

Abstract
Sedentary behavior (SB) is a major contributing factor to obesity and significant morbidity and mortality in adolescence and into adulthood, yet measuring SB is difficult. The purpose of this study was to assess the degree of construct validity of the ActiGraph GT3X+ inclinometer function and accelerometry metrics in objectively measuring SB and physical activity in young adult university students while performing semi-structured activities: lying, sitting, reading, playing seated video gaming, video watching, seated conversation, standing, stationary biking, and walking. These nine activities were objectively assessed using inclinometry and four output metrics from the ActiGraph based on the axis used to detect activity. Considering overall accuracy in measuring both sedentary behavior and physical activity, all four accelerometer metrics (94.7%-97.8%) outperformed the inclinometer function (70.9%). While accelerometry was overall more accurate at detecting the behaviors tested, inclinometry had similar or better accuracy than some accelerometry methods at detecting walking, biking, and standing. Using vector magnitude accelerometry with a sedentary threshold of 150 counts per minute was superior to other methods. The findings support use of accelerometry as a valid objective measure of body movement while use of inclinometry as a sole measure is not recommended. Additional research would be beneficial to improve the inclinometer and explore ways of combining this with accelerometer data for objectively measuring SB and physical activity.
Keywords: inclinometry, accelerometry, sedentary behavior, physical activity
Sedentary behavior (SB) is an emerging field of interest to health researchers, particularly because of its associations with obesity, acute and chronic disease development, and early mortality (Daniels et al., 2005; Fontaine, Redden, Wang, Westfall, & Allison, 2003; Freedman, Khan, Dietz, Srinivasan, & Berenson, 2001; Ogden, Carroll, Kit, & Flegal, 2012). Daily amounts of SB account for a major proportion of total behavior, particularly with the adolescent and young adult populations (American Heart Association [AHA], 2011). This population experiences 30-40 or more hours per week of non-sleeping SB, while most do not meet recommended physical activity guidelines (Nelson, Story, Larson, Neumark-Sztainer, & Lytle, 2008).
Although SB is part of the continuum of behavior and activity ranging from sedentary to light, moderate, and vigorous physical activity, SB plays a unique role in health regardless of other factors, including engagement in exercise. For example, the impact of SB on cardiovascular health is significant, independent of physical activity (Healy et al., 2008). Furthermore, independent of other variables, SB is linked with metabolic syndrome, hypertension, and colorectal cancer in adulthood (Healy et al., 2008; Marchand, Wilkens, Kolonel, Hankin, & Lyu, 1997). Because of its independent importance, defining and measuring SB is critical to accurately determining its effect on the health of individuals.
Quantifying SB is challenging because of difficulty measuring such low activity levels with existing self-reports or instrumentation. Development of valid measurements would provide a better way to estimate outcomes of SB. Better measurement would provide a means of exploring appropriate levels of SB and evaluating the effects of interventions designed to reduce SB (Bennett, Winters-Stone, Nail, & Scherer, 2006; Freedson, Pober, & Janz, 2005; Pate, O’Neill, & Lobelo, 2008; Sasaki, John, & Freedson, 2011). Currently, accelerometry is the standard for objectively measuring SB and is used for national research such as National Health and Nutrition Examination Survey (NHANES). Accelerometers use counts per minute (cpm) as a method of measurement, similar to steps per minute for pedometers. A “count” is the amount of movement and speed in a particular direction (acceleration). Older accelerometers measure movement in the vertical plane (Y-axis). Some newer accelerometer models can now measure movement in three directions, having X-, Y-, and Z-axes. In the young adult population SB has been defined as less than 100 cpm using the single, Y-axis only accelerometers (Troiano et al., 2008).
The prevalent tool of accelerometry is widely used for assessing SB by amount of whole body movement although new methods of measuring SB are becoming available. One novel method of investigating SB is by measuring body position using a device called an inclinometer. The inclinometer is new technology that appears to have some supporting validation (Carr & Mahar, 2012). Because lying and sitting positions have been previously described as sedentary (Pate et al., 2008), measuring SB by detecting these positions through body incline may prove useful beyond simply measuring total body movement done by accelerometry. If found to be accurate, an inclinometer would not only discriminate between sedentary and active behaviors but it would also report type of behavior (lying, sitting, or standing) which an accelerometer cannot give. An inclinometer, however, does not differentiate the physical activity intensity level like the accelerometer does. One device, the ActiGraph GT3X+, houses both an inclinometer and accelerometer within the same unit and can gather both data simultaneously.
