

Summary
Background
Type 2 diabetes mellitus (T2DM) is a common disease; the total number of diabetes patients is expected to reach 366 million by 2030. Magnesium has received considerable attention for its potential role in improving insulin sensitivity and preventing diabetes and its cardiovascular complications. Hypomagnesaemia is linked to poor control of type 2 diabetes mellitus, and depletion of serum magnesium occurs exponentially with duration of disease. The aim of this study was to measure serum magnesium level and the correlation of magnesium level with HbA1c in type 2 diabetes mellitus.
Methods
In this cross‐sectional study, we included 100 diabetic patients; blood is taken for measurement of both magnesium and HbA1c levels. Patients with risk factors of magnesium deficiency were not included.
Results
Of the total 100 patients recruited in our study, majority had diabetes for 8.0 years duration. The mean age of the patients was 53.97 ± 10.65 years, most of them were on oral hypoglycaemic agents (84.9%) followed by combination of oral hypoglycaemic agents and insulin (10.5%), and a small percentage were on insulin alone (4.7%). The mean of serum magnesium and HbA1c levels was 1.88 ± 0.25 mg/dL and 8.38% ± 1.53%, respectively. The majority of the patients had a normal level of magnesium (95.0%); however, most of them had uncontrolled blood glucose (82.0%). The study showed that the serum magnesium level and HbA1c are not significantly correlated (P = 0.462).
Conclusion
Normal magnesium levels were observed in majority of patients, there is no significant correlation between serum magnesium and HbA1c levels in patients with T2DM, but larger‐scale clinical trials are needed in future.
Keywords: HbA1c, magnesium, type 2 DM
1. INTRODUCTION
Type 2 diabetes mellitus (T2DM) is a chronic disease resulting from a complex inheritance‐environmental interaction along with other risk factors such as obesity and a sedentary lifestyle.1 The total number of diabetes is expected to reach 366 million by 2030.2 A high prevalence rate has been observed in developing countries and in populations undergoing “westernization” or modernization.1 In Iraq, the prevalence increased from 5% in 1978 to 19.7% in 2012.3
In spite of innovative methods in the management of diabetes mellitus, the morbidity and mortality continue to be high.4 The deleterious effect of diabetes in these patients is related to complications, including both macrovascular and microvascular complications.5, 6 Diet is widely believed to play an important role in the development of type 2 diabetes (T2D) and the associated complications.5, 6
The glycated haemoglobin (HbA1c) is widely used for evaluation of diabetes control.7 The HbA1c reveals the overall blood glucose levels over a period of 2‐3 months, and the common use of the HbA1c assay is to assess changes in metabolic control that follow an alteration in treatment.8
Magnesium (Mg) is one of the important components of many foods such as grains, nuts and green leafy vegetables, and it plays a key role in many fundamental biological processes, including energy metabolism. Mg has received considerable attention for its potential role in improving insulin sensitivity and preventing diabetes and its cardiovascular complications.9, 10 It is claimed that Mg deficiency is common in diabetic patients and there is an inverse relationship between Mg intake and incidence of T2DM.13
It was founded that poor glycaemic control, insulin resistance and low Mg level were strongly associated with increased the prevalence of microalbuminuria.14 Hypomagnesaemia is linked to poor control of type 2 diabetes mellitus, and depletion of serum magnesium occurs exponentially with duration of disease.15 It is now established that diabetes can by itself induce hypomagnesaemia which in turn induces or worsens diabetes mellitus.16
Although the assessment of serum magnesium level has been reported in many studies from various countries, the comparative studies within the diabetic population based on glycaemic control are limited. For this reason, we decided to study the level of serum magnesium in T2DM.
1.1. Aim of the study
The aim of this study was to find the correlation between magnesium and HbA1c levels in type 2 diabetes mellitus.
2. METHODS
2.1. Study design and sampling
This is a cross‐sectional study, which included 100 patients with type 2 DM, each week approximately 5‐7 patients were selected randomly, aged between 30 and 70 during the period of 6 months (January 2018 to June 2018).
The study conducted at Azadi Teaching Hospital at the department of internal medicine in cooperation with Duhok General Directorate of Health. All patients’ participating in this study signed informed consent to have their data collected and used for research. This study was approved by the Duhok General Directorate of Health Ethics Committee.
2.1.1. Inclusion criteria
All cases of type 2 diabetes mellitus without comorbidities and the age of patients was between 30 and 70 attending Azadi Teaching Hospital in Duhok.
2.1.2. Exclusion criteria
Patients with renal failure, patients who suffered from acute myocardial infarction in last six months, patients on diuretics, history of alcohol abuse, magnesium supplements/magnesium‐containing antacids, malabsorption and patients with chronic diarrhoea.
