

Abstract
Objective:
To review the literature regarding diagnosis and treatment of labral tear.
Data sources:
A systematic search was performed in PubMed using various search terms and their combinations including hip, labrum, acetabular labral tear, arthroscopy, diagnosis, and anatomy.
Study selection:
For each included study, information regarding anatomy, function, etiology, diagnosis, and management of acetabular labral tear was extracted.
Results:
Five hundred and sixty abstracts about anatomy, function, etiology, diagnosis, and management of acetabular labral tear were reviewed and 66 selected for full-text review. The mechanism of labral tear has been well explained while the long-term outcomes of various treatment remains unknown.
Conclusions:
Labral tear is generally secondary to femoroacetabular impingement, trauma, dysplasia, capsular laxity, and degeneration. Patients with labral tear complain about anterior hip or groin pain most commonly with a most consistent physical examination called positive anterior hip impingement test. Magnetic resonance arthrography is a reliable radiographic examination with arthroscopy being the gold standard. Conservative treatment consists of rest, non-steroidal anti-inflammatory medication, pain medications, modification of activities, physical therapy, and intra-articular injection. When fail to respond to conservative treatment, surgical treatment including labral debridement, labral repair, and labral reconstruction is often indicated.
Keywords: Hip, Labrum, Acetabular labral tear, Arthroscopy, Repair
Introduction
Labral tear is first introduced by Peterson in 1957 with 2 cases secondary to posterior hip dislocation.[1] In 1986, labral tear was 1st diagnosed arthroscopically.[2] With the development of imaging technique and arthroscopy, labral tear is diagnosed more frequently in patients complaining about groin pain nowadays than in the past.[3] Labral tear occurs most commonly under the circumstance of femoroacetabular impingement (FAI), which is characteristic by deformity of acetabulum, femoral head, or both.[4] If the torn labrum and the underlying etiology remains untreated, the hip joint may progress to osteoarthritis prematurely.[5,6] Labral repair is increasingly favored options as the preservation of labrum leads to a superior outcome compared with debridement of labrum.[7-9] With the advancement of techniques and instruments, when labrum is deemed irreparable due to a hypotrophy labrum or previous debrided labrum, the emergence of labral reconstruction seems to account for a more promising outcome than debridement despite long-term follow-up is needed for it to be a supportive evidence.[10,11] The purpose of this review was to present a comprehensive literature review about the diagnosis and different method of torn labral management.
Methods
Articles were searched online in PubMed using the following searched terms: (labrum OR labral) AND (hip). The search was updated until June 26, 2018. Studies and the abstracts associated with THA, Legg-Calve-Perthes disease, slipped capital femoral epiphysis and osteonecrosis were excluded accounting for 70 remaining articles. Studies were further filtrated with the inclusion criteria: information about anatomy, function, etiology, diagnosis, and management of acetabular labral tear. About 66 articles were included and reviewed for this study.
Anatomy and function of labrum
The labrum is a triangular fibrocartilage attached to the acetabular rim almost circumferentially with a transition into the transverse acetabular ligament at the acetabular notch [Figure 1].[12] The anterior portion of labrum is wider and thinner while the posterior labrum is thicker with a formation of sulcus that is easily misunderstood for pathology.[12,13] The innervation of labrum is most concentrated in the anterosuperior part with a composition of free nerve endings and sensory nerve end organs.[14] The blood supply of labrum is found to be circumferential originated from the obturator, superior gluteal, and inferior gluteal arteries.[13] The peripheral one-third of the labrum is vascular compared with its avascular articular side.[15,16] Moreover, the blood supply at the edge of labrum is less abundant than that of the base part of labrum.[16-18]
Figure 1.
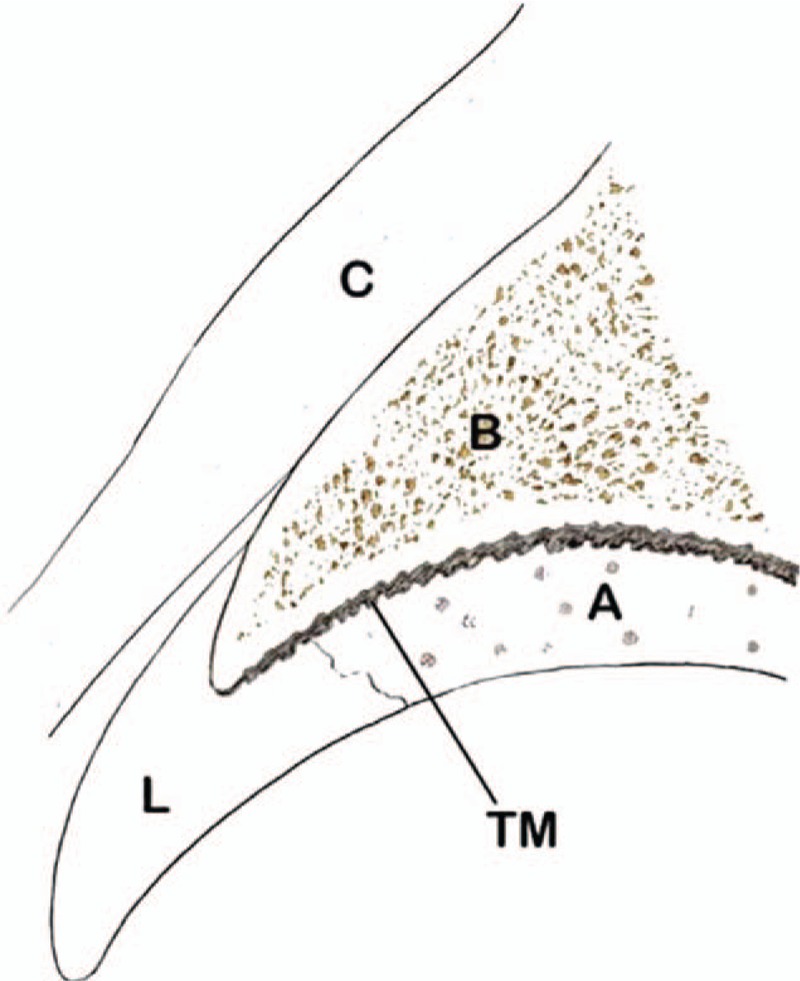
Relationship of the acetabular labrum and capsule. A: Articular cartilage; B: Acetabulum; C: Capsule; L: Labrum; TM: Tide mark.