Standardized cut points for defining sedentary and physically active behaviors by accelerometry have been used for NHANES, which includes the young adult population (Troiano et al., 2008). However, most thresholds were established using older technology that only utilized the single, vertical axis. Upgrades in technology now incorporate measuring movement in three dimensions and combining the data into a single vector, a method called vector magnitude. Minimal research exists that determines the threshold between sedentary and non-sedentary behavior using the vector magnitude. For example, although the typical accelerometry cut point for SB is <100 cpm (Treuth et al., 2004; Troiano et al., 2008), there is evidence that a higher threshold is more accurate (Romanzini, Petroski, Ohara, Dourado, & Reichert, 2012) such as <150 cpm (Kozey-Keadle, Libertine, Lyden, Staudenmayer, & Freedson, 2011). A higher threshold would make sense when using the vector magnitude since it gathers data from three axes, rather than a single axis. Once there are accurate and precise measurements of SB in controlled settings, researchers can then use these techniques to measure these behaviors in natural environments involving free-living conditions. The purposes of this study were to 1) explore the degree of construct validity of the inclinometer function within the ActiGraph GT3X+ device, as well as 2) assess ability to distinguish sedentary from non-sedentary behaviors using accelerometer thresholds of 100 cpm and 150 cpm using both single axis and vector magnitude methods.
Methods
Sample
The target population included young adult university students of varying socio-demographic backgrounds and body sizes. Study participants included a convenience sample of 18- to 20-year-old undergraduate students enrolled at a large public university in the Mid-Atlantic region. Sample size was based on studies with similar methods and outcomes (Carr & Mahar, 2012; Kozey-Keadle, et al., 2011). Once Institutional Review Board approval was granted for the study, participants were recruited through flyers, word-of-mouth, and electronic university announcement emails sent by various departments to the appropriate age group of students.
Recruitment inclusion criteria included young adult males and females aged 18- to 20-years-old who were able and agreed to wear the ActiGraph GT3X+ device and perform the following nine activities: lie down, sit, read a book while seated, play a seated video game, watch a video, engage in seated conversation/talk on the phone, stand, pedal on a stationary bike, and walk unassisted. Additional criteria included understanding written and spoken English, and no lower body injury or condition such that performing the activities was difficult, worsened the condition, or significantly altered the participant’s ability to perform the behaviors. Participants were compensated with a $10 gift card for completing the study.
Location
The study location was in a private space, within an exercise physiology laboratory, in a research center focused on healthy youth development. There were nine stations for each of the nine tested behaviors. Although completion of the entire series of nine behaviors occurred in the same laboratory, participants moved from station to station for testing each behavior in a predetermined order that was rotated between participants. The first six behaviors received a designation of typical, everyday SB, and the order was balanced to prevent any order effects. The last three behaviors (standing, stationary biking, walking) were also performed in a balanced order.
Anthropometrics
After obtaining informed written consent, participants were weighed twice to the nearest 0.1 pound using a digital scale (Seca Scale Robusta 813, Birmingham, UK) and an average of the two measures was used. Similarly, participants' height were measured twice using a stadiometer (Shorr Height Measuring Board, Olney, MD) to the nearest 0.1 cm and an average of the two measures was used. Finally, waist circumference was averaged using two measures with a Lifetime Tape Measure (Prym-Dritz Corp, Spartanburg, SC) taken at the level of the iliac crest, just below the umbilicus to the nearest 0.5 cm.
Sedentary Behaviors
The investigator reviewed the protocol instructions for each behavior with participants before beginning and reminded participants to perform the behaviors as they would at home or school. Participants completed nine behaviors for five minutes each with a one to two minute break between activities. The order in which the nine activities were completed was rotated between participants in an effort to reduce bias associated with completing the behaviors in any particular arrangement. The following section describes the participant’s positioning for each behavior.
Lying down
Participants were in the supine position on a padded laboratory exam table with pillow support for the head and were to lie quietly with eyes open so as to not fall asleep.
Sitting
Participants sat in a comfortable, padded, non-mobile upright chair for the sitting behavior. Participants were able to move and shift positions as long as they remained seated.
Reading
The reading behavior was done in the same fashion as the sitting behavior, with participants sitting at a table and having the option of reading Harry Potter or one of their own books.
Gaming
Participants played a free, popular online game—requiring minimal instruction and needing only the mouse to operate—using a desktop computer. Seating was similar to the sitting behavior criteria.
Watching
Participants viewed a short five-minute digitally animated film on a laptop computer. Participants sat in the same manner as above.
Talking
While seated, participants had the option of talking on their personal cell phone or having a casual conversation with the researcher.
Standing
Participants were required to stand for the duration of the testing period without moving, although they could shift positions as needed.
Physical Activities
Biking
Participants used a Monark 868 stationary bike (Monark Exercise, Sweden) at moderate intensity; equivalent to speeds between 50-60 revolutions per minute, while maintaining a workload of approximately 100 Watts. Seat and handle bar height were adjusted to a comfortable position as needed for each participant. Participants stayed within the moderate intensity limits and remained seated for the duration of the testing.
Walking
A Quinton Q65 treadmill (Quinton Instrument Co., Seattle, WA) was set to a speed of 3.0 miles per hour with no incline for participants to complete the walking activity. Participants were not to hold to the side or front handlebars and were to maintain a natural walking gait.
