

Madam,
A 55-year-old man presented with shortness of breath on mild exertion for 1 month. Coronary angiography revealed three vessels coronary artery disease. Transthoracic echocardiography demonstrated left ventricular ejection fraction of 30% with severe mitral regurgitation due to annular dilation, and no other valvular pathology [Figures 1 and 2]. The patient was scheduled for coronary artery bypass grafting surgery with mitral annuloplasty. Under moderate hypothermic cardiopulmonary bypass, three saphenous vein grafts were anastomized to the left anterior descending, obtuse marginal, and posterior descending artery. Left atriotomy was performed, and asymmetric mitral annular dilatation was treated by mitral ring annuloplasty using 28-mm CE Classic Annuloplasty Ring. After the surgery, weaning from cardiopulmonary bypass was started. Transesophageal echocardiography (TEE) was performed [Figures 3 and 4] and a diagnosis of new onset aortic regurgitation was made. TEE showed trivial residual mitral regurgitation; however, new aortic regurgitation jet was observed causing left ventricular distension [Figure 3]. Transesophageal aortic valve (AV) short axis view revealed tear in the noncoronary cusp of AV [Figure 4]. Cardiopulmonary bypass was reinitiated. Aortotomy was done and AV was inspected. Noncoronary cusp was frail and had approximately 1 cm horizontal tear. No suture or suture penetration or needle holes were seen on the aortic side of the valve. After the failed attempts of repair, AV was excised and replaced with 21-mm perimount-plus pericardial AV Bioprosthesis. Patient could be easily weaned from cardiopulmonary bypass with minimal inotropic support. Postoperative course of the patient remained stable.
Figure 1.

Preoperative transesophageal echocardiographic 2 chamber view showing mitral regurgitation
Figure 2.
Preoperative transesophageal echocardiographic aortic valve short axis view showing normal appearing aortic valve leaflets
Figure 3.

Transesophageal echocardiographic aortic valve long axis view showing aortic regurgitation jet from noncoronary cusp of aortic valve
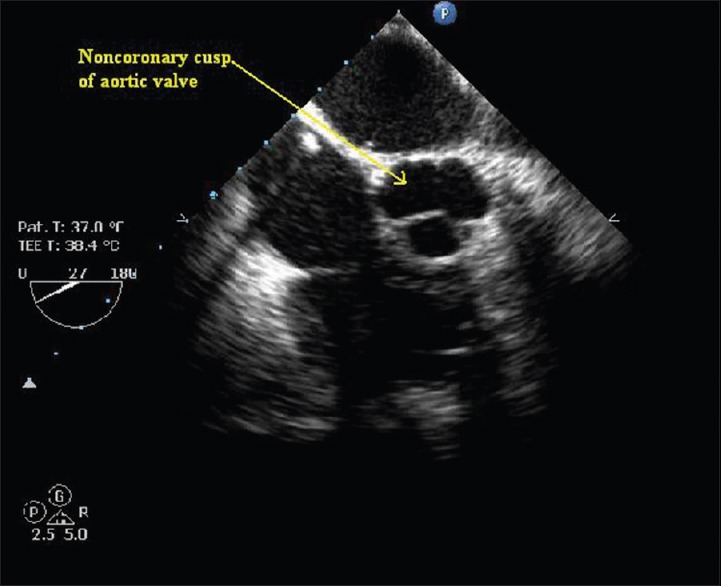
Figure 4.

Transesophageal echocardiographic aortic valve short axis view showing tear in noncoronary cusp of aortic valve
Mitral ring annuloplasty corrects and further prevents annular dilatation, thereby reducing mitral regurgitation.[1] Left ventricular outflow tract obstruction (3%), incomplete correction (3%), or suture dehiscence (2%) are known postoperative complications requiring reinstitution of cardiopulmonary bypass.[2]
Severe aortic regurgitation after mitral annuloplasty ring is an infrequent complication reported in sporadic case reports.[3] Any of the three AV leaflets are prone to iatrogenic injury depending on the surgery type, for example, noncoronary cusp during mitral and atrial septal defect operation, left coronary leaflet during mitral valve surgery and right coronary cusp during ventricular septal defect surgery, and pulmonary valve operation.[4,5] Suture needle perforation or suture entrapment of an AV cusp or aortic annulus distortion caused by sutures retaining the mitral valve can cause aortic regurgitation during mitral valve surgery.[3,6] However, in this case, we assume that tension by mitral annuloplasty ring might have pulled the adjacent tissue causing tear in the fragile noncoronary cusp. Although noncoronary and left coronary cusps are commonly affected in such cases, right coronary cusp tear after a mitral valve replacement has also been reported.[7] Al Yamani et al. suggested maneuvres such as pushing the aortic root from outside toward the mitral valve to improve exposure can increases the risk of AV injury.[7] Thorough intraoperative transesophageal echocardiography examination can detect iatrogenic AV injury and it can be addressed in the same surgical sitting.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Carpentier A, Chauvaud S, Fabiani JN, Deloche A, Relland J, Lessana A, et al. Reconstructive surgery of mitral valve incompetence: Ten-year appraisal. J Thorac Cardiovasc Surg. 1980;79:338–48. [PubMed] [Google Scholar]
- 2.Marwick TH, Stewart WJ, Currie PJ, Cosgrove DM. Mechanisms of failure of mitral valve repair: An echocardiographic study. Am Heart J. 1991;122(1 Pt 1):149–56. doi: 10.1016/0002-8703(91)90772-a. [DOI] [PubMed] [Google Scholar]
- 3.Ducharme A, Courval JF, Dore A, Leclerc Y, Tardif JC. Severe aortic regurgitation immediately after mitral valve annuloplasty. Ann Thorac Surg. 1999;67:1487–9. doi: 10.1016/s0003-4975(99)00230-1. [DOI] [PubMed] [Google Scholar]
- 4.Mehta AR, Hunsaker R. Iatrogenic aortic incompetence after mitral valve replacement. J Cardiothorac Vasc Anesth. 2007;21:276–8. doi: 10.1053/j.jvca.2006.05.007. [DOI] [PubMed] [Google Scholar]
- 5.Woo JJ, Koh YY, Chang KS, Hong SP. A case of iatrogenic aortic valve leaflet perforation after closure of a ventricular septal defect. Int J Cardiovasc Imaging. 2010;26(Suppl 1):169–72. doi: 10.1007/s10554-010-9587-2. [DOI] [PubMed] [Google Scholar]
- 6.Hill AC, Bansal RC, Razzouk AJ, Liu M, Bailey LL, Gundry SR. Echocardiographic recognition of iatrogenic aortic valve leaflet perforation. Ann Thorac Surg. 1997;64:684–9. doi: 10.1016/s0003-4975(97)00524-9. [DOI] [PubMed] [Google Scholar]
- 7.Al Yamani MI, Frapier JM, Battistella PD, Albat B. Right coronary cusp perforation after mitral valve replacement. Interact Cardiovasc Thorac Surg. 2013;16:387–8. doi: 10.1093/icvts/ivs522. [DOI] [PMC free article] [PubMed] [Google Scholar]