

β‐propeller protein‐associated neurodegeneration (BPAN), formerly referred to as static encephalopathy of childhood with neurodegeneration in adulthood, is a recently established subtype of neurodegeneration with brain iron accumulation.1 Developmental delay and epilepsy are present from early childhood and are usually stable until adolescence. In adulthood, these patients present with rapidly progressive dystonia‐parkinsonism and cognitive decline. In addition to iron accumulation in the substanta nigra (SN) and globus pallidus (GP), BPAN shows a unique pattern on T1‐weighted brain MRI in the form of hyperintensity of the SN with a central band of hypointensity.1 WDR45, a core autophagy gene located on the X chromosome, was identified as the causative gene of BPAN.2, 3 Given that most cases of BPAN have been diagnosed in adolescence or adulthood, symptoms during childhood are reviewed retrospectively, except in the case of one report of a 14‐year‐old girl.4 Here, we present the first video report of a child with BPAN before onset of neurological deterioration.
The patient, a 9‐year‐old girl, showed global developmental delay from early infancy. She controlled her head at 5 months of age and walked with support at 18 months, but did not acquire independent gait. She did not develop language. At 8 years, her developmental age, as estimated using the Kyoto Scale of Psychological Development 2001, was 6 months. She has had atonic seizures and complex partial seizures since 15 months of age. EEG showed frequent spikes in the bilateral frontal areas. Seizures were intractable by antiepileptic drugs, such as valproate, carbamazepine, clonazepam, clobazam, lamotorigine, levetiracetam, and bromide, and thus total callosotomy was performed at the age of 9 years, which resulted in marked reduction in seizure frequency. Although brain MRI at age 12 months revealed no abnormalities (Fig. 1A–C), perioperative brain MRI suggested iron accumulation in the bilateral SN and GP (Fig. 1D,E). T1‐weighted images revealed mild hyperintensity of the SN, but the central hypointense band was not evident (Fig. 1F). The patient was referred to our department for further investigation. She showed severe mental retardation, but had an interest in her surroundings and showed intense eye contact. Stereotypic hand movements, such as wringing and clapping, were notable (see Video). However, purposeful hand movements, such as reaching and grasping objects, were preserved. She showed truncal hypotonia with limb spasticity and gait ataxia, but dystonia‐parkinsonism was not observed. Given that her clinicoradiological features suggested the diagnosis of BPAN, we conducted WDR45 gene analysis. Direct sequencing detected a novel heterozygous nonsense mutation: c.1056C>G (p.Tyr352*), which was not found in ESP 6500 exomes or among our 575 control exomes.
Figure 1.
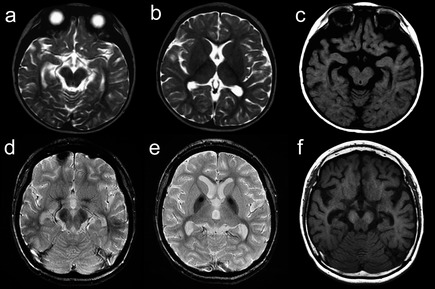
Brain MRI. Brain MRI at 12 months of age showed no abnormality in T2‐weighted (A and B) and T1‐weighted (C) images. At 9 years of age, T2*‐weighted images showed hypointensity in the SN (D) and in the anterocentral regions of the GP (E). Whereas the substantia nigra showed mild hyperintensity in T1‐weighted images, the central hypointensity band was not demonstrated (F).
This is the youngest patient with BPAN to have been reported on (although we reported this case as the youngest patient with BPAN, a 6‐year‐old girl with BPAN was reported during review process).5 It is important to delineate childhood features for earlier detection because elucidation of autophagic machinery in BPAN may lead to future therapeutic intervention to prevent neurological deterioration in adulthood.
It has been reported that patients with BPAN often show a Rett‐like phenotype.1, 4 Our patient showed mid‐line stereotypic hand movements, but, interestingly, purposeful hand movements were spared, as reported in another patient with this disorder.6 Preserved purposeful hand movements may be the “red flag” for BPAN in patients with Rett‐like syndrome. Other Rett‐like symptoms in our patient were intense eye gaze and small hands and feet, whereas she did not have microcephaly, breathing disturbance, sleep disorders, bruxism, peripheral vasomotor disturbances, and scoliosis.7 Future studies may clarify the common pathophysiology in BPAN and Rett syndrome, including that of hand stereotypes.
