

Mantle cell lymphoma (MCL), an aggressive B-cell malignancy accounting for 6% of non-Hodgkin lymphomas, remains incurable with standard therapy. Despite the approval of bortezomib,1 temsirolimus,2 lenalidomide,3 ibrutinib4 and acalabrutinib,5 patients with relapsed, refractory MCL have a survival of 2 years.
Although ibrutinib monotherapy provides significant efficacy [overall response rate (ORR), 68%; complete response rate, 21%; partial response rate, 47%] and is well tolerated in relapsed, refractory MCL, patients ultimately relapse (median progression-free survival, 13.9 months) following treatment with a Bruton tyrosine kinase (BTK) inhibitor. There are minimal outcome data for patients who progress after treatment with a BTK inhibitor and the optimal therapeutic approach has not been established. Recent retrospective analyses have reviewed several agents (including traditional chemotherapy, lenalidomide, bortezomib, and Pi3K inhibitors) in this setting. The collated data6 reveal an ORR of 20-48% and short progression-free survival and overall survival.7,8
Cheah and colleagues analyzed the effects of immunochemotherapy given after ibrutinib treatment in 31 patients. The ORR was 32% (complete response rate, 19%). The median overall survival was 8.4 months and the median duration of response was 6 months.7 Martin and colleagues also assessed the effects of post-ibrutinib therapy. In their study of 73 patients, the ORR was 26% (complete response rate, 7%) resulting in a median progression-free survival of 1.9 months and a median overall survival of 5.8 months.9 MCL-004 assessed a lenalidomide-based approach after ibrutinib (progressive disease, 88%; toxicity, 9%). The ORR to the initial ibrutinib therapy was 45%. Thirteen patients subsequently received lenalidomide, 11 lenalidomide-rituximab and 34 lenalidomide plus other therapy. The ORR was 29% and the median duration of response was 20 weeks.
Outside of MCL-004, no specific regimen has assessed more than 15 BTK inhibitor-resistant patients. Existing therapies do not overcome unfavorable tumor biology in this setting and novel combinations with differing targeted mechanisms are required.
BCL2 is overexpressed in MCL because of BCL2 loci amplification,10 defective protein degradation via lack of E3 ubiquitin ligase FBXO10, and transcriptional upregulation via BTK-mediated canonical nuclear factor-κB activation.11
Venetoclax is a potent, selective, oral BCL2 inhibitor. A recent phase 1 trial of venetoclax monotherapy in non-Hodgkin lymphoma included 28 patients with relapsed, refractory MCL.12 Within the whole cohort, toxicity was minimal and the ORR was 75% in MCL (21% complete responses). The median progression-free survival was 14 months, with 800 mg o.d. being a safe dose sufficient to achieve durable remissions. While these results are impressive, no patients had received prior treatment with a BTK inhibitor. To our knowledge, there are no data on the efficacy of venetoclax monotherapy outside of this initial publication and, in particular, no data published on the use of this BCL2 inhibitor after treatment with a BTK inhibitor. We retrospectively collected data on 20 relapsed, refractory MCL patients treated with off-label, free-of-charge venetoclax monotherapy (03/2016-05/2018) via a UK-wide compassionate use program supported by Abbvie. Data were collected from hospital records by the treating physician and included response to prior lines of therapy including BTK inhibitors, as well as duration on and reasons for stopping BTK inhibition. Pre-venetoclax data collected included Ann Arbor stage, simplified Mantle Cell Lymphoma International Prognostic Index (s-MIPI) score, histological subtype and Ki67% where available. Response was assessed by computed tomography alone or with positron emission tomography (Cheson 2014 criteria). One patient with heavy marrow infiltration at baseline was re-assessed with repeat marrow evaluation. Two patients with marked lymphocytosis and splenomegaly were included in the ORR analysis as response was clearly assessable. Three patients were evaluated clinically and therefore excluded from the ORR analysis but included in the survival analysis. Induction immunochemotherapy included high-dose cytarabine, high-dose cytarabine/maxi-CHOP-R (cyclophosphamide, doxorubicin, vincristine, prednisolone, rituximab) and autologous stem-cell transplantation consolidation.13 This pathway was considered a single treatment line. Rituximab maintenance following immunochemotherapy with or without autologous stem cell transplantation was also included in first treatment. Following consent within a compassionate use program, patients received venetoclax monotherapy in a weekly ramp-up phase starting at 20-100 mg o.d. to a maximum intended dose of 200-1200 mg o.d. until progressive disease, toxicity, death, or the physician’s or patient’s choice to stop this therapy. Detailed dosing information was available for 19/20 patients (Online Supplementary Table S1). The final intended dose was 800 mg o.d. for 7/19 (37%) patients and 1200 mg o.d. for 9/19 (47%) patients. The final intended dose was reached in 14/19 (74%) patients. Intended dose was not obtained because of neutropenia (n=1), sepsis (n=1), or progressive disease (n=3). Five patients who reached the final intended dose required a subsequent dose reduction (Online Supplementary Table S1).
