

Abstract
Background
General health checks are common elements of health care in some countries. They aim to detect disease and risk factors for disease with the purpose of reducing morbidity and mortality. Most of the commonly used individual screening tests offered in general health checks have been incompletely studied. Also, screening leads to increased use of diagnostic and therapeutic interventions, which can be harmful as well as beneficial. It is therefore important to assess whether general health checks do more good than harm. This is the first update of the review published in 2012.
Objectives
To quantify the benefits and harms of general health checks.
Search methods
We searched CENTRAL, MEDLINE, Embase, two other databases and two trials registers on 31 January 2018. Two review authors independently screened titles and abstracts, assessed papers for eligibility and read reference lists. One review author used citation tracking (Web of Knowledge) and asked trial authors about additional studies.
Selection criteria
We included randomised trials comparing health checks with no health checks in adults unselected for disease or risk factors. We did not include geriatric trials. We defined health checks as screening for more than one disease or risk factor in more than one organ system.
Data collection and analysis
Two review authors independently extracted data and assessed the risk of bias in the trials. We contacted trial authors for additional outcomes or trial details when necessary. When possible, we analysed the results with a random‐effects model meta‐analysis; otherwise, we did a narrative synthesis.
Main results
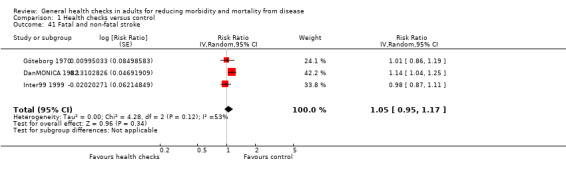
We included 17 trials, 15 of which reported outcome data (251,891 participants). Risk of bias was generally low for our primary outcomes. Health checks have little or no effect on total mortality (risk ratio (RR) 1.00, 95% confidence interval (CI) 0.97 to 1.03; 11 trials; 233,298 participants and 21,535 deaths; high‐certainty evidence, I2 = 0%), or cancer mortality (RR 1.01, 95% CI 0.92 to 1.12; 8 trials; 139,290 participants and 3663 deaths; high‐certainty evidence, I2 = 33%), and probably have little or no effect on cardiovascular mortality (RR 1.05, 95% CI 0.94 to 1.16; 9 trials; 170,227 participants and 6237 deaths; moderate‐certainty evidence; I2 = 65%). Health checks have little or no effect on fatal and non‐fatal ischaemic heart disease (RR 0.98, 95% CI 0.94 to 1.03; 4 trials; 164,881 persons, 10,325 events; high‐certainty evidence; I2 = 11%), and probably have little or no effect on fatal and non‐fatal stroke (RR 1.05 95% CI 0.95 to 1.17; 3 trials; 107,421 persons, 4543 events; moderate‐certainty evidence, I2 = 53%).
Authors' conclusions
General health checks are unlikely to be beneficial.
Plain language summary
General health checks for reducing illness and mortality
What is the aim of this review?
The aim of this Cochrane Review was to find out if general health checks reduce illness and deaths. This is an update of a previous Cochrane Review.
Key messages
Systematic offers of health checks are unlikely to be beneficial and may lead to unnecessary tests and treatments.
What was studied in the review?
General health checks involve multiple tests in a person who does not feel ill. The purpose is to find disease early, prevent disease from developing, or provide reassurance. Health checks are a common element of health care in some countries. Experience from screening programmes for individual diseases have shown that the benefits may be smaller than expected and the harms greater. We identified and analysed all randomised trials that compared invitations for one or more health checks for the general public with no invitations. We analysed the effect on illness and the risk of death, as well as other outcomes that reflect illness, for example, hospitalisation and absence from work.
What are the main results of the review?
We found 17 randomised trials that had compared a group of adults offered general health checks to a group not offered health checks.
Fifteen trials reported results and included 251,891 participants. Eleven of these trials had studied the risk of death, and included 233,298 participants and assessed 21,535 deaths. This is an unusually large amount of data in healthcare research, which allowed us to draw our main conclusions with a high degree of certainty. Health checks have little or no effect on the risk of death from any cause (high‐certainty evidence), or on the risk of death from cancer (high‐certainty evidence), and probably have little or no effect on the risk of death from cardiovascular causes (moderate‐certainty evidence). Likewise, health checks have little or no effect on heart disease (high‐certainty evidence) and probably have little or no effect on stroke (moderate‐certainty evidence).
We propose that one reason for the apparent lack of effect may be that primary care physicians already identify and intervene when they suspect a patient to be at high risk of developing disease when they see them for other reasons. Also, those at high risk of developing disease may not attend general health checks when invited or may not follow suggested tests and treatments.
How up to date is the review?
The review authors searched for studies published up to 31 January 2018.
Summary of findings
Summary of findings for the main comparison. General health checks versus usual care.
| General health checks for reducing morbidity and mortality from disease | |||||
|
Patient or population: general adult populations (geriatric trials not included) Setting: general practice or medical/research centre (Europe and USA) Intervention: one or more general health checks (screening by any healthcare provider for more than one disease or risk factor in more than one organ system using more than one test) Comparison: no health checks | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Certainty of the evidence (GRADE) | |
| Assumed riska | Corresponding risk | ||||
| Without health checks | With health checks | ||||
|
Total mortality Follow‐up: 4‐30 years |
68 per 1000 | 68 per 1000 (66 to 70) | RR 1.00 (0.97 to 1.03) | 233,298 (11) | ⊕⊕⊕⊕ high |
|
Cancer mortality Follow‐up: 4‐22 years |
26 per 1000 | 26 per 1000 (24 to 29) | RR 1.01 (0.92 to 1.12) | 139,290 (8) | ⊕⊕⊕⊕ high |
|
Cardiovascular mortality Follow‐up: 4‐30 years |
32 per 1000 | 34 per 1000 (30 to 37) | RR 1.05 (0.94 to 1.16) | 170,227 (9) | ⊕⊕⊕⊝b moderate |
|
Fatal and non‐fatal ischaemic heart disease Follow‐up: 4‐30 years |
66 per 1000 | 65 per 1000 (62 to 68) | RR 0.98 (0.94 to 1.03) | 164,881 (4) | ⊕⊕⊕⊕ high |
|
Fatal and non‐fatal stroke Follow‐up: 4‐30 years |
29 per 1000 | 30 per 1000 (28 to 34) | RR 1.05 (0.95 to 1.17) | 107,421 (3) | ⊕⊕⊕⊝c moderate |
| *The basis for the assumed risk is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio | |||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aSome trials used skewed randomisation in age and sex strata, giving unbalanced baselines (accounted for in the analysis estimates used). For this reason, control‐group event rates are somewhat misleading. The risk without the intervention is based on the median event rate in intervention and control groups combined. The corresponding risk with the intervention (and the 95% confidence interval for the difference), is based on the overall relative effect (and its 95% confidence interval).
bDowngraded due to serious inconsistency. Substantial unexplained heterogeneity in results (I2 = 65%)
cDowngraded due to serious inconsistency. Substantial heterogeneity in results (I2 = 53%)
Background
Description of the condition
General health checks are common elements of health care in some countries (Han 1997; Holland 2009), sometimes as systematic national programmes (Nakao 2018; Robson 2016). The evolution of medicine in the latter half of the 20th century has led to a great increase in diagnostic methods and increased expectations that many diseases can be prevented or discovered before there is irreversible damage.
Description of the intervention
General health checks involve a contact between a health professional and a person that is not motivated by symptoms, and where several screening tests are performed to assess general health. The purpose is to prevent future illness through earlier detection of disease or risk factors, or to provide reassurance. The terminology is confusing. Multiphasic screening, periodic health examination, annual physicals, and preventive health checks are examples of terms used to describe the intervention. Some studies investigated the effect of a single health check and some examined the effect of consecutive checks, and the diagnostic tests included vary considerably. We use the broad term 'general health check', which is frequently used by lay people and in advertising.
Few of the screening tests commonly included in general health checks have been evaluated according to accepted criteria, that is, in high‐quality randomised trials (UK National Screening Committee 2010). Whilst the benefits and harms of treatments for conditions such as hypertension and diabetes have been extensively studied in randomised trials, screening asymptomatic people for these conditions has been studied very little (Piper 2015; Selph 2015). Assessing cardiovascular risk with a risk score is common in health checks, but it is unclear whether it helps (Karmali 2017). When screening for individual conditions has been studied in randomised trials, the conclusions have varied. For example, screening for prostate cancer likely does not reduce disease‐specific mortality but has important harms (Ilic 2013; Martin 2018), whereas testing for faecal occult blood reduces colorectal cancer mortality, though at the cost of a large number of invasive examinations in healthy people (Holme 2013).
Health checks may be offered systematically to the general population as part of a national policy or private health insurance, or employers may offer them to their employees. They may also be purchased by the individual from commercial providers or provided by general practitioners. Health checks may be quite comprehensive and use advanced technologies, such as computed tomography or magnetic resonance imaging, although these interventions are not recommended for health checks because of unproven benefit and risk of harms (FDA 2018).
Some general health checks include a conversation with a health professional, possibly a questionnaire, and sometimes also a physical examination by a doctor. In essence these are screening tests, although a conversation may not be perceived as such. Lifestyle interventions are also frequently administered during a health check, for example, advice on diet and smoking. This is not screening but behavioural intervention, and appears to be of varying value. For example, systematic reviews have not shown a value for multiple risk factor interventions in general populations (Ebrahim 2011). There may be a small effect of modification of dietary fat intake, but the results are not clear (Hooper 2011; Hooper 2015). However, simple advice on quitting smoking has been shown to have an effect (Stead 2013).
Importantly, primary care physicians sometimes advise health checks or selected screening tests for patients that they think might benefit from them when they see the patients for other reasons. Such clinically motivated testing is often considered an integral part of primary care practice and the effects of systematic health checks are measured as an addition to this practice.
How the intervention might work
General health checks are expected to reduce morbidity and mortality through earlier detection and treatment of diseases and risk factors for diseases. For example, early detection of hypertension can lead to reductions in morbidity and mortality through treatment. Screening may detect precursors to disease, for example, colorectal adenomas or cervical dysplasia, the treatment of which may prevent cancer from developing. Also, identification of signs or symptoms of manifest disease that the person had not deemed important may be beneficial. Counselling on diet, weight and smoking may also be of value. Healthy people may feel reassured, which could decrease worry. The preventive nature of general health checks implies that most effects would be expected to have a latency of several years.
Screening healthy people can also be harmful. While we cannot be certain that screening leads to benefit, all medical interventions can lead to harm. A well‐known example is overdiagnosis of latent cancers or carcinoma in situ, which might not have progressed to become symptomatic or might have regressed spontaneously (Welch 2004). Furthermore, false‐positive test results can lead to unnecessary invasive diagnostic tests that may cause harm, and drug treatment of people with risk factors such as high cholesterol and elevated blood glucose can have adverse effects. False‐positive test results may cause unnecessary worry (Brewer 2007), and false‐negative results may lead to a false sense of security and delay medical attention when needed. Further, being labelled as having a disease, or even just as being at increased risk of getting a disease, may negatively affect healthy peoples' views of themselves (Barger 2006; Hamer 2010; Haynes 1978). It may also make it more difficult to obtain life and health insurance in some countries. Last but not least, there is a financial cost for patients and society in identifying and treating risk factors and diseases that might never have manifested themselves as illness or shortened life.
Why it is important to do this review
General health checks are mixtures of screening tests, few of which have been adequately studied, and it is not clear whether they do more good than harm. Systematic reviews of health checks have not found effects on morbidity and mortality, but some have found effects on surrogate outcomes such as blood pressure and cholesterol (Dyakova 2016; Krogsbøll 2012; Si 2014). We saw a need for a broad and comprehensive review of the randomised trials, with a focus on clinically important outcomes rather than surrogate outcomes. We chose not to review observational studies because the risk of bias is too great in relation to the expected effect sizes. This is the first update of the review published in 2012 (Krogsbøll 2012).
Objectives
To quantify the benefits and harms of general health checks.
Methods
Criteria for considering studies for this review
Types of studies
Randomised trials of general health checks compared with no health checks. We had no language restrictions. We included trials regardless of funding source.
Types of participants
Inclusion criteria
Adults, regardless of gender and ethnicity. The setting had to be primary care or the community. We included trials regardless of whether they were directed at the general population or a more narrow group, for example employees of a company.
Exclusion criteria
We did not include trials described as specifically targeting older people, or that only included people aged 65 years or more (see Differences between protocol and review). We also excluded trials in populations of people with specific known risk factors or diseases, for example, trials in people with hypertension or ischaemic heart disease.
Types of interventions
Screening for more than one disease or risk factor and in more than one organ system, whether performed only once or repeatedly. This definition excludes trials of screening for single diseases, for example prostate cancer, and trials of single screening tests which may detect more than one disease, for example spirometry.
We accepted trials that included a lifestyle intervention (for example advice on diet, smoking and exercise), in addition to screening, since this is a fairly well‐defined intervention that is often incorporated into health checks.
We included trials regardless of the type of healthcare provider, for example a doctor, nurse, or other health professional.
Types of outcome measures
Some trials and observational studies have investigated the effects of health checks on surrogate outcomes, for example cardiovascular risk factors, health behaviours, or cancer screening rates, and some have found positive effects, albeit generally small. However, there can be serious problems with using surrogate outcomes (Fleming 1996).
First, assessing the effect of changes in a surrogate outcome on morbidity and mortality is difficult and unreliable and requires modelling with assumptions that are difficult to test. There may be latency of effects (Ebrahim 2011), and uncertainty regarding the degree of reversibility of the risk. For example, quitting smoking reduces the risk of coronary heart disease and mortality, but slowly and probably not completely (Ben‐Shlomo 1994; Cook 1986). Also, it is difficult to know to what degree changes in risk factors and behaviours are maintained in the long term. Second, the use of surrogate outcomes disregards the harmful effects of follow‐up diagnostic procedures and treatments. An example is the drug rosiglitazone for diabetes, which reduced the surrogate outcome blood glucose but caused serious heart disease (Lehman 2010; Nissen 2010). This was not recognised in trials using surrogate outcomes only. Third, in order to measure changes in risk factors and health behaviours the participants need to attend a follow‐up session or answer questionnaires. Since it is impossible to blind the intervention group, and since the intervention is often partly behavioural, biased loss to follow‐up is to be expected. For example, people with adverse health behaviours might not feel inclined to confront the researchers again, which could lead to spurious improvements in surrogate outcomes in an available case analysis or a last observation carried forward analysis. Also, the lack of blinding may cause biased reporting of health behaviours.
For these reasons, we focused on outcomes that directly reflect the beneficial and harmful effects of health checks on the health of the participants and that can be reliably ascertained with long follow‐up. We chose total and disease‐specific mortality as our primary outcomes because these are less likely to be biased than other outcomes, are of direct relevance to participants, and capture both beneficial and harmful effects. However, we included some outcomes that are susceptible to attrition bias and reporting bias because they are important and cannot be assessed in other ways, for example self‐reported health and worry.
Primary outcomes
Total mortality
Disease‐specific mortality
Secondary outcomes
Morbidity (e.g. myocardial infarction)
New diagnoses (total and condition‐specific)
Admission to hospital
Disability (preferably patient‐reported)
Worry
Self‐reported health
Number of referrals to specialists
Number of non‐scheduled visits to general practitioners
Number of additional diagnostic procedures due to positive screening tests
New medications prescribed, and frequency and type of surgery
Absence from work
Harms
The main harmful effects of health checks are reflected in the above outcomes. The major harms are overdiagnosis, adverse psychological and behavioural effects, complications related to follow‐up investigations, and unnecessary treatments instigated as a result of overdiagnosis. While diagnostic, preventive and therapeutic activity can lead to improved health, they are also often harmful and should be balanced by reductions in morbidity and mortality to be justified. Estimating overdiagnosis will not be possible for all diseases due to the broad scope of the review and because increased incidence is a goal for some conditions, for example diabetes, but a problem for others, for example prostate cancer. These questions are more appropriately addressed in reviews of screening for individual diseases. However, a quantification of the change in the incidence of individual conditions is still valuable even though it may represent both beneficial and harmful effects. Another possible harm is a negative effect on health behaviours, for example failure to quit smoking due to reassurance of good health. Such effects would also be captured by the chosen outcomes.
Search methods for identification of studies
Electronic searches
The searches were revised relative to the previous version of this review to improve identification of relevant studies. Searches were limited to 2012 onwards to find material published since the date of searches carried out for the previous version of this review.
We searched the following databases on 31 January 2018:
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 12) in the Cochrane Library;
Database of Abstracts of Reviews of Effects (DARE; 2015, Issue 2) in the Cochrane Library;
MEDLINE Ovid (including Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations and Versions; 2012 to 24 January 2018);
Embase Ovid (2012 to 30 January 2018);
CINAHL EBSCO (Cumulative Index to Nursing and Allied Health Literature).
The EPOC Cochrane Information Specialist (CIS) developed the search strategies based on the protocol and the original search. The search strategies are presented in full in Appendix 1.
Searching other resources
Trial Registries
We searched the following resources on 31 January 2018:
International Clinical Trials Registry Platform (ICTRP), Word Health Organization (WHO) www.who.int/ictrp/en/;
ClinicalTrials.gov, US National Institutes of Health (NIH) clinicaltrials.gov.
We searched the reference lists of included studies and used citation tracking (Web of Knowledge) for all articles describing eligible trials. We asked authors of the included studies if they were aware of any other published, unpublished, or ongoing studies that could meet our inclusion criteria.
Data collection and analysis
Selection of studies
Two review authors (LTK and KJJ), independently assessed the potential relevance of all titles and abstracts identified through the searches and assessed full‐text copies of potentially eligible articles. We resolved disagreements discussion, involving the third author (PCG) when necessary. Two review authors (LTK and KJJ) independently searched reference lists, and one review author (LTK), used citation tracking (Web of Knowledge) on included articles.
Data extraction and management
Two authors (LTK and KJJ), independently extracted data from the included trials and entered them into a piloted data extraction form. When relevant information was missing from the reports we contacted the trial authors.
We extracted the following data from all included trials: study design, diagnostic tests used, total study duration, the number of participants allocated to each arm, number lost to follow‐up for each outcome, baseline comparability, setting, age, country, and date of study. We extracted the number of events or rates for mortality, hospitalisation (one or more), surgery, new medications, referrals to specialists and diagnostic procedures required because of positive screening tests, and for the number of physician visits. For ordinal scale outcomes we extracted the mean value; standard deviation; and name, range, and direction of the scale. When these data formats were not available we extracted what was possible to extract, including narrative accounts if the actual numbers were missing.
Assessment of risk of bias in included studies
We used the Cochrane 'Risk of bias' tool (Higgins 2017). The domains formally assessed were: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. We assessed the risk of contamination of the control group under 'Other bias'. We also assessed the randomised groups for baseline comparability.
Measures of treatment effect
For mortality, we used the risk ratio, except in cases where only hazard ratios were available. We treated ranking scales as continuous data when possible. For all measures we used 95% confidence intervals.
Three trials used skewed randomisation in several strata, for example, age and gender, providing intentionally unbalanced baseline characteristics (DanMONICA 1982; Inter99 1999; Stockholm 1969). In one case this was motivated by increased sampling efficiency, as the intervention group was also part of a cohort study (DanMONICA 1982), and in another case the researchers wanted to include more participants in groups judged likely to respond well to a lifestyle intervention (Inter99 1999). In all three cases, the trial authors adjusted for the imbalance using Cox regression. For some of the analyses, we obtained data on participants and events in each stratum and treated these as separate trials, summarising the effect with fixed‐effect meta‐analysis. This provided almost identical results to the published ones.
Unit of analysis issues
For cluster‐randomised trials we preferably used effect estimates and standard errors from analyses that took the clustering into account. When such estimates were not available we disregarded the effect of clustering and investigated the impact of this in a sensitivity analysis.
Dealing with missing data
We preferred data from intention‐to‐treat analyses (ITT). When these were not available, we assessed the possible bias resulting from missing data.
Assessment of heterogeneity
We assessed clinical and methodological differences between trials before doing any meta‐analyses, and we judged whether trials could be pooled. We assessed heterogeneity with the I2 statistic, which describes the variation between trials in relation to the total variation (Higgins 2003).
Assessment of reporting biases
Outcome reporting bias is difficult to assess in these trials but we noted whether the outcomes that we considered important had been reported. When the study design implied that data on other outcomes than the ones reported might have been investigated, we asked the trial authors for further data. In meta‐analyses with more than 10 trials, we made funnel plots.
Data synthesis
As specified in our protocol, we used random‐effects model meta‐analyses. In order to combine as many results as possible, we used the generic inverse variance method available in Review Manager 5 (Review Manager 2014). In some cases effect estimates were reported as hazard ratios, and we combined these with risk ratios in the meta‐analyses. When meta‐analysis was not possible, we did a narrative synthesis.
GRADE and 'Summary of findings' table
For our primary outcomes (total mortality, disease‐specific mortality), and morbidity (fatal and non‐fatal ischaemic heart disease, fatal and non‐fatal stroke), we used GRADE to assess and describe the certainty of evidence, using GRADEpro GDT software (GRADEpro GDT 2015). One review author (LK), assessed the quality of the evidence across all studies contributing to the meta‐analysis for each outcome using the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) as outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2017), using GRADEpro GDT software. Another review author (KJ), checked the assessments; we resolved any disagreements through discussion. We justified decisions to downgrade the quality of studies in the footnotes of the 'Summary of findings' table.
Subgroup analysis and investigation of heterogeneity
We pre‐planned the following subgroup analyses:
only one health check versus several;
physical examination by physician;
interventions that included advice on lifestyle;
age of trial;
geographical location of trial;
high versus low risk of bias;
long versus short follow‐up.
Sensitivity analysis
We decided to include cluster‐randomised trials despite anticipating that we had to ignore the clustering in some cases, and despite the greater risk of unsuccessful randomisation. To investigate the robustness of our results, we pre‐planned a sensitivity analysis excluding cluster‐randomised trials.
Results
Description of studies
Results of the search
The search for this update yielded 4021 records after removal of duplicates. From these, we selected 63 articles for full‐text assessment, plus four identified through other sources. Of these 67 articles, we excluded 56. The remaining 11 articles described four trials; one was new (DanMONICA 1982), one was already included but had new results (Inter99 1999), and two were ongoing trials. We did not identify any additional trials by searching reference lists and through citation tracking. In the previous version of this review, we included 16 trials (Ebeltoft 1992; Family Heart 1990; Göteborg 1963; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; Mankato 1982; New York 1971; Northumberland 1969; OXCHECK 1989; Salt Lake City 1972; South‐East London 1967; Stockholm 1969; Titograd 1971; WHO 1971), but two trials did not report results (New York 1971; Titograd 1971). With one new trial identified (DanMONICA 1982), we therefore had 17 trials in all, and 15 trials with data for our updated analysis (Figure 1).
1.
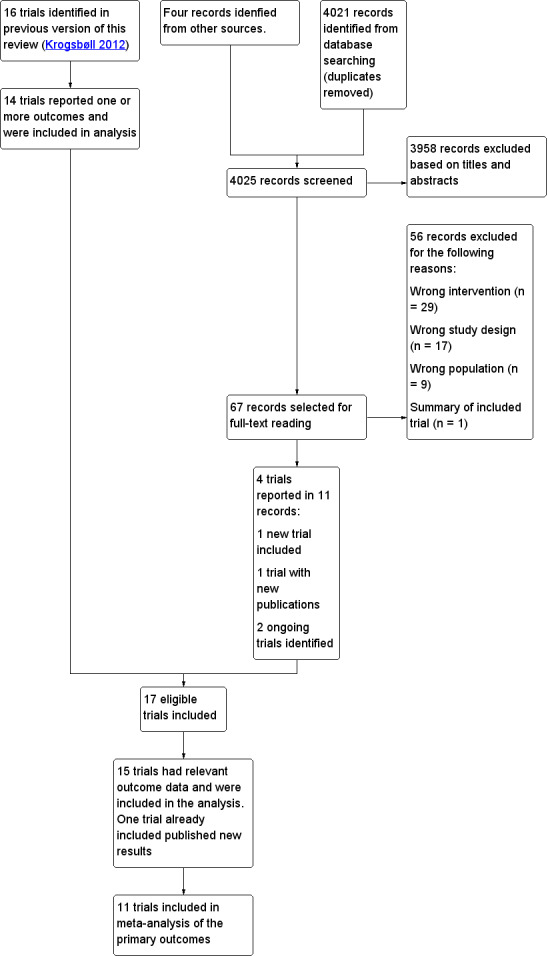
Study flow diagram
Included studies
We included 17 trials, 15 of which reported outcome data.
The 15 trials with data varied in size from 533 randomised participants in Northumberland 1969, to 61,301 in Inter99 1999. The total number of participants was 251,891 with 87,412 allocated to health checks and 164,479 to a control group. Eleven trials with 233,298 participants reported a total of 21,535 deaths (DanMONICA 1982; Ebeltoft 1992; Göteborg 1963; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971). The length of follow‐up for total mortality varied from 4 to 30 years, and it also varied for other outcomes. The trials that did not report mortality were often small (Mankato 1982; Northumberland 1969; Salt Lake City 1972), with the exception of the British Family Heart study (Family Heart 1990), which included 12,924 participants.
The setting was general practice in five trials (Family Heart 1990; Ebeltoft 1992; Northumberland 1969; OXCHECK 1989; South‐East London 1967), medical centre/research centre in nine trials (DanMONICA 1982; Göteborg 1963; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; Mankato 1982; Salt Lake City 1972; Stockholm 1969), and the workplace in one trial (WHO 1971). As per our inclusion criteria, they included people that were not selected for diseases or risk factors. Four trials randomised households or couples (Family Heart 1990; OXCHECK 1989; Salt Lake City 1972; South‐East London 1967), one randomised factories (WHO 1971), and ten randomised participants. Three trials were conducted in the USA (Kaiser Permanente 1965; Mankato 1982; Salt Lake City 1972), and twelve were conducted in Europe (DanMONICA 1982; Ebeltoft 1992; Family Heart 1990; Göteborg 1963; Göteborg 1970; Inter99 1999; Malmö 1969; Northumberland 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971).
The interventions offered can be broadly classified into two categories: screening focused on cardiovascular risk factors with a strong lifestyle intervention component, and broad screenings using many tests (often called multiphasic screening in older publications) but often without an important lifestyle intervention component. The very broad type of screening was mainly seen in trials that started in the 1960s and 1970s. Five trials included screening for cancer. The tests used were chest radiographs (Göteborg 1963; Malmö 1969); chest radiographs and faecal occult blood testing (South‐East London 1967); chest radiographs, mammography and cervical smears (Salt Lake City 1972); and chest radiographs, sigmoidoscopy, mammography and pelvic examinations (Kaiser Permanente 1965). One trial used abdominal ultrasound (DanMONICA 1982). See Table 2 for an overview of the interventions used. Six trials included a physical examination by a physician (Göteborg 1963; Kaiser Permanente 1965; Malmö 1969; Northumberland 1969; South‐East London 1967; Stockholm 1969), while nine trials did not (DanMONICA 1982; Ebeltoft 1992; Family Heart 1990; Göteborg 1970; Inter99 1999; Mankato 1982; OXCHECK 1989; Salt Lake City 1972; WHO 1971).
1. Overview of tests used in the trials.
| Blood pressure | Cholesterol | Height and weight | Risk score | Electrocardiogram | Biochemistry panel | History | Spirometry | Urine analyses | Diabetes | Clinical examination | Vision and/or hearing | Cancer screening | |
| Göteborg 1963 | x | x | x | x | x | Current symptoms, personal and family history | x | Fasting blood sugar | x | x | Chest X‐ray | ||
| Kaiser Permanente 1965 | x | Probably | x | x | x | Current symptoms, personal and family history | x | x | x | x | Chest X‐ray, mammography, pelvic exam, sigmoidoscopy | ||
| South‐East London 1967 | x | Probably | x | x | x | Current symptoms, personal history | x | x | x | Chest X‐ray, faecal occult blood | |||
| Malmö 1969 | x | x | x | x | Haematocrit, triglycerides, cholesterol | Interview and questionnaire, not specified | x | x | x | Chest X‐ray | |||
| Northumberland 1969 | ? | ? | ? | ? | ? | ? | Current symptoms | ? | ? | ? | ? | ? | ? |
| Stockholm 1969 | x | Probably | x | x | Current symptoms, personal history | x | x | ||||||
| Göteborg 1970 | x | x | x | x | Family history | ||||||||
| WHO 1971 | x | x | x | Current symptoms | |||||||||
| Salt Lake City 1972 | x | x | x | x | x | x | x | Chest X‐ray, mammography, cervical smear | |||||
| DanMONICA 1982 | x | x | x | x | Current symptoms, personal and family history | Peak flow | x | Not explicit, but abdominal ultrasound done | |||||
| Mankato 1982 | x | x | x | ||||||||||
| OXCHECK 1989 | x | x | x | Personal and family history | |||||||||
| Family Heart 1990 | x | x | x | Dundee | Personal and family history | Random capillary glucose | |||||||
| Ebeltoft 1992 | x | x | x | Anggaard | x | x | x | x | Non‐fasting blood glucose | x | |||
| Inter99 1999 | x | x | x | PRECARD | x | x | Oral glucose tolerance test |
Not all screening tests used are shown; see Characteristics of included studies for full details. The Kaiser Permanente 1965, South‐East London 1967, and Stockholm 1969 trials did not specify the contents of their biochemical screening. It seems unlikely that cholesterol was not included.
The uptake in the first screening round ranged between 50% (Mankato 1982) and 90% (Ebeltoft 1992) with a median of 80%. Kaiser Permanente 1965 did not use screening rounds at specific intervals but urged the intervention group repeatedly by written invitations and phone calls to utilise a pre‐paid health check.
We chose to label the studies with the year of trial start, instead of year of publication, for the following reasons: 1) year of publication would make the data look much younger than it is, especially in trials with very long follow‐up, 2) results were often scattered in several papers in different years, whereas year of trial start is more well‐defined. Other citations are labelled in the standard fashion with year of publication.
Excluded studies
We excluded 56 studies found in the updated search (Characteristics of excluded studies). The list of excluded studies (Characteristics of excluded studies) also includes one important but not eligible trial not found in the search (Lindholt 2017). In the previous version of the review, two articles were awaiting assessment (Brett 2012; Stickler 2000). These have been excluded.