Of the nine behaviors measured in the study, two were explicitly active by design: riding a stationary bike and walking on a treadmill. Riding the stationary bike had particular interest for this study, since pedaling at a moderate intensity is active; yet participants riding the stationary bike were in the seated position. Therefore, this activity determined whether inclinometry and/or accelerometry could accurately detect this form of seated exercise. Walking on a level treadmill at 3.0 miles per hour served as a standard for active behavior.
Demographic measures
Participants completed a simple form gathering demographic information on gender, age, semesters completed at school, and race/ethnicity.
Instrument
The ActiGraph GT3X+ is a single device that gathers both inclinometry and accelerometry data simultaneously. Therefore, participants wore just one device during the study. Participants were fitted with this device at the level of the waist, secured with an elastic band and buckle, and placed over the right hip.
The ActiGraph GT3X+ (ActiGraph, LLC, Pensacola, FL) device assessed activity by inclinometry and accelerometry. The GT3X+ is a small, unobtrusive, and essentially tamper resistant device which is well-tolerated by young adults and does not hinder activity (ActiGraph, 2013; de Vries, Bakker, Hopman-Rock, Hirasing, & van Mechelen, 2006). The GT3X+ houses both an accelerometer and inclinometer, weighing only 19 grams (ActiGraph, 2013). The inclinometer data is categorical and coded as lying, sitting, standing, or off. Accelerometry is captured in 3 axes and expressed in terms of cpm. The ActiGraph GT3X+ collected data at 30 Hz and then aggregated the data during the post-collection processing stage into 10-second epochs. The accelerometry feature of the GT3X+ is highly precise measuring SBs in both laboratory (Carr & Mahar, 2012; Sasaki et al., 2011) and in free-living conditions (Kaminsky & Ozemek, 2012; Santos-Lozano et al., 2012) according to accepted standards (Landis & Koch, 1977). Direct observation of all behaviors by the researcher provided a criterion measure of both SB and body position which was recorded each minute.
The GT3X+ accelerometer’s reliability and construct validity is high in children and young adults, typically ranging r=0.39-0.90 (de Vries et al., 2006) or, specifically to SB, between 80-98% agreement with direct observation (Carr & Mahar, 2012; Hänggi, Phillips, & Rowlands, 2013). While impressive, past research assessed validity using only single axis movement and did not take advantage of the ability of the GT3X+ to obtain the vector magnitude. Only one study, using a group that included young adults, has investigated the construct validity of the GT3X+ inclinometer, which found 63-67% agreement with direct observation (Carr & Mahar, 2012). Several studies supported criterion validity in comparison to the older accelerometer model (de Vries et al., 2006; Kaminsky & Ozemek, 2012; Sasaki et al., 2011).
Sedentary was defined as lying or sitting positions for the inclinometer method (standing was accepted as the appropriate code for the standing activity). Accelerometry data aggregation included two methods. First, the standard single axis only method was applied, using cut points at both 100 cpm (Axis100) and 150 cpm (Axis150) to determine sedentary versus active behavior. Because the accelerometer gathers movement data in three dimensions, the magnitude vector calculation used all three axes. The vector magnitude calculations compared both the 100 cpm (VM100) and 150 cpm (VM150) cut points for defining SB. Both cut points of <100 cpm and <150 cpm for SB are supported in the literature, and thus comparing accuracy of these two with this study was desirable (Kozey-Keadle et al., 2011). Utilizing the low-frequency extension option for the accelerometer improved detection of low-frequency movement; SB fits into this category.
The following is a simplified recap of the methods:
Inclinometer—inclinometer measurement only, with a sedentary definition of lying and sitting positions,
Axis100—single axis measure only with a sedentary definition of <100 cpm,
Axis150—single axis measure only with a sedentary definition of <150 cpm,
VM100—vector magnitude with a sedentary definition of <100 cpm,
VM150—vector magnitude with a sedentary definition of <150 cpm.
Statistical analyses
Statistical analyses were performed using SPSS 22.0 (IBM Corp., Chicago, IL). The five methods (inclinometer, Axis100, Axis150, VM100, VM150) were compared against the criterion of direct observation by the researcher. The researcher recorded the body position of the participants each minute during the study. Validity was calculated as the percent agreement of time spent lying and sitting from the inclinometer and time spent performing SB from the accelerometer against the criterion measure of direct observation, as noted by the researcher each minute during the study. All of the device data was available in 10-second epochs. Since each activity was performed for 5 minutes, there were 30 device data points per activity. Percent agreement of time was calculated as a comparison of those 30 data points that matched the direct observation. The 95% confidence interval for the mean was also calculated for each method.
Results
Of the 28 participants who elected to participate in the study (12 male, 16 female), every one completed the study in its entirety and there were no device failures. A summary of the sample demographics appears in Table 1. The sample was 57.1% female, and was closely split among 18 (28.6%), 19 (32.3%), and 20 (32.1%) year-olds. Of the sample, 25.0% were non-white or mixed ethnicity. The mean BMI was 22.8 (SD=3.1) kg/m2. By gender, the mean waist circumference was 86.6 (SD=9.1) cm and 84.2 (SD=7.7) cm, for males and females, respectively. Seven (25.0%) participants were overweight when considering either BMI (≥25.0 kg/m2) or waist circumference (≥102 cm for males, ≥88 cm for females).