2.2. Blood sampling
After an overnight fasting, 5 mL of venous blood was collected by standard procedure without tourniquet from each patient under complete aseptic conditions; 2.5 mL was placed in lithium heparin test tube. Serum was obtained by low‐speed centrifugation, the separation was done without undue delay, and after separation, the serum samples were stored at 2‐8°C and then used directly for magnesium analysis. Magnesium has been measured by Cobas 6000 (Roche, Mannheim, Germany) using colorimetric end‐point method. The other 2.5 mL was placed in EDTA test tube and used for HbA1c analysis. HbA1c was measured by enzyme‐linked immunosorbent assay (ELISA) test. The Statistical Package for Social Sciences (SPSS) was used for data analysis, and data were presented as mean ± standard deviation. Comparisons in variables were analysed using independent t test and Pearson correlation. P‐values were regarded significant when ≤0.05.
3. RESULTS
Of the total 100 patients recruited in our study, more than half of them were females with the male: female ratio of 0.54:1.00 and most of them had diabetes for 8.0 years (75%), while 35% of study population has diabetes of 3‐5 years. The mean age of the patients was 53.97 ± 10.65 years and the majority of them were on oral hypoglycaemic agents (84.9%), followed by the combination of oral hypoglycaemic agents and insulin (10.5%), and a small percentage were on insulin alone (4.7%). The mean of serum magnesium level and HbA1c was 1.88 ± 0.25 mg/dL and 8.38% ± 1.53%, respectively. The majority of the patients had a normal level of magnesium (95.0%); however, most of them had uncontrolled blood glucose (82.0%), as shown in Table 1. The study showed that the serum magnesium level and HbA1c are not significantly correlated with each other (P = 0.462) as shown in Figure 1.
Table 1.
General characteristics of study patients
| Patients’ characteristic (n = 96) | Frequency distribution | |
|---|---|---|
| Mean | Sta. deviation | |
| Age (y) | 53.97 | 10.65 |
| Serum magnesium level (mg/dL) | 1.88 | 0.25 |
| HbA1c (%) | 8.38 | 1.53 |
| Disease duration (y)[Link] | 8.0 | 7.25 |
| Frequency | Percentage | |
| Gender | ||
| Male | 35 | 35.0 |
| Female | 65 | 65.0 |
| Treatment type | ||
| Insulin | 4 | 4.7 |
| Oral hypoglycaemic agents (OHA) | 73 | 84.9 |
| Combined (insulin plus OHA) | 9 | 10.5 |
| History of myocardial infarction | 1 | 1.0 |
| HbA1c categories | ||
| Controlled (HbA1c <7) | 18 | 18.0 |
| Uncontrolled (HbA1c ≥7) | 82 | 82.0 |
| Serum magnesium ranges | ||
| Normal (1.5‐2.5 mg/dL) | 95 | 95.0 |
| Low Mg Level | 5 | 5.0 |
Median and interquartile range were calculated for disease duration.
Figure 1.
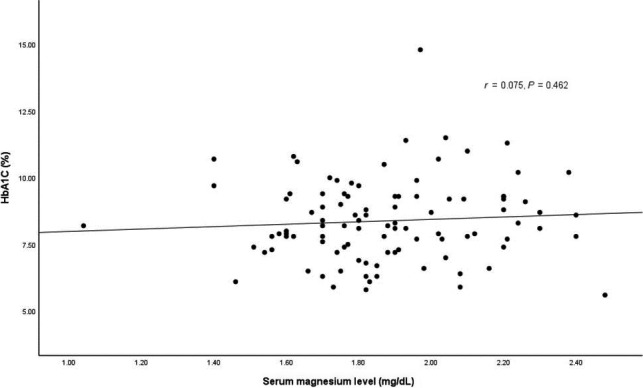
Correlation of serum magnesium level with HbA1c in type 2 diabetes patients (the correlation was not significant, P = 0.462)
The study did not show a significant difference in serum magnesium level between the patients with optimal and uncontrolled glucose level (P = 0.866). The serum magnesium level of both groups was in the normal range, as shown in Table 2.
Table 2.
Difference of serum magnesium level in patients with optimal and uncontrolled glucose level
| HbA1c | Serum magnesium level | P‐value (two‐sided) | |
|---|---|---|---|
| Mean | Sta. deviation | ||
| Optimal HbA1c | 1.88 | 0.23 | 0.866[Link] |
| Uncontrolled HbA1c | 1.87 | 0.26 | |
Independent t test was performed for statistical analysis.