Adverse event data, the incidence of tumor lysis syndrome, and anti-urate therapy were recorded. Adverse events were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. Follow-up was censored at the most recent hospital visit or death. Non-responsive MCL was defined as stable or progressive disease. Data were censored in May 2018. Progression-free survival, overall survival and duration of response were calculated in the standard fashion. Statistical analyses were performed in XLSTAT.
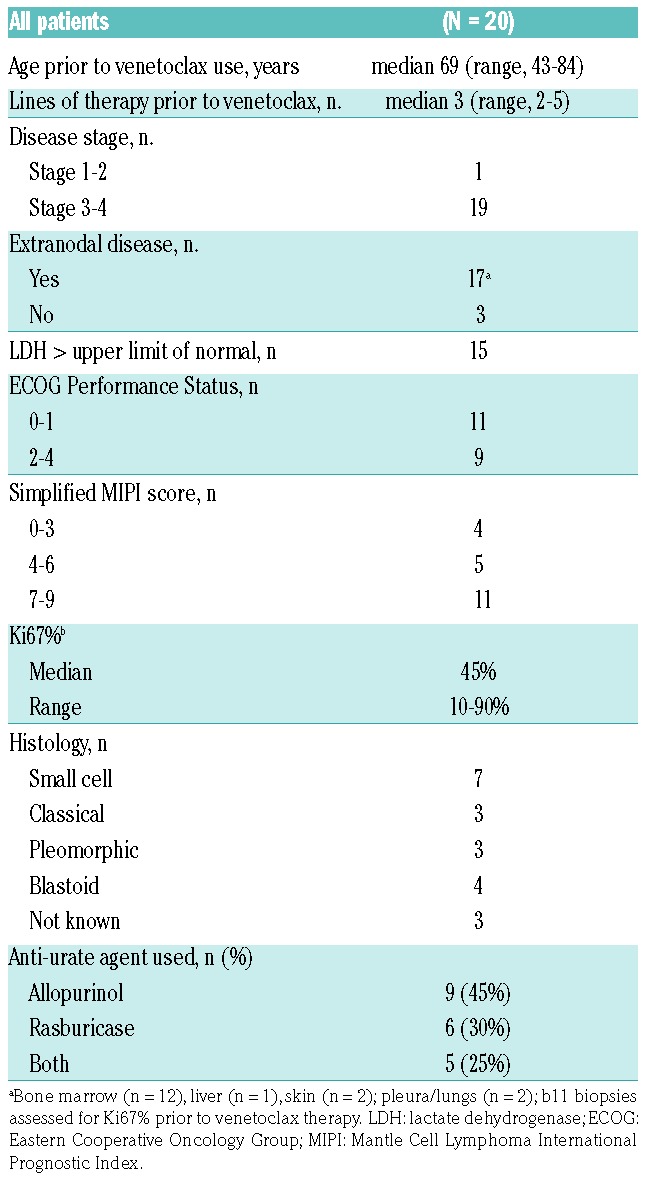
The median age of the patients was 69 years (range, 43-84) and there was a typical male predominance (85%) (Table 1). Patients had received a median of three prior therapies (range, 2-5): 40% had received a high-dose cytarabine-based induction regimen, with 30% undergoing autologous stem cell transplantation in first remission. At relapse (first or subsequent), all received a BTK inhibitor: ibrutinib (n=17), ibrutinib with donor lymphocyte infusion (n=1), tirabrutinib (n=2). The ORR to BTK inhibition was 55% (complete response rate, 15%), with a median progression-free survival of only 4.8 months (range, 0.7-34.9). Eighteen patients stopped treatment with the BTK inhibitor because of progressive disease and two because of toxicity (grade 4 thrombocytopenia; grade 4 subdural hemorrhage). After BTK inhibition, four relapsed with blastoid MCL (Table 2). Prior to venetoclax monotherapy, 95% had stage III/IV disease, 50% (9/18) had high risk according to the s-MIPI score and the median Ki67% was 45% (11 biopsies assessed).