Table 1.
Demographic Characteristics of the University Males (n=12) and Females (n=16)
| Items | Males, n (%) | Females, n (%) |
|---|---|---|
| Age (years) | ||
| 18 | 2 (16.7) | 6 (37.5) |
| 19 | 4 (33.3) | 7 (43.8) |
| 20 | 6 (50.0) | 3 (18.8) |
| Race | ||
| White/Caucasian | 9 (75.0) | 12 (75.0) |
| Other/Mixed | 3 (25.0) | 4 (25.0) |
| Body Mass Index (kg/m2) | ||
| Overweight (≥25.0) | 2 (16.7) | 3 (18.8) |
| Not overweight (<25.0) | 10 (83.3) | 13 (81.2) |
| Waist Circumference (cm) | ||
| Overweight (M≥102, F ≥88) | 1 (8.3) | 5 (31.2) |
| Not overweight (M <102, F <88) | 11 (91.7) | 11 (68.8) |
In considering the mean percentage of time that was coded correctly (Figure 1), the accelerometry data outperformed the inclinometry data in every category except for walking (all methods were 100% valid) and using the stationary bike in the case of the single axis methods (Axis100 and Axis150). The inclinometer varied in correctly identifying sedentary from active behaviors from a low of 44.9% during seated video gaming to a high of 100% for walking. For the Axis100 and Axis150 methods, validity in measuring these behaviors ranged from 98.8% to 100%, with the exception of the stationary bike activity, which was correct 54.8% and 48.8% of the time, respectively. Both vector magnitude methods perfectly detected active behaviors, and validity for measuring SB ranged from ≥90.5% for the VM100 method and ≥95.2% for the VM150 method. Full details of validity of the five methods on each behavior are reported in Figure 1.
Figure 1.
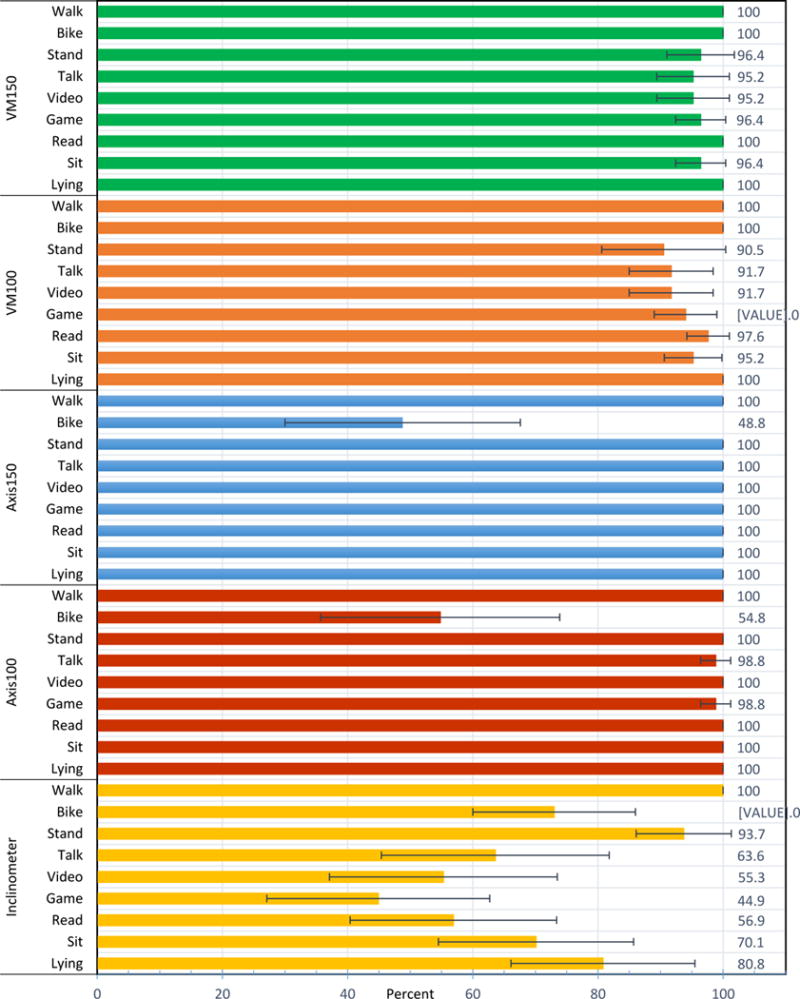
Percent Agreement to Direct Observations on Each Behavior by Method with 95% Confidence Interval. Inclinometer = inclinometer only; Axis100 = single axis with sedentary cutoff of <100 counts per minute (cpm); Axis150 = single axis with sedentary cutoff of <150 cpm; VM100 = vector magnitude with sedentary cutoff of <100 cpm; VM150 = vector magnitude with sedentary cutoff of <150 cpm.