Risk of bias in included studies
Risk of bias varied considerably between trials, but there were problems in most trials, mainly in relation to outcomes that required participation for follow‐up. The two major issues were lack of blinding and missing outcome data, whereas selection bias was unlikely in most trials.
For our primary outcomes, nine out of eleven trials reporting on these had low risk of selection bias, and ten out of eleven were at low risk of attrition bias. Kaiser Permanente 1965, South‐East London 1967 and Ebeltoft 1992 were biased towards no effect because of contamination and low contrast between groups. For OXCHECK 1989, we chose to combine all three intervention groups to achieve more power, accepting a loss of contrast. However, the results were similar when analysing the results for maximum contrast, that is only comparing those screened in year one with those in year four. Four trials were biased by design in favour of the screening group, due to follow‐up of detected problems at special centres (Göteborg 1963; Göteborg 1970; Malmö 1969; WHO 1971).
For other outcomes, detection bias, biased reporting of subjective outcomes, and biased dropout were major concerns in many of the trials. In particular, the patient‐reported outcomes should be viewed with caution due to the lack of blinding. Readers are referred to the 'Risk of bias' figures for an overview (Figure 2; Figure 3).
2.
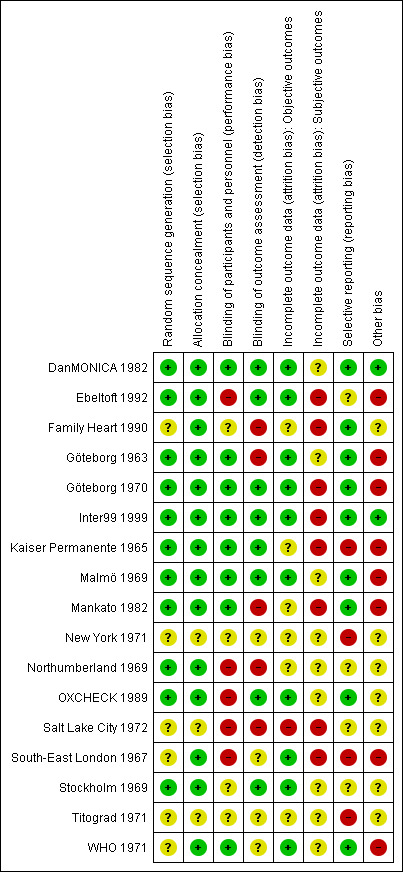
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study
3.
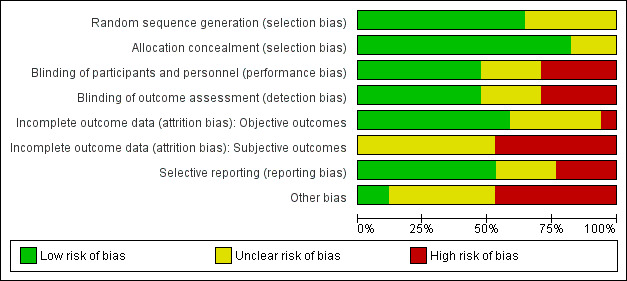
'Risk of bias; graph: review authors' judgements about each risk of bias item presented as percentages across all included trials
Allocation
Seven trials used a genuinely random method for generating the randomisation sequence (DanMONICA 1982; Ebeltoft 1992; Göteborg 1970; Inter99 1999; Mankato 1982; OXCHECK 1989; Stockholm 1969). We could not determine how six trials generated the sequence (Family Heart 1990; New York 1971; Salt Lake City 1972; South‐East London 1967; Titograd 1971; WHO 1971). Four trials used allocation methods such as date of birth (Göteborg 1963; Kaiser Permanente 1965; Malmö 1969; Northumberland 1969), but these trials included participants through lists or registers and allocated them all at once before making any contact with them, and we therefore judged the risk of selection bias to be low.
We judged allocation to be adequately concealed in 14 trials (DanMONICA 1982; Ebeltoft 1992; Family Heart 1990; Göteborg 1963; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; Mankato 1982; Northumberland 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971). It was unclear in three trials (New York 1971; Salt Lake City 1972; Titograd 1971).
We thus judged 11 trials as likely to be free from selection bias (DanMONICA 1982; Ebeltoft 1992; Göteborg 1963; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; Mankato 1982; Northumberland 1969; OXCHECK 1989; Stockholm 1969). We could not rule out selection bias in six trials. Five trials did not describe sequence generation (Family Heart 1990; New York 1971; Salt Lake City 1972; Titograd 1971; WHO 1971), and South‐East London 1967 used a matching procedure, which was unclearly described, for randomisation, and the sizes of the groups varied between publications.
Blinding
Performance bias
Performance bias in this context meant differences in medical attention and preventive and screening activities resulting from knowledge of allocation.
In eight trials, the risk of performance bias was low (DanMONICA 1982; Göteborg 1963; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; Mankato 1982; WHO 1971), in four trials it was unclear (Family Heart 1990; New York 1971; Stockholm 1969; Titograd 1971), and in five trials the risk was high (Ebeltoft 1992; Northumberland 1969; OXCHECK 1989; Salt Lake City 1972; South‐East London 1967), because the primary care physicians clearly had knowledge of the status of their patients. For example, in one trial primary care physicians had lifestyle conversations with a subset of their own patients (Ebeltoft 1992), and in another trial there was a sticker on the medical records indicating the allocation (OXCHECK 1989).
Detection bias
We present a single assessment of the risk of detection bias for each trial, although there were exceptions for some outcomes in some trials (see Characteristics of included studies).
Eight trials had a low risk for most outcomes (DanMONICA 1982; Ebeltoft 1992; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; OXCHECK 1989; Stockholm 1969), four trials had unclear risk (New York 1971; South‐East London 1967; Titograd 1971; WHO 1971), and five trials had a high risk (Family Heart 1990; Göteborg 1963; Mankato 1982; Northumberland 1969; Salt Lake City 1972).
Of the three trials that adjudicated the cause of death given on death certificates, one did this blinded (Malmö 1969), one unblinded (Göteborg 1963), and in one it was unclear (WHO 1971). The other eight trials reporting on mortality used public registers or death certificates without re‐classification (DanMONICA 1982; Ebeltoft 1992; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; OXCHECK 1989; South‐East London 1967; Stockholm 1969).
We considered answers to questionnaires to be at high risk of bias due to the lack of blinding of the intervention group.
Incomplete outcome data
Objective outcomes
For objective outcomes (for example mortality, physician visits), we judged the risk of attrition bias to be low in ten trials (DanMONICA 1982; Ebeltoft 1992; Göteborg 1963; Göteborg 1970; Inter99 1999; Malmö 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971), unclear in six trials (Family Heart 1990; Kaiser Permanente 1965; Mankato 1982; New York 1971; Northumberland 1969; Titograd 1971), and high in one trial (Salt Lake City 1972), which excluded participants who changed economic status, did not attend for screening, did not consult their physician about screening results, or did not participate in the one‐year follow‐up. This resulted in only 49% of the intervention group and 82% of the control group participants being included in the analyses. In Kaiser Permanente 1965, the trial authors considered participants as lost to follow‐up when they left the Kaiser health plan. This resulted in the loss of more than one third of participants for most outcomes. For mortality, only people leaving California were lost. The trial authors used registers, and estimated the loss to be 8% to 18% over the 16‐year study period (Friedman 1986). Other trial authors had access to mortality registers with much fewer losses (Ebeltoft 1992; Göteborg 1963; Göteborg 1970; Malmö 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971). WHO 1971 did not report cancer mortality from the Belgian part of the trial. The reason given for this was that all non‐coronary deaths were only categorised as such, without detailing the cause of death, as per the trial's protocol. The risk of bias due to this was unclear.
Subjective outcomes
In unblinded trials, attrition bias (bias due to incomplete outcome data in those lost to follow‐up) is a threat to any outcome that is dependent on the active participation of participants for follow‐up, for example answering a questionnaire, even when numbers lost to follow‐up are similar in the groups. None of the trials were at low risk of attrition bias, nine trials did not report subjective outcomes (DanMONICA 1982; Göteborg 1963; Malmö 1969; Northumberland 1969; New York 1971; OXCHECK 1989; Stockholm 1969; Titograd 1971; WHO 1971), and the risk was high in all other trials (Ebeltoft 1992; Family Heart 1990; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Mankato 1982; Salt Lake City 1972; South‐East London 1967).
Five trials investigated the possible effects of the missing data. In Inter99 1999, the authors investigated the effects of non‐response with logistic regression on serial measurements of self‐reported health. They found that extreme values of self‐reported health were associated with non‐response but judged it unlikely to have seriously biased the results (Pisinger 2009). The British Family Heart Study (Family Heart 1990) used imputation with the last observation carried forward in the analysis of self‐reported health and found no important differences. In another analysis they found twice as many smokers among non‐attenders as among attenders. The Minnesota Heart Health Program trial (Mankato 1982) and OXCHECK 1989 found similar evidence of bias in relation to smoking but no large differences for other variables.The Ebeltoft 1992 authors reported in a letter that there were no differences in sex, age, baseline smoking, and baseline body mass index (BMI) between non‐attenders in the intervention and control groups, but did not present the data (Engberg 2002). Important differences might not be statistically significant when the numbers are small.
None of the trials used optimal imputation techniques (for example multiple imputation). Last observation carried forward may give biased results, and the direction of the bias is unpredictable (Jørgensen 2014). Also, there might be differences in unmeasured factors, such as motivation and ability to change lifestyle, and we advise caution in interpreting these outcomes.
Selective reporting
We found nine trials to be at low risk of reporting bias (DanMONICA 1982; Family Heart 1990; Göteborg 1963; Göteborg 1970; Inter99 1999; Malmö 1969; Mankato 1982; OXCHECK 1989; WHO 1971), in four trials the risk was unclear (Ebeltoft 1992;; Northumberland 1969; Salt Lake City 1972; Stockholm 1969) and in four trials the risk of reporting bias was high: Kaiser Permanente 1965 collected data on surgery, prescriptions, and reasons for hospitalisation but did not publish them. They also collected and reported results on new diagnoses in early publications but not for the planned study period; South‐East London 1967 collected but did not report data on referrals, prescriptions, and investigations carried out; and New York 1971 and Titograd 1971 have never published any results. A funnel plot for mortality did not suggest publication bias (Figure 4).
4.
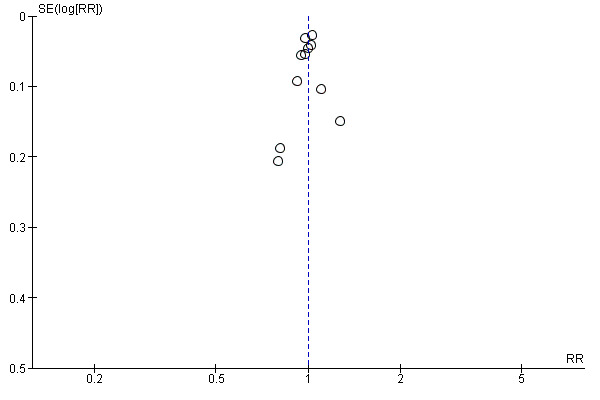
Funnel plot of comparison 1. Health checks versus control, outcome: 1.1 Total mortality.
Other potential sources of bias
Four trials had a design that could favour the screening group (Göteborg 1963; Göteborg 1970; Malmö 1969; WHO 1971). In these trials, conditions identified at screening were treated and followed at a special clinic or by the researchers whereas participants in the control group used their normal physicians. However, this could also increase possible iatrogenic harm.
Screening of the control group (contamination) would dilute both the beneficial and the harmful effects of the intervention. Only two trials assessed the number of participants in the control group having health checks. In Kaiser Permanente 1965, after 16 years, the mean number of health checks in the control group was 2.8 compared with 6.8 in the screening group, and 36% of the control group had not had a health check compared to 16% of the screening group. However this result cannot be generalised to the other trials or other populations, mainly because the participants were all members of the same health plan with access to the same high‐profiled multiphasic health screening. Also, screening has long been more popular in the USA than in Europe. In the South‐East London Screening Study (South‐East London 1967), there was very little interest in screening among the participants in the control group, and none were screened for the first five years (Trevelyan 1973). However, the control group was offered screening after five years, which biased the nine‐year results towards no effect.
The British Family Heart Study (Family Heart 1990), used both an internal and an external control group in order to investigate contamination. They found similar results when comparing with either control group indicating that contamination was not a big problem. In Ebeltoft 1992, which was set in a small town, the trial authors noted that the trial appeared to have a large positive influence on the health behaviours of the control group (Lauritzen 2012). Also, the control group was offered screening after five years while some data were collected for eight years. Mankato 1982 was conducted during a health promotion campaign, which may have diminished the effect of the intervention.
In summary, we found seven trials with a low risk of contamination (DanMONICA 1982; Göteborg 1963; Göteborg 1970; Inter99 1999; Malmö 1969; Stockholm 1969; WHO 1971), six trials in which it was unclear (Family Heart 1990; New York 1971; Northumberland 1969; OXCHECK 1989; Salt Lake City 1972; Titograd 1971), and four trials with a high risk of contamination (Ebeltoft 1992; Kaiser Permanente 1965; Mankato 1982; South‐East London 1967).
Two trials randomised people who had returned an initial questionnaire on health and lifestyle (Ebeltoft 1992; OXCHECK 1989). This limited the external validity because of self‐selection of people with an interest in health and lifestyle (Pill 1988; Waller 1990).
Effects of interventions
See: Table 1
Please note that included trials are labelled with year of trial start, rather than publication year, as described above.
Total mortality
Eleven trials reported total mortality (DanMONICA 1982; Ebeltoft 1992; Göteborg 1963; Göteborg 1970; Inter99 1999; Kaiser Permanente 1965; Malmö 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971).The median length of follow‐up was 10 years and the range was 4 to 30 years.The median event rate in the intervention and control groups combined was 7% and the range was 2% (OXCHECK 1989), to 36% (DanMONICA 1982), reflecting the different lengths of follow‐up (Table 3).
2. Overview of mortality.
| Deaths in intervention group | Participants in intervention group | Deaths in control group | Participants in control group | |
| Total mortality | ||||
| Göteborg 1963 | 146 | 1010 | 306 | 1956 |
| Kaiser Permanente 1965 | 585 | 5138 | 643 | 5536 |
| South‐East London 1967 | 196 | 3292 | 169 | 3132 |
| Stockholm 1969a | 492 | 3064 | 2503 | 29122 |
| Malmö 1969 | 49 | 809 | 60 | 804 |
| Göteborg 1970 | 1293 | 10004 | 2636 | 20018 |
| WHO 1971b | 1325 | 30489 | 1186 | 26971 |
| OXCHECK 1989 | 205 | 8307 | 54 | 2783 |
| Ebeltoft 1992 | 49 | 2030 | 43 | 1434 |
| Inter99 1999c | 595 | 11629 | 2568 | 47987 |
| DanMONICA 1982d | 2033 | 4789 | 4399 | 12994 |
| Cancer mortality | ||||
| Göteborg 1963 | 35 | 1010 | 73 | 1956 |
| Kaiser Permanente 1965 | 173 | 5138 | 190 | 5536 |
| South‐East London 1967 | 50 | 3292 | 47 | 3132 |
| Stockholm 1969a | 144 | 3064 | 757 | 29122 |
| Malmö 1969 | 17 | 809 | 9 | 804 |
| Göteborg 1970 | 315 | 10004 | 728 | 20018 |
| WHO 1971 | 564 | 23358 | 456 | 20957 |
| OXCHECK 1989 | 82 | 8307 | 23 | 2783 |
| Cardiovascular mortality | ||||
| Göteborg 1963 | 74 | 1010 | 132 | 1956 |
| Kaiser Permanente 1965 | 240 | 5138 | 256 | 5536 |
| South‐East London 1967 | 84 | 3292 | 52 | 3132 |
| Stockholm 1969a | 206 | 3064 | 947 | 29122 |
| Malmö 1969 | 14 | 809 | 33 | 804 |
| Göteborg 1970 | 526 | 10004 | 1077 | 20018 |
| WHO 1971b | 428 | 30489 | 398 | 26971 |
| OXCHECK 1989 | 83 | 8307 | 17 | 2783 |
| DanMONICA 1982d | 583 | 4798 | 1087 | 12994 |
aSkewed randomisation in age and needs strata, giving unbalanced baselines. bWe used a published effect estimate that took the matched pair cluster randomisation into account cSkewed randomisation in age and gender strata, giving unbalanced baselines. dSkewed randomisation in age and gender strata, giving unbalanced baselines.
Health checks have little or no effect on total mortality (RR 1.00, 95% CI 0.97 to 1.03; 11 trials; 233,298 participants and 21,535 deaths; high‐certainty evidence, I2 = 0%; Analysis 1.1). Subgroup and sensitivity analyses did not alter the results.
1.1. Analysis.
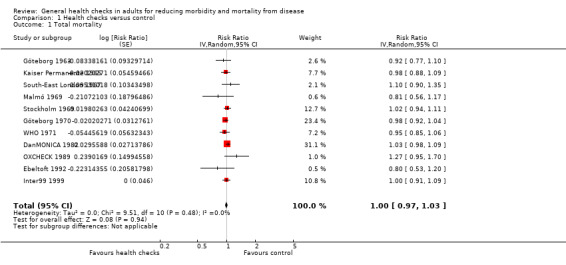
Comparison 1 Health checks versus control, Outcome 1 Total mortality.
Disease‐specific mortality
Cancer mortality
Eight trials reported cancer mortality (Göteborg 1963; Göteborg 1970; Kaiser Permanente 1965; Malmö 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971). Health checks have little or no effect and did not reduce cancer mortality (RR 1.01, 95% CI 0.92 to 1.12; 8 trials; 139,290 participants and 3663 deaths; high‐certainty evidence, I2 = 33%; Analysis 1.14). Subgroup and sensitivity analyses did not alter the results. Göteborg 1970 found a reduction in cancer mortality (RR 0.87, 95% CI 0.76 to 0.99), which is surprising since that trial only screened for cardiovascular risk factors. Furthermore, Göteborg 1970 was not successful in reducing smoking. We believe that the result is due to chance.
1.14. Analysis.
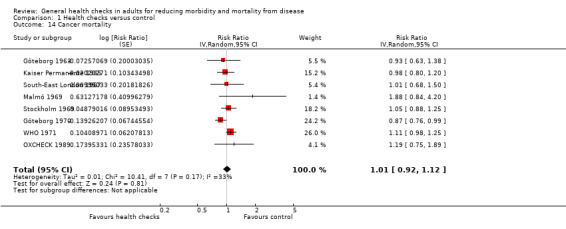
Comparison 1 Health checks versus control, Outcome 14 Cancer mortality.
Cardiovascular mortality
Nine trials reported cardiovascular mortality, although with differing definitions (DanMONICA 1982; Göteborg 1963; Göteborg 1970; Kaiser Permanente 1965; Malmö 1969; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971). Health checks probably have little or no effect and did not reduce cardiovascular mortality (RR 1.05, 95% CI 0.94 to 1.16; 9 trials; 170,227 participants and 6237 deaths; moderate‐certainty evidence; I2 = 65%; Analysis 1.27). One possible explanation for the large heterogeneity was the different definitions of the outcome among trials. For example, WHO 1971 only reported mortality from coronary heart disease whereas other trials combined deaths from ischaemic heart disease and stroke (DanMONICA 1982). One trial found a large reduction in cardiovascular mortality with health checks (Malmö 1969), while two trials found substantial increases (DanMONICA 1982; South‐East London 1967). Subgroup and sensitivity analyses did not alter the results, nor explain heterogeneity.
1.27. Analysis.
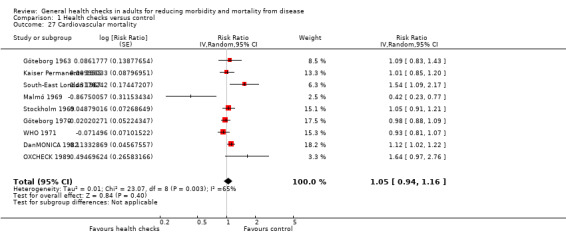
Comparison 1 Health checks versus control, Outcome 27 Cardiovascular mortality.
Morbidity
Combined fatal and non‐fatal ischaemic heart disease
Four trials reported combined fatal and non‐fatal ischaemic heart disease or coronary heart disease (DanMONICA 1982; Göteborg 1970; Inter99 1999; WHO 1971). Health checks have little or no effect on this (RR 0.98, 95% CI 0.94 to 1.03; 4 trials; 164,881 participants, 10,325 events; high‐certainty evidence; I2 = 11%; Analysis 1.40).
1.40. Analysis.
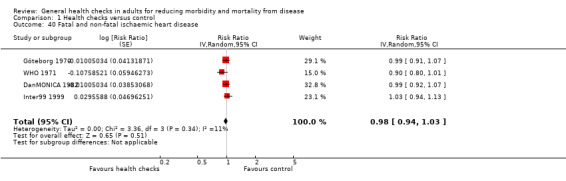
Comparison 1 Health checks versus control, Outcome 40 Fatal and non‐fatal ischaemic heart disease.
Combined fatal and non‐fatal stroke
Three trials reported combined fatal and non‐fatal stroke (DanMONICA 1982; Göteborg 1970; Inter99 1999). Health checks probably have little or no effect on this (RR 1.05 95% CI 0.95 to 1.17; 3 trials; 107,421 participants, 4543 events; moderate‐certainty evidence, I2 = 53%; Analysis 1.41). One trial found a large harmful effect of health checks (DanMONICA 1982), which caused the heterogeneity. This trial had the longest follow‐up of all trials (30 years), employed broad screening and used little lifestyle intervention.
1.41. Analysis.
Comparison 1 Health checks versus control, Outcome 41 Fatal and non‐fatal stroke.
Other measures of morbidity
Six other trials reported some measure of morbidity.
The OXCHECK 1989 authors supplied us with data on incident cancers. When pooling the three intervention groups and comparing with the control group the RR was 1.12 (95% CI 0.85 to 1.48). When using only the group screened at year one, for maximum contrast, the RR was 1.17 (95% CI 0.85 to 1.63).
Kaiser Permanente 1965 found that, after seven years, 61% of the intervention group reported having a chronic condition compared to 54% in the control group. The conditions were not defined and were likely to have included risk factors like elevated blood pressure or blood glucose.
The South‐East London Screening Study (South‐East London 1967) did not find effects on the prevalence of angina, changes on electrocardiogram indicating ischaemia, or bronchitic symptoms after five years. For angina the prevalence was 21.9% (screening) and 22.4% (control group), for ischaemic changes 17.9% (screening) and 16.6% (control), and for bronchitic symptoms 29.0% (screening) and 30.6% (control). They also specified the reasons for hospitalisation, using broad categories, such as cardiovascular causes, central nervous system causes, and neoplasms, but did not find differences.
Malmö 1969 reported reasons for hospitalisation in disease categories, for example ischaemic heart disease, cerebrovascular disease, and neoplasms, and did not find differences between groups. There was low power due to the stratification in disease categories. See the results on total hospitalisation below.
The British Family Heart Study (Family Heart 1990), investigated the effect on the prevalence of four conditions. They found substantially more participants with self‐reported high blood pressure and high cholesterol in the screening group, slightly more men with self‐reported diabetes in the screening group, and no effect on self‐reported coronary heart disease. After one year, 6.9% of the control group men had high blood cholesterol compared to 14% of the screening group. For women the results were 3.8% (control) and 9.7% (screening). For high blood pressure, the results for men were 14.8% (control) and 17.1% (screening); and for women, 13.0% (control) and 16.2% (screening). For diabetes, the results for men were 1.7% (control) and 3.3% (screening); and for women, 1.1% (control) and 1.2% (screening). For coronary heart disease, the results for men were 5.5% (control) and 5.9% (screening); and for the women, 1.1% (control) and 1.9% (screening). The results were similar when the trial authors calculated the results within each practice and pooled results. The results were at risk of detection bias and attrition bias.
Inter99 1999 found that health checks increased the incidence of diabetes in the first year, HR 1.68 (P = 0.0001), but that this evened out during further follow‐up.
In summary, health checks did not reduce morbidity in terms of actual illness, but they may increase the number of people diagnosed with elevated risk factors.
New diagnoses
In addition to conditions identified through the screening itself, screening might increase diagnostic activity between scheduled screenings due to increased physician contact in relation to follow‐up visits or due to a lowered threshold for consulting a physician. Cumulative rates of new diagnoses over time in the screened and unscreened groups would allow an assessment of the full effect of screening on diagnostic activity. However, only one trial reported such results (Kaiser Permanente 1965), and only for the first six years. In a 40% sample, Kaiser Permanente 1965 found a sharp divergence in the mean annual number of new diagnoses per participant immediately after the intervention started, with the differences being statistically significant each year. By adding the results for each year we found a mean number of new diagnoses per participant of 4.3 in the screening group and 3.6 in the control group. This corresponded to a 20% increase. The trial lasted for 16 years but follow‐up for new diagnoses was not continued.
Four trials reported their findings at the first screening of the intervention group but without comparisons with the control group over time. South‐East London 1967 found an average of 2.3 diseases per participant at the first screening. Of these, 53% were not previously known. Ebeltoft 1992 reported the percentage of participants with abnormal findings prompting health advice at the initial screening to be 76%. The most common reasons were raised CO concentration in expiratory air in smokers (37%), low physical endurance (30%), poor hearing (19%), poor sight (12%), and being overweight (16%). Increased cardiovascular risk was found in 11%, hypercholesterolaemia in 10%, hypertension in 10%, and elevated liver enzymes in 13%. Salt Lake City 1972 found a total of 2031 abnormalities in 384 people screened. This trial used very broad biochemical screening.
In summary, health checks may increase the number of new diagnoses (low‐certainty evidence).
Admission to hospital
Five trials reported hospitalisation using different measures, for example, admission rates, number of people admitted once or more, or number of days in hospital.
Kaiser Permanente 1965 reported the mean number of days in hospital over 18 years of follow‐up. The results were 10.0 days in the intervention group and 10.4 days in the control group. Roughly one third of participants had missing data. South‐East London 1967 reported the number of participants admitted to hospital once or more during nine years of follow‐up, RR 1.04 (95% CI 0.96 to 1.13). The amount of missing data was unclear but was probably low. Malmö 1969 also studied the number admitted once or more and found similar results, RR 1.05 (95% CI 0.92 to 1.20). There were 3% to 5% missing data. Salt Lake City 1972 compared hospitalisation rates before and after the intervention and did not find an effect, but they did find an effect on the number of nights in hospital in one of three subgroups, which was an unreliable result due to biased exclusions after randomisation. Ebeltoft 1992 compared admission rates in the two intervention groups with the control group and did not find an effect after eight years, rate ratio of 0.91 (95% CI 0.63 to 1.32). They also compared the random sample invited to participate in the trial with all not invited and found similar results, rate ratio of 0.97 (95% CI 0.80 to 1.18). There were 5% missing data.
In summary, health checks may make little or no difference to admission rates, number of people admitted once or more, or number of days in hospital (low‐certainty evidence).
Disability
Three trials investigated the effect on disability. Kaiser Permanente 1965 found that after 16 years 31% of the screening group and 30% of the control group reported total or partial disability on a questionnaire. Attrition was roughly one third and response rates around 75%, which left only half of the people randomised in this analysis. South‐East London 1967 found that 2.5% in the screening group and 1.8% in the control group reported major disability after five years. There were between 40% and 50% missing data in this analysis. Salt Lake City 1972 compared the number of disability days before and after the intervention and did not find an effect.
In summary, health checks may make little or no difference to disability (low‐certainty evidence).
Worry
Only two trials reported relevant results, using scales measuring psychological distress.
Ebeltoft 1992 used the General Health Questionnaire (GHQ‐12) at baseline and after one and five years. A decrease in score indicates a beneficial effect of the intervention. After one year, the change from baseline in the screening groups was an increase of 0.05 and in the control group a decrease of 0.16, P = 0.6. After five years, the screening group had a decrease of 0.23 and the control group had a decrease of 0.39, P = 0.73. They also investigated subgroups of smokers, overweight participants, people who were informed of an elevated risk and people informed of no elevated risk, and did not find effects. Participation was 79% after five years.
South‐East London 1967 used the Middlesex Hospital Questionnaire on a subset of participants after five years. In the anxiety domain of the scale, the trial authors found lower scores in the intervention group among men (lower scores are better). When pooling men and women, we found a mean score of 4.14 (standard deviation (SD) = 3.38, 602 participants) in the intervention group and 4.48 (SD = 3.63, 572 participants) in the control group, P = 0.10 (t‐test, equal variances). In the other domains assessed with this scale ('phobic', 'obsessional', 'somatic', 'depression', 'hysteria'), there were no effects. Follow‐up was roughly 90%.
In summary, health checks may make little or no difference to worry (low‐certainty evidence).
Self‐reported health
Four trials reported self‐reported health.
South‐East London 1967 found that after five years 53.6% of the screening group and 56.5% of the control group reported good or excellent health in the preceding two weeks (Chi2 = 3.274, P = 0.07).
Ebeltoft 1992 used a five‐point scale at baseline and after five years. After five years, 70% and 72% of the two intervention groups reported good or excellent health compared to 71% of the control group. Data on change from baseline were only available in a graph. This showed that approximately 12% in the intervention groups had an improvement in self‐reported health compared to approximately 20% in the control group.
In Family Heart 1990, 79.5% of the screening group and 75.7% of the internal control group reported good or excellent health after one year. This analysis used last observation carried forward for missing data. The pooled difference, taking into account the 13 different practices, was 3.8% in favour of screening, P = 0.004.
Inter99 1999 used SF‐12 and found slower deterioration of both physical and mental health components in the intervention group. For mental health, the difference after five years was approximately 2 on a 100‐point scale, where 50 is the mean of a reference population with a SD of 10. The effect was even smaller for physical health but was difficult to assess because of baseline imbalances in scores. The trial authors found indications of biased non‐response.
In summary, health checks may slightly improve self‐reported health (low‐certainty evidence).
