

Abstract
Purpose:
This study aims to compare the various distraction methods used during office cystoscopy to decrease pain and dissatisfaction among patients.
Materials and Methods:
Two hundred patients undergoing rigid cystoscopy between January 2017 and July 2017 were randomized into four groups of 50 patients: (1) Group I: Patients who listened to music during the cystoscopy, (2) Group II: Patients allowed real-time visualization of the cystoscopy, (3) Group III: Patients who listened to music and had real-time visualization of the procedure, (4) Group IV: Control group undergoing cystoscopy without any distraction used. A visual analog scale (VAS) (1–10) was used for a self-assessment of pain, satisfaction, and willingness for repeat cystoscopy.
Results:
Demographic characteristics, mean age, procedure duration, and procedure indications were statistically similar between the four groups. The mean VAS pain score were significantly lower in the three study Groups (I, II, and III) where distraction methods were used during cystoscopies as compared to the control Group IV (P < 0.001) and the satisfaction VAS scores and VAS scores for willingness to undergo a repeat procedure were significantly higher in the study groups (P < 0.001). Statistically significant decreased postprocedural pulse rate and blood pressure in comparison with to their preprocedural values were observed when distraction methods were used (P < 0.01). Patients undergoing cystoscopies listening to music and real-time visualization (Group III) had better VAS scores than the others (P < 0.01).
Conclusions:
Distraction methods reduce pain and increase satisfaction among patients. Best results are with combined listening to music and direct real-time visualization.
Keywords: Direct visualization, distraction methods, music, urethro-cystoscopies, visual analog scale
INTRODUCTION
Pain relief is something patients expect from their doctors. Unfortunately, it is also one of the most complicated tasks and often the best medical practice requires procedures that are not only uncomfortable but inflict pain.
Urethro-cystoscopy is a common outpatient urologic clinical examination; however, it is somewhat painful for patients and often causes feelings of fear and anxiety before the procedure.
In urology, urethra cystoscopies form an integral part of the initial evaluation of the patient's symptoms. In fact, the significance of urethra-cystoscopies in everyday urological practice has increased especially in the diagnosis and treatment of various urological conditions such as bladder carcinoma, tumor infiltration and hematuria.
Although it is an invasive procedure, neither does it justify the procedure to be done under full anesthesia nor at the same time the discomfort due to pain be ignored.
Various anesthetic techniques have been used for rigid cystoscopy, such as urethral lubrication, an intra-urethral lidocaine injection, or premedication with a short-acting intramuscular narcotic.[1]
In the past, use of inhalational agents, such as nitric oxide[2] and parenteral agents such as midazolam have been tried. These methods need proper monitoring. However, none of these approaches are sufficient to relieve pain, fear, and anxiety in patients during the procedure. Nonpharmacologic alternative treatment modalities also can be considered.[3] Over the past few years, evidence occurred that patients might benefit from watching their urethra-cystoscopy real-time on a video screen.[4,5,6,7] Music is an established complementary treatment for several diseases that allows for the reduction of pharmacological treatments to sedative doses.[8]
To the best of our knowledge, no study has compared music versus real-time direct visualization versus combined audiovisual effects in ameliorating the pain and increasing satisfaction levels for ambulatory cystoscopic procedure.
Aims and objectives
Our study is a randomized comparative observational study of the effect of music versus real-time visualization versus combined music plus direct visualization in amelioration of pain in comparison with those who undergo routine conventional cystoscopies. The study was undertaken with the following aims and objectives.
To analyze the pain and satisfaction scores of patients during urethro-cystoscopies
To study the pain and the satisfaction scores with listening to music and real-time visualization of the procedure during cystoscopies
To study the pain and the satisfaction scores with combined effects of listening to music and real-time visualizations of the procedure during cystoscopies
To compare the above findings with those who undergo routine, conventional cystoscopies.