The labrum is of great importance to the stability of hip joint as it deepens the acetabulum against femoral head translation. The labrum increases the articular surface by 22% and the acetabular volume by 33%.[13] In addition, labrum creates a vaccum with a negative pressure that increases the difficulty of dislocating the hip and retains the fluid within the central compartment to lubricate the joint and even the distribution of contact forces across the articular surface, preventing early arthritic wear.[13]
Etiology
Generally, acetabular labral tear is secondary to FAI, trauma, dysplasia, capsular laxity and degeneration.[19]
The FAI is the most common cause of labral tear.[4] It is a concept of incongruence between femoral head and acetabulum classified into cam, pincer, and mixed types. Cam type is a bony protrusion at the anterolateral head-neck junction thus the non-spherical portion collides with the acetabular rim producing a shear force to the adjacent articular cartilage meanwhile keeping the labrum untouched thus it dominantly disrupts the chondrolabral conjunction and causes the articular cartilage and labrum to delaminate but relatively preserve the labrum [Figure 2].[20,21] Conversely, Pincer type is characteristic by over-coverage of the femoral head by acetabulum focally or globally accounting for the breakdown of labrum and adjacent cartilage because the contact between proximal femur and acetabulum is linear [Figure 2].[20] Mixed type presents the deformity of both the femur and acetabulum.
Figure 2.
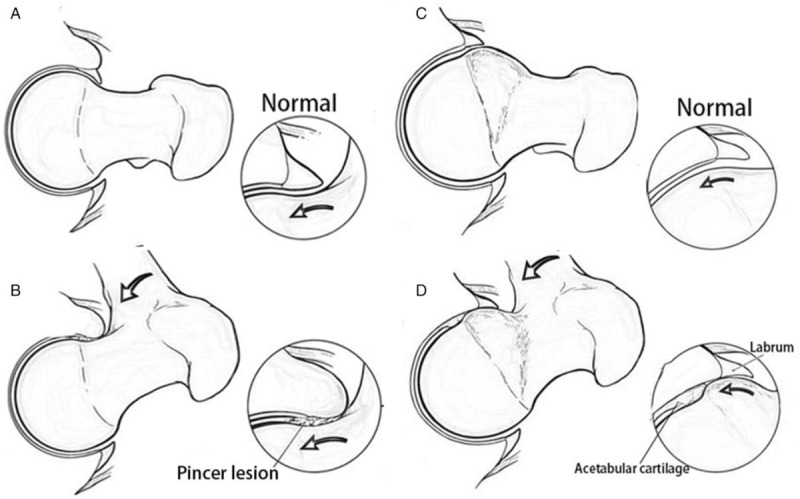
(A) Bony over-coverage of the anterior labrum. (B) With hip flexion, the anterior labrum gets crushed by the pincer lesion against the neck of the femur. (C) Bony prominence centered on the anterolateral femoral head/neck junction. (D) Delamination of labrum and cartilage progresses as the cam lesion glides under the labrum with hip flexion.
Labral tear is often a result of significant trauma causing either subluxation or dislocation of the femoral head and commonly associated with chondral injuries at femoral or acetabular side.[19] Capsular laxity correlating with underlying collagen disorders or hormonal influences can lead to the attenuation of the iliofemoral ligament under repetitive rotational activities. The combined effects finally cause the rotational instability of hip thus increasing the pressure on the anterior superior labrum as the head rides anterior in the joint.[19] Dysplastic bony abnormalities include a shallow acetabulum, a reduction in acetabular or femoral anteversion, acetabular retroversion, and a decreased head offset or perpendicular distance from the center of the femoral head to the axis of the femoral shaft, which changes the position of femoral head within the acetabulum thus decreasing joint surface area (anteriorly in most cases) and increasing stresses on the acetabulum and the labrum ultimately leading to a labral tear [Figures 3 and 4].[22,23] Labral tear under the circumstance of degeneration is more of a natural history of aging joint.[22]
Figure 3.
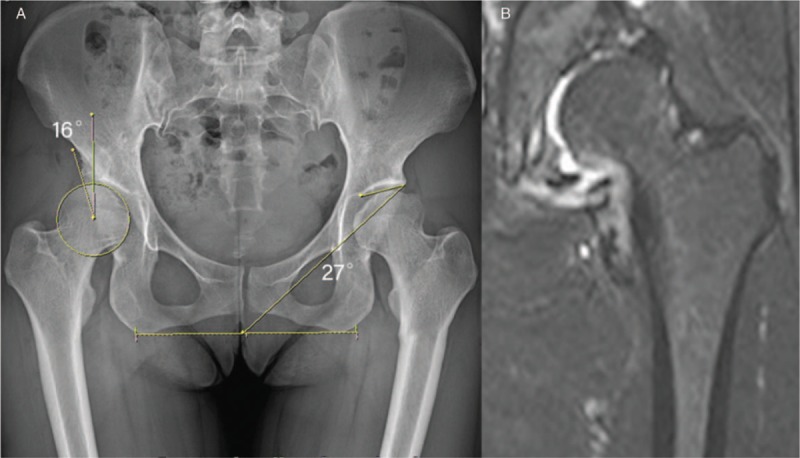
(A) Demonstrates a lateral center-edge angle of the right hip of 16° and acetabular roof angle or Tönnis angle of 27°. These measurements are both considered abnormal and consistent with acetabular dysplasia. (B) Coronal section magnetic resonance imaging of a dysplastic hip. The labrum is hypertrophic and contrast medium is running through the base of the labrum, an indication that the labrum is detached from the acetabular rim.
Figure 4.

The impingement test is performed by provoking pain with flexion, adduction, and internal rotation of the symptomatic hip.