Overall percent agreement was lower for the inclinometer compared to any of the accelerometer settings (Table 2). In assessing sedentary versus active behavior as the primary endpoint, the inclinometer was not as accurate as the accelerometer methods in detecting SB, but it did have similar success to the Axis100 and Axis150 methods in detecting active behaviors. With respect to the seated stationary bike, the inclinometer correctly detected a sitting position only 27.0% (95% confidence interval [CI]=14.1-40.0%) of the time. When total body movement exceeds the sedentary threshold, however, the inclinometer automatically codes for “standing”, regardless of actual body position. Therefore, when accepting the “standing” code as active, the accuracy jumps to 73.0% (95% CI=60.0%-86.0%). These differences affected the inclinometer’s active and overall accuracy. When considering true body position, validity of the inclinometer to detect active behaviors is 63.5% (95% CI=57.1-70.0%), with an overall accuracy of 65.8% (95% CI=59.9-71.8%). However, when accounting for the fact that the device automatically codes for “standing” when above the sedentary threshold, the inclinometer measures active behaviors correctly 86.5% (95% CI=80.0-92.9%) of the time, with an overall accuracy of 70.9% (95% CI=65.0-76.9%).
Table 2.
Percent Agreement (95% Confidence Interval) to Direct Observation by Method for Sedentary Behaviors, Active Behaviors, and Across All Behaviors
| Method | Sedentary Behaviors | Active Behaviors | Overall |
|---|---|---|---|
| Inclinometer | 66.5 (59.1-73.9) | 86.5 (80.0-92.9) | 70.9 (65.0-76.9) |
| Axis100 | 99.7 (99.0-100.4) | 77.4 (67.9-86.9) | 94.7 (92.4-97.0) |
| Axis150 | 100.0 (100.0-100.0) | 74.4 (65.0-83.8) | 94.3 (92.2-96.4) |
| VM100 | 94.4 (91.0-97.8) | 100.0 (100.0-100.0) | 95.6 (93.0-98.3) |
| VM150 | 97.1 (95.0-99.3) | 100.0 (100.0-100.0) | 97.8 (96.1-99.4) |
Note. Sedentary behaviors: lying down, sitting, reading, video gaming, watching a video, seated conversation, standing. Active behaviors: walking, stationary biking. Inclinometer = inclinometer only, with a sedentary definition of lying and sitting positions; Axis100 = uses the single axis measure only (Y-axis) with a sedentary definition of <100 counts/minute; Axis150 = uses the single axis measure only (Y-axis) with a sedentary definition of <150 counts/minute; VM100 = uses the vector magnitude combining X-Y-Z axes, with a sedentary definition of <100 counts/minute; VM150 = uses the vector magnitude combining X-Y-Z axes with a sedentary definition of <150 counts/minute.
Discussion
The aim of this study was to determine the validity of the ActiGraph GT3X+ in discriminating sedentary from non-sedentary behaviors in terms of both inclinometry and accelerometry. The results support the GT3X+ as a valid device for measuring SB and, in general, accelerometry outperforms inclinometry for measuring SB and in overall validity. Considering validity in measuring SB, all four accelerometry methods outperformed inclinometry.
The stationary bike activity played a major factor in determining the validity of each method, particularly with the single axis (Axis100, Axis 150) methods. Both vector magnitude methods detected biking as an active behavior 100% of the time, while the single axis methods were only 54.8% (Axis100) and 48.8% (Axis150) accurate. The discrepancy between the two methods probably lies in the fact that minimal up and down (Y-axis) movement occurs during seated biking, yet there may be more side to side (Z-axis) or forward and back (X-axis) movement that the participant does to maintain speed and momentum of pedaling. Any activity done while sitting is similar, since the very nature of sitting would take away or limit the factor of the vertical axis in contributing to the overall activity detected by the device. Using vector magnitude rather than a single axis for detecting SB and physical activity is still relatively new, particularly in the younger age groups, and has had mixed results. There is a need for further research in this area (Freedson et al., 2005; Howe, Staudenmayer, & Freedson, 2009).
Determining the superiority of single axis or vector magnitude accelerometry data would enhance research in the area of SB and physical activity (Freedson et al., 2005). This study suggests that the use of vector magnitude data might be better than single axis measurements in two specific ways. First, vector magnitude was an excellent method for measuring seated, but active, behaviors such as biking. Both vector magnitude methods surpassed single axis for both the 100 cpm and 150 cpm cut points for the biking activity. Overall accuracy in measuring all nine behaviors also favors vector magnitude over single axis (Table 2).
