

Abstract
Introduction:
GTs are rare, benign tumors, developing from a neuro-myo-arterial structure. Their typical location is in the hand, but they may develop anywhere else. Extra-digital glumus tumors GTs, like the location in the thigh, are rare and much more difficult to diagnose. They are usually misdiagnosed and unproperly treated, due to the absence of the typical symptoms.
Case Report:
We report a case of a GT of the thigh in a 25-year-old female, presenting with a painful mass on the posterior side of her left thigh, evolving for 15 months. She was suffering from pain and hyperesthesia of the underlying skin exacerbated by movements. The patient was successfully treated by excisional biopsy.
Conclusion:
Gts of the thigh represent an exceptional location of extra-digital Gts, very rare themselves. Pain, hypersensitivity to cold, and severe amyotrophy should raise suspicion for Gts. Through this case we discuss the diagnostic difficulties and the treatment of extra-digital Gts.
Keywords: Glomus tumor, lower limb, thigh
Learning Point of the Article:
Pain, hypersensitivity to cold, and severe amyotrophy should raise suspicion for glomus tumors regardless of its location.
Introduction
Glomus tumors (GTs) are rare, benign tumors arising from neuro-myo-arterial glomus bodies, accounting for <2% of soft tissue tumors [1], and a malignant transformation of this tumor with metastasis is possible but remains exceptional [2]. Typically, GT occurs in the hand and are relatively easily diagnosed following the classic triad of pain, tenderness, and hypersensitivity to cold. Howevr, they may develop anywhere, and extradigital GT, like the location in the thigh, is much more difficult to diagnose. They are usually misdiagnosed and unproperly treated, due to the absence of the typical symptoms. We report an exceptional case of extradigital GT causing thigh pain.
Case Report
A 25-year-old female without any significant pathological history, presented with a painful mass on the posterior side of her left thigh, with no history of trauma or septic inoculation, evolving for 15 months. She was suffering from pain and hyperesthesia of the underlying skin exacerbated by movements. The mass gradually increased in size becoming uncomfortable at rest. Physical examination revealed a soft immobile mass with tenderness to palpation and a normal overlying skin without inflammatory signs. Amyotrophy of the muscles of the tight was obvious compared to the opposite side. The left hip and knee range of motion were within normal limits. Ultrasonography showed a fluid mass consisting with an hydatid cyst of the soft tissue of the thigh. Magnetic resonance imaging (MRI) showed a rounded formation well-demarcated, developed in the biceps femoris muscle, measuring 3 cm × 2 cm × 2 cm with high signal intensity on T2-weighted images, low signal intensity on T1-weighted images, and having a liquid-liquid level. This lesion is regularly enhanced on the edge, consisting with an abscess of the biceps femoris muscle (Fig. 1a and b). Facing diagnosis difficulties, an excisional biopsy was performed. The histological study of the resected mass revealed a GT without malignant features and with negative margins (Fig. 2a, Fig. 2b, c). Postoperatively, the patient was immediately relieved from pain, and she has been pain free for the last year.
Figure 1.
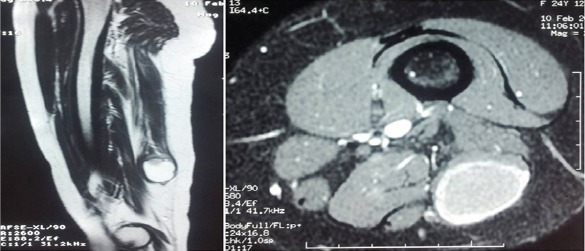
Magnetic resonance imaging of the left thigh. (a) Sagittal view showing a rounded formation, well limited, developed in the biceps femoris muscle, measuring 3 cm × 2 cm× 2 cm with high signal intensity on the T2-weighted image. (b) Axial view showing low signal intensity, enhancing with injection of gadolinium on the T1-weighted image, especially on the edge.
Figure 2.
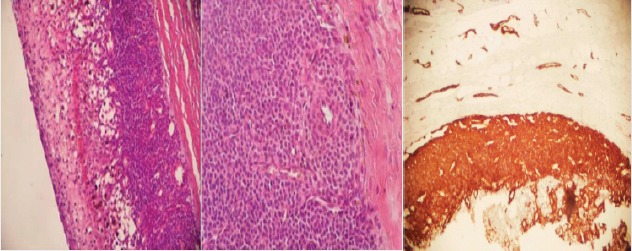
(a) Cystic glomus tumor with a solid pattern (Hematoxylin and eosin stain ×100). (b) Round and ovoid glomuscells surrounding a small vascular channel (Hematoxylin and eosin stain ×400). (c) Immunohistochemistry showing tumor cells strongly positive for smooth muscle actin (×100).