Referrals to specialists
Only one trial (Ebeltoft 1992), reported on this outcome, but we could not use the results in our analysis. The trial authors only had data from 1995 to 1999 but the screening took place in 1992 to 1993 (intervention groups screened), and 1997 (intervention groups and control group screened). Thus the expected increase in referrals following the intervention was not included in the analysis and any contrast between groups would be diluted by the 1997 screening. The trial authors made two comparisons and did not find effects in either analysis. When comparing the screening and control groups, the rate ratio was 1.04 (95% CI 0.85 to 1.26). When comparing the random sample invited to participate in the trial versus all eligible people not invited, the rate ratio was 0.94 (95% CI 0.84 to 1.06).
In summary, it is uncertain whether health checks increase or reduce referrals to specialists, as the certainty of this evidence is very low.
Non‐scheduled visits to general practitioners
Five trials reported physician visits. The length of follow‐up was between one and nine years, with missing outcome data ranging between 5% (Ebeltoft 1992) and 51% (Salt Lake City 1972).
Kaiser Permanente 1965 found a mean number of physician visits of 16.0 in both groups after five years, not including the screenings themselves. The results were reported without measures of uncertainty and data on this outcome were collected from a 20% subsample.
South‐East London 1967 did not find an effect on the mean annual number of physician visits. It was not clear whether the screening visits were included in this, and we cannot tell whether the results were from the five‐year or nine‐year follow‐up. We excluded participants who left the study before one year from the analyses (14% from the screening group and 13% from the control group).
Northumberland 1969 found an average number of consultations per participant of 5.4 in the screening group and 5.0 in the control group over 1½ years. This did not include the screenings themselves. When adding the screenings the results were 6.3 in the screening group and 5.0 in the control group. The trial authors did not specify the type of health check, and there was a high risk of detection bias, as the allocation was noted on the front cover of the participant's record.
Salt Lake City 1972 did not find effects after one year, but this result was unreliable due to biased exclusions. The screening visits were not included in the analysis.
Ebeltoft 1992 found an increased rate of physician visits after five years in the screening plus health discussion group compared to the control group, rate ratio of 1.15 (95% CI 1.02 to 1.31), but not in the screening only group compared to controls, rate ratio of 1.01 (95% CI 0.89 to 1.15). When comparing all those invited to participate in the trial with all not invited, the rate ratio was 1.01 (95% CI 0.93 to 1.10). However, this comparison included screening of the control group in 1997, diluting any differences between groups. The trial authors found a downward trend in the rate ratio over time favouring the intervention, but in the absence of an overall effect this is not a relevant observation. It likely reflects the initial increase in visits generated by the screenings themselves, which gave a high starting point for the trend analysis.
In summary, health checks may make little or no difference to the number of physician visits (low‐certainty evidence).
Additional diagnostic procedures required due to positive screening tests
We did not find any trials that reported this outcome.
Kaiser Permanente 1965 reported the mean number of laboratory tests per participant after five and 10 years, based on a 20% sample. After five years it was 23.8 in the screening group and 23.3 in the control group. The data after 10 years were not reported but the trial authors stated that there was no difference. The number of laboratory tests did not include the tests used at screening.
Prescriptions and surgery
None of the trials reported the total number of prescriptions, new drugs prescribed, or the number of operations performed. This is unfortunate since these are important factors for balancing the benefits and harms of health checks and for estimating the costs.
Five trials provided some results of relevance.
Göteborg 1970 examined random samples of the intervention group and control group and found that after 10 years of follow‐up 26.0% of the intervention group used antihypertensive medications compared to 19.6% in the control group (Chi2 = 16.41, P < 0.0001, our calculation). Kaiser Permanente 1965 reported narratively that prescription rates gathered from pharmacies showed a non‐significant trend towards increased prescription in the screening group, but only analysed data from years six and seven. Ebeltoft 1992 presented data on self‐reported use of selected types of drugs after five years. In the screening groups, 4.8% reported using blood pressure medication compared to 6.8% in the control group (Chi2 = 1.42, P = 0.23, our calculation). For diuretics, the figures were 3.7% (screening), and 3.9% (control group), and for heart medication they were 0.9% (screening), and 1.0% (control). Family Heart 1990 reported narratively that there was no difference between the intervention and control groups regarding use of drugs to lower blood pressure or cholesterol, or for diabetes. Mankato 1982 reported that the proportion of participants on blood pressure medication after one year was 13.8% in the intervention group and 9.8% in the control group (P < 0.05).
In summary, it is uncertain whether health checks increase or reduce prescriptions and surgery, as the certainty of this evidence is very low.
Absence from work
Two trials reported absence from work (Kaiser Permanente 1965; South‐East London 1967). Neither trial found an effect, and neither trial reported the exact results but only mentioned their findings in a narrative.
It is uncertain whether health checks increase or reduce absence from work as the certainty of this evidence is very low.
Subgroup and sensitivity analyses
We planned and performed several subgroup and sensitivity analyses. Some of the resulting subgroups were based on very few trials but are presented for completeness (see graphs). They should be interpreted with caution and we found no convincing patterns.
For outcomes not included in the meta‐analyses we were not able to discern any patterns except that the more recent trials often had a strong focus on lifestyle interventions, often had changes in risk factors as their primary outcomes, and were designed accordingly, with shorter follow‐up (Ebeltoft 1992; Family Heart 1990; Mankato 1982; OXCHECK 1989).
Discussion
Summary of main results
We found 17 randomised trials comparing the effect of systematic offers of one or more health checks versus usual care, 15 of which had reported results. Health checks have little or no effect on total mortality or cancer mortality (high‐certainty evidence), and probably have little or no effect on cardiovascular mortality (moderate‐certainty evidence), Similarly, health checks have little or no effect on fatal and non‐fatal ischaemic heart disease (high‐certainty evidence) and probably have little or no effect on fatal and non‐fatal stroke (moderate‐certainty evidence). This update included one new trial, the results of which confirm those of previous trials.
For total mortality our confidence interval includes a 3% reduction and a 3% increase, both of which would be clinically relevant. However, for the causes of death most likely to be influenced by health checks, cardiovascular and cancer‐specific mortality, there were no reductions either. A substantial latency of effects on mortality would be expected but we included several trials with very long follow‐up. Our results suggest that the lack of an effect on total mortality is not a chance finding, nor due to low power.
Overall completeness and applicability of evidence
The lack of effect on our primary outcomes was mirrored by a lack of effect on most of our secondary outcomes. The outcomes expected to reflect beneficial effects of the intervention were better studied and reported than the harmful outcomes. We expected the number of new diagnoses and initiated treatments to be reported since these are important elements of screening, but this was rarely the case. Only one trial reported the number of new diagnoses in the two groups, and only for the first six years although the intervention was continued for 16 years (Kaiser Permanente 1965). Drug use was only assessed for selected drugs and was mainly self‐reported. We also expected the number of follow‐up tests and referrals to specialists to be reported since they reflect the burden of screening on the participants and the healthcare system. However, these outcomes were rarely reported. Without knowing the amount of 'downstream' investigations following screening, it is not possible to evaluate the harms or costs (Walter 2013). This has long been recognised as a problem for screening in general (Raffle 2007).
Increased diagnostic and therapeutic activity would be expected if general health checks led to improved health, at least in the short term, as this is the main mechanism of the intervention. However, more diagnoses and more treatment in the absence of health improvements would indicate overdiagnosis and overtreatment. Overdiagnosis is the diagnosis of conditions that would not have caused symptoms or caused other problems for patients and is an inherent problem in any screening programme. Overdiagnosis leads to overtreatment, which has been documented particularly in cancer screening but is also an obvious harm in screening for cardiovascular risk factors, as reflected in the large numbers needed to treat for an additional beneficial outcome in primary prevention of cardiovascular disease (Welch 2011).
The included studies investigated the psychological consequences of general health checks to a somewhat greater extent, although only in a minority of trials. An interesting result is that we did not find any reliable effects on measures of psychological distress, self‐reported health, or absence from work. One systematic review (Boulware 2007), found beneficial effects of periodic health evaluations on worry in one trial of elderly people (Patrick 1999), and a systematic review of coronary heart disease risk scores found no harmful effects in two "fair‐quality" studies (Sheridan 2008). Regarding hypertension, cross‐sectional studies have found that people diagnosed with hypertension had poorer self‐reported health, regardless of whether they were correctly diagnosed or not (Barger 2006; Bloom 1981). However, a review of cohort studies found mixed effects on absenteeism and "fair‐quality" evidence that screening for hypertension does not cause adverse psychological effects (Sheridan 2003). One review found short‐term adverse psychological effects from predicting a person's risk of illness, but no long‐term effects (Shaw 1999). Similarly, a review of trials of any kind of screening found no long‐term effect on anxiety, depression, or quality of life, but the authors were not able to make conclusions about short‐term effects (Collins 2011). None of the trials we reviewed reported on short‐term adverse psychological effects.
The lack of beneficial effects indicates that general health checks did not work as intended in the included trials. Below, we explore possible reasons for the apparent lack of effect as well as challenges in generalising the results to the present day.
Bias
Three trials in our mortality meta‐analyses were biased towards no effect (Ebeltoft 1992; Kaiser Permanente 1965; South‐East London 1967), and in one trial we prioritised power over contrast in the merging of intervention groups (OXCHECK 1989). However, in a post hoc sensitivity analysis, removing these trials from the analyses did not change the results and only marginally expanded the confidence intervals.
Type of health check
Many of the older trials investigated very broad screening regimens, with a large potential for detecting abnormalities. Healthy people frequently harbour pathology that can be discovered by examination, imaging (Furtado 2005; Xiong 2005), or biopsy (Welch 2004), but this is not necessarily beneficial and it may be harmful (Welch 2011). The results from Kaiser Permanente 1965 suggested that it was, as they found increases in mortality due to lymphohaematopoietic cancers and suicide. This may be a random finding although the pattern appeared after seven years and continued throughout the full 16 years of the trial. The increase in available diagnostic tests might lead to more invasive follow‐up procedures today and more drug treatment and surgery, for example for prostate and thyroid cancer, with resulting harms. Today, no authorities recommend health checks as broad as studied in some of the older trials but they are still common, particularly among commercial providers (Grønhøj Larsen 2012).
Most of the trials that reported mortality did not have an explicit lifestyle intervention component, but we do not expect this element to be particularly important. Multiple risk factor interventions directed at general populations for the primary prevention of coronary heart disease have been extensively studied and did not find an effect on total or coronary heart disease‐specific mortality, or the number of cardiovascular events (Ebrahim 2011). One of the trials in our review included a randomised comparison between screening with and screening without scheduled face‐to‐face lifestyle conversations, but found no effect (Ebeltoft 1992).
Developments in therapy
Developments in preventive drug therapy might produce a different effect on cardiovascular outcomes today compared to the time when some of the trials were performed. For example, use of statins and angiotensin‐converting enzyme inhibitors instead of harmful drugs such as clofibrate (WHO 1984), and reserpine (Healy 2004), is likely to provide a considerable improvement. However, we cannot be certain that developments in drug treatments are always beneficial to patients because some modern drugs may have serious harms that are not known at present. For example, the diabetes drug rosiglitazone was on the market for 10 years before being withdrawn because it causes serious heart disease (Lehman 2010; Nissen 2010). Also, poor trial reporting of harms from commonly used preventive drugs, such as statins (Taylor 2013), may mean that adverse effects are more common than we think (Golomb 2012).
Thresholds for treating cardiovascular risk factors and diabetes are lower today than at the time most of the trials were conducted. This has lead to increased prescription of preventive drugs with demonstrated efficacy, for example statins (Taylor 2013), and antihypertensives (Wright 2009). However, the balance between benefits and harms may be unfavourable when the absolute risks are low, such as in a screened population, or when used in more heterogeneous populations with co‐morbidities. For example, the populations used for testing antihypertensive drugs were usually younger and had less co‐morbidity than the typical patient in general practice (Uijen 2007). The inclusion of results from a large trial conducted between 1999 and 2009 (Inter99 1999), indicates that the effect of health checks has not changed with time.
Therapy for identified disease has improved in many areas and this might lead to better effects of health checks over time. However, in the meta‐analyses arranged by year of trial start there are no visible time trends (Analysis 1.1; Analysis 1.27; Analysis 1.14).
Self‐selection
People who accept an invitation to a health check are often different from those who don't. They tend to have higher socioeconomic status (Pill 1988), lower cardiovascular risk (Waller 1990), less cardiovascular morbidity (Jørgensen 2003), and lower mortality (Bender 2015a; Göteborg 1970). This phenomenon is mirrored in studies of adherence to drug therapy, where high adherence to placebo is associated with reduced mortality (Simpson 2006). Thus, systematic health checks may not reach those who need prevention the most, and they have been called 'another example of inverse care' (Waller 1990).
Clinically motivated testing
Another possible reason for the lack of beneficial effects is that many physicians already carry out screening for cardiovascular risk factors or diseases in patients that they judge to be at high risk when they see them for other reasons. This is often considered an integral part of primary care practice. Clinically motivated testing may already have resulted in the identification of many people at high risk thus eroding the potential for a benefit from systematic screening.
Certainty of evidence
For the primary outcomes and for the combined fatal and non‐fatal events, the certainty of the evidence was high or moderate according to our GRADE assessment. This means that further research is unlikely to alter these estimates. For most of the other outcomes, the certainty was low, reflecting the scarcity of reported data.
Potential biases in the review process
We tried to avoid bias by using Cochrane methods, including a peer reviewed protocol, double and independent assessment of search results and full‐text articles, as well as double and independent data extraction and 'Risk of bias' assessment. Since the challenging terminology in this field could lead to overlooked trials, we made a special effort to search exhaustively, including handsearching of reference lists and citation tracking.
In the meta‐analyses, we ignored clustering by family in two trials (OXCHECK 1989; South‐East London 1967), and by factory in the analysis of cancer mortality from WHO 1971. In a pre‐specified sensitivity analysis, excluding cluster‐randomised trials resulted in very little change to the results.
We attempted to contact trial authors and succeeded in 11 cases (DanMONICA 1982; Ebeltoft 1992; Göteborg 1963; Göteborg 1970; Inter99 1999; Malmö 1969; Mankato 1982; OXCHECK 1989; South‐East London 1967; Stockholm 1969; WHO 1971). We often had questions about trial methods but since most trials were quite old, there is a risk that some answers may have been inaccurate.
Agreements and disagreements with other studies or reviews
A systematic review of health checks in general practice (Si 2014), and a Cochrane Review of systematic versus opportunistic screening for cardiovascular risk (Dyakova 2016), found results similar to ours. These reviews also included changes in risk factors, and both found small reductions in cholesterol and blood pressure. One systematic review of health checks included observational studies and geriatric studies but used a different definition of the intervention and included fewer trials (Boulware 2007). The trials that we reviewed are largely different but the results are broadly in line for the overlapping outcomes of total mortality, hospitalisation, disability, and the number of new diagnoses (disease detection). For worry, Boulware 2007 found one trial that showed a beneficial effect whereas we found two trials without an effect on this outcome.
We did not include geriatric trials because they included many interventions other than screening for disease and risk factors, and lifestyle interventions. A systematic review of 89 trials of complex interventions to improve physical function and maintain independent living in elderly people found beneficial effects on the risk of not living at home, nursing home admission, falls, hospital admissions, and physical function, but not mortality (Beswick 2008). In the subgroup of 28 trials of geriatric assessments for elderly people representing the general population, the results were similar except no effect on hospitalisation was found. Thus, the results were similar to ours except on outcomes of special relevance to older people where important benefits were found.
A 2017 trial of screening men aged 65 to 74 years for abdominal aortic aneurisms and central and peripheral hypertension found a reduction in total mortality after a median of 4.4 years although at the price of overtreatment with surgery and medicines (Lindholt 2017). This result could have been due to chance, as mortality from non‐CVD causes were also reduced, though not targeted by the intervention. Similarly, a cluster‐randomised trial of screening participants aged 65 or older for hypertension and cardiovascular risk factors found an effect on cardiovascular events after just one year and with an uptake of screening of only 20%; this result is also likely to be due to chance (Kaczorowski 2011). Nonetheless, people in that age group would seem a reasonable target for further studies of cardiovascular screening as the risk is high.
Authors' conclusions
Implications for practice.
Our results do not support the use of general health checks aimed at a general population. On the other hand, they do not imply either that physicians should stop clinically motivated testing and preventive activities, as such activities may be an important reason why an effect of general health checks has not been shown. Public healthcare initiatives to systematically offer general health checks and offers from private suppliers of general health checks are not supported by the best available evidence.
Implications for research.
We see no reason to do more trials of general health checks, as it seems futile based on the large amount of available data and the fact that the results of previous trials have now been confirmed by a recent large trial. Further research in health checks should be limited to studying the effect of one component at a time, and should include harmful effects. We also suggest that surrogate outcomes such as changes in risk factors are not used for assessing benefits since they do not capture harmful effects and since their relation to meaningful outcomes is usually in doubt. The required large randomised trials with long follow‐up are expensive but not nearly as expensive as the implementation of ineffective or harmful screening programmes. We suggest more focus on the effects of structural interventions to reduce disease, for example, higher taxes on tobacco and alcohol, or restricting corporate advertising for harmful products.
Feedback
Feedback from Verbeek et al, 8 November 2012
Summary
We would like to compliment Krogsbøll and colleagues for their rigorous review of general health checks for preventing morbidity and mortality in adults.
Since health checks are important in occupational settings we were very interested in the content and findings of this review.
From our appraisal, we felt that there were four items that appear contradictory. We would like to bring these to your attention as they could potentially alter the conclusions of the review.
1. What is the outcome of interest?
The title and the objective stated in the review suggest that the relevant outcomes of interest are patient morbidity and mortality. However, when describing the criteria for considering studies in the review, the authors only describe mortality as their primary outcome of interest. Consequentially, it would appear that studies that looked only at morbidity were left out of the selection process. We believe that morbidity is equally important. Restricting the scope of the review by having mortality as the only relevant outcome for patients (despite stating otherwise) is not realistic. There is evidence that we, as healthy persons, are fond of health checks even when we know that the findings cannot be used to improve our health. (Oboler 2002, Schwartz 2004)[JW1]
2. Should non‐randomised studies be excluded?
The authors state that non‐randomised studies are too prone to bias to be included in this review. However, in the risk of bias assessment, selection bias is not deemed plausible in spite of total lack of randomization and allocation concealment in many studies. In our view, this does not justify the exclusion of non‐randomised studies because this would be exactly the bias that you would expect from these studies. Including non‐randomised studies would certainly have increased the number of included studies and could have possibly affected the conclusions as well. In any case, it would have been helpful to have a definition of a randomized study because this is not self‐evident.
3. Is the quality of the evidence high?
The quality of evidence is rated as high based on the lack of selection bias in the included studies. The rating of high quality evidence means that it is very unlikely that future studies will change this result. However, in the conclusions, the authors state that the results of an ongoing study should be waited before final conclusions can be drawn. Given the uncertainty surrounding many of the older studies, we believe that this conclusion is justified and as such that the quality of the review evidence cannot be rated as high. Moreover, we wondered why the authors did not address publication bias. From the two studies that did not report their results in any form, it can be inferred that this must be a major factor. We believe consideration of these factors reduce the quality of the evidence to a lower level.
4. Should health checks only be carried out as part of an RCT?
The authors recommend that general health checks should only be evaluated as part of an RCT. We thought that Cochrane Reviews in general would not make recommendation to use or not use a certain health care intervention as the applicability of the evidence can vary in different settings. As the review did not find any harms, we don't see a reason why there should be a recommendation against the use of health checks.
References
Schwartz LM, Woloshin S, Fowler FJ Jr, Welch HG. Enthusiasm for cancer screening in the United States. JAMA. 2004 Jan 7;291(1):71‐8.
Oboler SK, Prochazka AV, Gonzales R, Xu S, Anderson RJ. Public expectations and attitudes for annual physical examinations and testing. Ann Intern Med.2002 May 7;136(9):652‐9
We agree with the conflict of interest statement below:
We certify that I have no affiliations with or involvement in any organization or entity with a financial interest in the subject matter of my feedback.
Reply
We would like to thank Jos Verbeek, Sharea Ijaz, Jani Ruotsalainen, and Christina Mischke for their comments and interest in our review.
1. The feedback authors write that we excluded trials that reported on morbidity and not on mortality. This is not correct. Indeed, we included and analysed several trials which did not report on mortality. Fourteen of the 16 included trials presented data on one or more of our pre‐specified outcomes and 9 of these had mortality data. We collected and presented data on morbidity from all trials under the heading ‘Morbidity’ in the results section. However, results on this outcome were surprisingly scarce and not reported in all trials.
Contrary to what Verbeek et al. seem to believe, we did not include trials with a ‘total lack of randomisation’. As we explain in the ‘risk of bias’ section, we rated trials as ‘low risk’ if they used a predictable sequence, such as date of birth, when the process used was likely to yield comparable groups and when all participants were allocated at once. Using such randomisation methods is acceptable if strictly implemented, which they often are in screening trials. The situation is very different from usual clinical trials where a clinician enrols one patient at a time, because of the predictability of the sequence, which can lead to severe bias. However, when all participants are allocated at the same time and before they are contacted, this concern doesn't exist.
We did note that some of the trials we included were not described as randomised trials, despite being experiments allocating participants to an intervention and a control arm through an unbiased process that can be considered random allocation. This oversight on part of the study authors makes these studies difficult to find; indeed some of them have been cited astonishingly little.
Verbeek et al. suggest that we should have included observational studies in the review. Cochrane reviews should not include non‐randomised studies in an area where randomised trials are feasible, and where the expected beneficial effects are small, because observational studies are too bias‐prone. A possible exception applies to harms, where less stringent criteria could be applied, and we will consider doing this in an update.
2. We assume that Verbeek et al. refer to the GRADE scores used in our summary of findings table when they argue that uncertainty about the results of future trials means that we should downgrade the currently available evidence from a “high” rating. They write: “However, in the conclusions, the authors state that the results of an ongoing study should be awaited before final conclusions can be drawn”.
This is not correct. We wrote that if the Inter99 trial (a recent trial that will soon report results) also shows no effect, then there is no reason to do further trials. This statement was about future research and did not relate to our conclusion about implications for practice. We concluded that systematic health checks for general adult populations are not supported by the available evidence, based on the simple fact that we could not find beneficial effects. We have no reason to believe that this would be different in trials performed today, as there was no indication of an effect in newer trials. We explain this in detail in the discussion section of the review. Furthermore, we have been informed that the Inter99 trial did not find beneficial effects of health checks either.
We agree with Verbeek et al. that publication bias is important, and we highlighted this by including and describing eligible trials with missing data. Verbeek et al. suggest that publication bias increases the uncertainty surrounding our results, but publication bias almost always favours the studied intervention. It is highly unlikely that the two trials in question did not publish results because they showed beneficial effects.
3. Verbeek et al. do not agree with our conclusions. The ‘Implications for practice’ section consists of three sentences. The first sentence states that our results do not support the use of general health checks outside the context of randomised trials, which is a simple fact and not a recommendation. The second sentence cautiously highlights that our results do not apply to opportunistic screening. The last clause in the third sentence emphasises that private suppliers of health checks do so without support from the best available evidence; this is also a statement of fact and not a recommendation.
In the third sentence, we write that ‘public healthcare initiatives to systematically offer general health checks should be resisted’. This is the logical implication of the available evidence since few would disagree that screening programmes should be based on trial evidence of a favourable balance between benefits and harms. We present strong evidence that there is little or no benefit, and some evidence of harm.
Verbeek et al. state that we did not find evidence of harms, but harms were infrequently studied which is a very different thing. This should not lead to a conclusion that harms were absent or infrequent, but should lead to concern about our lack of knowledge about the harms. We did find evidence of more diagnoses, and when we have strong evidence that benefits are very small or absent, these diagnoses represent over‐diagnosis. This may lead to overtreatment and in fact, we found an increased use of antihypertensives in some trials. Important potentially harmful outcomes were not reported at all, such as the number of follow‐up tests (some of which are invasive), the amount of surgery used, and measures of psychological distress at short or intermediate follow‐up.
The harms of labelling were poorly elucidated in the trials. Some observational studies have found important harmful effects. A 1984 study of Canadian steel workers showed that those labelled as patients with hypertension through screening had increased absenteeism from work and suffered a decline in marital adjustment, and in the fifth year after screening they earned $1093 less than colleagues who five years earlier had comparable wages (Johnston 1984) This effect on income was seen even in those who did not take their antihypertensive drug. Another study found important detrimental effects of antihypertensives on quality of life when asking the patients' spouses (Jachuk 1982). It is possible that some of the harms of labelling and treatment of elevated risk factors may be difficult to detect unless specifically looked for, as was the case with muscle problems and fatigue from statin treatment (Golomb 2012). We have started a study of the harms caused by health checks as reported in observational studies.
References
1. Johnston ME, Gibson ES, Terry CW et al. Effects of labelling on income, work and social function among hypertensive employees. J Chronic Dis 1984; 37:417‐23.
2. Jachuk SJ, Brierley H, Jachuk S, Willcox PM. The effect of hypotensive drugs on the quality of life. J R Coll Gen Pract 1982;32(235):103‐5.
3. Golomb BA, Evans MA, Dimsdale JE, White HL. Effects of statins on energy and fatigue with exertion: results from a randomized controlled trial. Arch Intern Med. 2012 Aug 13;172(15):1180‐2.
Contributors
Feedback from:
Jos Verbeek, Sharea Ijaz, Jani Ruotsalainen, and Christina Mischke, Cochrane Occupational Safety and Health Group.
Response to feedback from:
Lasse T Krogsbøll, Karsten Juhl Jørgensen, Christian Grønhøj Larsen, Peter C Gøtzsche, The Nordic Cochrane Centre.
What's new
| Date | Event | Description |
|---|---|---|
| 31 January 2018 | New search has been performed | This is the first update of the Cochrane Review published in 2012. We conducted a new search and updated other content. |
| 31 January 2018 | New citation required but conclusions have not changed | We identified one new trial and included mortality data from one already included trial. |
Acknowledgements
We thank the trial authors who helped us: Guy De Backer, Walter W Holland, Sven‐Olof Isacsson, Torben Jørgensen, Olof Lannerstad, Torsten Lauritzen, David Murray, Charlotta Pisinger, Lennart Welin, and Lars Wilhelmsen for additional information on their trials; and David Mant, Alice Fuller, Holger Theobald, Tea Skaarup, and Janus L Thomsen for providing unpublished outcome data.
We also thank the EPOC Information Specialist, Paul Miller, for designing and conducting the updated searches, and Michelle Fiander for designing and conducting the original search, as well as the editor (Denise O'Connor), managing editors (Julia Worswick and Jia Xi Han), and the peer reviewers (Sheila Page and Janet Wale) for their valuable comments.