Symptoms and physical examination
The most familiar complain of patients is the anterior hip or groin pain which may sometimes radiate to the knee.[22-24] In general, the pain develops gradually and occurs at night in most cases with patients describing a constant dull pain but may worsen with certain movement like walking, pivoting, prolonged sitting, and running representing a sharp pain.[24] The less mechanical symptoms include clicking, locking or catching, or giving way.[22,25]
As for physical examination, the most specific examination finding is positive anterior hip impingement test, which is performed in patient with 90° flexion of hip and knee, adduction and internal rotation of the symptomatic hip [Figure 4]. While the test provocates pain in the anterolateral hip or groin, it may imply that labral tear is located anteriorly.[24,26] In contrast, posterior hip impingement test, which is positive when pain is induced by letting patient lie prone with hip and knee extended and the passively extending, adducting, and externally rotating hip.[24] Other less-specific tests include Patrick/Faber test, resisted straight leg raise test, Log-roll test, and the apprehension test.[22,24]
Imaging evaluation
Because labral tear rarely occurs in the absence of subtle structural abnormalities of the hip and pelvis, it is important to find out those underlying causes through radiographic evaluation. Radiographic evaluations include an AP pelvis and a cross-table lateral of the affected side, magnetic resonance imaging (MRI) and magnetic resonance arthrography (MRA). The cross-table lateral radiograph was performed in the supine position, with the leg held in 15° of internal rotation and the contralateral hip in full flexion, which provides an accurate view of the amount of femoral head-neck off set. The AP pelvic radiographs are shot in standard fashion in the supine position, with the beam positioned directly over the pelvis, through which we can obtain a center-edge angle as a measurement for the evaluation of dysplasia, and a crossover sign indicating a pincer FAI [Figure 5].[27,28] MRI is used for an evaluation for chondral and labral lesion but standard MRI produces both false-positive results and an underestimation of labral pathology and has only 30% sensitivity and 36% accuracy whereas MRA produces better results, as the intra-articular or systemic infusion of gadolinium is required to obtain the detail necessary to study the labrum.[22,24,29] In addition, Radial MRI of single hip has been utilized to evaluate the labrum.[30-32] Radial imaging is performed by using a plane perpendicular to the acetabular rim, obtained from the oblique axial and coronal sequences. Slices in this plane are then obtained at a constant interval (usually 15° intervals) over 360° [Figure 5].
Figure 5.

(A) AP view of the right hip. The anterior (white dots) and posterior (black dots) rim of the acetabulum are marked. The superior portion of the anterior rim lies lateral to the posterior rim indicating overcoverage of the acetabulum. Anteriorly, it assumes a more normal medial position, creating the crossover sign as a positive indicator of pincer impingement. (B) Fat-suppressed oblique axial proton density weighted image shows linear high signal separating the anterior labrum roughly in halves, a radial tear.
Conservative treatment
Patients with a groin pain suspected to be a symptom of acetabular labral tear may initially receive a conservative treatment consisting of rest, non-steroidal anti-inflammatory medication, pain medications if necessary, modification of activities, physical therapy (PT) and intra-articular injection (IAI).[33] The pain may be reduced temporarily; however, the pain often recurs when the patient returns to his or her normal activities.[22] A 12-weeks PT protocol is noted to have good outcomes on 4 patients who experience decreased pain, increased strength, and improved function.[34] Aiming to improve the force-producing capacity and control of the muscles around the hip, the protocol is divided into 3 phases with emphasis on pain control, trunk stabilization, and movement correction in phase 1, muscle strengthening, recovery of normal ROM, and sense training in phase 2, progressing to participate in sports activity functionally in phase 3.[34]
As for IAI, the containment of injection usually includes an anesthetic agent and a corticosteroid, which acts as a role of diagnose as well as therapy. The positive response of anesthetic agents often helped to confirm that the labral tear was indeed the source of pain instead of other extra-articular pathologies such as psoas bursitis. The corticosteroid might have the ability of quieting the acute flare due to its anti-inflammatory effect. A study recently proposed provides the evidence to support the value of IAI. It shows that 85.7% of patients with labral pathology pre-arthroscopically respond positively to IAI (6 mL of 1% lidocaine, 6 mL of 0.25% bupivacaine, and 80 mg of triamcinolone) and at the same time more than half of the patients end up with immediate relief of pain after the injection (6 mL of 1% lidocaine, 6 mL of 0.25% bupivacaine, and 80 mg of triamcinolone).[35] Another research shows that 76.3% of the young athletes finally undergo surgical intervention after a non-operative treatment of PT, IAI, or both. However, the patients who have labral tear with FAI present a higher rate of surgery compared with those with isolated labral tear (51.3% vs. 25.0% with statistically significant difference), which indicates that that FAI comorbidity with hip labral tears increases the risk of surgery after non-operative management.[36]
Surgical treatment
Labral debridement
Labral debridement was the first documented procedure for labral tear. The torn part of labrum is debrided with the attempt to alleviate the patient's pain [Figure 6]. Short-term outcomes have turned out to be good to excellent in some researches with the advancement of hip arthroscopy.[37,38] However, compared with labral repair, excision of torn labrum accounts for an inferior outcome due to its loss of suction seal effect.[7,9,39] Thus, a recent study to identify the role of labral debridement states that, with narrow indication, selective debridement with labral preservation (SDLP) produced favorable outcomes comparable with a matched-pair labral repair group within a minimum 5-year follow-up. In this study, indications for SDLP includes stable labral base, at least 4 mm of the labral width, small focal tears with minimal intra-substance involvement and enough stable labral tissue preserved to maintain the suction-seal function.[40] In addition, Byrd and Jones[41] indicated that arthroscopic selective debridement can result in favorable long-term outcome supported by a 10-year follow-up in 50 patients who underwent selective labral debridement. Nonetheless, patients with pre-operative radiograph evidence of arthritis has been converted to THA in 7 of 8 patients totally, which implies that arthritis in the joint is a prognostic factor for poor outcomes. Under the circumstance of arthroscopic debridement for labral lesion secondary to dysplasia, patients frequently fail to relieve pain. In addition, because of the elimination of joint stability effect attributed to labrum, patients probably end up with detrimental clinical outcomes including progression of osteoarthritis and high reoperation rate.[42,43]
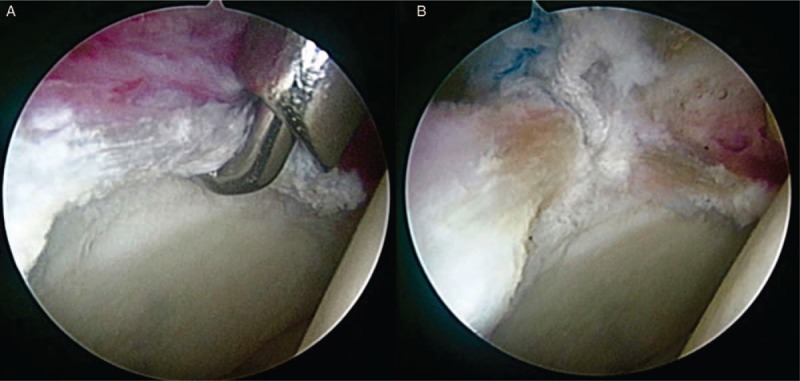
Figure 6.
