, and behavior define the intervention aim(s). For example, an intervention to promote the use of standing desks (the behavior) to reduce the prolonged sedentary behavior (the behavior) of office workers (the user group) to prevent chronic diseases, such as type 2 diabetes (the health problem) [52]. The intervention designers should explain the relationship between the health problem and the behavior. Scientific evidence provides the rationale. For example, the evidence that sedentary behavior and moderate-to-vigorous physical activity are independently associated with clustered cardiometabolic health supports the development of interventions to reduce office workers’ sedentary behavior [53]. Another example concerns myopia among children. A study showed that the time of outdoor activities was the most significant factor of myopia in 6-year and 7-year-old Chinese children [54]. Therefore, a reasonable intervention to reduce myopia (the health problem) among children (the user group) would be increasing their outdoor activity time (the behavior). Besides the scientific support, another rule concerns the measurability to enable quantitative analysis. The target health problem is not necessarily measurable in an intervention study, while the target behavior must be [55].
Behavioral theories (eg, see Figures 1 and 2) provide DHI developers with a toolbox to understand human behavior. Given the target user group, health problem, and behavior, developers ought to take one behavioral theory or a set of constructs from behavioral theories as the base of intervention design in the following step. We suggest that theory-based interventions should relate their strategies to specific constructs from behavioral theories. For example, an intervention design based on HAPA intended to support action planning (the construct) to reduce users’ sedentary behavior [56]. Therefore, in addition to measuring the sedentary behavior, the constructs in HAPA should also be assessed. When analyzing the intervention effect on action planning, the assessment of action planning is sufficient. However, in the case of analyzing the intervention effect on sedentary behavior, other constructs besides action planning also have to be considered. The participants should be grouped based on the level of their intention in the data analysis. Alternatively, the user group in the previous step can be adjusted to only focus on one user group with a specific level of intention.
Designing the Intervention Strategies, Characteristics, and Workflow
We have included 98 intervention strategies and six characteristics in our DHI taxonomy. DHI developers can select a set of strategies based on their idea and describe the characteristics of their strategies according to the DHI taxonomy. As the context of an intervention may vary over time, the workflow that allows an intervention to be delivered according to time, task, or event would be demanding [14]. The workflow design has been comprehensively illustrated in the BIT model [14] and the just-in-time adaptive intervention framework [57]. From the perspective of implementation difficulty, time-based workflow (eg, an hourly reminder in sedentary behavior interventions [6]) is the easiest. Task-based (eg, a set of interventions delivered to a user sequentially) or event-based (eg, adaptive food recommendation according to a user’s previous meal) workflow requires user data input. Because of the difficulty of acquiring users’ context data, the research on opportune moments for DHIs is still in the early stage [58,59].
Evaluating and Refining the Intervention Design
Intervention evaluation could include usability evolution (regarding human-computer interaction), an effectiveness evaluation (regarding behavior change) corresponding to the uptake and impact of the intervention, respectively [16].
During this step, DHI developers may backtrack to the previous step to adjust the target user group and measurements.
Think-aloud [60] and cognitive walkthrough can be used in the early stage of ideation creation and prototype to identify the usability issues. Then, a pilot study with a small number of participants would be deployed to test the feasibility of the whole study procedure. Because many interventions need field study, the pilot can also help find some unknown issues in real-world use. Finally, heuristic evaluations based on randomized controlled trials [17] or sequential multiple assignment randomized trials [61] have to be conducted to generate powerful results. In our framework, an iterative evaluation and refinement process is adopted. Because evaluation and refinement are always intertwined with each other, we place them in one step in our framework.
Discussion
Principal Findings
We have described TUDER, a holistic framework to guide DHI development. We also provide a checklist for DHI developers, as shown in Figure 5. By completing the checklist and reporting all the details of a DHI study, the data coding work in systematic reviews could be much reduced.
Figure 5.

Checklist for using TUDER (Targeting, Understanding, Designing, Evaluating and Refining).