We would like to acknowledge the National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane Effective Practice and Organisation of Care. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Appendices
Appendix 1. Search strategies
Medline (Ovid)
Ovid MEDLINE(R) Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily, Ovid MEDLINE and Versions(R) 1946 to January 24, 2018
| No. | Search terms | Results |
| 1 | physical examination/ and ((annual or gp or periodic or yearly or routine).ti. or ((primary adj2 (care or healthcare)) or primary health* or general practitioner? or general practice or family doctor? or family practice? or family physician?).ti,ab.) | 2518 |
| 2 | (health check* or healthcheck* or annual physical? or annual medical or medical check* or primary care check* or wellness check* or well care or wellcare or well woman or well visit?).ti. | 1250 |
| 3 | ((annual or periodic or regular or routine or yearly) and (check* or health* exam* or health evaluation? or medical exam* or physical? exam* or wellness check* or gp visit? or physician? visit? or doctor? visit? or office visit?)).ti. | 1036 |
| 4 | ((annual or yearly) adj2 (medical? or physical?)).ti. | 321 |
| 5 | ((annual or yearly) and visit?).ti. | 85 |
| 6 | (preventive? and (care check* or checkup? or check‐up? or visit? or exam* or family doctor? or gp or family physician? or general practitioner?)).ti. | 951 |
| 7 | ((multifactor* or multi‐factor*) adj5 prevent*).ti,ab. | 587 |
| 8 | (multiphasic adj2 (screening or test* or check*)).ti,ab. | 591 |
| 9 | comprehensive health test.ti,ab. | 1 |
| 10 | general health screening.ti,ab. | 123 |
| 11 | multiphasic screening/ | 1082 |
| 12 | ((diet or smoking or exercise or lifestyle or weight reduction or physical activity) and (screen* or check?) and (prevention or preventive or preventative)).ti,ab,hw. | 6239 |
| 13 | or/1‐12 | 13270 |
| 14 | mass screening/ | 92462 |
| 15 | ((general or prevent* or systematic or annual or yearly or periodic or regular or routine) adj5 (screen* or check? or checkup? or check‐up?)).ti,ab. | 43412 |
| 16 | (health check* or health screen*).ti,ab. | 8610 |
| 17 | or/14‐16 | 131434 |
| 18 | exp primary health care/ | 133960 |
| 19 | family practice/ | 63685 |
| 20 | physicians, primary care/ | 2461 |
| 21 | general practice/ | 11224 |
| 22 | physicians, family/ | 15722 |
| 23 | general practitioners/ | 5889 |
| 24 | exp outpatient clinics, hospital/ | 16432 |
| 25 | ambulatory care/ | 39769 |
| 26 | exp ambulatory care facilities/ | 50872 |
| 27 | exp community health services/ | 275718 |
| 28 | exp community health centers/ | 11479 |
| 29 | ((primary or communit*) adj5 (care or health*)).ti,ab. | 199287 |
| 30 | (family practi* or family doctor* or family physician* or gp* or general practi*).ti,ab. | 232557 |
| 31 | ((outpatient? or ambulatory) adj2 (care or healthcare or clinic? or service? or facilit*)).ti,ab. | 51853 |
| 32 | or/18‐31 | 840499 |
| 33 | 17 and 32 | 21387 |
| 34 | 13 or 33 | 33148 |
| 35 | exp randomized controlled trial/ | 452334 |
| 36 | controlled clinical trial.pt. | 92108 |
| 37 | randomi#ed.ti,ab. | 515152 |
| 38 | placebo.ab. | 185896 |
| 39 | randomly.ti,ab. | 284700 |
| 40 | Clinical Trials as topic.sh. | 182333 |
| 41 | trial.ti. | 176954 |
| 42 | or/35‐41 | 1165471 |
| 43 | exp animals/ not humans/ | 4418500 |
| 44 | 42 not 43 | 1074971 |
| 45 | 34 and 44 | 3608 |
| 46 | (2012* or 2013* or 2014* or 2015* or 2016* or 2017* or 2018*).dc,dp,ed,ep,yr. | 7162115 |
| 47 | 45 and 46 | 1380 |
Embase (Ovid)
Embase <1974 to 2018 January 30>
| No. | Search terms | Results |
| 1 | physical examination/ and ((annual or gp or periodic or yearly or routine).ti. or ((primary adj2 (care or healthcare)) or primary health* or general practitioner? or general practice or family doctor? or family practice? or family physician?).ti,ab.) | 4493 |
| 2 | (health check* or healthcheck* or annual physical? or annual medical or medical check* or primary care check* or wellness check* or well care or wellcare or well woman or well visit?).ti. | 1573 |
| 3 | ((annual or periodic or regular or routine or yearly) and (check* or health* exam* or health evaluation? or medical exam* or physical? exam* or wellness check* or gp visit? or physician? visit? or doctor? visit? or office visit?)).ti. | 1059 |
| 4 | ((annual or yearly) adj2 (medical? or physical?)).ti. | 268 |
| 5 | ((annual or yearly) and visit?).ti. | 120 |
| 6 | (preventive? and (care check* or checkup? or check‐up? or visit? or exam* or family doctor? or gp or family physician? or general practitioner?)).ti. | 957 |
| 7 | ((multifactor* or multi‐factor*) adj5 prevent*).ti,ab. | 731 |
| 8 | (multiphasic adj2 (screening or test* or check*)).ti,ab. | 676 |
| 9 | comprehensive health test.ti,ab. | 2 |
| 10 | general health screening.ti,ab. | 174 |
| 11 | multiphasic screening/ | 15 |
| 12 | ((diet or smoking or exercise or lifestyle or weight reduction or physical activity) and (screen* or check?) and (prevention or preventive or preventative)).ti,ab,hw. | 12703 |
| 13 | or/1‐12 | 21730 |
| 14 | mass screening/ | 53764 |
| 15 | ((general or prevent* or systematic or annual or yearly or periodic or regular or routine) adj5 (screen* or check? or checkup? or check‐up?)).ti,ab. | 61653 |
| 16 | (health check* or health screen*).ti,ab. | 11760 |
| 17 | or/14‐16 | 116488 |
| 18 | exp primary health care/ | 142065 |
| 19 | general practice/ | 77361 |
| 20 | general practitioner/ | 83925 |
| 21 | outpatient department/ | 55726 |
| 22 | outpatient care/ | 30596 |
| 23 | ambulatory care/ | 34813 |
| 24 | community care/ | 54643 |
| 25 | ((primary or communit*) adj5 (care or health*)).ti,ab. | 252747 |
| 26 | (family practi* or family doctor* or family physician* or gp* or general practi*).ti,ab. | 295621 |
| 27 | ((outpatient? or ambulatory) adj2 (care or healthcare or clinic? or service? or facilit*)).ti,ab. | 79745 |
| 28 | or/18‐27 | 777786 |
| 29 | 17 and 28 | 14822 |
| 30 | 13 or 29 | 35019 |
| 31 | random*.ti,ab. | 1261286 |
| 32 | factorial*.ti,ab. | 31877 |
| 33 | (crossover* or cross over*).ti,ab. | 91823 |
| 34 | ((doubl* or singl*) adj blind*).ti,ab. | 204152 |
| 35 | (assign* or allocat* or volunteer* or placebo*).ti,ab. | 881486 |
| 36 | crossover procedure/ | 54107 |
| 37 | single blind procedure/ | 30231 |
| 38 | randomized controlled trial/ | 485121 |
| 39 | double blind procedure/ | 145706 |
| 40 | or/31‐39 | 1952647 |
| 41 | exp animal/ not human/ | 4784380 |
| 42 | 40 not 41 | 1757385 |
| 43 | 30 and 42 | 4929 |
| 44 | limit 43 to yr="2012 ‐Current" | 2164 |
The Cochrane Library (Wiley)
| No. | Search terms | Results |
| #1 | [mh "physical examination"] and ((annual or gp or periodic or yearly or routine):ti or ((primary near/2 (care or healthcare)) or primary next health* or general next practitioner? or general next practice or family next doctor? or family next practice? or family next physician?):ti,ab) | 1581 |
| #2 | (health next check* or healthcheck* or annual next physical? or annual next medical or medical next check* or primary next care next check* or wellness next check* or well next care or wellcare or well next woman or well next visit?):ti | 67 |
| #3 | ((annual or periodic or regular or routine or yearly) and (check* or health* next exam* or health next evaluation? or medical next exam* or physical? next exam* or wellness next check* or gp next visit? or physician? next visit? or doctor? next visit? or office next visit?)):ti | 33 |
| #4 | ((annual or yearly) near/2 (medical? or physical?)):ti,ab | 0 |
| #5 | ((annual or yearly) and visit?):ti | 1 |
| #6 | (preventive? and (care next check* or checkup? or check‐up? or visit? or exam* or family doctor? or gp or family next physician? or general next practitioner?)):ti | 0 |
| #7 | ((multifactor* or multi‐factor*) near/5 prevent*):ti,ab | 170 |
| #8 | (multiphasic near/2 (screening or test* or check*)):ti,ab | 19 |
| #9 | comprehensive health test:ti,ab | 1 |
| #10 | general health screening:ti,ab | 11 |
| #11 | [mh "multiphasic screening"] | 16 |
| #12 | ((diet or smoking or exercise or lifestyle or weight next reduction or physical next activity) and (screen* or check?) and (prevention or preventive or preventative)):ti,ab,kw | 920 |
| #13 | {or #1‐#12} | 2737 |
| #14 | [mh "mass screening"] | 5774 |
| #15 | ((general or prevent* or systematic or annual or yearly or periodic or regular or routine) near/5 (screen* or check? or checkup? or check‐up?)):ti,ab | 2866 |
| #16 | (health next check* or health next screen*):ti,ab | 464 |
| #17 | {or #14‐#16} | 8202 |
| #18 | [mh "primary health care"] | 7246 |
| #19 | [mh "family practice"] | 2209 |
| #20 | [mh "physicians, primary care"] | 142 |
| #21 | [mh "general practice"] | 2616 |
| #22 | [mh "physicians, family"] | 486 |
| #23 | [mh "general practitioners"] | 210 |
| #24 | [mh "outpatient clinics, hospital"] | 712 |
| #25 | [mh "ambulatory care"] | 3877 |
| #26 | [mh "ambulatory care facilities"] | 1943 |
| #27 | [mh "community health services"] | 13670 |
| #28 | [mh "community health centers"] | 589 |
| #29 | ((primary or communit*) near/5 (care or health*)):ti,ab | 22011 |
| #30 | (family next practi* or family next doctor* or family next physician* or gp* or general next practi*):ti,ab | 13034 |
| #31 | ((outpatient? or ambulatory) near/2 (care or healthcare or clinic? or service? or facilit*)):ti,ab | 815 |
| #32 | {or #18‐#31} | 49879 |
| #33 | #17 and #32 | 1960 |
| #34 | #13 or #33 | 4494 |
| #35 | #13 or #33 Publication Year from 2012 to 2018 | 1890 |
CINAHL (Ebsco)
| No. | Search terms | Results |
| S1 | (MH "Physical Examination+") AND ( TI ((annual or gp or periodic or yearly or routine) ) | 508 |
| S2 | (MH "Physical Examination+") AND ( TI ((primary N2 (care or healthcare) or primary health* or general practitioner? or general practice or family doctor? or family practice? or family physician?)) or AB ((primary N2 (care or healthcare) or primary health* or general practitioner? or general practice or family doctor? or family practice? or family physician?)) ) | 1,527 |
| S3 | TI (health check* or healthcheck* or annual physical? or annual medical or medical check* or primary care check* or wellness check* or well care or wellcare or well woman or well visit?) | 1,615 |
| S4 | TI ((annual or periodic or regular or routine or yearly) and (check* or health* exam* or health evaluation? or medical exam* or physical? exam* or wellness check* or gp visit? or physician? visit? or doctor? visit? or office visit?)) | 255 |
| S5 | TI ((annual or yearly) N2 (medical? or physical?)) | 11 |
| S6 | TI ((annual or yearly) and visit?) | 48 |
| S7 | TI (preventive? and (care check* or checkup? or check‐up? or visit? or exam* or family doctor? or gp or family physician? or general practitioner?)) | 0 |
| S8 | TI (preventive? and (care check* or checkup? or check‐up? or visit? or exam* or family doctor? or gp or family physician? or general practitioner?)) | 289 |
| S9 | TI ((multifactor* or multi‐factor*) N5 prevent*) OR AB ((multifactor* or multi‐factor*) N5 prevent*) | 156 |
| S10 | TI ((multiphasic N2 (screening or test* or check*)) OR comprehensive health test OR general health screening) OR AB ((multiphasic N2 (screening or test* or check*)) OR comprehensive health test OR general health screening) | 168 |
| S11 | ((diet or smoking or exercise or lifestyle or weight reduction or physical activity) and (screen* or check?) and (prevention or preventive or preventative)) | 3,001 |
| S12 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 | 7,146 |
| S13 | (MH "Health Screening+") | 52,249 |
| S14 | TI (health check* or health screen*) OR AB (health check* or health screen*) | 7,223 |
| S15 | TI ((general or prevent* or systematic or annual or yearly or periodic or regular or routine) N5 (screen* or check? or checkup? or check‐up?)) OR AB ((general or prevent* or systematic or annual or yearly or periodic or regular or routine) N5 (screen* or check? or checkup? or check‐up?)) | 8,842 |
| S16 | S13 OR S14 OR S15 | 61,281 |
| S17 | MH "Primary Health Care" | 36,902 |
| S18 | MH "Family Practice" | 12,753 |
| S19 | MH "Physicians, Family" | 10,177 |
| S20 | MH "Outpatient Service" | 4,345 |
| S21 | MH "Ambulatory Care Facilities+" | 9,942 |
| S22 | MH "Ambulatory Care" | 7,041 |
| S23 | MH "Ambulatory Care Nursing" | 1,170 |
| S24 | MH "Community Health Centers+" | 3,645 |
| S25 | MH "Community Health Nursing+" | 24,267 |
| S26 | MH "Community Health Services+" | 273,950 |
| S27 | TI ((primary or communit*) N5 (care or health*)) OR AB ((primary or communit*) N5 (care or health*)) | 82,561 |
| S28 | TI (family practi* or family doctor* or family physician* or gp* or general practi*) OR AB (family practi* or family doctor* or family physician* or gp* or general practi*) | 35,041 |
| S29 | TI ((outpatient? or ambulatory) N2 (care or healthcare or clinic? or service? or facilit*)) OR AB ((outpatient? or ambulatory) N2 (care or healthcare or clinic? or service? or facilit*)) | 4,183 |
| S30 | S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 | 392,346 |
| S31 | S16 AND S30 | 53,111 |
| S32 | S16 OR S32 | 61,312 |
| S33 | PT randomized controlled trial | 41,291 |
| S34 | PT clinical trial | 55,646 |
| S35 | TI ( randomis* or randomiz* or randomly) OR AB ( randomis* or randomiz* or randomly) | 138,840 |
| S36 | (MH "Clinical Trials+") | 153,724 |
| S37 | (MH "Random Assignment") | 36,457 |
| S38 | S33 OR S34 OR S35 OR S36 OR S37 | 228,146 |
| S39 | S32 AND S38 | 4,442 |
| S40 | S39 Limiters ‐ Published Date: 20120101‐20181231; Exclude MEDLINE records | 409 |
Clinicaltrials.gov
| Search terms | Results |
| "health check" OR "health checks" OR "check ups" OR "check up" OR "checkups" OR "checkup" | |
| Limits: Interventional Studies | Adult, Senior | First posted from 01/01/2012 to 01/31/2018 | 79 |
WHO ICTRP
Search not limited by date as this is not possible on the ICTRP interface
| Search terms | Results |
| health check* | 96 |
| checkup* | 57 |
| check up* | 30 |
Appendix 2. GRADE evidence profiles
| Certainty assessment | Summary of findings | Importance | ||||||||||
| № of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | № of participants | Effect | Certainty | |||
| Health checks | Usual care | Relative (95% CI) | Absolute (95% CI) | |||||||||
| Total mortality (follow‐up: range 4 years to 30 years) | ||||||||||||
| 11 | Randomised trials | Not serious | Not serious | Not serious | Not serious | None | RR 1.00 (0.97 to 1.03) | 0 fewer per 1.000 (from 3 fewer to 3 more) | ⊕⊕⊕⊕ High | Critical | ||
| Cancer mortality (follow‐up: range 4 years to 22 years) | ||||||||||||
| 8 | Randomised trials | Not serious | Not serious | Not serious | Not serious | None | RR 1.01 (0.92 to 1.12) | 0 fewer per 1.000 (from 2 fewer to 3 more) | ⊕⊕⊕⊕ High | Critical | ||
| Cardiovascular mortality (follow‐up: range 4 years to 22 years) | ||||||||||||
| 9 | Randomised trials | Not serious | Serious | Not serious | Not serious | None | RR 1.05 (0.94 to 1.16) | 2 more per 1.000 (from 4 fewer to 3 more) | ⊕⊕⊕⊝ Moderate | Critical | ||
| Fatal and non‐fatal ischaemic heart disease (follow‐up: range 5 years to 30 years) | ||||||||||||
| 4 | Randomised trials | Not serious | Not serious | Not serious | Not serious | None | RR 0.98 (0.94 to 1.03) | 1 fewer per 1.000 (from 1 fewer to 1 fewer) | ⊕⊕⊕⊕ High | Important | ||
| Fatal and non‐fatal stroke (follow‐up: range 10 years to 30 years) | ||||||||||||
| 3 | Randomised trials | Not serious | Serious | Not serious | Not serious | None | RR 1.07 (1.00 to 1.14) | 3 more per 1.000 (from 0 fewer to 5 more) | ⊕⊕⊕⊝ Moderate | Important | ||
Data and analyses
Comparison 1. Health checks versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Total mortality | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.03] | |
| 2 Total mortality ‐ sensitivity analyses | 8 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.03] | |
| 2.1 Excluding cluster trials | 8 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.03] | |
| 3 Total mortality ‐ no. of health checks | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 3.1 One health check | 3 | Risk Ratio (Random, 95% CI) | 1.00 [0.94, 1.06] | |
| 3.2 More than one health check | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.97, 1.04] | |
| 4 Total mortality ‐ lifestyle intervention | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 4.1 Major lifestyle intervention | 5 | Risk Ratio (Random, 95% CI) | 0.99 [0.95, 1.03] | |
| 4.2 No major lifestyle intervention | 6 | Risk Ratio (Random, 95% CI) | 1.02 [0.98, 1.06] | |
| 5 Total mortality ‐ length of follow‐up | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 5.1 Up to five years | 2 | Risk Ratio (Random, 95% CI) | 1.03 [0.66, 1.60] | |
| 5.2 More than 5 years | 9 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.03] | |
| 6 Total mortality ‐ age of trial | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 6.1 Trial started before 1980 | 7 | Risk Ratio (Random, 95% CI) | 0.99 [0.95, 1.03] | |
| 6.2 Trial started after 1980 | 4 | Risk Ratio (Random, 95% CI) | 1.02 [0.96, 1.09] | |
| 7 Total mortality ‐ geographical location | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 7.1 USA | 1 | Risk Ratio (Random, 95% CI) | 0.98 [0.88, 1.09] | |
| 7.2 Europe | 10 | Risk Ratio (Random, 95% CI) | 1.01 [0.98, 1.04] | |
| 8 Total mortality ‐ examination by physician | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 8.1 Examination by physician | 5 | Risk Ratio (Random, 95% CI) | 1.00 [0.94, 1.06] | |
| 8.2 No examination by physician | 6 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.04] | |
| 9 Total mortality ‐ selection bias | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 9.1 Low risk of selection bias | 9 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.04] | |
| 9.2 Unclear risk of selection bias | 2 | Risk Ratio (Random, 95% CI) | 1.00 [0.93, 1.08] | |
| 9.3 High risk of selection bias | 0 | Risk Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 Total mortality ‐ performance bias | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 10.1 Low risk | 7 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.03] | |
| 10.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 1.02 [0.94, 1.11] | |
| 10.3 High risk | 3 | Risk Ratio (Random, 95% CI) | 1.08 [0.87, 1.33] | |
| 11 Total mortality ‐ detection bias | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 11.1 Low risk | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.97, 1.04] | |
| 11.2 Unclear risk | 2 | Risk Ratio (Random, 95% CI) | 1.00 [0.93, 1.08] | |
| 11.3 High risk | 1 | Risk Ratio (Random, 95% CI) | 0.92 [0.77, 1.10] | |
| 12 Total mortality ‐ incomplete outcome data | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 12.1 Low risk | 10 | Risk Ratio (Random, 95% CI) | 1.01 [0.98, 1.04] | |
| 12.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 0.98 [0.88, 1.09] | |
| 12.3 High risk | 0 | Risk Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 Total mortality ‐ contamination | 11 | Risk Ratio (Random, 95% CI) | 1.00 [0.98, 1.03] | |
| 13.1 Low risk | 7 | Risk Ratio (Random, 95% CI) | 1.00 [0.97, 1.03] | |
| 13.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 1.27 [0.95, 1.70] | |
| 13.3 High risk | 3 | Risk Ratio (Random, 95% CI) | 0.99 [0.90, 1.10] | |
| 14 Cancer mortality | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 15 Cancer mortality ‐ sensitivity analyses | 5 | Risk Ratio (Random, 95% CI) | 0.97 [0.85, 1.09] | |
| 15.1 Excluding cluster trials | 5 | Risk Ratio (Random, 95% CI) | 0.97 [0.85, 1.09] | |
| 16 Cancer mortality ‐ no. of health checks | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 16.1 Only one health check | 3 | Risk Ratio (Random, 95% CI) | 1.10 [1.00, 1.21] | |
| 16.2 More than one health check | 5 | Risk Ratio (Random, 95% CI) | 0.92 [0.83, 1.02] | |
| 17 Cancer mortality lifestyle intervention | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 17.1 Major lifestyle intervention | 3 | Risk Ratio (Random, 95% CI) | 1.01 [0.82, 1.24] | |
| 17.2 No major lifestyle intervention | 5 | Risk Ratio (Random, 95% CI) | 1.02 [0.91, 1.15] | |
| 18 Cancer mortality ‐ length of follow‐up | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 18.1 Up to five years | 2 | Risk Ratio (Random, 95% CI) | 1.33 [0.89, 1.99] | |
| 18.2 More than five years | 6 | Risk Ratio (Random, 95% CI) | 1.00 [0.90, 1.10] | |
| 19 Cancer mortality ‐ age of trial | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 19.1 Trial started before 1980 | 7 | Risk Ratio (Random, 95% CI) | 1.01 [0.91, 1.12] | |
| 19.2 Trial started after 1980 | 1 | Risk Ratio (Random, 95% CI) | 1.19 [0.75, 1.89] | |
| 20 Cancer mortality ‐ geographical location | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 20.1 Europe | 7 | Risk Ratio (Random, 95% CI) | 1.02 [0.91, 1.15] | |
| 20.2 USA | 1 | Risk Ratio (Random, 95% CI) | 0.98 [0.80, 1.20] | |
| 21 Cancer mortality ‐ examination by physician | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 21.1 Examination by physician | 5 | Risk Ratio (Random, 95% CI) | 1.02 [0.91, 1.15] | |
| 21.2 No examination by physician | 3 | Risk Ratio (Random, 95% CI) | 1.01 [0.82, 1.24] | |
| 22 Cancer mortality ‐ selection bias | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 22.1 Low risk | 6 | Risk Ratio (Random, 95% CI) | 0.98 [0.87, 1.10] | |
| 22.2 Unclear risk | 2 | Risk Ratio (Random, 95% CI) | 1.10 [0.98, 1.24] | |
| 22.3 High risk | 0 | Risk Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 23 Cancer mortality ‐ performance bias | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 23.1 Low risk | 5 | Risk Ratio (Random, 95% CI) | 1.00 [0.86, 1.16] | |
| 23.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 1.05 [0.88, 1.25] | |
| 23.3 High risk | 2 | Risk Ratio (Random, 95% CI) | 1.08 [0.80, 1.46] | |
| 24 Cancer mortality ‐ detection bias | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 24.1 Low risk | 5 | Risk Ratio (Random, 95% CI) | 0.99 [0.86, 1.13] | |
| 24.2 Unclear risk | 2 | Risk Ratio (Random, 95% CI) | 1.10 [0.98, 1.24] | |
| 24.3 High risk | 1 | Risk Ratio (Random, 95% CI) | 0.93 [0.63, 1.38] | |
| 25 Cancer mortality ‐ incomplete outcome data | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 25.1 Low risk | 6 | Risk Ratio (Random, 95% CI) | 0.98 [0.86, 1.12] | |
| 25.2 Unclear risk | 2 | Risk Ratio (Random, 95% CI) | 1.07 [0.96, 1.20] | |
| 25.3 High risk | 0 | Risk Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26 Cancer mortality ‐ contamination | 8 | Risk Ratio (Random, 95% CI) | 1.01 [0.92, 1.12] | |
| 26.1 Low risk | 5 | Risk Ratio (Random, 95% CI) | 1.01 [0.88, 1.17] | |
| 26.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 1.19 [0.75, 1.89] | |
| 26.3 High risk | 2 | Risk Ratio (Random, 95% CI) | 0.99 [0.82, 1.18] | |
| 27 Cardiovascular mortality | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 28 Cardiovascular mortality ‐ sensitivity analyses | 6 | Risk Ratio (Random, 95% CI) | 1.02 [0.92, 1.13] | |
| 28.1 Excluding cluster trials | 6 | Risk Ratio (Random, 95% CI) | 1.02 [0.92, 1.13] | |
| 29 Cardiovascular mortality ‐ no. of health checks | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 29.1 Only one health check | 3 | Risk Ratio (Random, 95% CI) | 0.89 [0.69, 1.14] | |
| 29.2 More than one health check | 6 | Risk Ratio (Random, 95% CI) | 1.10 [0.98, 1.23] | |
| 30 Cardiovascular mortality lifestyle intervention | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 30.1 Major lifestyle intervention | 3 | Risk Ratio (Random, 95% CI) | 0.99 [0.86, 1.15] | |
| 30.2 No major lifestyle intervention | 6 | Risk Ratio (Random, 95% CI) | 1.07 [0.93, 1.23] | |
| 31 Cardiovascular mortality ‐ length of follow‐up | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 31.1 Up to five years | 2 | Risk Ratio (Random, 95% CI) | 0.84 [0.22, 3.18] | |
| 31.2 More than five years | 7 | Risk Ratio (Random, 95% CI) | 1.05 [0.97, 1.13] | |
| 32 Cardiovascular mortality ‐ age of trial | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 32.1 Trial started before 1980 | 7 | Risk Ratio (Random, 95% CI) | 1.01 [0.90, 1.13] | |
| 32.2 Trial started after 1980 | 2 | Risk Ratio (Random, 95% CI) | 1.24 [0.89, 1.72] | |
| 33 Cardiovascular mortality ‐ geographical location | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 33.1 Europe | 8 | Risk Ratio (Random, 95% CI) | 1.05 [0.93, 1.18] | |
| 33.2 USA | 1 | Risk Ratio (Random, 95% CI) | 1.01 [0.85, 1.20] | |
| 34 Cardiovascular mortality ‐ examination by physician | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 34.1 Examination by physician | 5 | Risk Ratio (Random, 95% CI) | 1.03 [0.84, 1.27] | |
| 34.2 No examination by physician | 4 | Risk Ratio (Random, 95% CI) | 1.04 [0.92, 1.17] | |
| 35 Cardiovascular mortality ‐ selection bias | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 35.1 Low risk | 7 | Risk Ratio (Random, 95% CI) | 1.04 [0.93, 1.16] | |
| 35.2 Unclear risk | 2 | Risk Ratio (Random, 95% CI) | 1.17 [0.71, 1.91] | |
| 35.3 High risk | 0 | Risk Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 36 Cardiovascular mortality ‐ performance bias | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 36.1 Low risk | 6 | Risk Ratio (Random, 95% CI) | 0.99 [0.89, 1.11] | |
| 36.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 1.05 [0.91, 1.21] | |
| 36.3 High risk | 2 | Risk Ratio (Random, 95% CI) | 1.57 [1.18, 2.09] | |
| 37 Cardiovascular mortality ‐ detection bias | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 37.1 Low risk | 6 | Risk Ratio (Random, 95% CI) | 1.03 [0.91, 1.16] | |
| 37.2 Unclear risk | 2 | Risk Ratio (Random, 95% CI) | 1.17 [0.71, 1.91] | |
| 37.3 High risk | 1 | Risk Ratio (Random, 95% CI) | 1.09 [0.83, 1.43] | |
| 38 Cardiovascular mortality ‐ incomplete outcome data | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 38.1 Low risk | 8 | Risk Ratio (Random, 95% CI) | 1.05 [0.93, 1.18] | |
| 38.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 1.01 [0.85, 1.20] | |
| 38.3 High risk | 0 | Risk Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 39 Cardiovascular mortality ‐ contamination | 9 | Risk Ratio (Random, 95% CI) | 1.05 [0.94, 1.16] | |
| 39.1 Low risk | 6 | Risk Ratio (Random, 95% CI) | 1.00 [0.90, 1.12] | |
| 39.2 Unclear risk | 1 | Risk Ratio (Random, 95% CI) | 1.64 [0.97, 2.76] | |
| 39.3 High risk | 2 | Risk Ratio (Random, 95% CI) | 1.21 [0.81, 1.83] | |
| 40 Fatal and non‐fatal ischaemic heart disease | 4 | Risk Ratio (Random, 95% CI) | 0.98 [0.94, 1.03] | |
| 41 Fatal and non‐fatal stroke | 3 | Risk Ratio (Random, 95% CI) | 1.05 [0.95, 1.17] |
1.2. Analysis.
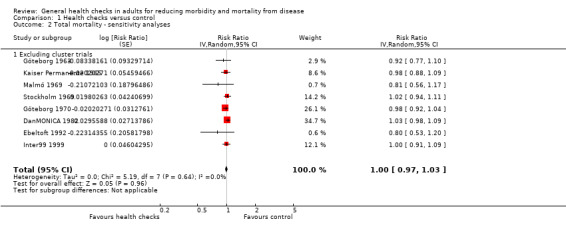
Comparison 1 Health checks versus control, Outcome 2 Total mortality ‐ sensitivity analyses.
1.3. Analysis.
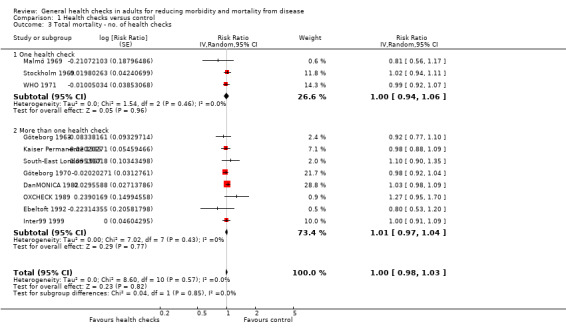
Comparison 1 Health checks versus control, Outcome 3 Total mortality ‐ no. of health checks.
1.4. Analysis.
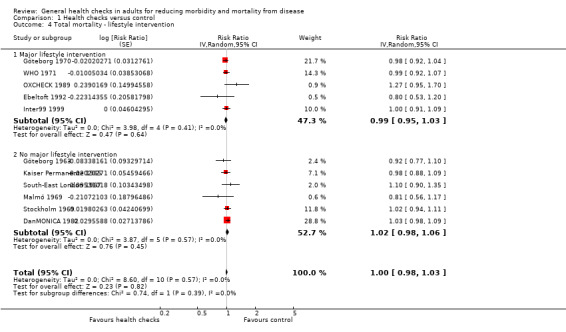
Comparison 1 Health checks versus control, Outcome 4 Total mortality ‐ lifestyle intervention.
1.5. Analysis.
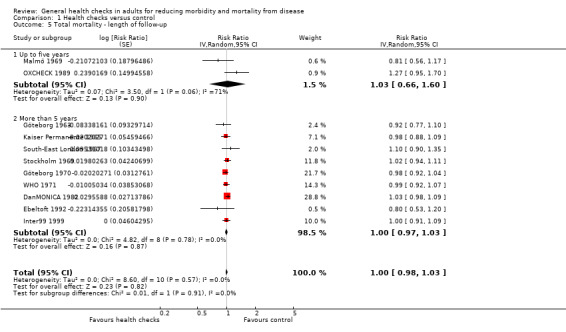
Comparison 1 Health checks versus control, Outcome 5 Total mortality ‐ length of follow‐up.
1.6. Analysis.
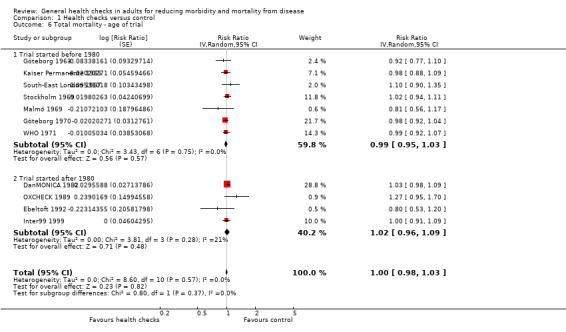
Comparison 1 Health checks versus control, Outcome 6 Total mortality ‐ age of trial.
1.7. Analysis.
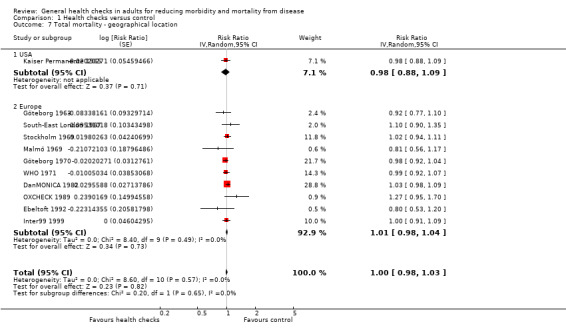
Comparison 1 Health checks versus control, Outcome 7 Total mortality ‐ geographical location.