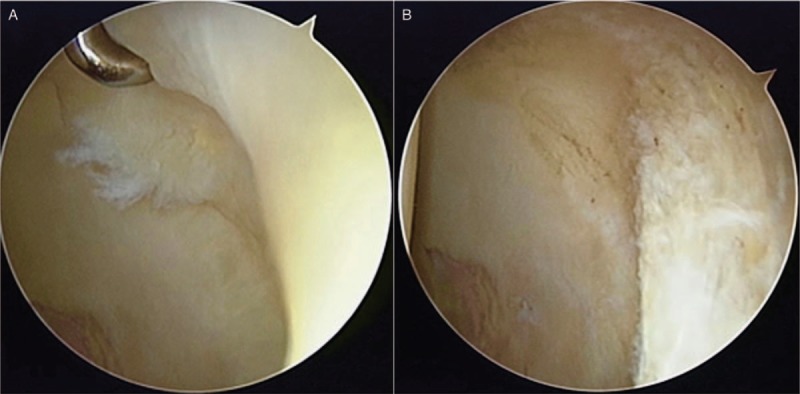
Arthroscopic view of a left hip from the anteriorolateral portal. (A) A fragmented labral tear with degeneration within its substance is identified. (B) The damaged portion has been removed, preserving the healthy substance of the labrum.
Labral repair
Since the role of labrum has been supported by evidence, resection of serious torn labrum may progress to a chondral lesion and premature arthritis and disrupt the role of labrum in proprioception associated with the mechanical pain. Conversely, preservation of labrum using labral refixation technique is increasingly becoming a more favorable option when it comes to decision making during the arthroscopy procedure when determine the fluid seal properties of the hip labrum under 5 conditions: (1) hip labrum intact, (2) labral tear, (3) labral repair with suture anchors, (4) partial labral resection, and (5) labral reconstruction using ipsilateral iliotibial band (ITB) autograft, conclusion is extracted that hip labral repair outperforms partial labral resection and reconstruction in preserving the joint fluid seal.[44] Similar research is introduced to characterize intra-articular fluid pressurization and hip stability to distraction forces in 6 labral conditions: intact, tear, repair, partial resection, reconstruction with ITB, and complete resection with conclusions that partial labral resection caused significant decreases in intra-articular fluid pressurization, the acetabular labrum was the primary hip stabilizer to distraction forces at small displacements and partial labral resection significantly decreased the distractive strength.[45] In an ovine model, labrum grossly healed 12 weeks after arthroscopic repair, which was a stable fibrovascular scar.[46]
With the development of instruments and techniques and the importance of the labrum being recognized, surgeons are increasingly interested in preserving as much as labrum as possible other than resection to restore its role as a gasket seal, assisting to stabilize the joint of hip and preventing an early degeneration of joint. Philippon et al[47] demonstrates that the labral repair is indicated if the labrum tissue is adequate (>7 mm) and the importance of pre-operative center-edge angle is emphasized to avoid over-resection while trimming the acetabular rim with the goal to just resect to the end of the rim chondrosis.[47] According to his previous study, the acetabular rim reduction was correlated with the pre-operative and post-operative center-edge angle presented by a formula that change in the center-edge angle = 1.8° + (0.65 × rim reduction in millimeters), thus the acetabular depth was measured intra-operatively prior to rim trimming and after rim trimming using a graduated intra-operative ruler.[48]
Commonly, looped repair is more suitable than labral base refixation when it comes to a small labrum (<5-mm width) because there is no sufficient tissue for penetration of the instrument. Conversely, the effect of the 2 techniques are likely the same given that both of them can restore the socket seal as for a medium to large labrum (more than 5-mm width). Nonetheless, there are still debates over the outcome of looped repair and labral base refixation. Looped repair deforms the triangular shape according to those in favor of pierced suture technique. On the contrary, opposite voices regarding labral base refixation claim that looped repair can not only maintain the suction seal of the labrum, but also avoid disrupting the substance of the labrum. In addition, the suture is so thin and might be able to be partially absorbed by labrum that the tension of pierced repair is suspected to preserve the triangular shape.[49] To find out whether difference exists between the 2 techniques, the outcome was measured by Hip outcome score-activities of daily living subscale (HOS-ADL), failure and revision rate in patients divided by 3 groups (looped, pierced, combined) in a mean 3-year follow-up, which shows no statistically significant difference among the groups.[50] Therefore, it may hint that suture type does not influence outcomes.
Even labral repair is increasingly preferable to preserve the suction seal, the labrum is unavoidably everted or inverted during the repair process despite every step being accurately administrated and the suture type (looped or pierced) on account that it is unable to separately adjust the suture limbs’ tension and labral position. Holding the purpose to obtain an optimal labral suction seal, an eversion-inversion labral repair is introduced. As is described in the study, for each anchor there are 2 suture passes in a mattress pattern with 1 penetrating the chondrolabral conjunction and the other entering through the actual labral tissue (usually the mid portion of the labrum) with the 2 suture-passing points aligned with the predrilled hole for the anchor placement. When the anchor is tapped in the hole, the suture is deliberately slackened to obtain controlled tensioning of labrum, which is the characteristic of this technique. After that the suture at the chondrolabral conjunction is tightened 1st to reattach the labral base to the bony rim followed by the suture located at the mid portion of labrum being tightened to control the eversion-inversion final position. The knotless anchor in this technique has the advantage of reducing the scar tissue formation and potential capsulolabral adhesions or iatrogenic chondral damage to the femoral head. Furthermore, the method is fine-tuning with 2 mattress-pattern sutures to evert or invert the larum in control thus creating a robust and optimal seal around the femoral head and restores normal anatomic function [Figure 7].[51]
Figure 7.