Table 1.
Baseline characteristics: prior therapies.
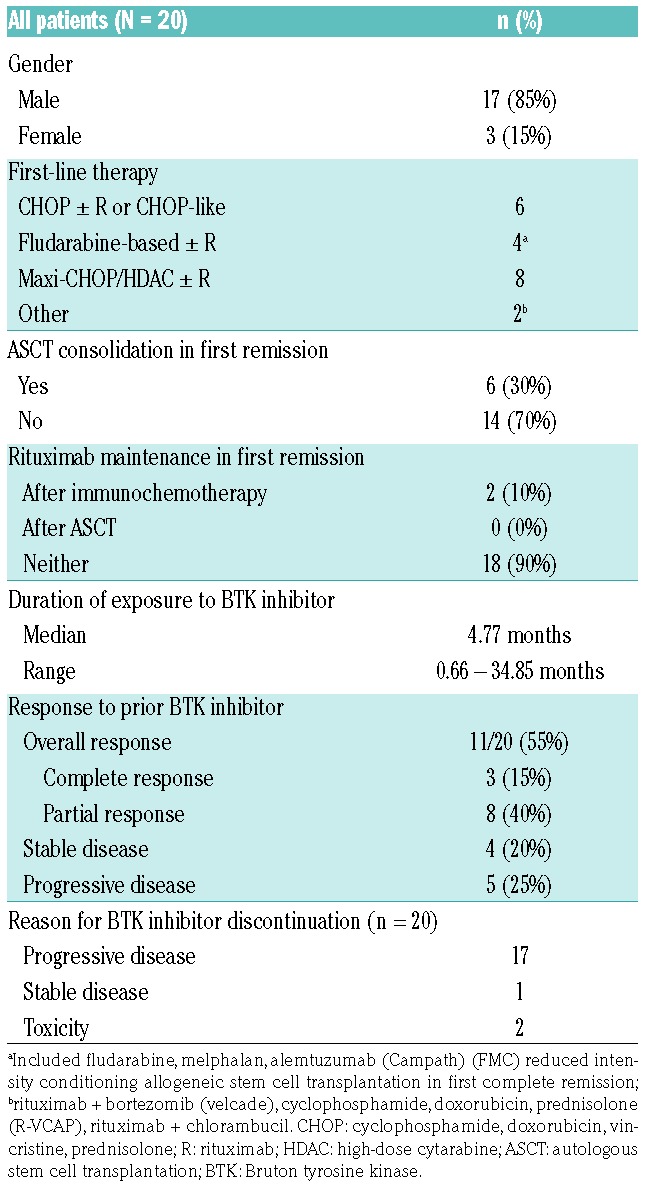
Table 2.
Baseline characteristics prior to venetoclax monotherapy.
Venetoclax monotherapy was well tolerated. There were no cases of clinical tumor lysis syndrome and four cases of transient, asymptomatic biochemical tumor lysis syndrome, managed successfully with temporary treatment cessation and re-challenge (Online Supplementary Table S2). Three patients required dose reductions to 600 mg o.d. because of adverse events: grade 2 fatigue (n=1) and grade 2 diarrhea (n=2). Seventeen adverse events were reported, including pneumonia (grade 3; n=3), sepsis (grade 4; n=1), fatigue (grade 2; n=2), neutropenia (grade 2; n=2) and diarrhea (grade 2; n=3) (Online Supplementary Table S3). Patients received allopurinol (45%), rasburicase (30%) or both (25%) as prophylaxis (Table 2).