We have built TUDER based on several existing related works [8,9,14,16,17]. The key contribution of this work is to embed behavioral theories, BCT taxonomy, and PSD principles into a holistic framework. We believe this framework will be beneficial to each of them. This holistic framework and the DHI taxonomy will also enable more research questions. We provide some examples as follows:
What combinations of DHI strategies, characteristics, and workflow work better than others? In [62], a meta-analysis shows several combinations of PSD principles were more effective, for example, tunneling and tailoring, reminders and similarity, and social learning and comparison. With consideration of the characteristics and workflow when coding the interventions, the results of intervention effectiveness analysis may change.
Is the DHI taxonomy able to explain more variance in DHI adherence? Kelders et al [11] systematically reviewed the impact of the PSD principles on adherence to Web-based interventions. Their model explained 55% of the variance in users’ adherence. The DHI taxonomy brings more perspectives to analyze the effects of the components in interventions.
As the TUDER framework is expected to be comprehensive, some parts are simplistic. For example, only a few behavioral theories are discussed. The DHI taxonomy is built upon two existing taxonomies. The DHI developers who are unfamiliar with the BCT taxonomy and PSD principles will find it challenging to use the DHI taxonomy.
Conclusion
This work presented the TUDER framework, containing four steps (targeting, understanding, designing, and evaluating and refining), two toolboxes (behavioral theories and DHI taxonomy), and a workflow. The framework aims to integrate the advantages of behavioral theories, BCT taxonomy, and persuasive technology design principles. Thus, it can help DHI researchers to design, evaluate, and report their studies in a formative and comprehensive way. By using this framework, future systematic reviews could have broader insights into DHI studies. To better bridge the research from different communities, we will continue to test and improve this framework.
Acknowledgments
This work was partially supported by SMARTACT. YW acknowledges the financial support from the China Scholarship Council.
Abbreviations
- BCT
behavior change technique
- BIT
behavioral intervention technology
- DHI
digital health intervention
- eHealth
electronic health
- HAPA
Health Action Process Approach
- HBM
Health Belief Model
- IDEAS
Integrate, Design, Assess, and Share
- PSD
persuasive system design
- SCT
Social Cognitive Theory
- TPB
Theory of Planned Behavior
- TTM
Transtheoretical Model of Behavior Change
- TUDER
Targeting, Understanding, Designing, Evaluating and Refining
Behavior change techniques word cloud.
{kind=link}
Overlap between persuasive system design principles and the behavior change technique taxonomy.
The complete list of elements in our DHI taxonomy.
Footnotes
Conflicts of Interest: None declared.
References
- 1.County Health Rankings & Roadmaps. [2019-01-08]. What is Health? http://www.countyhealthrankings.org/what-is-health .
- 2.US National Center for Health. [2018-11-20]. Leading Causes of Death https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm .
- 3.World Health Organization. [2019-01-08]. Classification of Digital Health Interventions v1.0 https://www.who.int/reproductivehealth/topics/mhealth/en/
- 4.Davis Rachel, Campbell Rona, Hildon Zoe, Hobbs Lorna, Michie Susan. Theories of behaviour and behaviour change across the social and behavioural sciences: a scoping review. Health Psychol Rev. 2015;9(3):323–44. doi: 10.1080/17437199.2014.941722. http://europepmc.org/abstract/MED/25104107 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Glanz Karen, Bishop Donald B. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health. 2010;31:399–418. doi: 10.1146/annurev.publhealth.012809.103604. doi: 10.1146/annurev.publhealth.012809.103604. [DOI] [PubMed] [Google Scholar]