An anterior labral repair is performed in this left hip. (A) The tear is probed from the anteriorolateral portal. (B) One anchors have been placed with all two suture limbs passed through the labrum in a mattress pattern.
In a retrospective comparative study with a mean 3.5-year follow-up, Larson and Giveans concluded that the Harris hip score (HHS), 12-item short form survey (SF-12), and visual analogue score (VAS) pain scores were all significantly better for the refixation group compared with the debridement group meanwhile good to excellent results were noted in 68% of the focal excision/debridement group and 92% of the refixation group, which is consistent with their previous study in a minimum 1-year follow-up showing that HHSs were significantly better for the refixation group (94.3) compared with the debridement group (88.9) while good to excellent results were noted in 66.7% of the debridement group and 89.7% of the refixation group.[7,39] Krych et al[9] prospectively compared outcomes between labral repair and labral debridement with 1:1 match in 36 female patients totally. It turned out that the repair group outperformed the debridement group in HOS-ADL (mean, 91.2 in the repair group, mean, 80.9 in the debridement group) and HOS-SSS scores (mean, 88.7 in the repair group, mean, 76.3 in the debridement group).[9] However, with regard to long-term outcome, Menge et al[52] demonstrated that data prospectively collected in 145 patients divided into 2 groups (repair and debridement) showed no significant difference in HOS-ADL and conversion rate of THA in a minimum 10-year follow-up. In this study, increased age, a joint space of ≤2 mm and acetabular microfracture were independently associated with an increased hazard rate for THA.
Labral reconstruction
In spite of the fact that labral repair is proved to have the ability of recreating the optimal nature of labrum and its biomechanics, in case where labral damage is hard to be repaired or a previously debrided labrum is deemed irreparable because of insufficient amount, reconstruction either in open surgery or under arthroscopy is indicated with an autograft or allograft being incised to replace the torn labrum [Figure 8].
Figure 8.

(A) Preoperative MRI reveals a labral tear with formation of paralabral cyst. (B) Intraoperative photograph after complete labral reconstruction with iliotibial band autograft. (C) AP pelvis radiograph after surgery with no evidence of radiograph arthrosis.
As first introduced by Ganz, surgical dislocation technique is proved to be able to give a full direct 360° view of acetabulum and labrum without the risk of disrupting the femoral head perfusion.[53] Taking advantage of this approach, surgeon can easily probe the hip joint and find out the location of labral lesion. Following that is circumferential or local labral reconstruction using anchors which are placed into the acetabular rim and suture passing through the base of labrum and being tied firmly to have labrum seated against the acetabular bone.
As for labral reconstruction arthroscopically, it is much more difficult to process compared with open surgery. There are several kinds of autograft being used to achieve the procedure including the ITB, the ligamentum teres capitis, and the gracilis tendon.[54] In contrast to the traditional open harvest of the ITB, Deshmane et al[55] reported an all-arthroscopic harvest labral reconstruction including the graft harvest and reconstruction portion, which is said to be potentially superior to the open procedure in reducing scarring tissue, bodily disfigurement, infection, and post-operative pain because of minimal invasiveness of the technique. Another article introduces a technique using a tensor fascia lata or ITB allograft and knotless suture anchors, claiming that it is advanced in easy tension adjustment and labral manipulation.[56] There is a report demonstrating that use the indirect head of rectus femoris as a local graft for the advantages of requiring less portals as rectus femoris is close to the anterosuperior acetabulum and eliminating the need for “back table work” and possibility of donor-site morbidity as the harvest and prepare work on graft are done through the same portal. In addition, the blood supply of the graft is retained to increase tissue viability.[57] Except for autograft inserted into the hip joint, ITB allograft tissue and a front-to-back approach is reported by White et al[58] who state that the allograft is chosen for the following reasons: (1) Allograft tissue gives an opportunity to create a more uniform, consistent graft because the most ideal section of the tissue can be used; (2) Length of the graft will not be limited in contrast to the autograft harvest from the host tissue; (3) Allograft tissue is more workable in the joint and less prone to swelling and fraying than tendinous grafts. In addition, the front-to-back technique permits the surgeon to excess graft after front-to-back fixation thus make a perfect match between the graft length and the labral defect.
To our knowledge, the conversion rate of THA after labral reconstruction ranges from 0% to 25% despite the superior post-operative outcome reported in various research.[10,11,59-66] With a minimum 1-year follow-up, Philippon et al[10] reported 4 of 47 patients had been converted to THA, 3 of those had a joint space of <2 mm thus indicated that joint space of <2 mm may be a risk factor for an inferior outcome for labral reconstruction. Similar studies were published to support this statement.[61,62] However, a recent research by White et al[65] showed that 13 of 131 hips undergoing labral reconstruction progressed to arthritis requiring THA without pre-operative joint space of <2 mm and Tönnis grade ≥2. Other studies have also indicated the similar outcome in patients showing Tönnis grade 0 or 1 in pre-operative radiograph.[60,64] This may raise the controversy over whether labral reconstruction can restore the suction seal effect which is of great importance to maintain the negative pressure within the joint and avoid direct contact between the cartilage surface of acetabulum and femoral head thus preventing a premature articular wear. In addition, long-term study is needed to ensure the role of labral reconstruction.
Summary
The acetabular labrum plays an important role in preventing a healthy hip from premature arthritis. The preservation of the hydraulic seal effect of labrum is closely associated with satisfactory clinical outcomes no matter what kind of surgical treatment is performed. With regard to irreparable labral lesions, debridement of the damaged labrum is obviously not a preferable option while the role of labral reconstruction remains uncertain due to a lack of long-term results. Thus further researches are supposed to focus on finding out an effective as well as cost-effective method for irreparable labral tear of acetabulum.
Conflicts of interest
None.