The inclinometer’s ability to accurately detect biking is mixed and depends on the output that the researcher is studying. Per the manufacturer’s design, once the GT3X+ device registers a high enough movement threshold (6 counts per second), the inclinometer output will automatically code as standing (Hawk, 2012). This feature explains why the inclinometer’s walk accuracy (100%) is better than the stand accuracy (93.7%). If the intent of the research is to distinguish between sedentary versus active behaviors, this design element is beneficial, as it will default to the standing output regardless of the actual incline. However, if detecting body position were the ultimate goal, this feature would prevent an accurate measurement. For example, when registering body incline, the inclinometer was only 27.0% accurate for detecting the sitting position while participants used the stationary bike. However, this accuracy jumped to 73.0% when adjusting for the fact that the standing position was considered active for that particular behavior. This too, has its drawbacks, since using “standing” as a default code for “active” would have the effect of categorizing the test of standing in place as being active, when in reality this expends very little energy. However, most people likely do not stand perfectly still or in a single spot for long periods. In fact, standing has been considered by some as non-sedentary as it may contribute to improved insulin and lipid management simply by not having the body in the lying or sitting sedentary positions (Duvivier et al., 2013). Considering these two dilemmas, the future use of the inclinometer likely plays a role when analyzing inclinometer and accelerometer data together, since integrating the two would resolve dual issues of “sitting but active” and “standing but sedentary.”
The results of this study support the general body of literature validating the ActiGraph GT3X+ accelerometer in measuring sedentary and active behaviors with the caveat that the standard of <100 cpm as the definition of sedentary should be raised to <150 cpm when using the vector magnitude. However, the current literature is fraught with discussion on whether single-axis versus vector magnitude is the best method for measuring sedentary and activity level (Freedson et al., 2005; Howe et al., 2009). Furthermore, the thresholds for SB and the various levels of physical activity differ depending on the population of interest (Freedson et al., 2005; Kozey-Keadle et al., 2011; Mattocks et al., 2007; Troiano et al., 2008; Trost, Loprinzi, Moore, & Pfeiffer, 2011). With respect to the inclinometer, although it had high (86.5%) accuracy for detecting active behaviors, its method of coding makes it unable to discriminate light, moderate, or vigorous activity, since all of these would be coded as “standing.” Thus, the best use of the inclinometer is to detect body position or use in conjunction with accelerometry data when assessing both sedentary and physical activity levels.
Additional results of this study demonstrate the difficulty in finding new objective measures of SB. While the inclinometer function within the ActiGraph device has the potential to help define behaviors in terms of body position, its use as the sole measure of SB is not supported by the results of this study. The ability to calibrate the angles that the inclinometer function uses to define the lying, sitting, and standing positions could likely improve the output of the device. While other inclinometer devices exist, the advantage of developing the inclinometer function for the ActiGraph would be that both metrics (inclinometer and accelerometer) would be available from a single unit and would also reduce participant burden. Both the accelerometer and the inclinometer add a unique perspective to measuring sedentary and active behaviors. Together, they measure both intensity and behavior. While the accelerometer differentiates the spectrum of total body movement, the inclinometer offers the ability to categorize how the body is engaged, be it lying, sitting, or standing. Future research to investigate combining inclinometer data with that of the accelerometer may give additional insight into what constitutes SB and physical activity.
Limitations
Limitations of this study include a small, mostly Caucasian sample. Results are not generalizable beyond the age ranges examined in this study. In addition, the study examined more SBs than active behaviors, by design, and was limited to discriminating typical lying and sitting behaviors against walking and biking. Body positioning during the behaviors may not have always been the natural position since participants were not in their free-living condition. Increasing testing time may have given a more accurate perspective on SB as participants “settle in” to their environment and the behavior being tested. Also, the behaviors tested may not be typical of SB in every population. Lastly, there was not a full discrimination between SB and light physical activity. However, validating the cut points for light, moderate, and vigorous physical activity was not an objective of this study. Rather the aim was to discriminate SB from routine physical activities predominantly used in the young adult university student population.
Implications
This study has expanded the knowledge of objective measurement of SB by contributing evidence about the validity of the ActiGraph GT3X+ and various methods in quantifying sedentary and active behaviors. The technology of inclinometry is relatively new, yet has demonstrated potential in measuring SB using body position as a criterion. This research concluded that the ActiGraph GT3X+ inclinometer feature is approximately 70% accurate in determining sedentary versus non-sedentary behavior overall, which is congruent with another study using the ActiGraph inclinometer function (Carr & Mahar, 2012). Rigorous scientific research could further improve the inclinometer by validating categorization of the angles of lying, sitting, and standing. An option to adjust these angle definitions through ActiGraph’s software may allow for correcting incline data, though accurately determining activities such as bicycling could continue to be problematic. Body position has been implicated as a strong factor in determining what is defined as sedentary (Pate et al., 2008). Therefore, the inclinometer has potential for future use in measuring SB though future research must explore the how and when of such use. Additionally, as long as it does not rely on constant body movement to gather data, like the accelerometer, the inclinometer could become a good way to detect low-threshold behaviors, which SB dominates.
Additional research is needed to help define appropriate sedentary, light, moderate, and vigorous activity in terms of three-dimensional movement (Sasaki et al., 2011). As vector magnitude is a relatively new way of analyzing accelerometry data, future studies should be clear about data processing and whether single-axis or vector magnitude was the selected method. This ultimately will influence the choice of activity cut points, such as the 100 versus 150 cpm threshold decision on SB.