The ORR to venetoclax monotherapy was 53% (18% complete responses; 35% partial responses). The median time to response on venetoclax was 48 days (range, 14-204). The median progression-free survival was 3.2 months (95% CI: 1.2-11.3 months) and the median overall survival was 9.4 months (95% CI: 1.5 months-not reached) (Figure 1A,B). The median duration of response was 8.1 months (95% CI: 2.8-9.8) and the progression-free survival was significantly improved in venetoclax responders (median 10.7 months: 95% CI: 3.7-12.3) compared to that in non-responders (median 1.1 months; 95% CI: 0.8-2.6; P=0.002) (Figure 1C, Online Supplementary Figure 1B). Although the initial ORR to venetoclax varied according to response to prior BTK inhibition [primary resistance to a BTK inhibitor (n=8): ORR 38% versus response to a BTK inhibitor (n=9): ORR 67%; P=0.24], this did not translate into an improved progression-free survival (data not shown). Likewise, duration on ibrutinib therapy (<4 versus >4 months) was not predictive of progression-free survival following venetoclax monotherapy (P=0.13) (Figure 1D). The s-MIPI score prior to venetoclax treatment also did not predict progression-free survival (P=0.714) (Online Supplementary Figure S1B). The progression-free survival of the two patients who stopped ibrutinib therapy because of toxicity was 4.3 months (best response: stable disease) and 10.0 months (best response: partial response).
Figure 1.

Survival outcome of patients with relapsed, refractory mantle cell lymphoma on venetoclax monotherapy. (A) Progression-free survival of all patients.(B) Overall survival of all patients. (C) Duration of response. (D) Progression-free survival according to duration on ibrutinib therapy.
Patients who had received only two lines of treatment prior to venetoclax monotherapy had a paradoxically shorter progression-free survival (median 1.3 months; 95% CI: 0.8-2.6) compared to that of more heavily pretreated patients (>2 prior lines) (median 10.0 months; 95% CI: 3.7-not reached; P=0.042). Similar results were seen when comparing patients with a time from initial MCL diagnosis to start of venetoclax of >4.5 years (median, 10.0 months; 95% CI: 2.6-not reached) versus <4.5 years (median, 1.3 months; 95% CI: 0.8-4.3); P=0.027) (Online Supplementary Figure S1C,D). As such, less heavily pre-treated patients were enriched for those with a considerably shorter time from MCL diagnosis to venetoclax commencement and therefore likely represented those with more aggressive disease biology. Four patients with blastoid disease had a short time from diagnosis to venetoclax monotherapy (0.8-2.1 years), possessed high Ki67% (75-90%), had an ORR of 25%, and all progressed by 2 months. Eight patients received treatment after venetoclax monotherapy (Online Supplementary Table S4). One patient underwent allogeneic stem cell transplantation following response to venetoclax monotherapy but subsequently relapsed.
To date, 12 patients have died; nine from progressive disease, two from the combination of progressive disease and infection, and one patient from secondary acute myeloid leukemia while in remission after treatment with rituximab, bendamustine and cytarabine (R-BAC) (Online Supplementary Table S1).
We present initial real-world data outlining the efficacy of venetoclax monotherapy in a cohort of patients with aggressive MCL in whom BTK inhibition had failed. The ORR and median progression-free survival after BTK inhibition were markedly inferior in this cohort than in the pivotal trials with ibrutinib4 and acalabrutinib5, suggesting that our cohort possessed particularly adverse clinical and biological features. We provide the first evidence of the tolerability and efficacy of venetoclax monotherapy in MCL in the post-BTK inhibitor setting. An ORR of 53% (complete response rate, 18%) is encouraging and compares favorably with that for other treatments in this setting; however the median progression-free survival was short. The response to venetoclax monotherapy in patients resistant to BTK inhibition provides an extension of the proof-of-principle initially obtained in chronic lymphocytic leukemia that BH3 mimetics have activity in BTKi-resistant lymphoproliferative disease.14 Subgroup analysis was limited by small numbers but prior response to BTK inhibition or duration of response did not predict progression-free survival.
Weaknesses of our study include the intrinsic biases associated with retrospective data reporting, the lack of centralized pathology review, formalized radiological reporting, and prospective adverse event reporting.