Footnotes
How to cite this article: Su T, Chen GX, Yang L. Diagnosis and treatment of labral tear. Chin Med J 2019;00:00–00. doi: 10.1097/CM9.0000000000000020
References
- 1.Dameron TB., Jr Bucket-handle tear of acetabular labrum accompanying posterior dislocation of the hip. J Bone Joint Surg Am 1959;41-A:131–134. [PubMed] [Google Scholar]
- 2.Suzuki S, Awaya G, Okada Y, Maekawa M, Ikeda T, Tada H. Arthroscopic diagnosis of ruptured acetabular labrum. Acta Orthop Scand 1986;57:513–515. [DOI] [PubMed] [Google Scholar]
- 3.Robertson WJ, Kadrmas WR, Kelly BT. Arthroscopic management of labral tears in the hip: a systematic review of the literature. Clin Orthop Relat Res 2007;455:88–92. doi: 10.1097/BLO.0b013e31802c7e0f. [DOI] [PubMed] [Google Scholar]
- 4.Wenger D, Kendell K, Miner M, Trousdale RT. Acetabular labral tears rarely occur in the absence of bony abnormalities. Clin Orthop Relat Res 2004;426:145–150. [DOI] [PubMed] [Google Scholar]
- 5.Tanzer M, Noiseux N. Osseous abnormalities and early osteoarthritis: the role of hip impingement. Clin Orthop Relat Res 2004;429:170–177. [PubMed] [Google Scholar]
- 6.Kim K, Hwang D, Lee C, Kwon ST. Influence of femoroacetabular impingement on results of hip arthroscopy in patients with early osteoarthritis. Clin Orthop Relat Res 2007;456:128–132. doi: 10.1097/01.blo.0000246542.49574.2c. [DOI] [PubMed] [Google Scholar]
- 7.Larson CM, Giveans MR, Stone RM. Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement: mean 3.5-year follow-up. Am J Sports Med 2012;40:1015–1021. doi: 10.1177/0363546511434578. [DOI] [PubMed] [Google Scholar]
- 8.Philippon M, Briggs K, Yen Y, Kuppersmith DA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: minimum two-year follow-up. J Bone Joint Surg Br 2009;91:16–23. doi: 10.1302/0301-620X.91B1.21329. [DOI] [PubMed] [Google Scholar]
- 9.Krych A, Thompson M, Knutson Z, Scoon J, Coleman SH. Arthroscopic labral repair versus selective labral debridement in female patients with femoroacetabular impingement: a prospective randomized study. Arthroscopy 2013;29:46–53. doi: 10.1016/j.arthro.2012.07.011. [DOI] [PubMed] [Google Scholar]
- 10.Philippon M, Briggs K, Hay C, Kuppersmith DA, Dewing CB, Huang MJ. Arthroscopic labral reconstruction in the hip using iliotibial band autograft: technique and early outcomes. Arthroscopy 2010;26:750–756. doi: 10.1016/j.arthro.2009.10.016. [DOI] [PubMed] [Google Scholar]
- 11.Domb B, El Bitar Y, Stake C, Trenga AP, Jackson TJ, Lindner D. Arthroscopic labral reconstruction is superior to segmental resection for irreparable labral tears in the hip: a matched-pair controlled study with minimum 2-year follow-up. Am J Sports Med 2014;42:122–130. doi: 10.1177/0363546513508256. [DOI] [PubMed] [Google Scholar]
- 12.Bharam S. Labral tears, extra-articular injuries, and hip arthroscopy in the athlete. Clin Sports Med 2006;25:279–292. doi: 10.1016/j.csm.2006.01.003. [DOI] [PubMed] [Google Scholar]
- 13.Seldes RM, Tan V, Hunt J, Katz M, Winiarsky R, Fitzgerald RHJr. Anatomy, histologic features, and vascularity of the adult acetabular labrum. Clin Orthop Relat Res 2001;382:232–240. [DOI] [PubMed] [Google Scholar]
- 14.Kim Y, Azuma H. The nerve endings of the acetabular labrum. Clin Orthop Relat Res 1995;320:176–181. [PubMed] [Google Scholar]
- 15.Petersen W, Petersen F, Tillmann B. Structure and vascularization of the acetabular labrum with regard to the pathogenesis and healing of labral lesions. Arch Orthop Trauma Surg 2003;123:283–288. doi: 10.1007/s00402-003-0527-7. [DOI] [PubMed] [Google Scholar]
- 16.Kelly BT, Shapiro GS, Digiovanni CW, Buly RL, Potter HG, Hannafin JA. Vascularity of the hip labrum: a cadaveric investigation. Arthroscopy 2005;21:3–11. doi: 10.1016/j.arthro.2004.09.016. [DOI] [PubMed] [Google Scholar]
- 17.Kalhor M, Horowitz K, Beck M, Nazparvar B, Ganz R. Vascular supply to the acetabular labrum. J Bone Joint Surg Am 2010;92:2570–2575. doi: 10.2106/JBJS.I.01719. [DOI] [PubMed] [Google Scholar]
- 18.Grant AD, Sala DA, Davidovitch RI. The labrum: structure, function, and injury with femoro-acetabular impingement. J Child Orthop 2012;6:357–372. doi: 10.1007/s11832-012-0431-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kelly B, Weiland D, Schenker M, Philippon MJ. Arthroscopic labral repair in the hip: surgical technique and review of the literature. Arthroscopy 2005;21:1496–1504. doi: 10.1016/j.arthro.2005.08.013. [DOI] [PubMed] [Google Scholar]
- 20.Philippon M, Stubbs A, Schenker ML, Maxwell RB, Ganz R, Leunig M. Arthroscopic management of femoroacetabular impingement: osteoplasty technique and literature review. Am J Sports Med 2007;35:1571–1580. doi: 10.1177/0363546507300258. [DOI] [PubMed] [Google Scholar]
- 21.Ito K, Leunig M, Ganz R. Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res 2004;429:262–271. [DOI] [PubMed] [Google Scholar]
- 22.Lewis C, Sahrmann S. Acetabular labral tears. Phys Ther 2006;86:110–121. [DOI] [PubMed] [Google Scholar]
- 23.Klaue K, Durnin C, Ganz R. The acetabular rim syndrome. A clinical presentation of dysplasia of the hip. J Bone Joint Surg Br 1991;73:423–429. [DOI] [PubMed] [Google Scholar]