Summary
In summary, there is a need to establish objective measurement standards for SB because of its important health consequences. There is a need for additional validation of novel methods of measuring SB before the variable is accepted for use in research. The inclinometer is moderately accurate overall, and would be improved with additional testing and calibration. Accelerometry remains a good standard by which to measure SB; however, clarity and refinement of appropriate thresholds for SB, and light, moderate, and vigorous physical activity needs additional appraisal across all age groups, as vector magnitude data becomes the standard. Therefore, as technology constantly advances, continuous assessment of valid and reliable methods for determining SB and physical activity will guide researchers in proper measurement. Collaborative efforts that include nursing, medicine, exercise physiology, public health, and others are needed to interpret SB measurement and to explore the implications of SB on healthy lifestyles.
Acknowledgments
Funding/disclosers: NIH pre-doctoral NRSA grant through NINR, Grant # F31 NR14366-01A1.
Footnotes
The authors declare no conflicts of interest.
Contributor Information
Neil E. Peterson, Assistant Professor, College of Nursing, Brigham Young University.
John R. Sirard, Assistant Professor, Department of Kinesiology, University of Massachusetts Amherst, 159D Totman Building, Amherst, MA, USA 01003, 413-545-7898.
Pamela A. Kulbok, Professor, School of Nursing, University of Virginia, 225 Jeanette Lancaster Way, Claude Moore Nursing Education Building 2003, Charlottesville, VA, USA 22908-0128, 434-924-0128.
Mark D. DeBoer, Associate Professor, School of Medicine, University of Virginia, Department of Pediatrics, PO Box 800793, Charlottesville, USA 22908, 434-924-9833.
Jeanne M. Erickson, Assistant Professor, College of Nursing, University of Wisconsin-Milwaukee, Cunningham Hall 671, 1921 E Hartford Ave, Milwaukee, WI, USA 53211, 414-229-6920.
References
- ActiGraph. GT3X+ and wGT3X+ device manual ActiGraph, LLC. 2013 Jan; Retrieved from https://help.theactigraph.com/entries/22041532.
- AHA. Understanding childhood obesity: 2011 statistical sourcebook. American Heart Association; 2011. Retrieved from http://www.heart.org/idc/groups/heart-public/@wcm/@fc/documents/downloadable/ucm_428180.pdf. [Google Scholar]
- Bennett JA, Winters-Stone K, Nail LM, Scherer J. Definitions of sedentary in physical-activity-intervention trials: a summary of the literature. Journal of Aging and Physical Activity. 2006;14(4):456–477. doi: 10.1123/japa.14.4.456. [DOI] [PubMed] [Google Scholar]
- Carr LJ, Mahar MT. Accuracy of Intensity and Inclinometer Output of Three Activity Monitors for Identification of Sedentary Behavior and Light-Intensity Activity. Journal of Obesity. 2012;2012:1–9. doi: 10.1155/2012/460271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniels SR, Arnett DK, Eckel RH, Gidding SS, Hayman LL, Kumanyika S, … Williams CL. Overweight in Children and Adolescents Pathophysiology, Consequences, Prevention, and Treatment. Circulation. 2005;111(15):1999–2012. doi: 10.1161/01.CIR.0000161369.71722.10. [DOI] [PubMed] [Google Scholar]
- De Vries SI, Bakker I, Hopman-Rock M, Hirasing RA, van Mechelen W. Clinimetric review of motion sensors in children and adolescents. Journal of Clinical Epidemiology. 2006;59(7):670–680. doi: 10.1016/j.jclinepi.2005.11.020. [DOI] [PubMed] [Google Scholar]
- Duvivier BMFM, Schaper NC, Bremers MA, van Crombrugge G, Menheere PPCA, Kars M, Savelberg HHCM. Minimal Intensity Physical Activity (Standing and Walking) of Longer Duration Improves Insulin Action and Plasma Lipids More than Shorter Periods of Moderate to Vigorous Exercise (Cycling) in Sedentary Subjects When Energy Expenditure Is Comparable. PLoS ONE. 2013;8(2):e55542. doi: 10.1371/journal.pone.0055542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of Life Lost Due to Obesity. JAMA: The Journal of the American Medical Association. 2003;289(2):187–193. doi: 10.1001/jama.289.2.187. [DOI] [PubMed] [Google Scholar]
- Freedman DS, Khan LK, Dietz WH, Srinivasan SR, Berenson GS. Relationship of Childhood Obesity to Coronary Heart Disease Risk Factors in Adulthood: The Bogalusa Heart Study. Pediatrics. 2001;108(3):712–718. doi: 10.1542/peds.108.3.712. [DOI] [PubMed] [Google Scholar]