MATERIALS AND METHODS
This is a four-arm parallel randomized control non-blinded study comparing the effect of various distraction methods during urethro cystoscopies. A total of 200 patients, with prior informed consent, were recruited into the study between April 2017 and September 2017, after proper scrutinizing the inclusion criteria.
The patients who came for ambulatory cystoscopic examination (CPE) were randomized into four groups.
Group I: Underwent CPE while listening to the music of his or her choice with the help of a headset
Group II: Underwent CPE with direct visualizations of the procedure in the monitor that was turned towards the patient
Group III: Underwent CPE with direct visualization along with listening to the music during the procedure
Group IV: Underwent routine conventional CPE without any distraction techniques being used.
The patients with lidocaine allergy, inability to comply with the experimental methods, urinary tract infection, anatomical problems with the urethra, any analgesic use during the 24 h before urethro-cystoscopy.
After taking informed consent from the patients, the CPE was performed in dorsal lithotomy position under local per-urethral application of 2% xylocaine jelly (for 10 min prior to cystoscopy) with 17.5F cystoscope sheath. Baseline vital parameters (pulse rate [PR] and systolic blood pressure [SBP]) were documented. During the procedure, the patients were monitored for their vital parameters with the help of pulse-oxymetry noninvasive blood pressure monitoring. Subsequently, all these patients will be given a visual analog scale (VAS) score sheet rate their pain sensation during the procedure on a scale of 1–10 with 1 being extremely painful and 10 being absolutely painless. The same surgeon will be performing all the cystoscopies. Similarly, their satisfaction level with the procedure will be recorded on an increasing VAS scale of 1–10 with 1 being highly unsatisfied and 10 being extremely satisfied. In addition, the willingness to undergo a repeat CPE was also recorded with the VAS scores.
Continuous data were expressed as a mean (±standard deviation). Comparative analysis between two groups was performed using the Chi-square test for categorical data and independent t-test or Mann–Whitney U-test for continuous data as applicable. All statistical tests were two-tailed, and P < 0.05 was considered as significant. We used SPSS software for analysis (version 20, IBM Corporation, NY, and USA).
RESULT ANALYSIS
General data
A total of 200 patients were evaluated (126 males and 74 females) with CPE with a mean age of 53.08 ± 9.91 years (range 25–74). The age (P = 0.05) and sex (P = 0.625) distribution among all the four groups were comparable without any significant differences [Table 1]. Fifty patients were recruited into each arm of the study. All the patients underwent CPE for the first time. No significant difference in the SBP and PR among the patients in all the four groups (P = 0.317 and P = 0.586, respectively) [Table 1].
Table 1.
Summary of patient characteristics and pre-procedural status
| Variable | Group I (music) | Group II (real-time visualization) | Group III (music + real-time visualization) | Group IV (control) | P |
|---|---|---|---|---|---|
| Age (years) | |||||
| Mean±SD | 53.68±8.60 | 55.92±10.00 | 50.66±11.01 | 52.08±10.04 | 0.813 |
| Range | 39.00-74.00 | 32.00-74.00 | 25.00-72.00 | 25.00-74.00 | |
| Sex | |||||
| Male (126) | 32 | 31 | 32 | 31 | 0.625 |
| Female (74) | 19 | 18 | 18 | 19 | |
| Procedure duration (min) | 5.26±1.26 | 5.58±1.34 | 5.44±1.30 | 5.70±1.24 | 0.395 |
| Indications for CPE | |||||
| Gross hematuria | 11 | 10 | 12 | 14 | |
| Microscopic hematuria | 4 | 3 | 4 | 3 | |
| LUTS | 18 | 20 | 21 | 24 | |
| Check CPE | 9 | 8 | 9 | 7 | |
| Bladder stones | 4 | 5 | 2 | 1 | |
| VVF assessment | 2 | 1 | 1 | 1 | |
| SUI | 2 | 3 | 1 | 0 | |
| 3 | |||||
| Preoperative PR (beats/min) | 76.06±6.12 | 75.76±6.23 | 75.48±4.67 | 77.04±6.67 | 0.586 |
| Preoperative SBP (mm of Hg) | 123.44±13.04 | 126.52±14.73 | 125.68±14.64 | 121.80±12.74 | 0.317 |
PR: Pulse rate, SBP: Systolic blood pressure, SD: Standard deviation, LUTS: lower urinary tract symptoms, VVF: vesico-vaginal fistula, SUI : stress urinary incontinence
Pain and satisfaction scores
The pain scores were analyzed and compared among the groups. The pain scores were significantly lower for Group I (4.08 ± 1.56), Group II (3.46 ± 1.43) and Group III (3.16 ± 1.25) when compared to the control Group IV (7.12 ± 1.85) (P < 0.001) [Figure 1]. The change in the vital parameters, as compared to the control Group IV which was highest (ΔPR = 9.40 ± 4.04 bpm; ΔSBP = 8.44 ± 4.0 mmHg), were significantly lower in the study Groups I, II, III, (P < 0.001 for both) lowest being for patient in whom music and real-time visualization of procedure were used for distraction (ΔPR = 3.6 ± 2.12 bpm; ΔSBP = 4.08 ± 2.45 mmHg).