- 24.Hunt D, Clohisy J, Prather H. Acetabular labral tears of the hip in women. Phys Med Rehabil Clin N Am 2007;18:497–520. doi: 10.1016/j.pmr.2007.05.007. [DOI] [PubMed] [Google Scholar]
- 25.Narvani A, Tsiridis E, Kendall S, Chaudhuri R, Thomas P. A preliminary report on prevalence of acetabular labrum tears in sports patients with groin pain. Knee Surg Sports Traumatol Arthrosc 2003;11:403–408. doi: 10.1007/s00167-003-0390-7. [DOI] [PubMed] [Google Scholar]
- 26.Burnett R, Della Rocca G, Prather H, Curry M, Maloney WJ, Clohisy JC. Clinical presentation of patients with tears of the acetabular labrum. J Bone Joint Surg Am 2006;88:1448–1457. doi: 10.2106/JBJS.D.02806. [DOI] [PubMed] [Google Scholar]
- 27.Eijer H, Myers S, Ganz R. Anterior femoroacetabular impingement after femoral neck fractures. J Orthop Trauma 2001;15:475–481. [DOI] [PubMed] [Google Scholar]
- 28.Garbuz D, Masri B, Haddad F, Duncan CP. Clinical and radiographic assessment of the young adult with symptomatic hip dysplasia. Clin Orthop Relat Res 2004;418:18–22. [DOI] [PubMed] [Google Scholar]
- 29.Czerny C, Hofmann S, Neuhold A, Tschauner C, Engel A, Recht MP, et al. Lesions of the acetabular labrum: accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225–230. doi: 10.1148/radiology.200.1.8657916. [DOI] [PubMed] [Google Scholar]
- 30.Kubo T, Horii M, Harada Y, Noguchi Y, Yutani Y, Ohashi H, et al. Radial-sequence magnetic resonance imaging in evaluation of acetabular labrum. J Orthop Sci 1999;4:328–332. [DOI] [PubMed] [Google Scholar]
- 31.Kubo T, Horii M, Yamaguchi J, Inoue S, Fujioka M, Ueshima K, et al. Acetabular labrum in hip dysplasia evaluated by radial magnetic resonance imaging. J Rheumatol 2000;27:1955–1960. [PubMed] [Google Scholar]
- 32.Ueshima K, Takahashi KA, Fujioka M, Arai Y, Horii M, Asano T, et al. Relationship between acetabular labrum evaluation by using radial magnetic resonance imaging and progressive joint space narrowing in mild hip dysplasia. Magn Reson Imaging 2006;24:645–650. doi: 10.1016/j.mri.2005.12.009. [DOI] [PubMed] [Google Scholar]
- 33.Groh M, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med 2009;2:105–117. doi: 10.1007/s12178-009-9052-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Yazbek PM, Ovanessian V, Martin RL, Fukuda TY. Nonsurgical treatment of acetabular labrum tears: a case series. J Orthop Sports Phys Ther 2011;41:346–353. doi: 10.2519/jospt.2011.3225. [DOI] [PubMed] [Google Scholar]
- 35.Kivlan B, Martin R, Sekiya J. Response to diagnostic injection in patients with femoroacetabular impingement, labral tears, chondral lesions, and extra-articular pathology. Arthroscopy 2011;27:619–627. doi: 10.1016/j.arthro.2010.12.009. [DOI] [PubMed] [Google Scholar]
- 36.Cianci A, Sugimoto D, Stracciolini A, Yen YM, Kocher MS, d’Hemecourt PA. Nonoperative management of labral tears of the hip in adolescent athletes: description of sports participation, interventions, comorbidity, and outcomes. Clin J Sport Med 2019;29:24–28. doi: 10.1097/JSM.0000000000000503. [DOI] [PubMed] [Google Scholar]
- 37.Byrd J, Jones K. Prospective analysis of hip arthroscopy with 2-year follow-up. Arthroscopy 2000;16:578–587. doi: 10.1053/jars.2000.7683. [DOI] [PubMed] [Google Scholar]
- 38.O’leary J, Berend K, Vail T. The relationship between diagnosis and outcome in arthroscopy of the hip. Arthroscopy 2001;17:181–188. doi: 10.1053/jars.2001.21481. [DOI] [PubMed] [Google Scholar]
- 39.Larson C, Giveans M. Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement. Arthroscopy 2009;25:369–376. doi: 10.1016/j.arthro.2008.12.014. [DOI] [PubMed] [Google Scholar]
- 40.Chen A, Yuen L, Ortiz-Declet V, Litrenta J, Maldonado DR, Domb BG. Selective debridement with labral preservation using narrow indications in the hip: minimum 5-year outcomes with a matched-pair labral repair control group. Am J Sports Med 2018;46:297–304. doi: 10.1177/0363546517739566. [DOI] [PubMed] [Google Scholar]
- 41.Byrd J, Jones K. Prospective analysis of hip arthroscopy with 10-year followup. Clin Orthop Relat Res 2010;468:741–746. doi: 10.1007/s11999-009-0841-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Parvizi J, Bican O, Bender B, Mortazavi SM, Purtill JJ, Erickson J, et al. Arthroscopy for labral tears in patients with developmental dysplasia of the hip: a cautionary note. J Arthroplasty 2009;24:110–113. doi: 10.1016/j.arth.2009.05.021. [DOI] [PubMed] [Google Scholar]
- 43.Kalore N, Jiranek W. Save the torn labrum in hips with borderline acetabular coverage. Clin Orthop Relat Res 2012;470:3406–3413. doi: 10.1007/s11999-012-2499-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Philippon M, Nepple J, Campbell K, Dornan GJ, Jansson KS, LaPrade RF, et al. The hip fluid seal--Part I: the effect of an acetabular labral tear, repair, resection, and reconstruction on hip fluid pressurization. Knee Surg Sports Traumatol Arthrosc 2014;22:722–729. doi: 10.1007/s00167-014-2874-z. [DOI] [PubMed] [Google Scholar]
- 45.Nepple J, Philippon M, Campbell K, Dornan GJ, Jansson KS, LaPrade RF, et al. The hip fluid seal--Part II: the effect of an acetabular labral tear, repair, resection, and reconstruction on hip stability to distraction. Knee Surg Sports Traumatol Arthrosc 2014;22:730–736. doi: 10.1007/s00167-014-2875-y. [DOI] [PubMed] [Google Scholar]