- 6.Wang Yunlong, Wu Lingdan, Lange Jan-Philipp, Fadhil Ahmed, Reiterer Harald. Persuasive technology in reducing prolonged sedentary behavior at work: A systematic review. Smart Health. 2018 Jun;7-8:19–30. doi: 10.1016/j.smhl.2018.05.002. doi: 10.1016/j.smhl.2018.05.002. [DOI] [Google Scholar]
- 7.Hekler E. Klasnja P. Froehlich JE. Buman MP Mind the Theoretical Gap: Interpreting, Using, and Developing Behavioral Theory in HCI Research. CHI 2013; 2013; Paris, France. 2013. [DOI] [Google Scholar]
- 8.Abraham Charles, Michie Susan. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008 May;27(3):379–87. doi: 10.1037/0278-6133.27.3.379. doi: 10.1037/0278-6133.27.3.379.2008-08834-010 [DOI] [PubMed] [Google Scholar]
- 9.Oinas-Kukkonen H. Persuasive Systems Design: Key Issues, Process Model, and System Features. CAIS. 2009;24 doi: 10.17705/1CAIS.02428. [DOI] [Google Scholar]
- 10.Geuens Jonas, Swinnen Thijs Willem, Westhovens Rene, de Vlam Kurt, Geurts Luc, Vanden Abeele Vero. A Review of Persuasive Principles in Mobile Apps for Chronic Arthritis Patients: Opportunities for Improvement. JMIR Mhealth Uhealth. 2016 Oct 13;4(4):e118. doi: 10.2196/mhealth.6286. http://mhealth.jmir.org/2016/4/e118/ v4i4e118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kelders Saskia M, Kok Robin N, Ossebaard Hans C, Van Gemert-Pijnen Julia E W C. Persuasive system design does matter: a systematic review of adherence to web-based interventions. J Med Internet Res. 2012 Nov 14;14(6):e152. doi: 10.2196/jmir.2104. http://www.jmir.org/2012/6/e152/ v14i6e152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Middelweerd Anouk, Mollee Julia S, van der Wal C Natalie, Brug Johannes, Te Velde Saskia J. Apps to promote physical activity among adults: a review and content analysis. Int J Behav Nutr Phys Act. 2014 Jul 25;11:97. doi: 10.1186/s12966-014-0097-9. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-014-0097-9 .s12966-014-0097-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Olander Ellinor K, Fletcher Helen, Williams Stefanie, Atkinson Lou, Turner Andrew, French David P. What are the most effective techniques in changing obese individuals' physical activity self-efficacy and behaviour: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2013 Mar 03;10:29. doi: 10.1186/1479-5868-10-29. https://ijbnpa.biomedcentral.com/articles/10.1186/1479-5868-10-29 .1479-5868-10-29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mohr David C, Schueller Stephen M, Montague Enid, Burns Michelle Nicole, Rashidi Parisa. The behavioral intervention technology model: an integrated conceptual and technological framework for eHealth and mHealth interventions. J Med Internet Res. 2014 Jun 05;16(6):e146. doi: 10.2196/jmir.3077. http://www.jmir.org/2014/6/e146/ v16i6e146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.World Health Organization. [2019-01-08]. eHealth https://www.who.int/ehealth/about/en/
- 16.van Gemert-Pijnen Julia E W C, Nijland Nicol, van Limburg Maarten, Ossebaard Hans C, Kelders Saskia M, Eysenbach Gunther, Seydel Erwin R. A holistic framework to improve the uptake and impact of eHealth technologies. J Med Internet Res. 2011 Dec 05;13(4):e111. doi: 10.2196/jmir.1672. http://www.jmir.org/2011/4/e111/ v13i4e111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mummah Sarah Ann, Robinson Thomas N, King Abby C, Gardner Christopher D, Sutton Stephen. IDEAS (Integrate, Design, Assess, and Share): A Framework and Toolkit of Strategies for the Development of More Effective Digital Interventions to Change Health Behavior. J Med Internet Res. 2016 Dec 16;18(12):e317. doi: 10.2196/jmir.5927. http://www.jmir.org/2016/12/e317/ v18i12e317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sutton SR. International Encyclopedia of the Social & Behavioral Sciences. London: Elsevier; 2002. Health Behavior: Psychosocial Theories; p. 10. [Google Scholar]