1.8. Analysis.
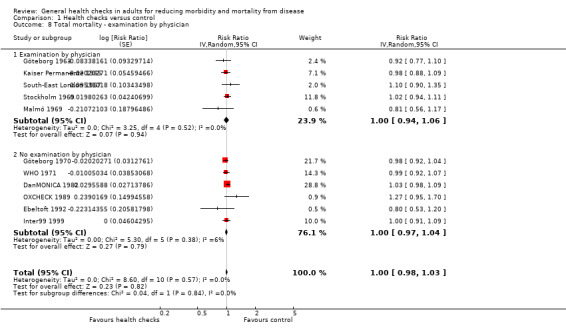
Comparison 1 Health checks versus control, Outcome 8 Total mortality ‐ examination by physician.
1.9. Analysis.
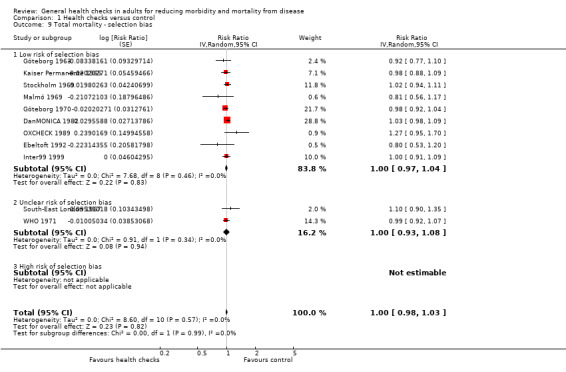
Comparison 1 Health checks versus control, Outcome 9 Total mortality ‐ selection bias.
1.10. Analysis.
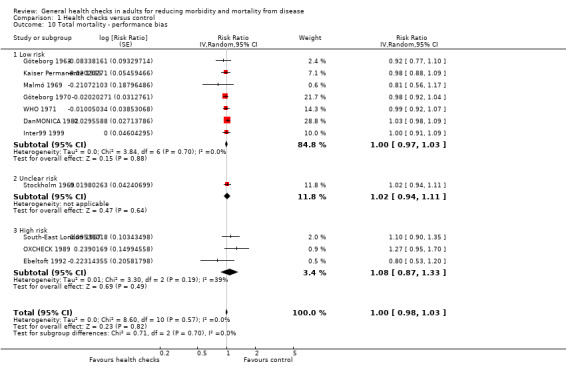
Comparison 1 Health checks versus control, Outcome 10 Total mortality ‐ performance bias.
1.11. Analysis.
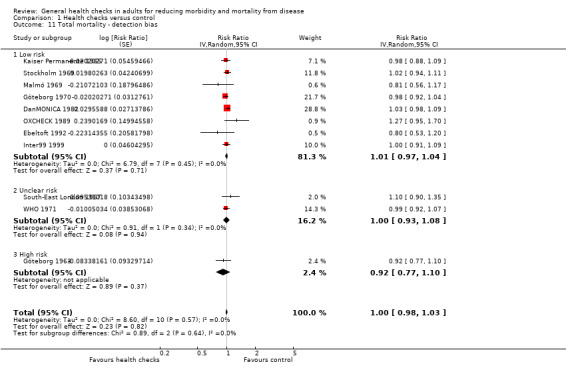
Comparison 1 Health checks versus control, Outcome 11 Total mortality ‐ detection bias.
1.12. Analysis.
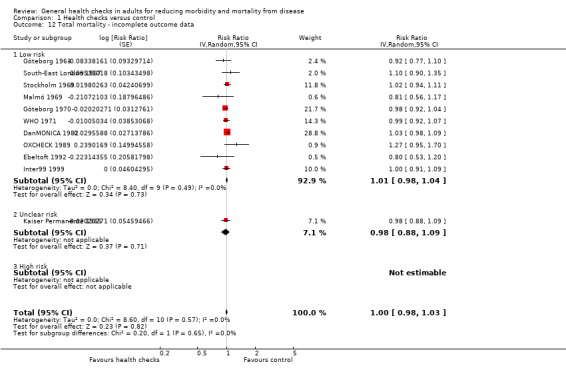
Comparison 1 Health checks versus control, Outcome 12 Total mortality ‐ incomplete outcome data.
1.13. Analysis.
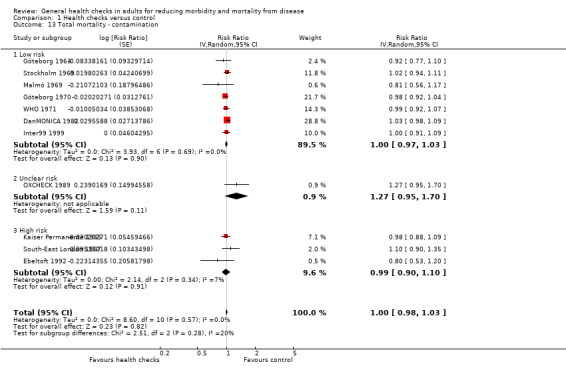
Comparison 1 Health checks versus control, Outcome 13 Total mortality ‐ contamination.
1.15. Analysis.
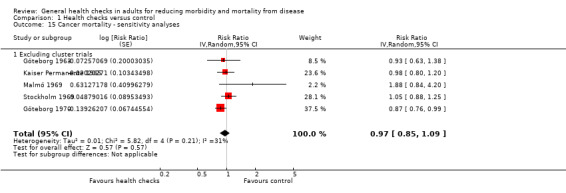
Comparison 1 Health checks versus control, Outcome 15 Cancer mortality ‐ sensitivity analyses.
1.16. Analysis.
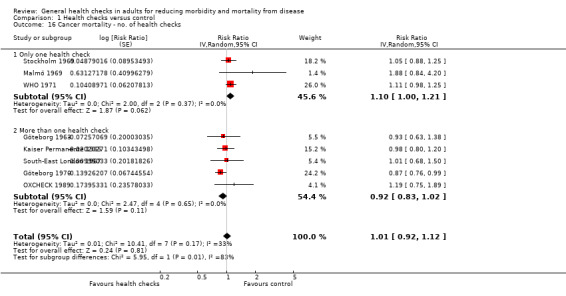
Comparison 1 Health checks versus control, Outcome 16 Cancer mortality ‐ no. of health checks.
1.17. Analysis.
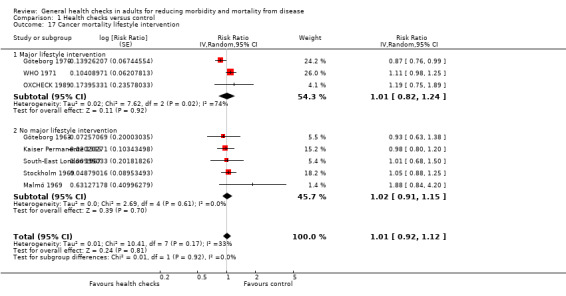
Comparison 1 Health checks versus control, Outcome 17 Cancer mortality lifestyle intervention.
1.18. Analysis.
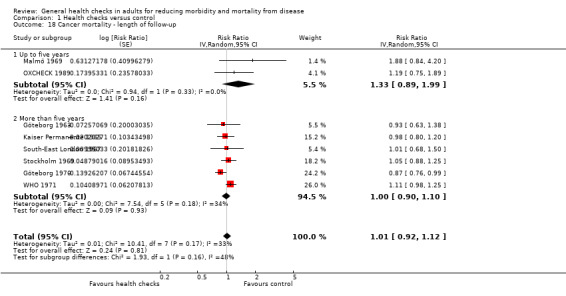
Comparison 1 Health checks versus control, Outcome 18 Cancer mortality ‐ length of follow‐up.
1.19. Analysis.
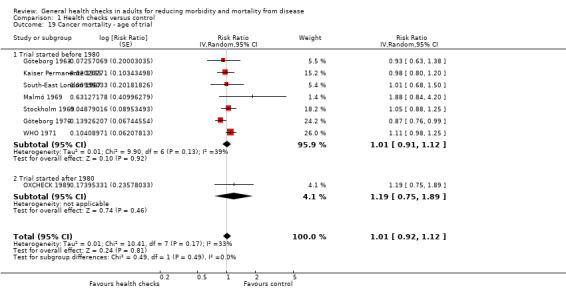
Comparison 1 Health checks versus control, Outcome 19 Cancer mortality ‐ age of trial.
1.20. Analysis.
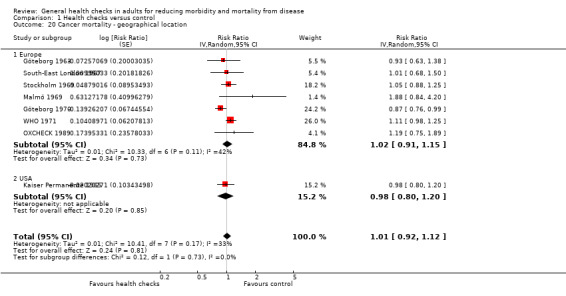
Comparison 1 Health checks versus control, Outcome 20 Cancer mortality ‐ geographical location.
1.21. Analysis.
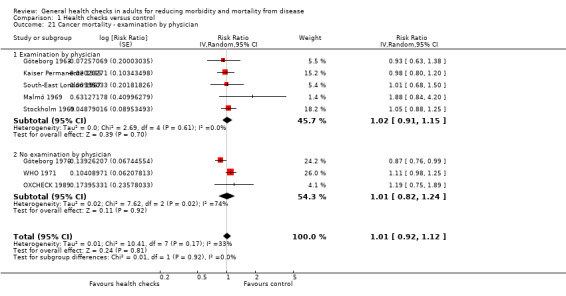
Comparison 1 Health checks versus control, Outcome 21 Cancer mortality ‐ examination by physician.
1.22. Analysis.
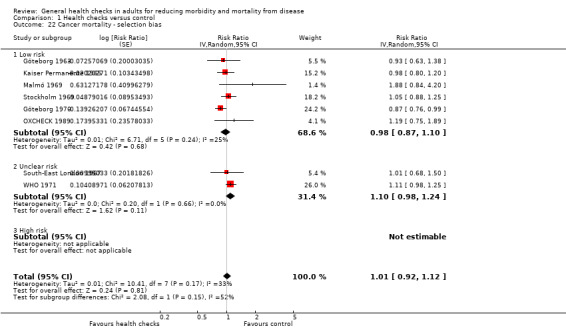
Comparison 1 Health checks versus control, Outcome 22 Cancer mortality ‐ selection bias.
1.23. Analysis.
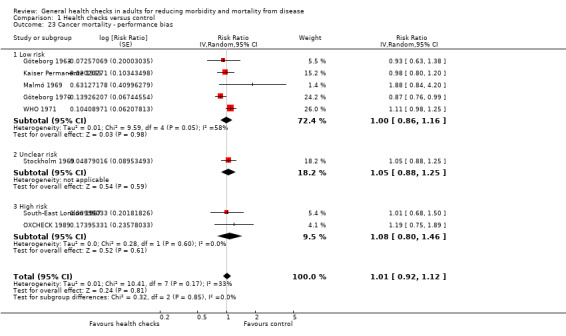
Comparison 1 Health checks versus control, Outcome 23 Cancer mortality ‐ performance bias.
1.24. Analysis.
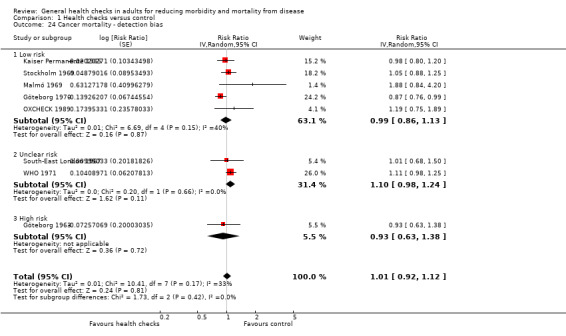
Comparison 1 Health checks versus control, Outcome 24 Cancer mortality ‐ detection bias.
1.25. Analysis.
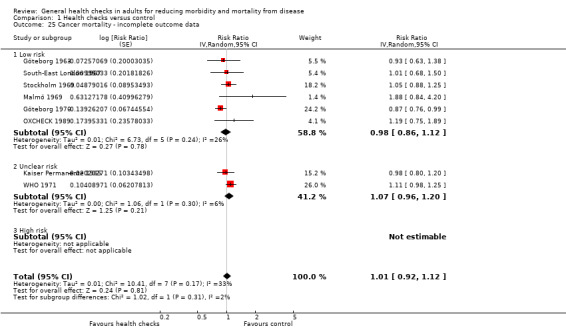
Comparison 1 Health checks versus control, Outcome 25 Cancer mortality ‐ incomplete outcome data.
1.26. Analysis.
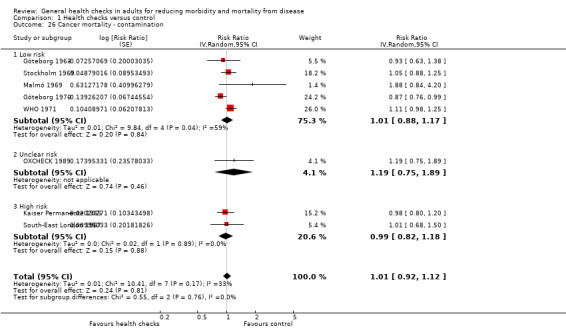
Comparison 1 Health checks versus control, Outcome 26 Cancer mortality ‐ contamination.
1.28. Analysis.
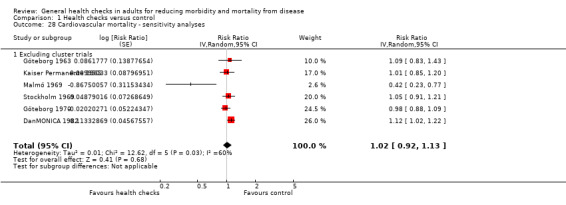
Comparison 1 Health checks versus control, Outcome 28 Cardiovascular mortality ‐ sensitivity analyses.
1.29. Analysis.
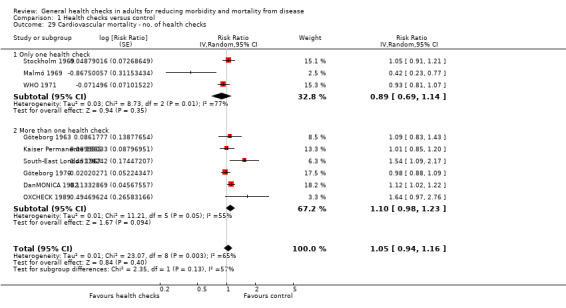
Comparison 1 Health checks versus control, Outcome 29 Cardiovascular mortality ‐ no. of health checks.
1.30. Analysis.
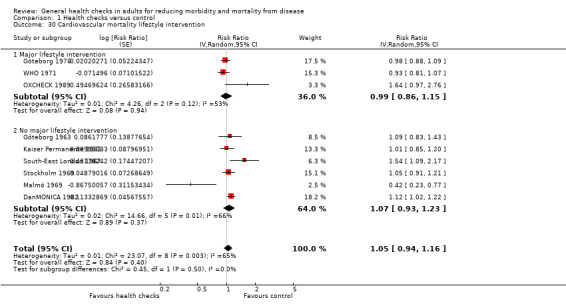
Comparison 1 Health checks versus control, Outcome 30 Cardiovascular mortality lifestyle intervention.
1.31. Analysis.
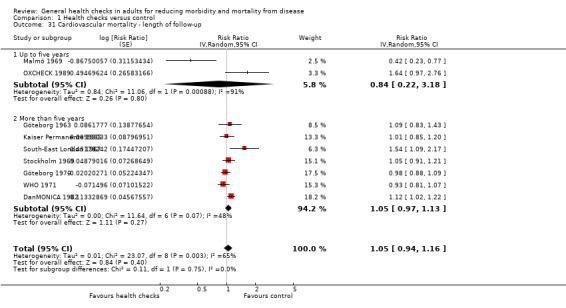
Comparison 1 Health checks versus control, Outcome 31 Cardiovascular mortality ‐ length of follow‐up.
1.32. Analysis.
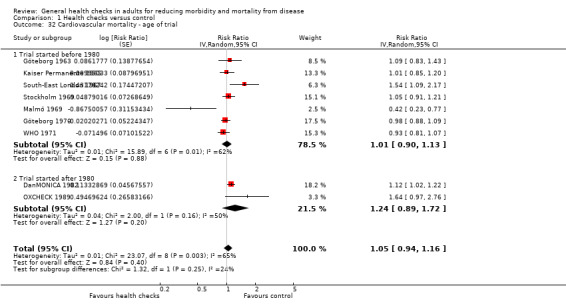
Comparison 1 Health checks versus control, Outcome 32 Cardiovascular mortality ‐ age of trial.
1.33. Analysis.
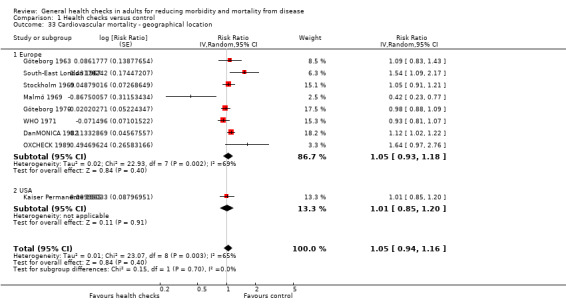
Comparison 1 Health checks versus control, Outcome 33 Cardiovascular mortality ‐ geographical location.
1.34. Analysis.
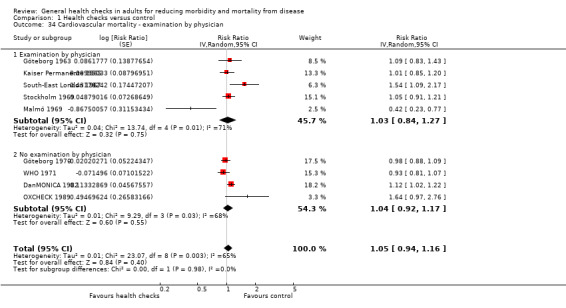
Comparison 1 Health checks versus control, Outcome 34 Cardiovascular mortality ‐ examination by physician.
1.35. Analysis.
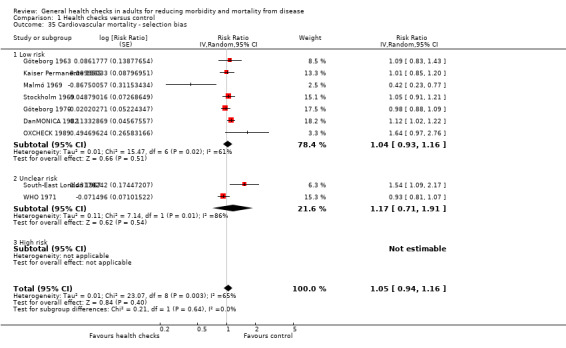
Comparison 1 Health checks versus control, Outcome 35 Cardiovascular mortality ‐ selection bias.
1.36. Analysis.
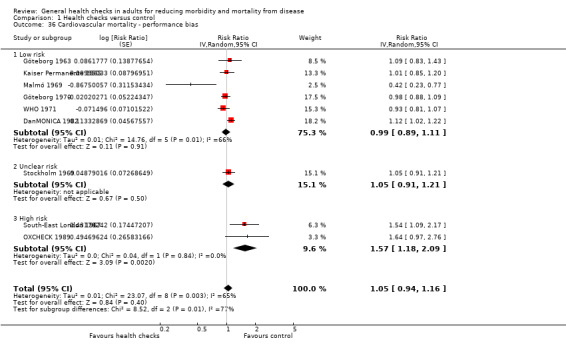
Comparison 1 Health checks versus control, Outcome 36 Cardiovascular mortality ‐ performance bias.
1.37. Analysis.
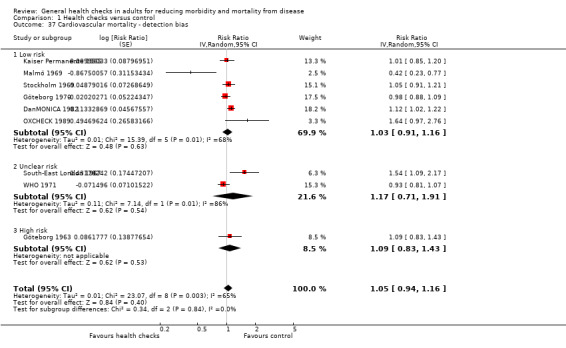
Comparison 1 Health checks versus control, Outcome 37 Cardiovascular mortality ‐ detection bias.
1.38. Analysis.
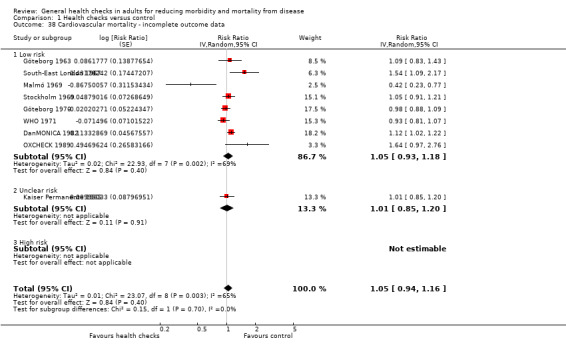
Comparison 1 Health checks versus control, Outcome 38 Cardiovascular mortality ‐ incomplete outcome data.
1.39. Analysis.
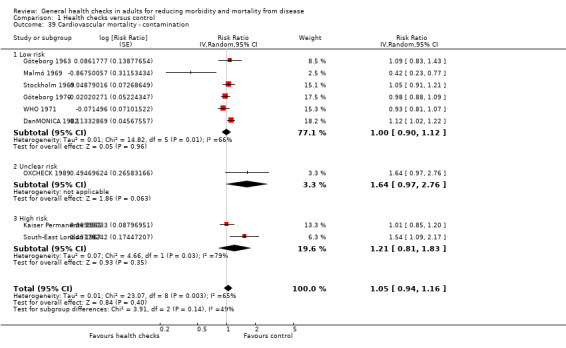
Comparison 1 Health checks versus control, Outcome 39 Cardiovascular mortality ‐ contamination.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
DanMONICA 1982.
| Methods | Design: parallel‐group randomised trial As part of the WHO MONICA project, age‐ and sex‐stratified random samples were drawn for a population study, first from 9 municipalities around Copenhagen (October 1982), and later from 2 more municipalities in the same area (March 1983), giving a total sample size of n = 17,845. From this sample, random subsets from each age stratum were drawn (n = 4807) and invited for health checks. The non‐invited participants were never contacted (n = 13,038). Participants in the first health check were re‐invited after 5 and 10 years. The study was not originally thought of as a randomised trial, but the sampling frame was kept, allowing this to be analysed as such a trial. We have not identified issues that should compromise the results. Follow‐up: approximately 30 years |
|
| Participants | Men and women aged 30, 40, 50 and 60 years at trial start Setting: medical centre/research centre Location: municipalities around Copenhagen, Denmark Number randomised: see above |
|
| Interventions | All 3 health checks included history, height and weight, BP, pulse, ECG, abdominal ultrasound, urine sample, serum lipids In addition:
Participation: 79% in the 1st round. 51% participated in all 3 rounds |
|
| Outcomes | Total mortality (30 years) CV mortality (fatal IHD + fatal stroke) (30 years) Fatal and non‐fatal IHD (30 years) Fatal and non‐fatal stroke (30 years) |
|
| Notes | Excluded 51 participants who died or emigrated after randomisation but before the 1st screening, and 11 participants who moved from an early sampled municipality to a later sampled municipality (see under methods) and were thus sampled twice. Results were calculated by the trial authors using Cox regression, adjusting for the age‐ and sex‐stratification in the sampling scheme. Participants with the outcome of interest at baseline were excluded from the analysis of that particular outcome, e.g. stroke. For CV mortality, we obtained unpublished data from the trial authors: number of participants and number of events in each of the 8 strata, and summarised the effect using fixed‐effect meta‐analysis. The trial authors also supplied us with an effect estimated with Cox regression, adjusting for the randomisation technique. Results from these analyses were nearly identical. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation done with computer (T Skaaby, personal communication) |
| Allocation concealment (selection bias) | Low risk | All participants randomised before any contact was made |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Control group never contacted. Intervention group cannot be blinded, but this is not expected to lead to bias, given that any behavioural effects are part of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Data from public registries |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | Data from public registries with little loss to follow‐up |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | No subjective outcomes |
| Selective reporting (reporting bias) | Low risk | No indications of selective reporting. Since it was not planned as a trial, outcomes cannot have been pre‐specified. However, the outcomes reported are highly relevant (mortality and morbidity). Effect on cancer mortality will soon be published (T Skaarup, personal communication) |
| Other bias | Low risk | No other sources of bias identified |
Ebeltoft 1992.
| Methods | Design: parallel‐group randomised trial A random sample (n = 2000) was taken from the whole eligible population (n = 3464). The sample was sent a short questionnaire, and participants returning the questionnaire and giving consent (n = 1507) were included and randomised into 3 groups. 1 group was offered screening (n = 502), another group was offered screening plus health discussions (n = 504), and the 3rd group had usual care (n = 501). All included participants were sent a more detailed questionnaire before the intervention. The intervention was repeated after 1 year. After 5 years all 3 groups were mailed questionnaires and invited for a follow‐up screening. Participants were also followed in national registers for 8 years and 2 comparisons were made: 1) between the 3 intervention groups and 2) between the 2000 randomly invited to participate in the trial (plus 30 in whom invitation failed for administrative reasons) and the 1434 not invited. |
|
| Participants | Men and women aged 30‐49 years identified through practice registers Setting: general practice Location: Ebeltoft, Denmark Number randomised: See above |
|
| Interventions | Screening included the following:
Participants randomised to additional health discussions were invited to annual 45 min health talks with their physician regarding lifestyle changes. Participants randomised to screening only were sent a personalised letter explaining the findings and giving recommendations. Uptake of screening: 1st round 90%, second round 81%‐83% |
|
| Outcomes | Mortality (8 years) Physician visits (8 years) Hospitalisation (8 years) Worry (5 years) Self‐reported health (5 years) |
|
| Notes | The screening and the screening + health discussion groups were combined in the reports, as there were no differences in outcomes. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: ”An Aarhus County statistician performed invitation and intervention randomization by computer, independently of the investigators.” |
| Allocation concealment (selection bias) | Low risk | All participants were allocated at once, independently of the investigators |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Lack of blinding of GPs and control group may have led to performance bias |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The most important outcomes were assessed using register data and were not subject to detection bias. Self‐reported outcomes (self‐reported health, worry, medication use) may have been biased by the absence of blinding, and is an exception to the overall rating |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | Public registries were used with 5% loss to follow‐up. Characteristics of participants lost were similar between groups |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | Loss to follow‐up was between 24% and 31%, which indicate a high risk of bias in the context of an unblinded trial |
| Selective reporting (reporting bias) | Unclear risk | Unclear |
| Other bias | High risk | All participants had returned an initial questionnaire, which limits external validity because non‐respondents were not included in some of the analyses. The trial was set in a small town, and the authors have reported that the trial had a great influence on the control group |
Family Heart 1990.
| Methods | Design: cluster‐randomised trial 13 matched pairs of general practices were randomised to either intervention or control (external control group). In the intervention practices, eligible men were randomised to either intervention or control (internal control group) and their partners were included. The intervention group was invited for screening and lifestyle intervention at baseline. After 1 year both intervention and control groups were invited. Only those participants who attended their 1st health check were included in the analyses, i.e. at baseline for the intervention group and after 1 year for the control group |
|
| Participants | Men aged 40‐59 years, and their partners, regardless of age Setting: general practice Location: UK Number randomised: not clear. Only the number of households and participants who attended screening are given. The number of people in each group were 3436 (screening), 3576 (internal control) and 5912 (external control). The number of households in each group was 2373 (screening), 2342 (internal control) and 3890 (external control), with a response rate of 73% (adjusted for 'ghosts') |
|
| Interventions | Nurse‐led screening for CV risk factors and a lifestyle intervention Screening tests used:
Coronary risk score (Dundee) was communicated to each participant. The frequency of follow‐up examinations was determined by this score together with other individual risk factors, and ranged between every 2 months (highest risk quintile) and yearly (lowest risk quintile). Lifestyle advice was given, and personally negotiated lifestyle changes were recorded in a booklet. Uptake of screening: 73% |
|
| Outcomes | Morbidity (prevalence of certain conditions) (1 year) Self‐reported health (1 year) Medication use (1 year) |
|
| Notes | We chose to use results from the comparison with the internal control group only. The trial authors found similar effect sizes when using either control group | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Low risk | Quote: “Within each intervention practice, the list of men was randomly divided into 2 groups: intervention and an internal comparison group” Comment: allocation was done on the full list all at once |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not described |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Lack of blinding can cause bias in self‐reported outcomes |
| Incomplete outcome data (attrition bias) Objective outcomes | Unclear risk | No objective outcomes included |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | Only participants attending health checks were included in the analysis. For those attending, the trial authors investigated the possible effect of excluding non‐returners at the 1‐year screening in the intervention group, and found small differences in baseline morbidity but large differences in baseline smoking |
| Selective reporting (reporting bias) | Low risk | We do not know what was stated in the protocol, but all outcomes that can reasonably be expected seem to be reported |
| Other bias | Unclear risk | The trial authors found similar results using both the internal and external control group. However, since the effects were small and possibly due to bias and acclimatisation to BP measurement, this does not rule out contamination of the internal control group |
Göteborg 1963.