- Freedson P, Pober D, Janz KF. Calibration of accelerometer output for children. Medicine and Science in Sports and Exercise. 2005;37(11 Suppl):S523–530. doi: 10.1249/01.mss.0000185658.28284.ba. [DOI] [PubMed] [Google Scholar]
- Hänggi JM, Phillips LRS, Rowlands AV. Validation of the GT3X ActiGraph in children and comparison with the GT1M ActiGraph. Journal of Science and Medicine in Sport / Sports Medicine Australia. 2013;16(1):40–44. doi: 10.1016/j.jsams.2012.05.012. [DOI] [PubMed] [Google Scholar]
- Hawk L. How does the ActiGraph device determine inclination (for waist wear locations)? ActiGraph Support. 2012 Dec 18; Retrieved January 25, 2014, from https://help.theactigraph.com/entries/22652363-How-Does-The-ActiGraph-Device-Determine-Inclination-for-Waist-Wear-Locations-
- Healy GN, Wijndaele K, Dunstan DW, Shaw JE, Salmon J, Zimmet PZ, Owen N. Objectively measured sedentary time, physical activity, and metabolic risk: the Australian Diabetes, Obesity and Lifestyle Study (AusDiab) Diabetes Care. 2008;31(2):369–371. doi: 10.2337/dc07-1795. [DOI] [PubMed] [Google Scholar]
- Howe CA, Staudenmayer JW, Freedson PS. Accelerometer prediction of energy expenditure: Vector magnitude versus vertical axis. Medicine & Science in Sports & Exercise December 2009. 2009;41(12):2199–2206. doi: 10.1249/MSS.0b013e3181aa3a0e. [DOI] [PubMed] [Google Scholar]
- Kaminsky LA, Ozemek C. A comparison of the Actigraph GT1M and GT3X accelerometers under standardized and free-living conditions. Physiological Measurement. 2012;33(11):1869–1876. doi: 10.1088/0967-3334/33/11/1869. [DOI] [PubMed] [Google Scholar]
- Kozey-Keadle S, Libertine A, Lyden K, Staudenmayer J, Freedson PS. Validation of wearable monitors for assessing sedentary behavior. Med Sci Sports Exerc. 2011;43(8):1561–1567. doi: 10.1249/MSS.0b013e31820ce174. [DOI] [PubMed] [Google Scholar]
- Landis JR, Koch GG. The Measurement of Observer Agreement for Categorical Data. Biometrics. 1977;33(1):159–174. doi: 10.2307/2529310. [DOI] [PubMed] [Google Scholar]
- Marchand LL, Wilkens LR, Kolonel LN, Hankin JH, Lyu LC. Associations of Sedentary Lifestyle, Obesity, Smoking, Alcohol Use, and Diabetes with the Risk of Colorectal Cancer. Cancer Research. 1997;57(21):4787–4794. [PubMed] [Google Scholar]
- Mattocks C, Leary S, Ness A, Deere K, Saunders J, Tilling K, Riddoch C. Calibration of an accelerometer during free-living activities in children. International Journal of Pediatric Obesity. 2007;2(4):218–226. doi: 10.1080/17477160701408809. [DOI] [PubMed] [Google Scholar]
- Nelson MC, Story M, Larson NI, Neumark-Sztainer D, Lytle LA. Emerging adulthood and college-aged youth: An overlooked age for weight-related behavior change. Obesity. 2008;16(10):2205–2211. doi: 10.1038/oby.2008.365. [DOI] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999-2010. Journal of the American Medical Association. 2012;307(5):483–490. doi: 10.1001/jama.2012.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pate RR, O’Neill JR, Lobelo F. The Evolving Definition of “Sedentary”. Exercise and Sport Sciences Reviews. 2008;36(4):173–178. doi: 10.1097/JES.0b013e3181877d1a. [DOI] [PubMed] [Google Scholar]
- Romanzini M, Petroski EL, Ohara D, Dourado AC, Reichert FF. Calibration of ActiGraph GT3X, Actical and RT3 accelerometers in adolescents. European Journal of Sport Science. 2012:1–9. doi: 10.1080/17461391.2012.732614. [DOI] [PubMed] [Google Scholar]
- Santos-Lozano A, Torres-Luque G, Marín P, Ruiz J, Lucia A, Garatachea N. Intermonitor Variability of GT3X Accelerometer. International Journal of Sports Medicine. 2012;33(12):994–999. doi: 10.1055/s-0032-1312580. [DOI] [PubMed] [Google Scholar]
- Sasaki JE, John D, Freedson PS. Validation and comparison of ActiGraph activity monitors. Journal of Science and Medicine in Sport. 2011;14(5):411–416. doi: 10.1016/j.jsams.2011.04.003. [DOI] [PubMed] [Google Scholar]
- Treuth MS, Schmitz K, Catellier DJ, McMurray RG, Murray DM, Almeida MJ, Pate R. Defining Accelerometer Thresholds for Activity Intensities in Adolescent Girls. Medicine and Science in Sports and Exercise. 2004;36(7):1259–1266. [PMC free article] [PubMed] [Google Scholar]
- Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Medicine and Science in Sports and Exercise. 2008;40(1):181–188. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc. 2011;43(7):1360–1368. doi: 10.1249/MSS.0b013e318206476e. [DOI] [PubMed] [Google Scholar]