Similar to findings described in previous reports,1, 4 brain MRI during early childhood was unremarkable. This patient demonstrates that brain iron accumulation in BPAN can develop as early as 9 years of age. In contrast, the characteristic T1‐weighted MRI pattern in adult BPAN, hyperintensity with the central hypointense band in the SN, was not demonstrated, which probably appears later and in association with neurodegeneration.
Author Roles
(1) Research Project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript Preparation: A. Writing of the First Draft, B. Review and Critique.
S.U.: 1C, 3A
H.S.: 1C
S.K.: 1C, 3B
Y.N.: 1C
N.M.: 1C
Disclosures
Funding Sources and Conflicts of Interest: The authors report no sources of funding and no conflicts of interest.
Financial Disclosures for previous 12 months: H.S. is funded by a Grant‐in‐Aid for Scientific Research (B) from the Japan Society for the Promotion of Science and a research grant from the Takeda Science Foundation. N.M. is supported by grants from a Grant‐in‐Aid for Scientific Research (A) from the Japan Society for the Promotion of Science, the Takeda Science Foundation, the fund for Creation of Innovation Centers for Advanced Interdisciplinary Research Areas Program in the Project for Developing Innovation Systems, the Strategic Research Program for Brain Sciences, and a Grant‐in‐Aid for Scientific Research on Innovative Areas (Transcription Cycle) from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
Supporting information
A video accompanying this article is available in the supporting information here.
Video. The patient constantly shows midline stereotypic hand movements, but purposeful hand movements, such as reaching and grasping objects, can be observed. Also noted is intense eye gaze. Although she can stand and walk with support, she shows gait ataxia.
Appendix Although we reported this case as the youngest patient with BPAN to have been reported on, a 6‐year‐old girl with BPAN was reported during review process (Okamoto N et al. Am J Med Genet Part A 2014;164A:3095–3099).
Acknowledgments
The authors thank Drs. Michiharu Morino and Hiroshi Ozawa for providing the patient's clinical information.
Relevant disclosures and conflicts of interest are listed at the end of this article.
References
- 1. Hayflick SJ, Kruer MC, Gregory A, et al. Beta‐propeller protein‐associated neurodegeneration: a new X‐linked dominant disorder with brain iron accumulation. Brain 2013;136:1708–1717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Haack TB, Hogarth P, Kruer MC, et al. Exome sequencing reveals de novo WDR45 mutations causing a phenotypically distinct, X‐linked dominant form of NBIA. Am J Hum Genet 2012;91:1144–1149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Saitsu H, Nishimura T, Muramatsu K, et al. De novo mutations in the autophagy gene WDR45 cause static encephalopathy of childhood with neurodegeneration in adulthood. Nat Genet 2013;45:445–449. [DOI] [PubMed] [Google Scholar]
- 4. Ohba C, Nabatame S, Iijima Y, et al. De novo WDR45 mutation in a patient showing clinically Rett syndrome with childhood iron deposition in brain. J Hum Genet 2014;59:292–295. [DOI] [PubMed] [Google Scholar]
- 5. Okamoto N, Ikeda T, Hasegawa T, et al. Early manifestations of BPAN in a pediatric patient. Am J Med Genet Part A 2014;164A:3095–3099. [DOI] [PubMed] [Google Scholar]
- 6. Kasai‐Yoshida E, Kumada S, Yagishita A, et al. First video report of static encephalopathy of childhood with neurodegeneration in adulthood. Mov Disord 2013;28:397–399. [DOI] [PubMed] [Google Scholar]
- 7. Neul JL, Kaufmann WE, Glaze DG, et al. Rett syndrome: revised diagnostic criteria and nomenclature. Ann Neurol 2010;68:944–950. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
A video accompanying this article is available in the supporting information here.
Video. The patient constantly shows midline stereotypic hand movements, but purposeful hand movements, such as reaching and grasping objects, can be observed. Also noted is intense eye gaze. Although she can stand and walk with support, she shows gait ataxia.
Appendix Although we reported this case as the youngest patient with BPAN to have been reported on, a 6‐year‐old girl with BPAN was reported during review process (Okamoto N et al. Am J Med Genet Part A 2014;164A:3095–3099).