Figure 1.
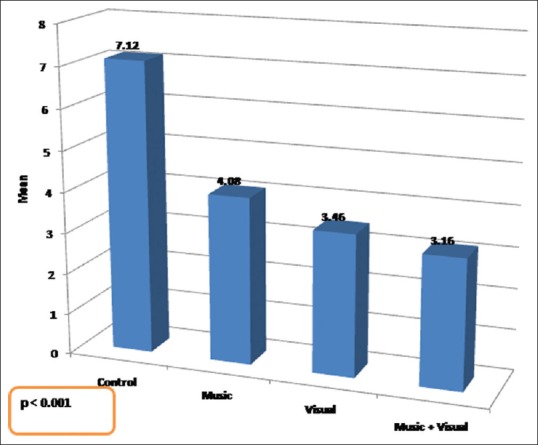
Visual analog scale scores for pain sensation in all the four arms
The satisfaction scores were also predictably higher in the study arm Groups I, II, III when compared to control arm Group IV (P < 0.001) and so was the VAS scores for a willingness for repeat CPE procedure in future (P < 0.001) [Table 2 and Figure 2].
Table 2.
Pain, willingness to undergo the procedure and satisfaction during cystoscopic examination postprocedure
| Objective assessment of distraction effect on CPE | |||||
|---|---|---|---|---|---|
| Variable | Group I (music) | Group II (real-time visualization) | Group III (music + real-time visualization) | Group IV (control) | P |
| Postoperative pulse (beats/min) | 82.14±6.33 | 79.44±6.47 | 79.88±5.27 | 86.44±5.67 | <0.001 |
| Postoperative SBP (mm of Hg) | 130.56±12.59 | 130.60±14.57 | 130.96±14.65 | 130.24±11.88 | 0.995 |
| Δ Intraoperative pulse (rate/min) | 6.08±2.91 | 4.40±2.42 | 3.68±2.02 | 9.40±4.04 | <0.0001 |
| Δ Intraoperative SBP (mmHg) | 7.12±3.98 | 5.28±2.20 | 4.08±2.45 | 8.44±4.1 | <0.0001 |
| Postoperative pain VAS | 4.08±1.56 | 3.46±1.43 | 3.16±1.25 | 7.12±1.85 | <0.0001 |
| Postoperative satisfaction VAS scores | 5.20±1.13 | 7.16±1.36 | 7.18±1.64 | 2.68±1.13 | <0.0001 |
| Willingness for a repeat CPE VAS scores | 5.18±5.18 | 7.24±1.40 | 7.50±1.19 | 3.62±1.76 | <0.0001 |
SBP: Systolic blood pressure, VAS: Visual analog scale
Figure 2.