- 19.Glanz Karen, Rimer Barbara K, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. San Francisco: Jossey-Bass; 2008. [Google Scholar]
- 20.Bandura Albert. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review. 1977;84(2):191–215. doi: 10.1037/0033-295X.84.2.191. doi: 10.1037/0033-295X.84.2.191. [DOI] [PubMed] [Google Scholar]
- 21.Prochaska J O, Velicer W F. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48. doi: 10.4278/0890-1171-12.1.38. doi: 10.4278/0890-1171-12.1.38. [DOI] [PubMed] [Google Scholar]
- 22.Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the Health Belief Model. Health Educ Q. 1988;15(2):175–83. doi: 10.1177/109019818801500203. [DOI] [PubMed] [Google Scholar]
- 23.Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes. 1991 Dec;50(2):179–211. doi: 10.1016/0749-5978(91)90020-T. doi: 10.1016/0749-5978(91)90020-T. [DOI] [Google Scholar]
- 24.Davis Rachel, Campbell Rona, Hildon Zoe, Hobbs Lorna, Michie Susan. Theories of behaviour and behaviour change across the social and behavioural sciences: a scoping review. Health Psychol Rev. 2015;9(3):323–44. doi: 10.1080/17437199.2014.941722. http://europepmc.org/abstract/MED/25104107 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000 Jan;55(1):68–78. doi: 10.1037//0003-066x.55.1.68. [DOI] [PubMed] [Google Scholar]
- 26.Schwarzer R. Modeling Health Behavior Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Applied Psychology. 2008 Jan;57(1):1–29. doi: 10.1111/j.1464-0597.2007.00325.x. doi: 10.1111/j.1464-0597.2007.00325.x. [DOI] [Google Scholar]
- 27.Miller NE, Dollard J. Journal of Communication. New Haven, CT: Yale University Press; 1941. Social learning and imitation. [Google Scholar]
- 28.Conner M, Norman P. Predicting Health Behaviour. London: Open University Press; 2005. [Google Scholar]
- 29.Sutton S. How does the Health Action Process Approach (HAPA) Bridge the Intention–Behavior Gap? An Examination of the Model's Causal Structure. Applied Psychology. 2008 Jan;57(1):66–74. doi: 10.1111/j.1464-0597.2007.00326.x. doi: 10.1111/j.1464-0597.2007.00326.x. [DOI] [Google Scholar]
- 30.Schwarzer R. Health Action Process Approach (HAPA) as a Theoretical Framework to Understand Behavior Change. AP. 2016 Dec 05;30(121):119. doi: 10.15517/ap.v30i121.23458. doi: 10.15517/ap.v30i121.23458. [DOI] [Google Scholar]
- 31.Maher Jaclyn P, Conroy David E. Habit strength moderates the effects of daily action planning prompts on physical activity but not sedentary behavior. J Sport Exerc Psychol. 2015 Feb;37(1):97–107. doi: 10.1123/jsep.2014-0258. [DOI] [PubMed] [Google Scholar]
- 32.Adult Meducation. [2019-01-08]. Facilitating Behavior Change http://adultmeducation.com/FacilitatingBehaviorChange.html .
- 33.Klasnja Predrag, Hekler Eric B, Korinek Elizabeth V, Harlow John, Mishra Sonali R. Toward Usable Evidence: Optimizing Knowledge Accumulation in HCI Research on Health Behavior Change. Proc SIGCHI Conf Hum Factor Comput Syst; CHI 2017; May 6-11, 2017; Colorado. 2017. May, pp. 3071–3082. http://europepmc.org/abstract/MED/30272059 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mark Conner, Paul Norman. Predicting health behaviour: Research and practice with social cognition models. Safety Science. 2005;24 doi: 10.1016/S0925-7535(97)81483-X. doi: 10.1016/S0925-7535(97)81483-X. [DOI] [Google Scholar]
- 35.Maberry Steven L. Physical Activity Promotion from the Social Cognitive Theory Perspective: An Examination of Mobile Fitness Apps. 2016. [2019-01-08]. https://digitalcommons.lsu.edu/gradschool_dissertations/3803/
- 36.Champion VL. Instrument development for health belief model constructs. ANS Adv Nurs Sci. 1984 Apr;6(3):73–85. doi: 10.1097/00012272-198404000-00011. [DOI] [PubMed] [Google Scholar]
- 37.Ajzen Icek. Constructing a TpB Questionnaire: Conceptual and Methodological Considerations. 2006. http://citeseerx.ist.psu.edu/viewdoc/summary;jsessionid=011E42C7D4396A688EA04E1D0DFBF6F0?doi=10.1.1.601.956 .
- 38.Schwarzer Ralf. The Health Action Process Approach. http://www.hapa-model.de .