Discussion
Gts are hamartomas developing from a neuro-myo-arterial structure at the level of the dermo-hypodermic junction: The glomus body. Glomus bodies are arteriovenous anastomoses found throughout the body. Their function is to regulate the local skin blood flow, and they play an important role in thermoregulation [1]. The first case of GT was reported by Wood [3] in 1812 under the name of “painful subcutaneous tubercle.” GT is very rare and represent 2% of soft tissue tumors, typically located in the hand. Extra digital locations are even rarer, the location in the thigh is exceptional, and only a few cases were reported in the literature. Schiefer [2] reported five cases of GT located in the thigh on 56 cases of extradigital GT, and Luis et al. [4] reported only one case of GT located in the thigh on 29 cases of GT located in the lower limb. Typical GT of the hand is easily diagnosed following the classic triad of pain, tenderness, and hypersensitivity to cold. Extradigital GT, and especially when located in thigh, is much more difficult to diagnose and is usually misdiagnosed and unproperly treated, due to the absence of the specific symptoms, the frequent small size of the tumor, and its deep location. Lee et al. [5] reported a study comparing 42 patients with extradigital GT and 110 patients with digital GT, and the incidence of pain and sensitivity to cold were significantly lower in extradigital GT, with no significant difference in the incidence of tenderness between extradigital and digital GT. Our patient was suffering from pain and hyperesthesia of the underlying skin exacerbated by movement and severe amyotrophy of the muscles of the tight without hypersensitivity to cold. Based on interrogation and physical examination, it is difficult to suspect a GT at this stage. Several diagnostic methods such as MRI and ultrasonography have been suggested to assist in rapid and accurate diagnosis. Ultrasonography is a useful tool in the diagnosis of extradigital GT, it is not expensive, and it is easily available, but ultrasonographic findings (hypoechoic rounded well-demarcated mass) compared to other cystic lesions are not specific. Pain, hypersensitivity to cold, and severe amyotrophy should raise suspicion for GT, and it should be included in the differential diagnosis of cystic lesions. MRI is probably the most sensitive imaging tool for diagnosing extradigital GT. The typical appearance of a GT on MRI is a high signal intensity on T2-weighted images and low signal intensity on T1-weighted images enhancing with injection of gadolinium, especially on the edge. Complete excisional biopsy remains the best way leading to a final diagnosis after histological study. It is an effective treatment providing good results (immediate relief from pain) like in our case. Some authors recommend pre-operative angiography to delineate tumor extension, and others use of a microscope to ensure complete excision. Sclerotherapy and electron beam irradiation have been used alternatively to obliterate these tumors[4]. Recurrence after surgical treatment is rare but could be related to multiple GTs.
Conclusion
GT of the thigh represents an exceptional location of extradigital GT, very rare themselves. Pain, hypersensitivity to cold, and severe amyotrophy should raise suspicion for GT. They are usually difficult to diagnose with a significant delay. MRI allows a reliable diagnostic approach; however, confirmation requires histological study after surgical biopsy. Complete resection allows immediate relief of pain, but recurrence remains possible.
Clinical Message.
Gts are rare vascular tumors. The usual presentation is a solitary nodule in the distal portion of a finger, but they can also occur everywhere. Pain, hypersensitivity to cold, and severe amyotrophy should raise suspicion for GTs. Their diagnosis is histological. However, modern imaging tools, including high-resolution MRI, allow a reliable diagnostic approach.
Biography

Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that Informed consent of the patient is taken for publication of this case report
References
- 1.Gombos Z, Zhang PJ. Glomus tumor. Arch Pathol Lab Med. 2008;132:1448–52. doi: 10.5858/2008-132-1448-GT. [DOI] [PubMed] [Google Scholar]
- 2.Schiefer TK, Parker WL, Anakwenze OA, Amadio PC, Inwards CY, Spinner RJ, et al. Extradigital glomus tumors:A 20-year experience. Mayo Clin Proc. 2006;81:1337–44. doi: 10.4065/81.10.1337. [DOI] [PubMed] [Google Scholar]
- 3.Wood W. On painful subcutaneous tubercle. Edinburgh Med J. 1812;8:283–91. [PMC free article] [PubMed] [Google Scholar]
- 4.Luis LR, Jr, Kaoru GR, Shemuel PB, Mills JL., Sr Lower extremity glomus tumors:Comprehensive review for surgeons. Vascular. 2008;16:326–32. doi: 10.2310/6670.2008.00064. [DOI] [PubMed] [Google Scholar]
- 5.Lee DW, Yang JH, Chang S, Won CH, Lee MW, Choi JH, et al. Clinical and pathological characteristics of extradigital and digital glomus tumours:A retrospective comparative study. J Eur Acad Dermatol Venereol. 2011;25:1392–7. doi: 10.1111/j.1468-3083.2011.03979.x. [DOI] [PubMed] [Google Scholar]