- 46.Philippon M, Arnoczky S, Torrie A. Arthroscopic repair of the acetabular labrum: a histologic assessment of healing in an ovine model. Arthroscopy 2007;23:376–380. doi: 10.1016/j.arthro.2007.01.017. [DOI] [PubMed] [Google Scholar]
- 47.Philippon M, Faucet S, Briggs K. Arthroscopic hip labral repair. Arthrosc Tech 2013;2:e73–e76. doi: 10.1016/j.eats.2012.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Philippon M, Wolff A, Briggs KK, Zehms CT, Kuppersmith DA. Acetabular rim reduction for the treatment of femoroacetabular impingement correlates with preoperative and postoperative center-edge angle. Arthroscopy 2010;26:757–761. doi: 10.1016/j.arthro.2009.11.003. [DOI] [PubMed] [Google Scholar]
- 49.Domb B, Hartigan D, Perets I. Decision making for labral treatment in the hip: repair versus débridement versus reconstruction. J Am Acad Orthop Surg 2017;25:e53–e62. doi: 10.5435/JAAOS-D-16-00144. [DOI] [PubMed] [Google Scholar]
- 50.Sawyer G, Briggs K, Dornan G, Ommen ND, Philippon MJ. Clinical outcomes after arthroscopic hip labral repair using looped versus pierced suture techniques. Am J Sports Med 2015;43:1683–1688. doi: 10.1177/0363546515581469. [DOI] [PubMed] [Google Scholar]
- 51.Moreira B, Pascual-Garrido C, Chadayamurri V, Mei-Dan O. Eversion-inversion labral repair and reconstruction technique for optimal suction seal. Arthrosc Tech 2015;4:e697–e700. doi: 10.1016/j.eats.2015.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Menge T, Briggs K, Dornan G, McNamara SC, Philippon MJ. Survivorship and outcomes 10 years following hip arthroscopy for femoroacetabular impingement: labral debridement compared with labral repair. J Bone Joint Surg Am 2017;99:997–1004. doi: 10.2106/JBJS.16.01060. [DOI] [PubMed] [Google Scholar]
- 53.Ganz R, Gill T, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119–1124. [DOI] [PubMed] [Google Scholar]
- 54.Ayeni O, Alradwan H, de Sa D, Philippon MJ. The hip labrum reconstruction: indications and outcomes--a systematic review. Knee Surg Sports Traumatol Arthrosc 2014;22:737–743. doi: 10.1007/s00167-013-2804-5. [DOI] [PubMed] [Google Scholar]
- 55.Deshmane P, Kahlenberg C, Patel R, et al. All-arthroscopic iliotibial band autograft harvesting and labral reconstruction technique. Arthrosc Tech 2013;2:e15–e19. doi: 10.1016/j.eats.2012.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.McConkey M, Moreira B, Mei-Dan O. Arthroscopic Hip Labral Reconstruction and Augmentation Using Knotless Anchors. Arthrosc Tech 2015;4:e701–e705. doi: 10.1016/j.eats.2015.07.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Sharfman Z, Amar E, Sampson T, et al. Arthroscopic Labrum Reconstruction in the Hip Using the Indirect Head of Rectus Femoris as a Local Graft: Surgical Technique. Arthrosc Tech 2016;5:e361–e364. doi: 10.1016/j.eats.2016.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.White B, Herzog M. Arthroscopic labral reconstruction of the hip using iliotibial band allograft and front-to-back fixation technique. Arthrosc Tech 2016;5:e89–e97. doi: 10.1016/j.eats.2015.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Sierra R, Trousdale R. Labral reconstruction using the ligamentum teres capitis: report of a new technique. Clin Orthop Relat Res 2009;467:753–759. doi: 10.1007/s11999-008-0633-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Walker J, Pagnotto M, Trousdale RT, Sierra RJ. Preliminary pain and function after labral reconstruction during femoroacetabular impingement surgery. Clin Orthop Relat Res 2012;470:3414–3420. doi: 10.1007/s11999-012-2506-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Boykin R, Patterson D, Briggs KK, Dee A, Philippon MJ. Results of arthroscopic labral reconstruction of the hip in elite athletes. Am J Sports Med 2013;41:2296–2301. doi: 10.1177/0363546513498058. [DOI] [PubMed] [Google Scholar]
- 62.Geyer M, Philippon M, Fagrelius TS, Briggs KK. Acetabular labral reconstruction with an iliotibial band autograft: outcome and survivorship analysis at minimum 3-year follow-up. Am J Sports Med 2013;41:1750–1756. doi: 10.1177/0363546513487311. [DOI] [PubMed] [Google Scholar]
- 63.Matsuda D, Burchette R. Arthroscopic hip labral reconstruction with a gracilis autograft versus labral refixation: 2-year minimum outcomes. Am J Sports Med 2013;41:980–987. doi: 10.1177/0363546513482884. [DOI] [PubMed] [Google Scholar]
- 64.Camenzind R, Steurer-Dober I, Beck M. Clinical and radiographical results of labral reconstruction. J Hip Preserv Surg 2015;2:401–409. doi: 10.1093/jhps/hnv062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.White B, Stapleford A, Hawkes TK, Finger MJ, Herzog MM. Allograft use in arthroscopic labral reconstruction of the hip with front-to-back fixation technique: minimum 2-year follow-up. Arthroscopy 2016;32:26–32. doi: 10.1016/j.arthro.2015.07.016. [DOI] [PubMed] [Google Scholar]
- 66.Amar E, Sampson T, Sharfman ZT, Caplan A, Rippel N, Atzmon R, et al. Acetabular labral reconstruction using the indirect head of the rectus femoris tendon significantly improves patient reported outcomes. Knee Surg Sports Traumatol Arthrosc 2018;26:2512–2518. doi: 10.1007/s00167-017-4641-4. [DOI] [PubMed] [Google Scholar]