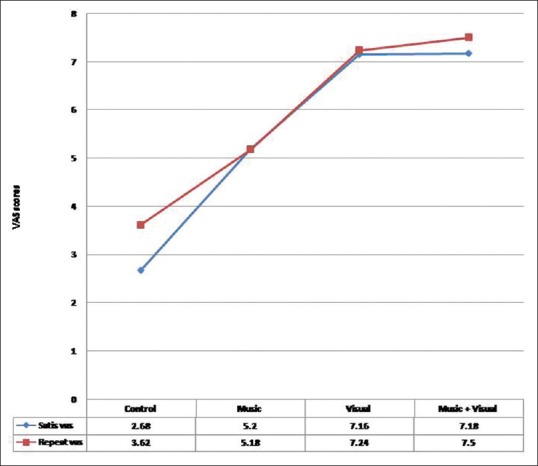
Visual analog scale scores for satisfaction and willingness for repeat CPE
Among the study Groups I, II, III, the pain scores and the satisfaction scores were best among the patient in Group III (music and real-time visualization) followed by patients in Group II (only real-time visualization) and Group I (only music as distraction method).
DISCUSSION
The patients who are referred for CPE are often inquisitive about the pain associated with the procedure and enquire regarding the measures that would be undertaken for pain relief during the procedure. The definition of pain, as proposed by the International Association for the Study of Pain, is “an unpleasant sensory and emotional experience associated with either actual or potential tissue damage, or described regarding such damage.”[9] In the established and frequently used VAS method of self-assessment of pain, patients score their own pain sensation on a scale of 0–10 or cartoons of suffering faces.[10] There is an element of discomfort and mainly in the form of pain that is associated with CPE procedure itself.[11]
Various methods have been used in the past for reducing these pain symptoms. Earlier modifications were related to the instruments itself mainly in the form of narrower sheath used during CPE or using flexible cystoscopes.[12] Using intraurethral topical anesthetic agent has been a common practice to reduce the pain during the CPE. However, Patel et al.[13] in their meta-analysis have mentioned that there was no significant difference in pain control during CPE with intra-urethral application if 2% lidocaine jelly when compared with only lubricant jelly.
The use of music to promote relaxation has a long history in medicine and music is a low-cost and harmless addition to clinical settings that evoke measurable reductions in pain and anxiety.[14,15] As an alternative treatment modality, music reduces perceptions of discomfort by activating the cingulo-frontal cortex, which functions in attention shifting[16] and pain modulation.[17] Music also has anxiolytic effects and has been applied to ameliorate stressful interventions.[18] Music significantly increased patient willingness to undergo a repeated procedure. This is particularly promising for the treatment of bladder tumors, which necessitate regular cystoscopic follow-ups.[19]
Malloy and Milling have showed the efficacy of virtual distraction in the reduction of pain sensation.[20] In this context, recently, there has been a trend in using various distraction methods for pain relief during CPE. Multiple studies are available to prove the benefit of music being used as a successful distraction method for CPE.[21,22] Yeo et al.[19] demonstrated the efficacy of distraction using listening to classical music during CPE for reduction of procedure-related pain and discomfort. Zhang et al.[7] allowed the patient to view the CPE procedure on a screen as a distraction method with promising results.
No study till date, to the best of our knowledge, have tested the efficacy of combing music with real-time visualization of the CPE procedure on a screen as a tool for distraction during CPE. The present study not only addressed this combined modality of distraction but also compared its efficacy with the control group of not using any distraction method (Group IV) and also with the single modalities of distraction (Groups I and II).
Like Clements et al.,[4] our study uses the VAS 0–10 as a tool for comparison of the pain sensation of the four arms of the study. We also used the same VAS scale to score their satisfaction for the procedure and also their willingness to undergo the same procedure in case needed in the future. In contrast to the other studies where a more narrowed selection criterion had been used, our study uses a broad selection criterion with exclusion of only patients with lignocaine allergy. Unlike Soomro et al.,[6] where more than one urologist was involved in the CPE and thus having the possibility of mixed results on the pain sensation based on the varied skills and performance of the urologists; in our study, there was only one urologist who performed all the CPE.