| Methods | Design: parallel‐group randomised trial Included all men born in 1913 and living in Göteborg, Sweden, in 1962. Allocation of participants was done according to date of birth before any contact was made. The intervention group was invited for 3 rounds of screening and the control group was not contacted. All participants were followed through registries for mortality over 15 years |
|
| Participants | Men aged 50 years Setting: medical centre/research centre Location: Göteborg, Sweden Number of people randomised: 1013 (screening) and 1967 (control). Analyses were based on number of people alive when the intervention started on 1 January 1963, which were 1010 (screening) and 1956 (control) |
|
| Interventions | The 1st screening was performed by staff at a local hospital and used the following tests:
Half of the intervention group also had a psychiatric interview. The other half had a psychiatric questionnaire and an examination of lung function In 1967, the examination also included a physical test at maximum load The 1973 examination is unclearly described, but included height, weight, skinfold thickness and questions about morbidity, well‐being and utilisation of medical care Uptake of screening at 1st round: 85%, second round 80%, 3rd round 74% |
|
| Outcomes | Total mortality (15 years) CV mortality (15 years) Cancer mortality (15 years) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “All men meeting these criteria who were born on a date divisible by three (the third, sixth, ninth day and so on of each month) comprised the study sample". "The men who were born on other days were regarded as the control group” Comment: allocation method used is likely to yield comparable groups. All men in the eligible age range and geographical area were included and allocated before any contact was made |
| Allocation concealment (selection bias) | Low risk | As above |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The regular physicians of the participants in the intervention group were not involved with the study and the control group was not informed about the trial |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Death certificates were assessed, and some were reclassified for cause of death. The participants doing this were not blinded to allocation status (L Welin, personal communication) |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | Loss to follow‐up for mortality was 0.3% in the intervention group and 1.0% in the control group |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | No subjective outcomes |
| Selective reporting (reporting bias) | Low risk | |
| Other bias | High risk | Conditions discovered at screening were treated at the hospital where the screening was conducted. Thus, the standard of care given to the screening group likely differed from that available to the control group, which might bias the results. The control group and their regular physicians were not informed about the trial (L Welin, personal communication), which gives a low risk of contamination |
Göteborg 1970.
| Methods | Design: parallel‐group randomised trial Included all men in Gothenburg who were born between 1915 and 1925. These were randomised to an intervention group and 2 control groups. They were followed in registers for mortality and morbidity until the end of 1983, with a mean follow‐up time of 11.8 years |
|
| Participants | Men aged 47‐55 years at entry Setting: medical centre/research centre Location: Gothenburg, Sweden Number of people randomised: 10,004 (intervention), 10,011 (control 1) and 10,007 (control 2) |
|
| Interventions | The intervention group was invited to 2 screenings with a 4‐year interval. Screening tests used:
BP, cholesterol and smoking were treated if they exceeded specified thresholds. Systolic BP > 160 mm Hg or diastolic BP > 95 were followed bienially. Systolic BP > 175 mm Hg or diastolic BP > 115 mm Hg were treated with drugs. People with cholesterol > 6.8 mmol/L were offered dietary advice. Cholesterol > 7.8 mmol/L was re‐measured and treated with dietary advice. When necessary, this was supplemented with clofibrate or nicotinic acid. Clofibrate use was stopped when its adverse effects became known. People smoking > 15 cigarettes/day were invited to an anti‐smoking clinic. Uptake of screening: 75% at 1st round Control group 1: a 2% random sample was invited to screening at baseline, and an 11% random sample after 4 years Control group 2 : not contacted at all After 10 years a 20% random sample from the intervention group and control group 1 were invited to re‐examination |
|
| Outcomes | Mortality (11.8 years) CV mortality (coronary mortality + stroke mortality) (11.8 years) Cancer mortality (11.8 years) Morbidity (fatal and non‐fatal coronary heart disease, fatal and non‐fatal stroke) (11.8 years) Prescriptions (self‐reported use of antihypertensives) |
|
| Notes | We combined fatal coronary heart disease and fatal stroke as CV mortality We pooled the 2 control groups in the meta‐analyses |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was done by computer (L Wilhelmsen, personal communication) |
| Allocation concealment (selection bias) | Low risk | All participants were randomised before contact |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | GPs and the control group were not contacted |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Cause of death was recorded from death certificates. Use of antihypertensive medication was assessed at a personal interview with a physician (L Wilhelmsen, personal communication) |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | Complete follow‐up for total and cause‐specific mortality |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | 20% (n = 2000) from the intervention group and control group 1 were invited to re‐examination after 10 years. In the intervention group, 74% attended. In control group 1, 70% attended. Due to lack of blinding there is a high risk of bias |
| Selective reporting (reporting bias) | Low risk | Outcomes were pre‐specified in an early article |
| Other bias | High risk | Hypertensives and smokers were treated and followed in a special clinic, thus getting a different standard of care from the 2 control groups |
Inter99 1999.
| Methods | Design: parallel‐group randomised trial All 61,301 participants aged 30, 35, 40, 45, 50, 55 and 60 years and living in 11 municipalities in the south‐western part of Copenhagen County on 2 December 1998 were included. A random sample was invited to screening and those remaining constituted the control group. The randomisation was weighted based on age and sex, so that a desired age distribution was attained in the intervention group, and sex was equalled. This was accounted for in the analysis, using Cox regression. The intervention group and a random subsample of the control group (n = 5264) had questionnaires at baseline and after 1, 3 and 5 years of follow‐up. All participants were followed up through central registers. For analysis of morbidity and mortality, participants with IHD or stroke at baseline were excluded from each of these analyses. Also excluded 377 participants that died, emigrated, disappeared or changed personal identification number in the 3.5 month period between randomisation and the defined start date |
|
| Participants | Men and women aged 30‐60 years Setting: medical centre/research centre Location: Copenhagen, Denmark Number randomised: 13,016 (screening) and 48,285 (control) |
|
| Interventions | The screening included:
Absolute 10‐year risk of IHD was assessed using the PRECARD computer program, with individual counselling on risk factors and adverse health behaviours. High‐risk participants were offered 4 health checks (years 0, 1, 3 and 5), low‐risk participants were offered 2 (years 0 and 5). The intervention group was further randomised into high‐ or low‐intensity treatment of risk factors. The high‐intensity group participants who had a high risk of IHD were offered 6 sessions of group counselling during a 4‐6 month period, and were re‐invited for a similar intervention after 1 and 3 years. In the low‐intensity group no participants were offered group counselling Uptake of screening: 1st round 53% The control group was not contacted, except for the sample that received questionnaires |
|
| Outcomes | Mortality (10 years) Fatal and non‐fatal IHD (10 years) Fatal and non‐fatal stroke (10 years) Self‐reported health (5 years) |
|
| Notes | For morbidity and mortality, we used the reported hazard ratios which were from an analysis that took the weighted randomisation into account. The results on self‐reported health are based on a comparison between the intervention group and the subsample of the control group who had questionnaires |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “From the study population an age‐ and sex‐stratified random sample comprising 13,016 individuals was drawn”. Randomisation was done by computer (T Jørgensen, personal communication) |
| Allocation concealment (selection bias) | Low risk | Groups were formed before any participants were contacted |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding of the intervention group was not possible. The control group, including the subsample who received questionnaires, were not informed about the trial (T Jørgensen, personal communication) Medical follow‐up of high‐risk participants was by the participants’ GPs, who were informed at the beginning of the study but not otherwise involved |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Mortality and morbidity: low risk. Results from public registries Self‐reported outcomes: high risk. Lack of blinding |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | Results from registries with little loss to follow‐up |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | Loss to follow‐up for self‐reported health was 27% in the intervention group and 20% in the sample of the control group who received questionnaires. There is a risk of attrition bias due to the lack of blinding |
| Selective reporting (reporting bias) | Low risk | No indications of selective reporting |
| Other bias | Low risk | The control group was not informed about the trial and their regular physicians were not involved with the conduct of the trial. Oversampled people aged 40‐55 to the intervention group because that group was thought to be most susceptible to the lifestyle intervention. Adjustments for this were made in the analysis |
Kaiser Permanente 1965.
| Methods | Design: parallel‐group randomised trial In April 1964, a sample of members of the Kaiser‐Permanente Health Plan in San Francisco and Oakland, California, USA, aged 35‐54 years were divided into an intervention group and a control group using an allocation rule based on membership number. Starting in 1965, people in the intervention group were urged annually, by telephone and letter, to have the multiphasic screening examination offered by the Kaiser Health Plan. The intervention lasted 16 years. Participants were followed using questionnaires and registers. |
|
| Participants | Men and women aged 35‐54 years who were members of a large health plan and thus mainly people with employment Setting: medical centre/research centre (healthcare plan members) Location: California, USA Number of people randomised: 5156 (intervention) and 5557 (control). For analyses, the trial authors included people alive on 1 January 1965, when the intervention started. Thus, the groups analysed were: 5138 (intervention) and 5536 (control) |
|
| Interventions | The intervention was annual urging to have a broad medical screening. Screening tests used:
Women were advised to have a pelvic examination by a gynaecologist. Sigmoidoscopy was recommended for all participants aged ≥ 40 years. In early years there was a follow‐up visit by a physician, including a physical examination, but in later years (not specified) the follow‐up could also be performed by a nurse practitioner supervised by a physician. The control group was not urged but could have a similar health check if they wished, as part of their health plan. The control group received questionnaires about their health |
|
| Outcomes | Mortality (16 years) CV mortality (16 years) Cancer mortality (16 years) Morbidity Hospitalisation Physician visits Disability New diagnoses |
|
| Notes | People who left the Kaiser Permanente Health Plan were not followed‐up. This led to attrition of about 35% in both groups after 16 years, possibly selected as those who lost their employment. An exception to this is mortality, which was assessed using registers. Participants who were found to have moved too far away to be called for a health check after allocation were excluded. There were also exclusions due to identity mix‐ups, i.e. participants having > 1 health plan ID number. The exact figure is not given for the intervention group, but is stated to be over 200. However, the discrepancy between the groups is larger. Excluded participants were included in the analysis of mortality after 11 years, without important differences. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “The terminal digit and fourth digit of each member’s unique seven‐digit medical record number were used to assign participants to the two groups. Those with one particular terminal digit were assigned to the study group and those with another terminal digit were assigned to the control group. Those with a third terminal digit were assigned to the former if they had one of two particular fourth digits and to the latter if they had one of two other fourth digits. Medical record numbers are assigned sequentially to new members and are never reassigned.” Comment: the method used was likely to yield comparable groups, and all participants were allocated at the same time, before contact |
| Allocation concealment (selection bias) | Low risk | See above |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Neither the subjects nor their physicians were aware that they were participating in a controlled trial" In the regular mail surveys, the participants were not informed about the trial but told that the survey was about improving health services to members |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Trained readers, blind to the study or control group membership status of the patients, examined the charts selected and abstracted diagnostic data.” Quote: “Specially trained personnel, blind to the study or control group membership status of the hospital patients, coded the diagnostic and operative procedure data according to the system of the Hospital Adaption of the International Classification of Diseases (1968).” Quote: "Death certificate copies received from the State were checked against Kaiser Foundation Health Plan clinical records in order to confirm identification of the decedents as study and control group members. Those death certificates accepted for analysis were coded for underlying cause of death (again by trained persons who were blind to the study or control group membership status of the individuals involved), using the International Classification of Diseases Adapted, Eighth Revision." Comment: blinded adjudication of all objective outcomes. Self‐reported disability is an exception to this, and may be biased |
| Incomplete outcome data (attrition bias) Objective outcomes | Unclear risk | Quote: "Since surveys of the subjects still in the Health Plan indicated they used Kaiser‐Permanente facilities for over 80% of their outpatient clinic data were gathered from Kaiser clinical charts and hospital data from Health Plan computerized records". Quote: "In June 1980 3326 or 64,5% [64.5%] of the study group and 3544 or 63,8% [63.8%] of the control group were still members" Quote: "Deaths were ascertained by matching names of subjects no longer active in the Health Plan against State of California mortality records. Mortality surveillance thereby included subjects who left the Health Plan unless they became residents of another state." Comment: people who left the Kaiser Permanente Health Plan were not followed‐up. This led to attrition of about 35% in both groups after 16 years. Only people leaving California were lost to follow‐up for mortality, and the trial authors assessed this to be 8%‐18% |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | As above. The large attrition combined with a 75% response rate at each survey meant that at 16 years of follow‐up fewer than half of the participants randomised were included in the analyses |
| Selective reporting (reporting bias) | High risk | Data on surgery, reasons for hospitalisation and number of prescriptions were collected but never published |
| Other bias | High risk | After 16 years of intervention the mean number of health checks was 6.8 in the intervention group and 2.8 in the control group. In the intervention group 16% of the participants had never had a health check, compared to 36% in the control group. Thus, there was contamination of the control group. |
Malmö 1969.
| Methods | Design: parallel‐group randomised trial All men born in 1914 and living in Malmö, Sweden in early 1969 were included in the study. Men born in even‐numbered months were invited to screening and men born in uneven‐numbered months were not. 5‐year follow‐up through registries. |
|
| Participants | Men only, all aged 55 year Setting: medical centre/research centre Location: Malmö, Sweden Numbers randomised: 809 (screening) and 804 (control) |
|
| Interventions | The intervention group was invited to 1 screening Screening tests used:
Participants with hypertension and impaired lung function were followed and treated at the hospital. Of 178 participants classified as heavy smokers, 51 were offered a group counselling intervention to quit. Of these, 5 were prescribed sedatives. Uptake: 87% The control group was not contacted |
|
| Outcomes | Total mortality (5 years) CV mortality (5 years) Cancer mortality (5 years) Hospitalisation Morbidity |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “...all men born in even‐numbered months in 1914 were invited to take part in an examination of cardiovascular and pulmonary function” Comment: all participants were allocated at the same time, before contact, and the method used is likely to yield comparable groups |
| Allocation concealment (selection bias) | Low risk | See above |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The control group and their regular physicians were unaware of the trial |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The person assessing cause of death was not aware of the allocation (S Isacsson, personal communication). Hospitalisation data were from public registers |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | Loss to follow‐up was 1% for mortality. For hospitalisation it was 3.6% (intervention) and 5.6% (control) |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | No subjective outcomes were reported |
| Selective reporting (reporting bias) | Low risk | No indications of selective reporting. Reports all expected outcomes |
| Other bias | High risk | Conditions identified at screening were followed and treated at a hospital in contrast to the control group who were followed by GPs. Thus, the standard of care was likely different. Participants in the control group and their primary care physicians were unaware of the trial, which gives a low risk of contamination. |
Mankato 1982.
| Methods | Design: parallel‐group randomised trial Addresses representing the entire community were randomised. In the intervention group, the whole household was invited for screening, but only 1 eligible participant from each household, selected randomly, was included in the trial and followed. The control group was not invited. After 1 year, participants in the intervention group who attended the initial screening were re‐invited, and the control group was invited for their 1st time |
|
| Participants | Men and women aged 25‐74 years Setting: medical centre/research centre Location: Mankato, Minnesota, USA Number randomised: 1156 (screening) and 1167 (control) |
|
| Interventions | Screening tests used:
Results of tests were returned during the visit. Participants received health education at each measurement station, either on videotape, printed materials, or both. After measurements each family spent 20 min with a health educator to review test results and receive further health advice. The average visit lasted 75 min Participants with high BP or high cholesterol were referred to their regular physician Uptake of screening: 50% The control group was not invited until end of trial |
|
| Outcomes | Prescriptions (self‐reported use of antihypertensive drugs) | |
| Notes | Simultaneously with the trial, a population‐based programme to educate about risk factors for coronary heart disease was going on. This programme included an offer of screening tests for coronary heart disease risk at the same centre that also conducted the trial. However, participants in the control group were systematically excluded from attending the screening clinic for the duration of the trial | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was done by computer (D Murray, personal communication) |
| Allocation concealment (selection bias) | Low risk | All participants were randomised at the same time, before any contact |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: “Except for the recruitment supervisor, HHC [screening site, our comment], staff members were not informed of the study until its conclusion". Quote: "In addition, participants were not informed of their treatment condition and were scheduled together during the 1983 follow‐up. They were identified only through a special code kept secret from the staff." Physicians were not informed about the trial, but participants with high BP or high cholesterol were referred to their regular physician for treatment (D Murray, personal communication) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | The included outcome (medication use) was self‐reported (D Murray, personal communication) and could be biased due to lack of blinding |
| Incomplete outcome data (attrition bias) Objective outcomes | Unclear risk | No objective outcomes |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | Only half of those invited attended their 1st screening and were included in analyses. In addition, there was a 12% loss to follow‐up in the intervention group between the baseline screening and the follow‐up screening. 7% of the control group participants moved away before the 1‐year screening. In summary, in both groups about 40% of those randomised were included in the analyses |
| Selective reporting (reporting bias) | Low risk | No indications of selective reporting |
| Other bias | High risk | A population‐based programme to educate about risk factors for coronary heart disease was ongoing during the trial. This may have diminished the effect of the intervention |
New York 1971.
| Methods | Design: cluster‐randomised trial A random 80% sample of eligible families was invited for screening and the remaining 20% were not. Sampling was stratified by Medicaid status and the presence of a child 12‐18 years of age. The main aim was to assess whether health checks would reduce the health difference between poor and non‐poor families. The trial appears planned to last 3‐4 years, but the trial authors noted that the follow‐up could be prolonged if the results indicated an effect on health differentials between economic groups |
|
| Participants | Families with ≥ 1 person aged 12‐74 years old, enrolled for ≥ 1 years in the Health Insurance Plan of Greater New York Setting: medical centre/research centre Location: New York City, New York, USA Number randomised: not clear. The papers mention an expected number of 7000 non‐poor families in the intervention group and a somewhat smaller number of poor families. The control group would be 20% of this size |
|
| Interventions | Screening tests used:
|
|
| Outcomes | No outcomes reported. The trial was designed to investigate disability and absence from work. Mortality data were also to be gathered | |
| Notes | The programme was discontinued after the 1st screening round, but follow‐up was planned to continue. We have not found reports of the results | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not enough information available to assess |
| Allocation concealment (selection bias) | Unclear risk | Not enough information available to assess |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not enough information available to assess |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not enough information available to assess |
| Incomplete outcome data (attrition bias) Objective outcomes | Unclear risk | Not enough information available to assess |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | Not enough information available to assess |
| Selective reporting (reporting bias) | High risk | No results reported |
| Other bias | Unclear risk | Not enough information available to assess |
Northumberland 1969.
| Methods | Design: parallel‐group randomised trial All eligible men were allocated at the same time before any contact was made, excluding 7% because of serious illness. Participants were allocated by date of birth to 1 of 3 groups: questionnaire and full examination, questionnaire and examination if indicated by answers to the questionnaire, and neither questionnaire nor examination. We used the 1st and the last group in our analyses. Outcomes were assessed from medical records |
|
| Participants | Men aged 50‐59 years Setting: general practice Location: England, UK Numbers randomised: 242 (intervention) and 291 (control) |
|
| Interventions | The examination is not specified, is described in the article as a "routine health examination", a "full examination", and "screening programme". It took an average of 26 min Uptake of screening: 90% |
|
| Outcomes | Physician visits | |
| Notes | Also reported prescription of drugs, use of laboratory investigations, sickness certifications and admissions to hospital, but in a way we could not use | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The randomisation sequence was based on date of birth. All eligible men were allocated at the same time before any contact was made, excluding 7%, balanced across groups, because of serious illness. Trial authors found small imbalances in the past medical histories between groups, but also noted that there might have been bias in the assessment of this. All in all, we judge that the method used is likely to have produced comparable groups |
| Allocation concealment (selection bias) | Low risk | See above |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Physicians were involved in trial conduct, were aware of screening status, and treated both screened and unscreened participants |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Bias could have been introduced in completing the past history recording as the group that the participant was assigned to was indicated on the front page of the schedule". Comment: all outcomes were abstracted from participant records and therefore susceptible to detection bias |
| Incomplete outcome data (attrition bias) Objective outcomes | Unclear risk | Not described |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | No subjective outcomes reported |
| Selective reporting (reporting bias) | Unclear risk | Unclear |
| Other bias | Unclear risk | Cannot rule out contamination of the control group |
OXCHECK 1989.
| Methods | Design: cluster‐randomised trial People who returned an initial questionnaire were included and randomised by household into 4 groups: health checks at year 1 and 4; at year 2 and 4; at year 3 and 4; and only at year 4. The 1st 3 groups constituted the intervention groups and the last group was a control group. Participants in the 1st 2 groups were further randomised to annual re‐checks or no re‐checks |
|
| Participants | Men and women aged 35‐64 years Setting: general practice Location: Luton and Dunstable, UK Number randomised: 2776, 2771 and 2760 (screening groups) and 2783 (control) |
|
| Interventions | CV screening conducted by specially trained nurses (45‐60 min) Screening tests used:
Counselling about risk factors. Follow‐up visits for risk factors (10‐20 min). Annual re‐checks were similar to initial health check, but briefer (30 min). Uptake of screening: 1st round 80%, re‐checks 76%‐79% |
|
| Outcomes | Mortality (4 years) CV mortality (4 years) Cancer mortality (4 years) Morbidity (cancer incidence) (4 years) |
|
| Notes | The trial was designed for studying changes in risk factors and not mortality, but we obtained mortality data from the trial authors In the meta‐analyses, we combined the 3 groups invited to screening in year 1, 2 and 3 and compared them with the control group. The results were similar when analysing the results for maximum contrast, i.e. only comparing those screened in year 1 with those in year 4 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was done independently of the research team, using a computerised algorithm (D Mant, personal communication) |
| Allocation concealment (selection bias) | Low risk | The computer generated a list of names for each practice indicating the intervention group to which each individual participant had been allocated (D Mant, personal communication) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "A sticker was attached to the outside of each patient's general practice notes indicating the randomisation group" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Cause of death and cancer incidence were from national statistics and likely unbiased |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | No subjective outcomes |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Unclear risk | Only people who returned an initial questionnaire were included, which limits external validity due to self‐selection Risk of contamination is unclear |
Salt Lake City 1972.
| Methods | Design: cluster‐randomised trial Randomised by family. Allocation ratio was 3:2 (intervention:control) Participants consisted of random samples from 3 groups: 200 families with a low‐income and a pre‐paid healthcare programme, 200 families with a low‐income and no pre‐paid healthcare programme, and 166 middle‐income families, who had volunteered for a study of health care |
|
| Participants | Age > 18 years Setting: medical centre/research centre Location: Salt Lake City, Utah, USA Number randomised: 642 (intervention) and 454 (control) |
|
| Interventions | Both groups had a baseline interview measuring health status (Bush index), number of disability days caused by illness, patterns of healthcare utilisation, health knowledge, attitudes toward the healthcare system (Hulka scale) and Pilowsky’s scale of hypochondriasis. The intervention group was urged by telephone to obtain a multiphasic screening examination at no cost. Each participant’s physician had to give permission for them to participate. After screening the results were sent to the physician for interpretation and follow‐up Screening tests used:
Uptake of screening: 60% The control group was not urged to be screened |
|
| Outcomes | Hospitalisation Physician visits Disability |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No description |
| Allocation concealment (selection bias) | Unclear risk | No description |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Primary care physicians had to give permission for each person to participate. Lack of blinding of physicians could cause performance bias |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were patient‐reported and susceptible to bias due to the lack of blinding |
| Incomplete outcome data (attrition bias) Objective outcomes | High risk | Those who changed economic status, did not attend for screening, did not consult their physician about screening results, or who did not participate in the 1‐year follow‐up, were excluded. This resulted in only 49% of the intervention group and 82% of the control group participants being included in analyses |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | As above |
| Selective reporting (reporting bias) | Unclear risk | Unclear |
| Other bias | Unclear risk | Not enough information to judge the risk of contamination |
South‐East London 1967.
| Methods | Design: cluster‐randomised trial Eligible people were identified through registers and randomised by family to intervention or control. The screening group was invited by letter to 2 rounds of screening, with a 2‐year interval. After 5 years both groups were invited for screening, but the trial authors state that this screening was "non‐prescriptive, in the sense that no therapeutic activity was expected to result from it". Follow‐up was continued for a further 4 years |
|
| Participants | Men and women aged 40‐64 years Setting: general practice Location: London, UK Number randomised: according to 1 paper the numbers were 3460 (screening) and 3337 (control) (Trevelyan 1973 (see South‐East London 1967)), whereas another gives 3876 (screening) and 3353 (control) (South‐East London Study Group 1977 (see South‐East London 1967)). The mortality analyses were based on 3292 (intervention) and 3132 (control) participants |
|
| Interventions | Screening tests used:
Advice on smoking and weight was given to all for whom it was appropriate. All results were passed on to the participant's GP Uptake of screening: 1st round 73%, second round 66% |
|
| Outcomes | Mortality (9 years) CV mortality (not including stroke) (9 years) Cancer mortality (9 years) Hospitalisation Morbidity Physician visits Self‐reported health Disability Worry |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Eligible participants and couples were listed alphabetically and alternate allocation was used. After randomisation, a matching took place which is unclearly described. It resulted in the exclusion of 276 participants from the control group The sizes of the groups vary between reports |
| Allocation concealment (selection bias) | Low risk | Participants were identified and randomised before any contact was made |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "All information gathered at both screening sessions was passed on to the general practitioners" Comment: GPs were not blinded, which gives a risk of performance bias. Not clear whether the control group was informed about the trial |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No mention of blinding of outcome assessment. Self‐reported outcomes are susceptible to bias due to lack of blinding |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | After 5 years 20% of the participants had migrated from the area and were lost to follow‐up for physician visits but not for other objective outcomes. Thus low risk for these outcomes but high risk for the outcome "physician visits" |
| Incomplete outcome data (attrition bias) Subjective outcomes | High risk | Loss to follow‐up for subjective outcomes after 5 years was 47% (intervention) and 41% (control) |
| Selective reporting (reporting bias) | High risk | According to an early report, data were collected on prescriptions issued, referrals and investigations carried out, but were not reported and are not available |
| Other bias | High risk | The control group was screened after 5 years, which biased the 9‐year results towards no effect A high degree of involvement of GPs gives a risk of contamination |
Stockholm 1969.
| Methods | Design: parallel‐group randomised trial A sample was drawn from the eligible population and divided into 3 age groups. From these, a random sample was drawn using sample fractions in the proportions of 3:2:1, with the highest fraction for the youngest age stratum. These people were sent a questionnaire about social and physical difficulties and health needs. Based on this, and on data from the public inpatient register, they were substratified by expected needs for medical services: high need, low need, no need, and unknown need. Randomisation to screening and control groups took place within these strata, but proportionally more were randomised to screening in the 2 groups with high and low needs for services compared to those with no or unknown needs for services. The trial authors used regression analysis, in which they controlled for the baseline imbalances introduced by the randomisation scheme. Participants were followed for mortality in registers for 22 years |
|
| Participants | Men and women aged 18‐65 Setting: medical centre/research centre Location: Stockholm, Sweden Number randomised: 3064 (screening) and 29,122 (control) |
|
| Interventions | Participants in the intervention group were invited to 1 screening Screening tests used:
Participants with identified need for specialist services were directly referred, whereas participants were instructed to contact their primary care physician for other identified issues. Simple services like reassurance and prescription of simple medications (not specified) were provided by the researchers. Uptake of screening: 84% The control group was not invited |
|
| Outcomes | Total mortality (22 years) CV mortality (22 years) Cancer mortality (22 years) |
|
| Notes | We obtained data on mortality within each of the 12 strata in which randomisation was performed, and treated them as 12 separate trials, each giving an estimate of the effect. We then combined the results with a fixed‐effect model meta‐analysis, and used this estimate for our meta‐analysis. Our result is nearly identical to that of the trial authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was done by computer (H Theobald, personal communication) |
| Allocation concealment (selection bias) | Low risk | All participants were randomised at the same time |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | The Intervention group could not be blinded. Not clear whether the control group and their GPs were aware of the trial |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Cause of death on death certificate was used |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | < 1% missing outcome data. |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | No subjective outcomes |
| Selective reporting (reporting bias) | Unclear risk | Data on hospitalisation, operations and cancer incidence have been collected but not yet published (H Theobald, personal communication) |
| Other bias | Unclear risk | Both groups had a questionnaire at baseline. The effect of this is unclear |
Titograd 1971.
| Methods | Design: parallel‐group randomised trial A random sample was drawn from the eligible population and randomly divided into an intervention and a control group. A 20% random subsample of both groups were interviewed at baseline. Analysis was planned after 6 years, and follow‐up would be continued for a further 4 years in case of no effect |
|
| Participants | Men and women aged 30‐49 years Setting: medical centre/research centre Location: Podgorica, Montenegro (Titograd, former Yugoslavia at the time of the trial) Number randomised: 6577 (screening) and 6573 (control) |
|
| Interventions | The intervention group was invited for screening at baseline and with 2‐year intervals. Follow‐up of positive test results and treatment of identified conditions done according to specified regimens. The control group was not invited for screening Screening tests used:
|
|
| Outcomes | No outcomes were reported. The outcomes studied were mortality, morbidity (from medical records), absence from work, and utilisation of outpatient and inpatient services | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not enough information available to assess |
| Allocation concealment (selection bias) | Unclear risk | Not enough information available to assess |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not enough information available to assess |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not enough information available to assess |
| Incomplete outcome data (attrition bias) Objective outcomes | Unclear risk | Not enough information available to assess |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | Not enough information available to assess |
| Selective reporting (reporting bias) | High risk | No results reported |
| Other bias | Unclear risk | Not enough information available to assess |
WHO 1971.