4. DISCUSSION
Many studies have been done to estimate the serum magnesium level in T2DM patients and its correlation with HbA1c, but in Duhok, very few data are available regarding the serum magnesium level in diabetic patients, and to the best of our knowledge, this study is the first to evaluate the correlation of magnesium level with HbA1c in type 2 diabetes mellitus in Duhok. Sex distribution in Table 1 represents that the ratio of females is greater than males which are agreed with many studies reported in different countries.15, 16
The magnesium is an essential cofactor of more than 300 enzymes including those important in glycolysis, neuromuscular transmission, synthesis of carbohydrates, proteins, lipid and nucleic acids, and it has a role in insulin's secretion, its binding and its activity.11, 13, 18 The serum magnesium level in the present study was normal in 95% of cases, and our results were comparable with other studies, such as the results of Masood et al19 and Walter et al20 whose reported the normal Mg level in both T2DM patients and healthy controls. But Wälti et al21 showed that serum Mg concentrations of 37.6% of the diabetics were below the reference range and the findings of many studies which were reported low magnesium serum levels in T2DM.22
The HbA1c levels were uncontrolled in about 82% of patients enrolled in this study, and our results were in agreement with many studies which reported high HbA1c levels in T2DM.23, 24
Our results showed no correlation between serum Mg level and HbA1c level in contrast to many studies reported that there is an inverse correlation between serum Mg level and HbA1c,25 some studies showed normal Mg levels in T2DM but lack data correlation to HbA1c.
The nonsignificant correlation between serum Mg level and HbA1c of this study may be due to our exclusion of patients on diuretic and patients with renal failure or may be due to dietary intake of our population. Our results were in contrast to that reported by Siddique et al26 who founded that hypomagnesaemia is associated with higher level of HbA1c. Also, Tilal et al showed that there is a strong negative correlation between the serum level of magnesium and HbA1c level. Meanwhile, Navarrete‐Cortes (2016) revealed that the magnesium supplementation does not improve HbA1c or insulin sensitivity in diabetic subjects with normomagnesaemia.27
4.1. Limitation of study
Being cross‐sectional study and small sample size are main limitations. Larger‐scale clinical trials are needed in future to determine whether there is a correlation between serum Mg level and HbA1c level in T2DM.
5. CONCLUSION
Normal magnesium levels were observed in about 95% of patients with T2DM, and HbA1c levels were uncontrolled in 82% of patients which enrolled in this study. There is no significant correlation between serum Mg level and HbA1c level in patients with T2DM.
ETHICAL APPROVAL
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
CONFLICT OF INTEREST
Authors declare that they have no conflict of interest.
AUTHOR CONTRIBUTIONS
All authors have equally contributed in this study, and they all agreed on the final manuscript.
DATA ACCESSIBILITY
None.
ACKNOWLEDGEMENTS
We would like to thanks Dr. Rezvan for helping us in statistics.
Saeed H, Haj S, Qasim B. Estimation of magnesium level in type 2 diabetes mellitus and its correlation with HbA1c level. Endocrinol Diab Metab. 2019;2:e48 10.1002/edm2.48
Funding information
The authors funded the study.
REFERENCES
- 1. Wu Y, Ding Y, Tanaka Y, Zhang W. Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int J Med Sci. 2014;11(11):1185‐1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047‐1053. [DOI] [PubMed] [Google Scholar]
- 3. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4‐14. [DOI] [PubMed] [Google Scholar]
- 4. Forouhi NG, Luan J, Cooper A, Boucher BJ, Wareham NJ. Baseline serum 25‐hydroxy vitamin d is predictive of future glycemic status and insulin resistance: the Medical Research Council Ely Prospective Study 1990–2000. Diabetes. 2008;57(10):2619‐2625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Yang W, Lu J, Weng J, et al. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362(12):1090‐1101. [DOI] [PubMed] [Google Scholar]
- 6. Mangou A, Grammatikopoulou MG, Mirkopoulou D, Sailer N, Kotzamanidis C, Tsigga M. Associations between diet quality, health status and diabetic complications in patients with type 2 diabetes and comorbid obesity. Endocrinol Nutr. 2012;59(2):109‐116. [DOI] [PubMed] [Google Scholar]