The present study shows that distraction method is an effective method in reducing the pain sensation during CPE. To the best of our knowledge, no randomized study is available comparing the various distraction methods. We compared the effect of music, real-time visualization and combined music plus real-time visualization with the standard cystoscopy without any use of distraction methods. Although the pain scores were better with use of single distraction method used (music and real-time visualization), yet combining them both result in better VAS scores for pain sensation. In addition, the change in the vital parameters which are surrogate markers for sympathetic response to pain was lower when combined two methods of distraction used as compared to single distraction method.
The satisfaction VAS score was also significantly higher as were their willingness for a repeat procedure if required later among patients who were subjected to distraction methods, and particularly so among those who were exposed to combined music and visual effect.
CONCLUSIONS
Distraction methods used during the CPE would definitely help in reduction of the subjective pain sensation and improve patients’ satisfaction and objectively in positively decrease in the sympathetic response to pain as demonstrated in their immediate change in vital parameters with the procedure. Although music or direct visualization alone can be effective as a distraction method, combining them both would prove to be more beneficial in ameliorating the pain and discomfort during CPE.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Song YS, Song ES, Kim KJ, Park YH, Ku JH. Midazolam anesthesia during rigid and flexible cystoscopy. Urol Res. 2007;35:139–42. doi: 10.1007/s00240-007-0091-7. [DOI] [PubMed] [Google Scholar]
- 2.Calleary JG, Masood J, Van-Mallaerts R, Barua JM. Nitrous oxide inhalation to improve patient acceptance and reduce procedure related pain of flexible cystoscopy for men younger than 55 years. J Urol. 2007;178:184–8. doi: 10.1016/j.juro.2007.03.036. [DOI] [PubMed] [Google Scholar]
- 3.McCaffery M. Nursing approaches to nonpharmacological pain control. Int J Nurs Stud. 1990;27:1–5. doi: 10.1016/0020-7489(90)90018-e. [DOI] [PubMed] [Google Scholar]
- 4.Clements S, Sells H, Wright M. Use of video in flexible cystoscopy: A prospective randomized study of effect on patient experience. Ambul Surg. 2004;11:45–6. [Google Scholar]
- 5.Patel AR, Jones JS, Angie S, Babineau D. Office based flexible cystoscopy may be less painful for men allowed to view the procedure. J Urol. 2007;177:1843–5. doi: 10.1016/j.juro.2007.01.070. [DOI] [PubMed] [Google Scholar]
- 6.Soomro KQ, Nasir AR, Ather MH. Impact of patient's self-viewing of flexible cystoscopy on pain using a visual analog scale in a randomized controlled trial. Urology. 2011;77:21–3. doi: 10.1016/j.urology.2010.08.012. [DOI] [PubMed] [Google Scholar]
- 7.Zhang ZS, Tang L, Wang XL, Xu CL, Sun YH. Seeing is believing: A randomized controlled study from china of real-time visualization of flexible cystoscopy to improve male patient comfort. J Endourol. 2011;25:1343–6. doi: 10.1089/end.2011.0084. [DOI] [PubMed] [Google Scholar]
- 8.López-Cepero Andrada JM, Amaya Vidal A, Castro Aguilar-Tablada T, García Reina I, Silva L, Ruiz Guinaldo A, et al. Anxiety during the performance of colonoscopies: Modification using music therapy. Eur J Gastroenterol Hepatol. 2004;16:1381–6. doi: 10.1097/00042737-200412000-00024. [DOI] [PubMed] [Google Scholar]