- 39.Michie Susan, Richardson Michelle, Johnston Marie, Abraham Charles, Francis Jill, Hardeman Wendy, Eccles Martin P, Cane James, Wood Caroline E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013 Aug;46(1):81–95. doi: 10.1007/s12160-013-9486-6. doi: 10.1007/s12160-013-9486-6. [DOI] [PubMed] [Google Scholar]
- 40.Mummah Sarah A, King Abby C, Gardner Christopher D, Sutton Stephen. Iterative development of Vegethon: a theory-based mobile app intervention to increase vegetable consumption. Int J Behav Nutr Phys Act. 2016 Aug 08;13:90. doi: 10.1186/s12966-016-0400-z. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-016-0400-z .10.1186/s12966-016-0400-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mummah Sarah Ann, Mathur Maya, King Abby C, Gardner Christopher D, Sutton Stephen. Mobile Technology for Vegetable Consumption: A Randomized Controlled Pilot Study in Overweight Adults. JMIR Mhealth Uhealth. 2016 May 18;4(2):e51. doi: 10.2196/mhealth.5146. http://mhealth.jmir.org/2016/2/e51/ v4i2e51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Dombrowski Su, Sniehotta Ff, Avenell A, Johnston M, MacLennan G, Araújo-Soares V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: a systematic review. Health Psychology Review. 2012 Mar;6(1):7–32. doi: 10.1080/17437199.2010.513298. doi: 10.1080/17437199.2010.513298. [DOI] [Google Scholar]
- 43.Gardner Benjamin, Smith Lee, Lorencatto Fabiana, Hamer Mark, Biddle Stuart J H. How to reduce sitting time? A review of behaviour change strategies used in sedentary behaviour reduction interventions among adults. Health Psychol Rev. 2016;10(1):89–112. doi: 10.1080/17437199.2015.1082146. http://europepmc.org/abstract/MED/26315814 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Michie Susan, Abraham Charles, Whittington Craig, McAteer John, Gupta Sunjai. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009 Nov;28(6):690–701. doi: 10.1037/a0016136. doi: 10.1037/a0016136.2009-20990-006 [DOI] [PubMed] [Google Scholar]
- 45.Conroy David E, Yang Chih-Hsiang, Maher Jaclyn P. Behavior change techniques in top-ranked mobile apps for physical activity. Am J Prev Med. 2014 Jun;46(6):649–52. doi: 10.1016/j.amepre.2014.01.010. doi: 10.1016/j.amepre.2014.01.010.S0749-3797(14)00040-3 [DOI] [PubMed] [Google Scholar]
- 46.Crane David, Garnett Claire, Brown James, West Robert, Michie Susan. Behavior change techniques in popular alcohol reduction apps: content analysis. J Med Internet Res. 2015 May 14;17(5):e118. doi: 10.2196/jmir.4060. http://www.jmir.org/2015/5/e118/ v17i5e118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Direito Artur, Dale Leila Pfaeffli, Shields Emma, Dobson Rosie, Whittaker Robyn, Maddison Ralph. Do physical activity and dietary smartphone applications incorporate evidence-based behaviour change techniques? BMC Public Health. 2014 Jun 25;14:646. doi: 10.1186/1471-2458-14-646. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-14-646 .1471-2458-14-646 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lyons Elizabeth J, Lewis Zakkoyya H, Mayrsohn Brian G, Rowland Jennifer L. Behavior change techniques implemented in electronic lifestyle activity monitors: a systematic content analysis. J Med Internet Res. 2014 Aug 15;16(8):e192. doi: 10.2196/jmir.3469. http://www.jmir.org/2014/8/e192/ v16i8e192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.BCT Taxonomy v1. [2019-01-08]. Intervention Collection http://www.bct-taxonomy.com/interventions .