- 7. Saudek CD, Derr RL, Kalyani RR. Assessing glycemia in diabetes using self‐monitoring blood glucose and hemoglobin A1c. JAMA. 2006;295(14):1688‐1697. [DOI] [PubMed] [Google Scholar]
- 8. Pfab T, Slowinski T, Godes M, Halle H, Priem F, Hocher B. Low birth weight, a risk factor for cardiovascular diseases in later life, is already associated with elevated fetal glycosylated hemoglobin at birth. Circulation. 2006;114(16):1687‐1692. [DOI] [PubMed] [Google Scholar]
- 9. Agrawal P, Arora S, Singh B, Manamalli A, Dolia PB. Association of macrovascular complications of type 2 diabetes mellitus with serum magnesium levels. Diabetes Metab Syndr. 2011;5(1):41‐44. [DOI] [PubMed] [Google Scholar]
- 10. Kousa A, Puustinen N, Karvonen M, Moltchanova E. The regional association of rising type 2 diabetes incidence with magnesium in drinking water among young adults. Environ Res. 2012;112:126‐128. [DOI] [PubMed] [Google Scholar]
- 11. Rodriguez‐Moran M, Simental Mendia LE, Zambrano Galvan G, Guerrero‐Romero F. The role of magnesium in type 2 diabetes: a brief based‐clinical review. Magnes Res. 2011;24(4):156‐162. [DOI] [PubMed] [Google Scholar]
- 12. Shaikh S, Karira KA. Magnesium deficiency in heart failure patients with diabetes mellitus. J Pak Med Assoc. 2011;61(9):901‐903. [PubMed] [Google Scholar]
- 13. Kim DJ, Xun P, Liu K, et al. Magnesium intake in relation to systemic inflammation, insulin resistance, and the incidence of diabetes. Diabetes Care. 2010;33(12):2604‐2610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Xu B, Sun J, Deng X, et al. Low serum magnesium level is associated with microalbuminuria in chinese diabetic patients. Int J Endocrinol. 2013;2013:580685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Ramadass S, Basu S, Srinivasan AR. SERUM magnesium levels as an indicator of status of Diabetes Mellitus type 2. Diabetes Metab Syndr. 2015;9(1):42‐45. [DOI] [PubMed] [Google Scholar]
- 16. Jayaraman S, Rajendran K, Suthakaran PK, et al. Study on serum magnesium levels and glycemic status in newly detected type 2 diabetes patients. Int J Adv Med. 2017;3(1):11‐14. [Google Scholar]
- 17. Barbagallo M, Dominguez LJ. Magnesium and type 2 diabetes. World J Diabetes. 2015;6(10):1152‐1157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Tosiello L. Hypomagnesemia and diabetes mellitus. A review of clinical implications. Arch Intern Med. 1996;156(11):1143‐1148. [PubMed] [Google Scholar]
- 19. Masood N, Baloch GH, Ghori RA, Memon IA, Memon MA, Memon MS. Serum zinc and magnesium in type‐2 diabetic patients. J Coll Physicians Surg Pak. 2009;19(8):483‐486. [PubMed] [Google Scholar]
- 20. Walter RM Jr, Uriu‐Hare JY, Olin KL, et al. Copper, zinc, manganese, and magnesium status and complications of diabetes mellitus. Diabetes Care. 1991;14(11):1050‐1056. [DOI] [PubMed] [Google Scholar]
- 21. Walti MK, Zimmermann MB, Spinas GA, Hurrell RF. Low plasma magnesium in type 2 diabetes. Swiss Med Wkly. 2003;133(19–20):289‐292. [DOI] [PubMed] [Google Scholar]
- 22. Seedahmed T‐H, Ahmed SM. Correlation between the plasma magnesium levels and glycated haemoglobin in Sudanese patients with type 2 diabetes mellitus in Khartoum State. Adv Diabetes Metab. 2013;1(1):1‐5. [Google Scholar]
- 23. Andrade CS, Ribeiro GS, Santos C, Neves R, Moreira ED Jr. Factors associated with high levels of glycated haemoglobin in patients with type 1 diabetes: a multicentre study in Brazil. BMJ Open. 2017;7(12):e018094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Al‐Timimi DJ, Ali AF. Serum 25(OH) D in diabetes mellitus type 2: relation to glycaemic control. J Clin Diagn Res. 2013;7(12):2686‐2688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Rao YS, V DR. Serum magnesium levels in type 2 diabetes. Int J Res Med Sci. 2016;4:991‐994. [Google Scholar]
- 26. Siddiqui MU, Ali I, Zakariya M, Asghar SP, Ahmed MR, Ibrahim GH. Frequency of hypomagnesemia in patients with uncontrolled type ii diabetes mellitus. Pak Armed Forces Med J. 2016;66(6). [Google Scholar]
- 27. Navarrete‐Cortes A, Ble‐Castillo JL, Guerrero‐Romero F, et al. No effect of magnesium supplementation on metabolic control and insulin sensitivity in type 2 diabetic patients with normomagnesemia. Magnes Res. 2014;27(2):48‐56. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
None.