- 9.Cook KF, Dunn W, Griffith JW, Morrison MT, Tanquary J, Sabata D, et al. Pain assessment using the NIH toolbox. Neurology. 2013;80:S49–53. doi: 10.1212/WNL.0b013e3182872e80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Louly PG, Medeiros-Souza P, Santos-Neto L. N-of-1 double-blind, randomized controlled trial of tramadol to treat chronic cough. Clin Ther. 2009;31:1007–13. doi: 10.1016/j.clinthera.2009.05.015. [DOI] [PubMed] [Google Scholar]
- 11.Aaronson DS, Walsh TJ, Smith JF, Davies BJ, Hsieh MH, Konety BR, et al. Meta-analysis: Does lidocaine gel before flexible cystoscopy provide pain relief? BJU Int. 2009;104:506–9. doi: 10.1111/j.1464-410X.2009.08417.x. [DOI] [PubMed] [Google Scholar]
- 12.Tsuchida S, Sugawara H. A new flexible fibercystoscope for visualization of the bladder neck. J Urol. 1973;109:830–1. doi: 10.1016/s0022-5347(17)60554-8. [DOI] [PubMed] [Google Scholar]
- 13.Patel AR, Jones JS, Babineau D. Lidocaine 2% gel versus plain lubricating gel for pain reduction during flexible cystoscopy: A meta-analysis of prospective, randomized, controlled trials. J Urol. 2008;179:986–90. doi: 10.1016/j.juro.2007.10.065. [DOI] [PubMed] [Google Scholar]
- 14.Lee DW, Chan AC, Wong SK, Fung TM, Li AC, Chan SK, et al. Can visual distraction decrease the dose of patient-controlled sedation required during colonoscopy. A prospective randomized controlled trial? Endoscopy. 2004;36:197–201. doi: 10.1055/s-2004-814247. [DOI] [PubMed] [Google Scholar]
- 15.Harikumar R, Raj M, Paul A, Harish K, Kumar SK, Sandesh K, et al. Listening to music decreases need for sedative medication during colonoscopy: A randomized, controlled trial. Indian J Gastroenterol. 2006;25:3–5. [PubMed] [Google Scholar]
- 16.Kondo H, Morishita M, Osaka N, Osaka M, Fukuyama H, Shibasaki H, et al. Functional roles of the cingulo-frontal network in performance on working memory. Neuroimage. 2004;21:2–14. doi: 10.1016/j.neuroimage.2003.09.046. [DOI] [PubMed] [Google Scholar]
- 17.Valet M, Sprenger T, Boecker H, Willoch F, Rummeny E, Conrad B, et al. Distraction modulates connectivity of the cingulo-frontal cortex and the midbrain during pain – An fMRI analysis. Pain. 2004;109:399–408. doi: 10.1016/j.pain.2004.02.033. [DOI] [PubMed] [Google Scholar]
- 18.Lee DW, Chan KW, Poon CM, Ko CW, Chan KH, Sin KS, et al. Relaxation music decreases the dose of patient-controlled sedation during colonoscopy: A prospective randomized controlled trial. Gastrointest Endosc. 2002;55:33–6. doi: 10.1067/mge.2002.120387. [DOI] [PubMed] [Google Scholar]
- 19.Yeo JK, Cho DY, Oh MM, Park SS, Park MG. Listening to music during cystoscopy decreases anxiety, pain, and dissatisfaction in patients: A pilot randomized controlled trial. J Endourol. 2013;27:459–62. doi: 10.1089/end.2012.0222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Malloy KM, Milling LS. The effectiveness of virtual reality distraction for pain reduction: A systematic review. Clin Psychol Rev. 2010;30:1011–8. doi: 10.1016/j.cpr.2010.07.001. [DOI] [PubMed] [Google Scholar]
- 21.Zhang ZS, Wang XL, Xu CL, Zhang C, Cao Z, Xu WD, et al. Music reduces panic: An initial study of listening to preferred music improves male patient discomfort and anxiety during flexible cystoscopy. J Endourol. 2014;28:739–44. doi: 10.1089/end.2013.0705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Raheem OA, Mirheydar HS, Lee HJ, Patel ND, Godebu E, Sakamoto K, et al. Does listening to music during office-based flexible cystoscopy decrease anxiety in patients: A prospective randomized trial. J Endourol. 2015;29:791–6. doi: 10.1089/end.2015.0029. [DOI] [PubMed] [Google Scholar]