Venetoclax monotherapy produces an encouraging initial ORR in relapsed, refractory MCL after BTK inhibition with minimal toxicity, thereby providing further evidence for its place in investigations of rational, novel combinations in this setting. Specific clinical benefit was gained in responding patients but the global progression-free survival was disappointing. Synergy between BTK inhibitors and BCL2 inhibitors has been demonstrated in BTK-sensitive and resistant MCL cells in vitro and in vivo11 and early clinical data on the combination of ibrutinib-venetoclax (n=24) suggest safety, high complete metabolic responses (71%) and high minimal residual disease-negativity (67% marrow; 8-color flow cytometry).15
Supplementary Material
Footnotes
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Goy A, Bernstein SH, Kahl BS, et al. Bortezomib in patients with relapsed or refractory mantle cell lymphoma: updated time-to-event analyses of the multicenter phase 2 PINNACLE study. Ann Oncol. 2009;20(3):520–525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hess G, Herbrecht R, Romaguera J, et al. Phase III study to evaluate temsirolimus compared with investigator’s choice therapy for the treatment of relapsed or refractory mantle cell lymphoma. J Clin Oncol. 2009;27(23):3822–3829. [DOI] [PubMed] [Google Scholar]
- 3.Trneny M, Lamy T, Walewski J, et al. Phase II randomized, multicenter study of lenalidomide vs. best investigator’s choice in relapsed/refractory mantle cell lymphoma: results of the MCL-002 (SPRINT) study. Blood. 2014;124(21):626. [Google Scholar]
- 4.Wang ML, Rule S, Martin P, et al. Targeting BTK with Ibrutinib in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2013;369(6):507–516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wang M, Rule S, Zinzani PL, et al. Acalabrutinib in relapsed or refractory mantle cell lymphoma (ACE-LY-004): a single-arm, multicentre, phase 2 trial. Lancet. 2018;391(10121):659–667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hershkovitz-Rokah O, Pulver D, Lenz G, Shpilberg O. Ibrutinib resistance in mantle cell lymphoma: clinical, molecular and treatment aspects. Br J Haematol. 2018;181(3):306–319. [DOI] [PubMed] [Google Scholar]
- 7.Cheah CY, Chihara D, Romaguera JE, et al. Patients with mantle cell lymphoma failing ibrutinib are unlikely to respond to salvage chemotherapy and have poor outcomes. Ann Oncol. 2015;26(6):1175–1179. [DOI] [PubMed] [Google Scholar]
- 8.Epperla N, Hamadani M, Cashen AF, et al. Predictive factors and outcomes for ibrutinib therapy in relapsed/refractory mantle cell lymphoma—a “real world” study. Hematol Oncol. 2017;35(4):528–535. [DOI] [PubMed] [Google Scholar]
- 9.Martin P, Maddocks K, Leonard JP, et al. Postibrutinib outcomes in patients with mantle cell lymphoma. Blood. 2016;127(12):1559–1563. [DOI] [PubMed] [Google Scholar]
- 10.Bentz M, Plesch A, Bullinger L, et al. t(11;14)-positive mantle cell lymphomas exhibit complex karyotypes and share similarities with B-cell chronic lymphocytic leukemia. Genes Chromosom Cancer. 2000;27(3):285–294. [PubMed] [Google Scholar]
- 11.Li Y, Bouchlaka MN, Wolff J, et al. FBXO10 deficiency and BTK activation upregulate BCL2 expression in mantle cell lymphoma. Oncogene. 2016;35(48):6223–6234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Davids MS, Roberts AW, Seymour JF, et al. Phase I first-in-human study of venetoclax in patients with relapsed or refractory non-Hodgkin lymphoma. J Clin Oncol. 2017;35(8):826–833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Geisler CH, Kolstad A, Laurell A, et al. Long-term progression-free survival of mantle cell lymphoma after intensive front-line immunochemotherapy with in vivo-purged stem cell rescue: a non-randomized phase 2 multicenter study by the Nordic Lymphoma Group. Blood. 2008;112(7):2687–2693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jones JA, Mato AR, Wierda WG, et al. Venetoclax for chronic lymphocytic leukaemia progressing after ibrutinib: an interim analysis of a multicentre, open-label, phase 2 trial. Lancet Oncol. 2018;19(1):65–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tam CS, Anderson MA, Pott C, et al. Ibrutinib plus venetoclax for the treatment of mantle-cell lymphoma. N Engl J Med. 2018;378(13):1211–1223. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.