| Methods | Design: cluster‐randomised trial 40 matched pairs of factories were randomised to intervention or control. Follow‐up varied between factories, but was between 5 and 6 years |
|
| Participants | Men aged 40‐59 years at entry Setting: workplace Location: UK, Belgium, Poland and Italy. Spain was also part of the trial, but was not included in the analyses of events because it started late compared to the other part of the trial. This decision was made before results were available to the investigators Numbers randomised: 30,489 (intervention) and 30,392 (control). A 10% random sample of the control group was screened at baseline and was not included in the analysis of events. Thus, the numbers analysed were: 30,489 (intervention) and 26,971 (control) |
|
| Interventions | Screening tests used:
The men at highest risk (10%‐20%, definitions varied between centres), were called for a physician interview and given advice and treatment. All men at the intervention factories were given advice on cholesterol‐lowering dietary changes. Individual advice was given when relevant for smoking cessation, weight reduction, exercise, control of hypertension. Participants were treated and followed‐up by the research teams. Annually, a random 5% sample was re‐examined. At the end of follow‐up, all in the intervention and control groups were invited to examination. Uptake of screening: 86% |
|
| Outcomes | Total mortality (5‐6 years) CV mortality (only reported coronary mortality, which we used) Cancer mortality (only data from the UK, Poland and Italy parts of the trial) Morbidity (fatal and non‐fatal coronary heart disease) |
|
| Notes | Effect estimate from an appropriate analysis, taking clustering into account, was reported for total and coronary heart disease mortality and we used this in our meta‐analysis. For cancer mortality, no such estimate was reported, and we thus ignored the clustering in the meta‐analysis, but investigated the effect in a pre‐specified sensitivity analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | 1 centre used coin‐flips (G De Backer, personal communication). No description is available for the other centres |
| Allocation concealment (selection bias) | Low risk | Quote: "Twenty‐four large industrial groups (mainly factories) were recruited and then paired according to type of industry and are. 1 of each pair was allocated at random to receive the intervention programme while the other served as a control". Quote: "[The factories] were required to commit themselves to participation before knowing whether their allocation would be to an active programme of intervention or to a passive control status" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Primary care physicians and the control group were not informed about the trial |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of assessment of cause of death is not described in the articles summarising all countries. There was blinded assessment in the UK and Belgium, but we cannot rule out unblinded assessment in other centres Morbidity (coronary heart disease) was only assessed for those still employed. Although likely lowering the number of events, this should be the same in both groups. In contrast, trying to assess morbidity in people no longer employed would have risked biasing the results in favour of the control group |
| Incomplete outcome data (attrition bias) Objective outcomes | Low risk | Quote: "Survival status at end of trial was established in 99.8%." Comment: thus, total and coronary heart disease mortality are at low risk of attrition bias. Cancer mortality is an exception, because it was not reported from the Belgian part of the trial. The reason given for this is that all non‐coronary deaths were only categorised as such, without detailing the cause of death, as per the trial's protocol. The risk of bias due to this is unclear |
| Incomplete outcome data (attrition bias) Subjective outcomes | Unclear risk | No subjective outcomes included |
| Selective reporting (reporting bias) | Low risk | Outcomes were pre‐specified in early articles |
| Other bias | High risk | Participants in the intervention groups were treated and followed by the research team, in contrast to the control group. Thus, the standard of care was different |
BP: blood pressure; BMI: body mass index; CV: cardiovascular; ECG: electrocardiogram; FEV: forced expiratory volume; GP: General Practitioner; HDL: high‐density lipoprotein; IHD: ischaemic heart disease; LDL: low‐density lipoprotein; MI: myocardial infarction; VLDL: very low‐density lipoprotein; WHO: World Health Organization
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| ACTRN12610000511033 | Wrong intervention |
| Ajay 2014 | Wrong patient population |
| Ayorinde 2013 | Wrong study design |
| Baicker 2013 | Wrong intervention |
| Barry 2017 | Wrong intervention |
| Bender 2015b | Wrong study design |
| Brett 2012 | Wrong population |
| Caley 2014 | Wrong study design |
| Campbell Scherer 2014 | Wrong intervention |
| Carter 2016 | Wrong study design |
| Chang 2016 | Wrong study design |
| Charles 2012 | Wrong study design |
| Charles 2013 | Wrong intervention |
| Cochrane 2012 | Wrong intervention ‐ both groups screened at baseline |
| Dalsgaard 2014 | Wrong study design |
| Davis Lameloise 2013 | Wrong intervention ‐ both groups screened at baseline |
| Diederichsen 2015 | Wrong patient population |
| Dirven 2013 | Wrong intervention |
| Doughty 2014 | Wrong intervention |
| Duncan 2016 | Wrong intervention ‐ both groups screened at baseline |
| Dyakova 2016 | Wrong study design |
| Echouffo Tcheugui 2015 | Wrong intervention |
| Engelsen 2014 | Wrong study design |
| Grunfeld 2013 | Wrong intervention |
| Haas 2016 | Wrong intervention |
| Haas 2017 | Wrong intervention |
| Harris 2012 | Wrong intervention |
| Harris 2017 | Wrong intervention |
| Herman 2012 | Wrong intervention |
| Herman 2014 | Wrong intervention ‐ both groups screened at baseline |
| Herrigel 2014 | Summary of included study, but not by trial authors |
| Høj 2014 | Wrong intervention |
| Høj 2018 | Wrong intervention |
| Ijkema 2014 | Wrong patient population |
| ISRCTN11833436 | Wrong intervention |
| Kaczorowski 2011 | Wrong age group |
| Khetan 2017 | Wrong study design |
| Kozela 2012 | Wrong study design |
| Lindholt 2017 | Wrong age group |
| Lindsay 2013 | Wrong study design |
| Mar 2014 | Wrong study design |
| McDermott 2016 | Wrong intervention |
| McKenzie 2013 | Wrong patient population |
| NCT02224248 | Wrong intervention ‐ both groups screened at baseline |
| NCT02615769 | Wrong intervention ‐ both groups screened at baseline |
| NTR2379 | Wrong study design |
| Oldenburg 2015 | Wrong intervention ‐ both groups screened at baseline |
| Orts 2016 | Wrong intervention |
| Panniyammakal 2017 | Wrong patient population |
| Paszat 2017 | Wrong intervention |
| Rodondi 2012 | Wrong study design |
| Si 2014 | Wrong study design |
| Simmons 2012 | Wrong intervention |
| Simmons 2017 | Wrong study design |
| Stickler 2000 | Wrong population |
| Yan 2013 | Wrong intervention |
Characteristics of ongoing studies [ordered by study ID]
Check Your Health.
| Trial name or title | Check your health (CORE) |
| Methods | Randomised trial |
| Participants | Men and women aged 30‐49 years |
| Interventions | Health checks |
| Outcomes | CVD risk factors, physical activity level, quality of life, sick leave, labour market attachment |
| Starting date | 2013 |
| Contact information | |
| Notes |
NCT01979107.
| Trial name or title | Early detection of and intervention towards chronic diseases among individuals without formal education |
| Methods | Randomised trial |
| Participants | Men with low formal education |
| Interventions | Health checks + lifestyle intervention |
| Outcomes | Smoking status, chronic disease detection, alcohol consumption, physical activity, perceived stress |
| Starting date | 2013 |
| Contact information | |
| Notes |
CVD: cardiovascular disease
Differences between protocol and review
We originally expected to include trials of geriatric screening but found that the intervention in most of these differed too much from our perception of what constitutes a health check. The actual medical screening was usually a minor component in a complex intervention involving other important interventions, for example, screening for functional status; social, financial or legal needs; or home safety; or interventions such as specialist revision of individual medication or falls prevention. Consequently, it would not be possible to isolate the effect of the screening and we therefore chose not to include trials that were described as targeting an elderly population or that only included people over 65 years of age. Complex interventions directed at elderly people, including geriatric assessments, have been reviewed by Beswick and colleagues (Beswick 2008).
In the first version of the review, Christian Grønhøj Larsen was a co‐author.
We have changed the wording of the outcome "Patient worry" to "worry", because the review deals with general populations and not only patients.
We added results on fatal and non‐fatal ischaemic heart disease and stroke to the summary of findings table, as they were the most important secondary results.
Contributions of authors
PCG initiated the project, LTK drafted the protocol and KJJ and PCG provided comments. LTK and KJJ screened titles and abstracts and made decisions about inclusion of trials. LTK and KJJ extracted data, LTK analysed data and drafted the review, and KJJ and PCG contributed to the revisions. In the first version of the review, Christian Grønhøj Larsen participated in screening and inclusion of trials, and commented on the manuscript.
Sources of support
Internal sources
-
Nordic Cochrane Centre, Denmark.
Salary and facilities
External sources
-
Trygfonden, Denmark.
Part of salary for LTK
Declarations of interest
Lasse T. Krogsbøll: none known
Karsten Juhl Jørgensen: none known
Peter C. Gøtzsche: none known
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
DanMONICA 1982 {published data only}
- Skaaby T, Jørgensen T, Linneberg A. Effects of invitation to participate in health surveys on the incidence of cardiovascular disease: a randomized general population study. International Journal of Epidemiology 2017;46(2):603‐11. [DOI] [PubMed] [Google Scholar]
Ebeltoft 1992 {published and unpublished data}
- Christensen B, Engberg M, Lauritzen T. No long‐term psychological reaction to information about increased risk of coronary heart disease in general practice. European Journal of Cardiovascular Prevention and Rehabilitation 2004;11(3):239‐43. [DOI] [PubMed] [Google Scholar]
- Engberg M, Christensen B, Karlsmose B, Lous J, Lauritzen T. Can systematic general health screening and patient‐physician health discussions improve the cardiovascular profile of the population? A randomized controlled trial in general practice with a 5‐year follow‐up [Kan systematiske generelle helbredsundersøgelser og helbredssamtaler forbedre den kardiovaskulære risikoprofil i befolkningen? En randomiseret og kontrolleret undersøgelse i almen praksis med fem års opfølgning]. Ugeskrift for Laeger 2002;164(25):3354‐60. [PubMed] [Google Scholar]
- Engberg M, Christensen B, Karlsmose B, Lous J, Lauritzen T. General health screenings to improve cardiovascular risk profiles: a randomized controlled trial in general practice with 5‐year follow‐up. The Journal of Family Practice 2002;51(6):546‐52. [PubMed] [Google Scholar]
- Geest TA, Engberg M, Lauritzen T. Discordance between self‐evaluated health and doctor‐evaluated health in relation to general health promotion. Scandinavian Journal of Primary Health Care 2004;22(3):146‐51. [DOI] [PubMed] [Google Scholar]
- Kanstrup H, Refsgaard J, Engberg M, Lassen JF, Larsen ML, Lauritzen T. Cholesterol reduction following health screening in general practice. Scandinavian Journal of Primary Health Care 2002;20(4):219‐23. [DOI] [PubMed] [Google Scholar]
- Karlsmose B, Lauritzen T, Engberg M, Parving A. A randomised controlled trial of screening for adult hearing loss during preventive health checks. The British Journal of General Practice 2001;51(466):351‐5. [PMC free article] [PubMed] [Google Scholar]
- Larsen EL, Thomsen JL, Lauritzen T, Engberg M. [Forebyggende helbredsundersøgelser og helbredssamtaler i almen praksis ‐ en analyse af patientperspektivet. En analyse med særligt fokus på Sundhedsprojekt Ebeltoft og andre randomiserede studier]. Medicinsk Teknologivurdering ‐ puljeprojekter 6(7). Copenhagen (Denmark): Sundhedsstyrelsen, Center for Evaluering og Medicinsk Teknologivurdering 2006.
- Lauritzen T. [Helbredsundersøgelser og samtaler reducerer deltagernes risikoscore for hjerte‐kar‐sygdom]. Månedsskrift for Almen Praksis 2012;90(3):245‐50. [Google Scholar]
- Lauritzen T, Jensen MS, Thomsen JL, Christensen B, Engberg M. Health tests and health consultations reduced cardiovascular risk without psychological strain, increased healthcare utilization or increased costs. An overview of the results from a 5‐year randomized trial in primary care. The Ebeltoft Health Promotion Project (EHPP). Scandinavian Journal of Public Health 2008;36(6):650‐61. [DOI] [PubMed] [Google Scholar]
- Lauritzen T, Leboeuf‐Yde C, Lunde IM, Nielsen KD. Ebeltoft project: baseline data from a five‐year randomized, controlled, prospective health promotion study in a Danish population. The British Journal of General Practice 1995;45(399):542‐7. [PMC free article] [PubMed] [Google Scholar]
- Lauritzen T, Nielsen KD, Leboeuf‐Yde C, Lunde IM. The health project Ebeltoft: health check ups and discussions in general practice. Basic data from a 5‐year, prospective, randomized, controlled population study. Ugeskrift for Laeger 1997;159(25):3940‐6. [PubMed] [Google Scholar]
- Rasmussen SR, Kilsmark J, Hvenegaard A, Thomsen JL, Engberg M, Lauritzen T, et al. [Forebyggende helbredsundersøgelser og helbredssamtaler i almen praksis. En sundhedsøkonomisk analyse af »Sundhedsprojekt Ebeltoft«]. Medicinsk Teknologivurdering – puljeprojekter; 6(6). Copenhagen (Denmark): Sundhedsstyrelsen, Center for Evaluering og Medicinsk Teknologivurdering 2006.
- Rasmussen SR, Thomsen JL, Kilsmark J, Hvenegaard A, Engberg M, Lauritzen T, et al. Preventive health screenings and health consultations in primary care increase life expectancy without increasing costs. Scandinavian Journal of Public Health 2007;35(4):365‐72. [DOI] [PubMed] [Google Scholar]
- Thomsen JL, Karlsmose B, Parner ET, Thulstrup AM, Lauritzen T, Engberg M. Secondary healthcare contacts after multiphasic preventive health screening: a randomized trial. Scandinavian Journal of Public Health 2006;34(3):254‐61. [DOI] [PubMed] [Google Scholar]
- Thomsen JL, Parner ET. Methods for analysing recurrent events in health care data. Examples from admissions in Ebeltoft Health Promotion Project. Family Practice 2006;23(4):407‐13. [DOI] [PubMed] [Google Scholar]
- Thomsen JL, Parner ET, Karlsmose B, Thulstrup AM, Lauritzen T, Engberg M. Effect of preventive health screening on long‐term primary health care utilization. A randomized controlled trial. Family Practice 2005;22(3):242‐8. [DOI] [PubMed] [Google Scholar]
Family Heart 1990 {published data only}
- Davies G, Pyke S, Kinmonth AL, Family Heart Study Group. Effect of non‐attenders on the potential of a primary care programme to reduce cardiovascular risk in the population. BMJ 1994;309(6968):1553‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Family Heart Study Group. British family heart study: its design and method, and prevalence of cardiovascular risk factors. The British Journal of General Practice 1994;44(397):62‐7. [PMC free article] [PubMed] [Google Scholar]
- Family Heart Study Group. Randomised controlled trial evaluating cardiovascular screening and intervention in general practice: principal results of British Family Heart Study. BMJ 1994;308(6924):313‐20. [PMC free article] [PubMed] [Google Scholar]
- Marteau TM, Kinmonth AL, Pyke S, Thompson SG, Family Heart Study Group. Readiness for lifestyle advice: self‐assessments of coronary risk prior to screening in the British Family Heart Study. The British Journal of General Practice 1995;45(390):5‐8. [PMC free article] [PubMed] [Google Scholar]
- Marteau TM, Kinmonth AL, Thompson S, Pyke S, British Family Heart Study Group. The psychological impact of cardiovascular screening and intervention in primary care: a problem of false reassurance?. The British Journal of General Practice 1996;46(411):577‐82. [PMC free article] [PubMed] [Google Scholar]
- Pyke SD, Wood DA, Kinmonth AL, Thompson SG, Family Heart Study Group. Change in coronary risk and coronary risk factor levels in couples following lifestyle intervention. Archives of Family Medicine 1997;6(4):354‐60. [DOI] [PubMed] [Google Scholar]
Göteborg 1963 {published data only}
- Grimby G, Bjure J, Aurell M, Ekström‐Jodal B, Tibblin G, Wilhelmsen L. Work capacity and physiologic responses to work. Men born in 1913. The American Journal of Cardiology 1972;30(1):37‐42. [DOI] [PubMed] [Google Scholar]
- Larsson B, Björntorp P, Tibblin G. The health consequences of moderate obesity. International Journal of Obesity 1981;5(2):97‐116. [PubMed] [Google Scholar]
- Tibblin G. A population study of 50‐year‐old men. An analysis of the non‐participation group. Acta Medica Scandinavica 1965;178(4):453‐9. [DOI] [PubMed] [Google Scholar]
- Tibblin G. High blood pressure in men aged 50 ‐‐ a population study of men born in 1913. Acta Medica Scandinavica 1967;470:1‐84. [PubMed] [Google Scholar]
- Tibblin G, Aurell E, Hjortzberg‐Nordlund H, Paulin S, Risholm L, Sanne H, et al. A general health examination of a random sample of 50‐year‐old men in Göteborg. Acta Medica Scandinavica 1965;177:739‐49. [DOI] [PubMed] [Google Scholar]
- Tibblin G, Welin L, Larsson B, Ljungberg IL, Svärdsudd K. The influence of repeated health examinations on mortality in a prospective cohort study, with a comment on the autopsy frequency. The study of men born in 1913. Scandinavian Journal of Social Medicine 1982;10(1):27‐32. [DOI] [PubMed] [Google Scholar]
Göteborg 1970 {published data only}
- Wilhelmsen L, Berglund G, Elmfeldt D, Tibblin G, Wedel H, Pennert K, et al. The multifactor primary prevention trial in Göteborg, Sweden. European Heart Journal 1986;7(4):279‐88. [DOI] [PubMed] [Google Scholar]
- Wilhelmsen L, Ljungberg S, Wedel H, Werkö L. A comparison between participants and non‐participants in a primary preventive trial. Journal of Chronic Diseases 1976;29(5):331‐9. [DOI] [PubMed] [Google Scholar]
- Wilhelmsen L, Tibblin G, Werkö L. A primary preventive study of Gothenburg, Sweden. Preventive Medicine 1972;1(1):153‐60. [DOI] [PubMed] [Google Scholar]
Inter99 1999 {published data only}
- Jørgensen T, Borch‐Johnsen K, Thomsen TF, Ibsen H, Glümer C, Pisinger C. A randomized non‐pharmacological intervention study for prevention of ischaemic heart disease: baseline results Inter99. European Journal of Cardiovascular Prevention and Rehabilitation 2003;10(5):377‐86. [DOI] [PubMed] [Google Scholar]
- Jørgensen T, Jacobsen RK, Toft U, Aadahl M, Glümer C, Pisinger C. Effect of screening and lifestyle counselling on incidence of ischaemic heart disease in general population: Inter99 randomised trial. BMJ 2014;4(7):e004530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jørgensen T, Ladelund S, Borch‐Johnsen K, Pisinger C, Schrader AM, Thomsen T, et al. Screening for risk of cardiovascular disease is not associated with mental distress: the Inter99 study. Preventive Medicine 2009;48(3):242‐6. [DOI] [PubMed] [Google Scholar]
- Lau CJ, Pisinger C, Husemoen LL, Jacobsen RK, Linneberg A, Jørgensen T. Effect of general health screening and lifestyle counselling on incidence of diabetes in general population: Inter99 randomised trial. Preventive Medicine 2016;91:172‐79. [DOI] [PubMed] [Google Scholar]
- Pisinger C, Ladelund S, Glümer C, Toft U, Aadahl M, Jørgensen T. Five years of lifestyle intervention improved self‐reported mental and physical health in a general population: the Inter99 study. Preventive Medicine 2009;49(5):424‐8. [DOI] [PubMed] [Google Scholar]
Kaiser Permanente 1965 {published data only}
- Collen M. Cost analysis of the Kaiser Foundations systemized health evaluation. Preventive Medicine USA. New York: Prodist, 1976. [Google Scholar]
- Collen MF. The cost‐effectiveness of health checkups‐‐an illustrative study. Western Journal of Medicine 1984;141(6):786‐92. [PMC free article] [PubMed] [Google Scholar]
- Collen MF, Dales LG, Friedman GD, Flagle CD, Feldman R, Siegelaub AB. Multiphasic checkup evaluation study. 4. Preliminary cost benefit analysis for middle‐aged men. Preventive Medicine 1973;2(2):236‐46. [DOI] [PubMed] [Google Scholar]
- Cutler JL, Ramcharan S, Feldman R, Siegelaub AB, Campbell B, Friedman GD, et al. Multiphasic checkup evaluation study. 1. Methods and population. Preventive Medicine 1973;2(2):197‐206. [DOI] [PubMed] [Google Scholar]
- Dales LG, Friedman GD, Collen MF. Evaluating periodic multiphasic health checkups: a controlled trial. Journal of Chronic Diseases 1979;32(5):385‐404. [DOI] [PubMed] [Google Scholar]
- Dales LG, Friedman GD, Collen MF. Evaluation of a periodic multiphasic health checkup. Methods of Information in Medicine 1974;13(3):140‐6. [PubMed] [Google Scholar]
- Dales LG, Friedman GD, Ramcharan S, Siegelaub AB, Campbell BA, Feldman R, et al. Multiphasic Checkup Evaluation Study. 3. Outpatient clinic utilization, hospitalization, and mortality experience after seven years. Preventive Medicine 1973;2(2):221‐35. [DOI] [PubMed] [Google Scholar]
- Friedman GD, Collen MF, Fireman BH. Multiphasic Health Checkup Evaluation: a 16‐year follow‐up. Journal of Chronic Diseases 1986;39(6):453‐63. [DOI] [PubMed] [Google Scholar]
- Ramcharan S, Cutler JL, Feldman R, Siegelaub AB, Campbell B, Friedman GD, et al. Multiphasic checkup evaluation study. 2. Disabilty and chronic disease after seven years of multiphasic health checkups. Preventive Medicine 1973;2(2):207‐20. [DOI] [PubMed] [Google Scholar]
- Selby JV, Friedman GD, Collen MF. Sigmoidoscopy and mortality from colorectal cancer: the Kaiser Permanente Multiphasic Evaluation Study. Journal of Clinical Epidemiology 1988;41(5):427‐34. [DOI] [PubMed] [Google Scholar]
Malmö 1969 {published data only}
- Isacsson SO, Janzon L. Results of a quit‐smoking research project in a randomly selected population. Scandinavian Journal of Social Medicine 1976;4(1):25‐9. [DOI] [PubMed] [Google Scholar]
- Lannerstad O. Död och sjukdom bland medelålders män. Malmö: University of Lund, 1978. [Google Scholar]
- Lannerstad O. Morbidity related to smoking and other risk factors. A population study of disability pension, hospital care and sickness benefit days among middle‐aged men in Malmö, Sweden. Scandinavian Journal of Social Medicine 1980;8(1):25‐31. [DOI] [PubMed] [Google Scholar]
- Lannerstad O, Sternby NH, Isacsson SO, Lindgren G, Lindell SE. Effects of a health screening on mortality and causes of death in middle‐aged men. A prospective study from 1970 to 1974 of mean in Malmö, born 1914. Scandinavian Journal of Social Medicine 1977;5(3):137‐40. [DOI] [PubMed] [Google Scholar]
Mankato 1982 {published data only}
- Murray DM, Luepker RV, Pirie PL, Grimm RH, Bloom E, Davis MA, et al. Systematic risk factor screening and education: a community‐wide approach to prevention of coronary heart disease. Preventive Medicine 1986;15(6):661‐72. [DOI] [PubMed] [Google Scholar]
New York 1971 {published data only}
- Fink R, Shapiro S, Rosenberg C. Social research problems in studies involving multiphasic health testing. Health Services Research 1972;7(4):314‐21. [PMC free article] [PubMed] [Google Scholar]
- Shapiro S. Evaluation of two contrasting types of screening programs. Preventive Medicine 1973;2(2):266‐77. [DOI] [PubMed] [Google Scholar]
- Shapiro S, Fink R, Rosenberg C. A program to measure the impact of multiphasic health testing on health differentials between poverty and non‐poverty groups. Medical Care 1972;10(3):207‐14. [DOI] [PubMed] [Google Scholar]
Northumberland 1969 {published data only}
- Bennett AE, Fraser IG. Impact of a screening programme in general practice: a randomized controlled trial. International Journal of Epidemiology 1972;1(1):55‐60. [DOI] [PubMed] [Google Scholar]
OXCHECK 1989 {published and unpublished data}
- Imperial Cancer Research Fund OXCHECK Study Group. Effectiveness of health checks conducted by nurses in primary care: final results of the OXCHECK study. BMJ 1995;310(6987):1099‐104. [PMC free article] [PubMed] [Google Scholar]
- Imperial Cancer Research Fund OXCHECK Study Group. Effectiveness of health checks conducted by nurses in primary care: results of the OXCHECK study after one year. BMJ 1994;308(6924):308‐12. [PMC free article] [PubMed] [Google Scholar]
- Imperial Cancer Research Fund OXCHECK Study Group. Prevalence of risk factors for heart disease in OXCHECK trial: implications for screening in primary care. BMJ 1991;302(6784):1057‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langham S, Thorogood M, Normand C, Muir J, Jones L, Fowler G. Costs and cost effectiveness of health checks conducted by nurses in primary care: the OXCHECK study. BMJ 1996;312(7041):1265‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Neill C. The OXCHECK Study: a nursing perspective. Oxford and Collaborators Health Check. Health Reports 1994;6(1):160‐5. [PubMed] [Google Scholar]
Salt Lake City 1972 {published data only}
- Olsen DM, Kane RL, Proctor PH. A controlled trial of multiphasic screening. New England Journal of Medicine 1976;294(17):925‐30. [DOI] [PubMed] [Google Scholar]
South‐East London 1967 {published data only}
- D'Souza MF, Swan AV, Shannon DJ. A long‐term controlled trial of screening for hypertension in general practice. Lancet 1976;1(7971):1228‐31. [DOI] [PubMed] [Google Scholar]
- Eastwood MR, Trevelyan MH. Relationship between physical and psychiatric disorder. Psychological Medicine 1972;2(4):363‐72. [DOI] [PubMed] [Google Scholar]
- South‐East London Screening Study Group. A controlled trial of multiphasic screening in middle‐age: results of the South‐East London Screening Study. 1977. International Journal of Epidemiology 2001;30(5):935‐40. [DOI] [PubMed] [Google Scholar]
- Stone DH, Crisp AH. The effect of multiphasic screening on aspects of psychiatric status in middle age: results of a controlled trial in general practice. International Journal of Epidemiology 1978;7(4):331‐4. [DOI] [PubMed] [Google Scholar]
- Stone DH, D'Souza MF. Multiphasic screening in middle age: results and implications of a controlled trial in British general practice. Israel Journal of Medical Sciences 1981;17(2‐3):215‐21. [PubMed] [Google Scholar]
- The South‐East London Study Group. A controlled trial of multiphasic screening in middle‐age: results of the South‐East London screening study. International Journal of Epidemiology 1977;6(4):357‐63. [DOI] [PubMed] [Google Scholar]
- Trevelyan H. Study to evaluate the effects of multiphasic screening within general practice in Britain: design and method. Preventive Medicine 1973;2(2):278‐94. [DOI] [PubMed] [Google Scholar]
Stockholm 1969 {published data only}
- Theobald H, Bygren LO, Carstensen J, Hauffman M, Engfeldt P. Effects of an assessment of needs for medical and social services on long‐term mortality: a randomized controlled study. International Journal of Epidemiology 1998;27(2):194‐8. [DOI] [PubMed] [Google Scholar]
Titograd 1971 {published data only}
- Thorner RM, Djordjevic D, Vuckmanovic C, Pesic B, Culafic B, Mark F. A study to evaluate the effectiveness of multiphasic screening in Yugoslavia. Preventive Medicine 1973;2(2):295‐301. [DOI] [PubMed] [Google Scholar]
WHO 1971 {published data only}
- Kornitzer M, Rose G. WHO European collaborative trial of multifactorial prevention of coronary heart disease. Preventive Medicine 1985;14(3):272‐8. [DOI] [PubMed] [Google Scholar]
- Rose G. European collaborative trial of multifactorial prevention of coronary heart disease. Lancet 1987;1(8534):685. [DOI] [PubMed] [Google Scholar]
- World Health Organization European Collaborative Group. An international controlled trial in the multifactorial prevention of coronary heart disease. International Journal of Epidemiology 1974;3(3):219‐24. [DOI] [PubMed] [Google Scholar]
- World Health Organization European Collaborative Group. European collaborative trial of multifactorial prevention of coronary heart disease: final report on the 6‐year results. Lancet 1986;1(8486):869‐72. [PubMed] [Google Scholar]
- World Health Organization European Collaborative Group. Multifactorial trial in the prevention of coronary heart disease: 1. recruitment and initial findings. European Heart Journal 1980;1(1):73‐80. [PubMed] [Google Scholar]
- World Health Organization European Collaborative Group. Multifactorial trial in the prevention of coronary heart disease: 2. risk factor changes at two and four years. European Heart Journal 1982;3(2):184‐90. [PubMed] [Google Scholar]
- World Health Organization European Collaborative Group. Multifactorial trial in the prevention of coronary heart disease: 3. incidence and mortality results. European Heart Journal 1983;4(3):141‐7. [PubMed] [Google Scholar]
- World Health Organization European Collaborative Group. WHO European collaborative trial in the multifactorial prevention of coronary heart disease. Copenhagen (Denmark): World Health Organization 1989. [PubMed]
- World Health Organization European Collaborative Group. WHO European collaborative trial in the multifactorial prevention of coronary heart disease. IARC Scientific Publications 1990;103:123‐31. [PubMed] [Google Scholar]
References to studies excluded from this review
ACTRN12610000511033 {published data only}
- ACTRN12610000511033. A randomised controlled trial on the effect of My Health Check, a new interactive web‐based decision tool, on the adoption of health preventive behaviours in volunteers aged 30‐69 years. www.anzctr.org.au (First received 31 January 2018).