- 50.Fogg BJ. Persuasive Technology: Using Computers to Change What We Think and Do. Burlington: Morgan Kaufmann; 2002. [Google Scholar]
- 51.Oinas-Kukkonen H. A foundation for the study of behavior change support systems. Pers Ubiquit Comput. 2012 Jul 19;17(6):1223–1235. doi: 10.1007/s00779-012-0591-5. doi: 10.1007/s00779-012-0591-5. [DOI] [Google Scholar]
- 52.De Cocker Katrien, Veldeman Charlene, De Bacquer Dirk, Braeckman Lutgart, Owen Neville, Cardon Greet, De Bourdeaudhuij Ilse. Acceptability and feasibility of potential intervention strategies for influencing sedentary time at work: focus group interviews in executives and employees. Int J Behav Nutr Phys Act. 2015 Feb 18;12:22. doi: 10.1186/s12966-015-0177-5. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-015-0177-5 .10.1186/s12966-015-0177-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Knaeps Sara, Bourgois Jan G, Charlier Ruben, Mertens Evelien, Lefevre Johan, Wijndaele Katrien. Ten-year change in sedentary behaviour, moderate-to-vigorous physical activity, cardiorespiratory fitness and cardiometabolic risk: independent associations and mediation analysis. Br J Sports Med. 2018 Aug;52(16):1063–1068. doi: 10.1136/bjsports-2016-096083. http://bjsm.bmj.com/cgi/pmidlookup?view=long&pmid=27491779 .bjsports-2016-096083 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Rose Kathryn A, Morgan Ian G, Smith Wayne, Burlutsky George, Mitchell Paul, Saw Seang-Mei. Myopia, lifestyle, and schooling in students of Chinese ethnicity in Singapore and Sydney. Arch Ophthalmol. 2008 Apr;126(4):527–30. doi: 10.1001/archopht.126.4.527. doi: 10.1001/archopht.126.4.527.126/4/527 [DOI] [PubMed] [Google Scholar]
- 55.Stephen. W. Designing For Behavior Change: Applying Psychology And Behavioral Economics. Sebastopol, California: O'Reilly Media; 2018. [Google Scholar]
- 56.Yunlong Wang, Ahmed Fadhil, Harald Reiterer. Supporting Action Planning for Sedentary Behavior Change by Visualizing Personal Mobility Patterns on Smartphone. PervasiveHealth '18; May 21- May 24, 2018; New York, USA. 2018. [Google Scholar]
- 57.Nahum-Shani Inbal, Smith Shawna N, Spring Bonnie J, Collins Linda M, Witkiewitz Katie, Tewari Ambuj, Murphy Susan A. Just-in-Time Adaptive Interventions (JITAIs) in Mobile Health: Key Components and Design Principles for Ongoing Health Behavior Support. Ann Behav Med. 2018 May 18;52(6):446–462. doi: 10.1007/s12160-016-9830-8.10.1007/s12160-016-9830-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Akane S, Paul J, Mary C. 2017. Designing Opportune Stress Intervention Delivery Timing using Multi-modal Data; 2017 Seventh International Conference on Affective Computing and Intelligent Interaction (ACII); 23-26 Oct. 2017; San Antonio, TX, USA. 2017. [Google Scholar]
- 59.Wang Yunlong, Duan Le, Mueller Jens, Butscher Simon, Reiterer Harald. “Fingerprints”: Detecting meaningful moments for mobile health intervention. The 18th International Conference on Human-Computer Interaction with Mobile Devices and Services Adjunct, MobileHCI 2016; 6TH - 9TH, 2016; Florence, Italy. 2016. [DOI] [Google Scholar]
- 60.Joe Jonathan, Chaudhuri Shomir, Le Thai, Thompson Hilaire, Demiris George. The use of think-aloud and instant data analysis in evaluation research: Exemplar and lessons learned. J Biomed Inform. 2015 Aug;56:284–91. doi: 10.1016/j.jbi.2015.06.001. https://linkinghub.elsevier.com/retrieve/pii/S1532-0464(15)00111-2 .S1532-0464(15)00111-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Collins Linda M, Murphy Susan A, Strecher Victor. The multiphase optimization strategy (MOST) and the sequential multiple assignment randomized trial (SMART): new methods for more potent eHealth interventions. Am J Prev Med. 2007 May;32(5 Suppl):S112–8. doi: 10.1016/j.amepre.2007.01.022. http://europepmc.org/abstract/MED/17466815 .S0749-3797(07)00051-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Wildeboer Gina, Kelders Saskia M, van Gemert-Pijnen Julia E W C. The relationship between persuasive technology principles, adherence and effect of web-Based interventions for mental health: A meta-analysis. Int J Med Inform. 2016 Dec;96:71–85. doi: 10.1016/j.ijmedinf.2016.04.005. doi: 10.1016/j.ijmedinf.2016.04.005.S1386-5056(16)30054-5 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Behavior change techniques word cloud.
Overlap between persuasive system design principles and the behavior change technique taxonomy.
The complete list of elements in our DHI taxonomy.