Ajay 2014 {published data only}
- Ajay VS, Tian M, Chen H, Wu Y, Li X, Dunzhu D, et al. A cluster‐randomized controlled trial to evaluate the effects of a simplified cardiovascular management program in Tibet, China and Haryana, India: study design and rationale. BMC public health 2014;14:924. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ayorinde 2013 {published data only}
- Ayorinde AA, Porteous T, Sharma P. Screening for major diseases in community pharmacies: a systematic review. International Journal of Pharmacy Practice 2013;21:349‐61. [DOI: ] [DOI] [PubMed] [Google Scholar]
Baicker 2013 {published data only}
- Baicker K, Taubman SL, Allen HL, Bernstein M, Gruber JH, Newhouse JP, et al. Oregon Health Study Group. The Oregon experiment ‐ effects of medicaid on clinical outcomes. New England Journal of Medicine 2013;368:1713‐22. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Barry 2017 {published data only}
- Barry E, Roberts S, Oke J, Vijayaraghavan S, Normansell R, Greenhalgh T. Efficacy and effectiveness of screen and treat policies in prevention of type 2 diabetes: systematic review and meta‐analysis of screening tests and interventions. BMJ 2017;356:i6538. [DOI: ] [DOI] [PubMed] [Google Scholar]
Bender 2015b {published data only}
- Bender AM, Kawachi I, Jørgensen T, Pisinger C. Neighborhood deprivation is strongly associated with participation in a population‐based health check. PLoS ONE 2015;10(6):e0129819. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Brett 2012 {published data only}
- Brett T, Arnold‐Reed D, Phan C, Cadden F, Walker W, Manea‐Walley W, et al. The Fremantle Primary PreventionStudy: a multicentre randomised trial of absolute cardiovascular risk reduction.. British Journal of General Practice 2012;62(594):e22‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Caley 2014 {published data only}
- Caley M, Chohan P, Hooper J, Wright N. The impact of NHS Health Checks on the prevalence of disease in general practices: a controlled study. British Journal of General Practice 2014;64:e516‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Campbell Scherer 2014 {published data only}
- Campbell‐Scherer D, Rogers J, Manca D, Lang‐Robertson K, Bell S, Salvalaggio G, et al. Guideline harmonization and implementation plan for the BETTER trial: building on existing tools to improve chronic disease prevention and screening in family practice. CMAJ Open 2014;2:E1‐E10. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Carter 2016 {published data only}
- Carter P, Bodicoat DH, Davies MJ, Ashra NB, Riley D, Joshi N, et al. A retrospective evaluation of the NHS Health Check Programme in a multi‐ethnic population. Journal of Public Health 2016;38:534‐42. [DOI: 10.1093/pubmed/fdv115] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chang 2016 {published data only}
- Chang KC, Lee JT, Vamos EP, Soljak M, Johnston D, Khunti K, et al. Impact of the National Health Service Health Check on cardiovascular disease risk: a difference‐in‐differences matching analysis. CMAJ Open 2016;188:E228‐38. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Charles 2012 {published data only}
- Charles M, Simmons RK, Williams KM, Roglic G, Sharp SJ, Kinmonth AL, et al. Cardiovascular risk reduction following diagnosis of diabetes by screening: 1‐year results from the ADDITION‐Cambridge trial cohort. British Journal of General Practice 2012;62:e396‐e402. [DOI] [PMC free article] [PubMed] [Google Scholar]
Charles 2013 {published data only}
- Charles M, Fleischer J, Witte DR, Ejskjaer N, Borch‐Johnsen K, Lauritzen T, et al. Impact of early detection and treatment of diabetes on the 6‐year prevalence of cardiac autonomic neuropathy in people with screen‐detected diabetes: ADDITION‐Denmark, a cluster‐randomised study. Diabetologia 2013;56:101‐8. [DOI] [PubMed] [Google Scholar]
Cochrane 2012 {published data only}
- Cochrane T, Davey R, Iqbal Z, Gidlow C, Kumar J, Chambers R, et al. NHS health checks through general practice: randomised trial of population cardiovascular risk reduction. BMC public health 2012;12:944. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dalsgaard 2014 {published data only}
- Dalsgaard EM, Vestergaard M, Skriver MV, Maindal HT, Lauritzen T, Borch‐Johnsen K, et al. Psychological distress, cardiovascular complications and mortality among people with screen‐detected type 2 diabetes: follow‐up of the ADDITION‐Denmark trial. Diabetologia 2014;57:710‐7. [DOI: ] [DOI] [PubMed] [Google Scholar]
Davis Lameloise 2013 {published data only}
- Davis‐Lameloise N, Hernan A, Janus ED, Stewart E, Carter R, Bennett CM, et al. Melbourne Diabetes Prevention Study (MDPS) research group. The Melbourne Diabetes Prevention Study (MDPS): study protocol for a randomized controlled trial. Trials 2013;14:31. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Diederichsen 2015 {published data only}
- Diederichsen AC, Rasmussen LM, Søgaard R, Lambrechtsen J, Steffensen FH, Frost L, et al. The Danish Cardiovascular Screening Trial (DANCAVAS): study protocol for a randomized controlled trial. Trials 2015;16:554. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dirven 2013 {published data only}
- Dirven JA, Tange HJ, Muris JW, Haaren KM, Vink G, Schayck OC. Early detection of COPD in general practice: patient or practice managed? A randomised controlled trial of two strategies in different socioeconomic environments. Primary Care Respiratory Journal 2013;22:331‐7. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Doughty 2014 {published data only}
- Doughty RN. Randomised controlled trial: community screening for heart failure: ready for prime time?. Evidence‐Based Medicine 2014;19:107. [DOI: ] [DOI] [PubMed] [Google Scholar]
Duncan 2016 {published data only}
- Duncan S, Goodyear‐Smith F, McPhee J, Zinn C, Grøntved A, Schofield G. Family‐centered brief intervention for reducing obesity and cardiovascular disease risk: a randomized controlled trial. Obesity (Silver Spring, Md.) 2016;24:2311‐18. [DOI] [PubMed] [Google Scholar]
Dyakova 2016 {published data only}
- Dyakova M, Shantikumar S, Colquitt JL, Drew CM, Sime M, MacIver J, et al. Systematic versus opportunistic risk assessment for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews 2016, Issue 2. [DOI: 10.1002/14651858.CD010411.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Echouffo Tcheugui 2015 {published data only}
- Echouffo‐Tcheugui JB, Simmons RK, Prevost AT, Williams KM, Kinmonth AL, Wareham NJ, et al. Long‐term effect of population screening for diabetes on cardiovascular morbidity, self‐rated health, and health behavior. Annals of Family Medicine 2015;13:149‐57. [DOI] [PMC free article] [PubMed] [Google Scholar]
Engelsen 2014 {published data only}
- Engelsen C, Koekkoek PS, Godefrooij MB, Spigt MG, Rutten GE. Screening for increased cardiometabolic risk in primary care: a systematic review. British Journal of General Practice 2014;64(627):e616‐e626. [DOI] [PMC free article] [PubMed] [Google Scholar]
Grunfeld 2013 {published data only}
- Grunfeld E, Manca D, Moineddin R, Thorpe KE, Hoch JS, Campbell‐Scherer D, et al. BETTER Trial Investigators. Improving chronic disease prevention and screening in primary care: results of the BETTER pragmatic cluster randomized controlled trial. BMC Family Practice 2013;14:175. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Haas 2016 {published data only}
- Haas J. Randomized trial of a personalized multi‐condition risk assessment in primary care. International Journal for Quality in Health Care 2016;28 (Supplement 1):42‐3. [DOI: ] [Google Scholar]
Haas 2017 {published data only}
- Haas JS, Baer HJ, Eibensteiner K, Klinger EV, Hubert S, Getty G, et al. A cluster randomized trial of a personalized multi‐condition risk assessment in primary care. American Journal of Preventive Medicine 2017;52:100‐5. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Harris 2012 {published data only}
- Harris MF, Fanaian M, Jayasinghe UW, Passey ME, McKenzie SH, Powell Davies G, et al. A cluster randomised controlled trial of vascular risk factor management in general practice. Medical Journal of Australia 2012;197:387‐93. [DOI] [PubMed] [Google Scholar]
Harris 2017 {published data only}
- Harris MF, Parker SM, Litt J, Driel M, Russell G, Mazza D, et al. Preventive Evidence into Practice Partnership Group. An Australian general practice based strategy to improve chronic disease prevention, and its impact on patient reported outcomes: evaluation of the preventive evidence into practice cluster randomised controlled trial. BMC Health Services Research 2017;17:637. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Herman 2012 {published data only}
- Herman PM, Szczurko O, Cooley K, Seely D. A naturopathic approach to the prevention of cardiovascular disease: a cost effectiveness analysis of a randomized multi‐worksite trial. BMC Complementary and Alternative Medicine. Conference: International Research Congress on Integrative Medicine and Health 2012;12 Suppl 1:O25. [Google Scholar]
Herman 2014 {published data only}
- Herman PM, Szczurko O, Cooley K, Seely D. A naturopathic approach to the prevention of cardiovascular disease: cost‐effectiveness analysis of a pragmatic multi‐worksite randomized clinical trial. Journal of Occupational and Environmental Medicine / American College of Occupational and Environmental Medicine 2014;56:171‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Herrigel 2014 {published data only}
- Herrigel DJ, Willett LR, Jørgensen T. 2014 ‐ Intensive population‐level screening and counseling did not reduce ischemic heart disease at 10 years. ACP Journal Club 2014;161:2. [DOI] [PubMed] [Google Scholar]
Høj 2014 {published data only}
- Høj K, Skriver MV, Hansen AL, Christensen B, Maindal HT, Sandbæk A. Effect of including fitness testing in preventive health checks on cardiorespiratory fitness and motivation: study protocol of a randomized controlled trial. BMC public health 2014;14:1057. [DOI] [PMC free article] [PubMed] [Google Scholar]
Høj 2018 {published data only}
- Høj K, Vinther Skriver M, Terkildsen Maindal H, Christensen B, Sandbæk A. The effect of cardiorespiratory fitness assessment in preventive health checks: a randomised controlled trial. European Journal of Public Health 2018;28:173‐9. [DOI: ] [DOI] [PubMed] [Google Scholar]
Ijkema 2014 {published data only}
- Ijkema R, Aerde MA, Aalst CM, Ballegooijen M, Oudkerk M, Koning HJ. A randomized controlled trial measuring the effectiveness of screening for cardiovascular disease using classic risk assessment and coronary artery calcium: the ROBINSCA study. European Journal of Preventive Cardiology 2014;21:S21. [Google Scholar]
ISRCTN11833436 {published data only}
- ISRCTN11833436. Impact evaluation of Oportunidades. www.isrctn.com (First received 31 January 2018).
Kaczorowski 2011 {published data only}
- Kaczorowski J, Chambers L, Dolovich L, Paterson JM, Karwalajtys T, Gierman T, et al. Improving cardiovascular health at population level: 39 community cluster randomised trial of Cardiovascular Health Awareness Program (CHAP). BMJ 2011;342:d442. [DOI] [PMC free article] [PubMed] [Google Scholar]
Khetan 2017 {published data only}
- Khetan AK, Purushothaman R, Chami T, Hejjaji V, Madan Mohan SK, Josephson RA, et al. The effectiveness of community health workers for CVD prevention in LMIC. Global Heart 2017;12:233‐243.e6. [DOI: ] [DOI] [PubMed] [Google Scholar]
Kozela 2012 {published data only}
- Kozela M, Szafraniec K, Broda G, Cichocka I, Drygas W, Gąsior Z, et al. POLKARD Study Group. Detection and treatment of hypercholesterolemia in primary health care: results of the POLKARD program of the Ministry of Health of the Republic of Poland. Polskie Archiwum Medycyny Wewnetrznej 2012;122:154‐61. [DOI] [PubMed] [Google Scholar]
Lindholt 2017 {published data only}
- Lindholt JS, Søgaard R. Population screening and intervention for vascular disease in Danish men (VIVA): a randomised controlled trial. Lancet 2017;390:2256‐65. [DOI] [PubMed] [Google Scholar]
Lindsay 2013 {published data only}
- Lindsay P, Connor Gorber S, Joffres M, Birtwhistle R, McKay D, Cloutier L, Canadian Task Force on Preventive Health Care (CTFPHC). Recommendations on screening for high blood pressure in Canadian adults. Canadian Family Physician Medecin de Famille Canadien 2013;59:927‐33, e393‐400. [PMC free article] [PubMed] [Google Scholar]
Mar 2014 {published data only}
- Mar C. Review: Primary care–based general health checks improve surrogate but not clinical outcomes. ACP Journal Club 2014;160:1‐1. [DOI] [PubMed] [Google Scholar]
McDermott 2016 {published data only}
- McDermott L, Wright AJ, Cornelius V, Burgess C, Forster AS, Ashworth M, et al. Enhanced invitation methods and uptake of health checks in primary care: randomised controlled trial and cohort study using electronic health records. Health Technology Assessment 2016;20(84):1‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
McKenzie 2013 {published data only}
- McKenzie SH, Jayasinghe UW, Fanaian M, Passey M, Harris MF. Analysis of the psychological impact of a vascular risk factor intervention: results from a cluster randomized controlled trial in Australian general practice. BMC Family Practice 2013;14:190. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT02224248 {published data only}
- NCT02224248. Effect of including fitness testing in preventive health checks on cardiorespiratory fitness and motivation. www.clinicaltrials.gov (First received 31 January 2018).
NCT02615769 {published data only}
- NCT02615769. Effect on attendance if including focused information of spirometry in preventive health checks. www.clinicaltrials.gov (First received 31 January 2018).
NTR2379 {published data only}
- NTR2379. The effectiveness of health check‐ups for promoting healthy behavior: a quasi‐experimental study. www.trialregister.nl (First received 31 January 2018).
Oldenburg 2015 {published data only}
- Oldenburg B, Sathish T, Thankappan KR, Balachandran S, D'Esposito F, Mathews E, et al. Identifying people at high risk for type 2 diabetes: preliminary results from the Kerala Diabetes Prevention Programme. Diabetologia 2015;58:S166. [Google Scholar]
Orts 2016 {published data only}
- Ørts LM, Løkke A, Bjerregaard AL, Maindal HT, Sandbæk A. Effect on attendance by including focused information on spirometry in preventive health checks: study protocol for a randomized controlled trial. Trials 2016;17(1):571. [DOI] [PMC free article] [PubMed] [Google Scholar]
Panniyammakal 2017 {published data only}
- Panniyammakal P, Harikrihnan S, Prabhakaran D. A PROgramme of lifestyle Intervention in families for cardiovascular risk reduction (PROLIFIC Study): design and rationale of a family based randomized controlled trial. European Journal of Preventive Cardiology. Conference: Europrevent 2017. Spain 2017;24:S27. [DOI] [PMC free article] [PubMed] [Google Scholar]
Paszat 2017 {published data only}
- Paszat L, Sutradhar R, O'Brien MA, Lofters A, Pinto A, Selby P, et al. BETTER HEALTH: Durham ‐‐ protocol for a cluster randomized trial of BETTER in community and public health settings. BMC Public Health 2017;17:754. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rodondi 2012 {published data only}
- Rodondi N, Auer R, Bosset Sulzer V, Ghali WA, Cornuz J. Atherosclerosis screening by noninvasive imaging for cardiovascular prevention: a systematic review. Journal of General Internal Medicine 2012;27:220‐31. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Si 2014 {published data only}
- Si S, Moss JR, Sullivan TR, Newton SS, Stocks NP. Effectiveness of general practice‐based health checks: a systematic review and meta‐analysis. British Journal of General Practice 2014;64:e47‐e53. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Simmons 2012 {published data only}
- Simmons RK, Echouffo‐Tcheugui JB, Sharp SJ, Sargeant LA, Williams KM, Prevost AT, et al. Screening for type 2 diabetes and population mortality over 10 years (ADDITION‐Cambridge): a cluster‐randomised controlled trial. Lancet 2012;380:1741‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Simmons 2017 {published data only}
- Simmons RK, Griffin SJ, Witte DR, Borch‐Johnsen K, Lauritzen T, Sandbæk A. Effect of population screening for type 2 diabetes and cardiovascular risk factors on mortality rate and cardiovascular events: a controlled trial among 1,912,392 Danish adults. Diabetologia 2017;60(11):2183‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stickler 2000 {published data only}
- Stickler GB. Are yearly physical examinations in adolescents necessary?. Journal of the American Board of Family Practice 2000;13(3):172‐7. [DOI] [PubMed] [Google Scholar]
Yan 2013 {published data only}
- Yan LL, Fang W, Delong E, Yao C, Neal B, Peterson ED, et al. China rural health initiative ‐ primary care provider study: a large cluster‐randomized controlled trial of high cardiovascular risk management in rural China. Circulation 2013;128:2715‐16. [Google Scholar]
References to ongoing studies
Check Your Health {published data only}
- Maindal HT, Støvring H, Sandbaek A. Effectiveness of the population‐based Check Your Health preventive programme conducted in primary care with 4 years follow‐up [the COREtrial]: study protocol for a randomised controlled trial. Trials 2014;15:341. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT01979107 {published data only}
- NCT01979107. Early detection of and intervention towards chronic diseases among individuals without formal education. www.clinicaltrials.gov (First received 31 January 2018).
Additional references
Barger 2006
- Barger SD, Muldoon MF. Hypertension labelling was associated with poorer self‐rated health in the Third US National Health and Nutrition Examination Survey. Journal of Human Hypertension 2006;20(2):117‐23. [PUBMED: 16267563] [DOI] [PubMed] [Google Scholar]
Ben‐Shlomo 1994
- Ben‐Shlomo Y, Smith GD, Shipley MJ, Marmot MG. What determines mortality risk in male former cigarette smokers?. American Journal of Public Health 1994;84(8):1235‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bender 2015a
- Bender AM, Jørgensen T, Pisinger C. Is self‐selection the main driver of positive interpretations of general health checks? The Inter99 randomized trial. Preventive Medicine 2015;81:42‐8. [DOI] [PubMed] [Google Scholar]
Beswick 2008
- Beswick AD, Rees K, Dieppe P, Ayis S, Gooberman‐Hill R, Horwood J, et al. Complex interventions to improve physical function and maintain independent living in elderly people: a systematic review and meta‐analysis. Lancet 2008;371(9614):725‐35. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bloom 1981
- Bloom JR, Monterossa S. Hypertension labeling and sense of well‐being. American Journal of Public Health 1981;71(11):1228‐32. [DOI] [PMC free article] [PubMed] [Google Scholar]
Boulware 2007
- Boulware LE, Marinopoulos S, Phillips KA, Hwang CW, Maynor K, Merenstein D, et al. Systematic review: the value of the periodic health evaluation. Annals of Internal Medicine 2007;146(4):289‐300. [DOI] [PubMed] [Google Scholar]
Brewer 2007
- Brewer NT, Salz T, Lillie SE. Systematic review: the long‐term effects of false‐positive mammograms. Annals of Internal Medicine 2007;146(7):502‐10. [PUBMED: 17404352] [DOI] [PubMed] [Google Scholar]
Collins 2011
- Collins RE, Lopez LM, Marteau TM. Emotional impact of screening: a systematic review and meta‐analysis. BMC Public Health 2011;11:603. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cook 1986
- Cook DG, Shaper AG, Pocock SJ, Kussick SJ. Giving up smoking and the risk of heart attacks. Lancet 1986;2(8520):1376‐80. [DOI] [PubMed] [Google Scholar]
Ebrahim 2011
- Ebrahim S, Taylor F, Ward K, Beswick A, Burke M, Davey Smith G. Multiple risk factor interventions for primary prevention of coronary heart disease. Cochrane Database of Systematic Reviews 2011, Issue 1. [DOI: 10.1002/14651858.CD001561.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Engberg 2002
- Engberg M, Christensen B, Karlsmose B, Lauritzen T. Re: Should general health surveys be offered to the population?. Ugeskrift for Laeger 2002;164(36):4200‐1. [PubMed] [Google Scholar]
FDA 2018
- US Food, Drug Administration. Full‐body CT scans ‐ what you need to know. www.fda.gov/Radiation‐EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX‐Rays/ucm115340.htm (accessed 22 March 2018).
Fleming 1996
- Fleming TR, DeMets DL. Surrogate end points in clinical trials ‐ are we being misled?. Annals of Internal Medicine 1996;125(7):605‐13. [DOI] [PubMed] [Google Scholar]
Friedman 1986
- Friedman GD, Collen MF, Fireman BH. Multiphasic Health Checkup Evaluation: a 16‐year follow‐up. Journal of Chronic Diseases 1986;39(6):453‐63. [DOI] [PubMed] [Google Scholar]
Furtado 2005
- Furtado CD, Aguirre DA, Sirlin CB, Dang D, Stamato SK, Lee P, et al. Whole‐body CT screening: spectrum of findings and recommendations in 1192 patients. Radiology 2005;237(2):385‐94. [DOI] [PubMed] [Google Scholar]
Golomb 2012
- Golomb BA, Evans MA, Dimsdale JE, White HL. Effects of statins on energy and fatigue with exertion: results from a randomized controlled trial. Archives of Internal Medicine 2012;172(15):1180‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version Accessed 20 January 2019. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Grønhøj Larsen 2012
- Grønhøj Larsen C, Jørgensen KJ, Gøtzsche PC. Regular health checks: cross sectional survey. PloS One 2012;7(3):e33694. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hamer 2010
- Hamer M, Batty GD, Stamatakis E, Kivimaki M. Hypertension awareness and psychological distress. Hypertension 2010;56:547‐50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Han 1997
- Han PK. Historical changes in the objectives of the periodic health examination. Annals of Internal Medicine 1997;127(10):910‐7. [DOI] [PubMed] [Google Scholar]
Haynes 1978
- Haynes RB, Sackett DL, Taylor DW, Gibson ES, Johnson AL. Increased absenteeism from work after detection and labelling of hypertensive patients. New England Journal of Medicine 1978;299(14):741‐4. [PUBMED: 692548] [DOI] [PubMed] [Google Scholar]
Healy 2004
- Healy D. Let Them Eat Prozac. New York and London: New York University Press, 2004. [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2017
- Higgins JP, Altman DG, Sterne JA (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Holland 2009
- Holland WW. Periodic health examination ‐ a brief history and critical assessment. Eurohealth 2009;15(4):16‐20. [Google Scholar]
Holme 2013
- Holme Ø, Bretthauer M, Fretheim A, Odgaard‐Jensen J, Hoff G. Flexible sigmoidoscopy versus faecal occult blood testing for colorectal cancer screening in asymptomatic individuals. Cochrane Database of Systematic Reviews 2013, Issue 9. [DOI: 10.1002/14651858.CD009259.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hooper 2011
- Hooper L, Summerbell CD, Thompson R, Sills D, Roberts FG, Moore H, et al. Reduced or modified dietary fat for preventing cardiovascular disease. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD002137.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hooper 2015
- Hooper L, Martin N, Abdelhamid A, Davey Smith G. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database of Systematic Reviews 2015, Issue 6. [DOI: 10.1002/14651858.CD011737] [DOI] [PubMed] [Google Scholar]
Ilic 2013
- Ilic D, Neuberger M, Djulbegovic M, Dahm P. Screening for prostate cancer. Cochrane Database of Systematic Reviews 2013, Issue 1. [DOI: 10.1002/14651858.CD004720.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jørgensen 2003
- Jørgensen T, Borch‐Johnsen K, Thomsen TF, Ibsen H, Glümer C, Pisinger C. A randomized non‐pharmacological intervention study for prevention of ischaemic heart disease: baseline results Inter99. European Journal of Cardiovascular Prevention and Rehabilitation 2003;10(5):377‐86. [DOI] [PubMed] [Google Scholar]
Jørgensen 2014
- Jørgensen AW, Lundstrøm LH, Wetterslev J, Astrup A, Gøtzsche PC. Comparison of results from different imputation techniques for missing data from an anti‐obesity drug trial. PLoS One 2014;9(11):e111964. [DOI] [PMC free article] [PubMed] [Google Scholar]
Karmali 2017
- Karmali KN, Persell SD, Perel P, Lloyd‐Jones DM, Berendsen MA, Huffman MD. Risk scoring for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews 2017, Issue 3. [DOI: 10.1002/14651858.CD006887.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lauritzen 2012
- Lauritzen T. [Helbredsundersøgelser og samtaler reducerer deltagernes risikoscore for hjerte‐kar‐sygdom]. Månedsskrift for Almen Praksis 2012;90(3):245‐50. [Google Scholar]
Lehman 2010
- Lehman R, Yudkin JS, Krumholz H. Licensing drugs for diabetes. BMJ 2010;341:c4805. [DOI] [PubMed] [Google Scholar]
Martin 2018
- Martin RM, Donovan JL, Turner EL, Metcalfe C, Young GJ, Walsh EI, et al. Effect of a low‐intensity PSA‐based screening interventionon prostate cancer mortality: the CAP randomized clinical trial. JAMA 2018;319(9):883‐95. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nakao 2018
- Nakao Y, Miyamoto Y, Ueshima K, Nakao K, Nakai M, Nishimura K, et al. Effectiveness of nationwide screening and lifestyle intervention for abdominal obesity and cardiometabolic risks in Japan: the metabolic syndrome and comprehensive lifestyle intervention study on nationwide database in Japan (MetS ACTION‐J study). PLoS One 2018;13(1):e0190862. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nissen 2010
- Nissen SE, Wolski K. Rosiglitazone revisited. An updated meta‐analysis of risk for myocardial infarction and cardiovascular mortality. Archives of Internal Medicine 2010;170(14):1191‐201. [DOI] [PubMed] [Google Scholar]
Patrick 1999
- Patrick DL, Grembowski D, Durham M, Beresford SA, Diehr P, Ehreth J, et al. Cost and outcomes of Medicare reimbursement for HMO preventive services. Health Care Financing Review 1999;20(4):25‐43. [PMC free article] [PubMed] [Google Scholar]
Pill 1988
- Pill R, French J, Harding K, Stott N. Invitation to attend a health check in a general practice setting: comparison of attenders and non‐attenders. Journal of the Royal College of General Practitioners 1988;38(307):53‐6. [PMC free article] [PubMed] [Google Scholar]
Piper 2015
- Piper M, Evans CV, Burda BU, Margolis KL, O'Connor E, Whitlock EP. Diagnostic and predictive accuracy of blood pressure screening methods with consideration of rescreening intervals: a systematic review for the U.S. Preventive Services Task Force. Annals of Internal Medicine 2015;162(3):192‐204. [DOI] [PubMed] [Google Scholar]
Pisinger 2009
- Pisinger C, Ladelund S, Glümer C, Toft U, Aadahl M, Jørgensen T. Five years of lifestyle intervention improved self‐reported mental and physical health in a general population: the Inter99 study. Preventive Medicine 2009;49(5):424‐8. [DOI] [PubMed] [Google Scholar]
Raffle 2007
- Raffle A, Gray M. Screening: Evidence and Practice. New York: Oxford University Press, 2007. [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Robson 2016
- Robson J, Dostal I, Sheikh A, Eldridge S, Madurasinghe V, Griffiths C, et al. The NHS Health Check in England: an evaluation of the first 4 years. BMJ Open 2016;6(1):e008840. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schünemann 2017
- Schünemann HJ, Oxman AD, Higgins JP, Vist GE, Glasziou P, Akl E, et al. on behalf of the Cochrane GRADEing Methods Group and the Cochrane Statistical Methods Group. Chapter 11: Completing ‘Summary of findings’ tables and grading the confidence in or quality of the evidence. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Selph 2015
- Selph S, Dana T, Blazina I, Bougatsos C, Patel H, Chou R. Screening for type 2 diabetes mellitus: a systematic review for the U.S. Preventive Services Task Force. Annals of Internal Medicine 2015;162(11):765‐76. [DOI] [PubMed] [Google Scholar]
Shaw 1999
- Shaw C, Abrams K, Marteau TM. Psychological impact of predicting individuals' risks of illness: a systematic review. Social Science & Medicine 1999;49(12):1571‐98. [DOI] [PubMed] [Google Scholar]
Sheridan 2003
- Sheridan S, Pignone M, Donahue K. Screening for high blood pressure: a review of the evidence for the U.S. Preventive Services Task Force. American Journal of Preventive Medicine 2003;25(2):151‐8. [PUBMED: 12880884] [DOI] [PubMed] [Google Scholar]
Sheridan 2008
- Sheridan SL, Crespo E. Does the routine use of global coronary heart disease risk scores translate into clinical benefits or harms? A systematic review of the literature. BMC Health Services Research 2008;8:60. [DOI: 10.1186/1472-6963-8-60] [DOI] [PMC free article] [PubMed] [Google Scholar]
Simpson 2006
- Simpson SH, Eurich DT, Majumdar SR, Padwal RS, Tsuyuki RT, Varney J, et al. A meta‐analysis of the association between adherence to drug therapy and mortality. BMJ 2006;333(7557):15. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stead 2013
- Stead LF, Buitrago D, Preciado N, Sanchez G, Hartmann‐Boyce J, Lancaster T. Physician advice for smoking cessation. Cochrane Database of Systematic Reviews 2013, Issue 5. [DOI: 10.1002/14651858.CD000165.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Taylor 2013
- Taylor F, Huffman MD, Macedo AF, Moore THM, Burke M, Davey Smith G, et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews 2013, Issue 1. [DOI: 10.1002/14651858.CD004816.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Trevelyan 1973
- Trevelyan H. Study to evaluate the effects of multiphasic screening within general practice in Britain: design and method. Preventive Medicine 1973;2(2):278‐94. [DOI] [PubMed] [Google Scholar]
Uijen 2007
- Uijen AA, Bakx JC, Mokkink HG, Weel C. Hypertension patients participating in trials differ in many aspects from patients treated in general practices. Journal of Clinical Epidemiology 2007;60(4):330‐5. [DOI] [PubMed] [Google Scholar]
UK National Screening Committee 2010
- UK National Screening Committee. Programme appraisal criteria. www.screening.nhs.uk/criteria (accessed 3 August 2012).
Waller 1990
- Waller D, Agass M, Mant D, Coulter A, Fuller A, Jones L. Health checks in general practice: another example of inverse care?. BMJ 1990;300(6732):1115‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Walter 2013
- Walter LC, Fung KZ, Kirby KA, Shi Y, Espaldon R, O'Brien S, et al. Five‐year downstream outcomes following prostate‐specific antigen screening in older men. JAMA Internal Medicine 2013;173(10):866‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Welch 2004
- Welch HG. Should I be tested for cancer? Maybe not and here's why. Berkeley: University of California Press, 2004. [Google Scholar]
Welch 2011
- Welch HG, Schwartz LM, Woloshin S. Overdiagnosed ‐ Making people sick in the pursuit of health. Boston: Beacon Press, 2011. [Google Scholar]
WHO 1984
- Oliver MF, Heady JA, Morris JN, Cooper J, on behalf of the Committee of Principal Investigators. WHO cooperative trial on primary prevention of ischaemic heart disease with clofibrate to lower serum cholesterol: final mortality follow‐up. Report of the Committee of Principal Investigators. Lancet 1984;2(8403):600‐4. [PubMed] [Google Scholar]
Wright 2009
- Wright JM, Musini VM. First‐line drugs for hypertension. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD001841.pub2] [DOI] [PubMed] [Google Scholar]
Xiong 2005
- Xiong T, Richardson M, Woodroffe R, Halligan S, Morton D, Lilford RJ. Incidental lesions found on CT colonography: their nature and frequency. The British Journal of Radiology 2005;78(925):22‐9. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Krogsbøll 2011
- Krogsbøll LT, Jørgensen KJ, Gøtzsche PC. General health checks for reducing morbidity and mortality from disease. Cochrane Database of Systematic Reviews 2011, Issue 2. [DOI: 10.1002/14651858.CD009009] [DOI] [Google Scholar]
Krogsbøll 2012
- Krogsbøll LT, Jørgensen KJ, Grønhøj Larsen C, Gøtzsche PC. General health checks in adults for reducing morbidity and mortality from disease. Cochrane Database of Systematic Reviews 2012, Issue 10. [DOI: 10.1002/14651858.CD009009.pub2] [DOI] [PubMed] [Google Scholar]