

Abstract
Introduction:
Bilateral anterior column acetabulum fractures in literature have been reported due to osteoporosis and seizure disorders. Very few cases have been reported after road traffic accident (RTA) and that too in a young patient without osteoporosis. We present a similar case in a young patient following a high-velocity injury managed with open reduction and internal fixation (ORIF).
Case Report:
A 28-year-old male presented with bilateral anterior column acetabulum fracture following RTA. The patient was initially admitted to emergency and stabilized hemodynamically. He was operated later with ORIF on both sides using ilioinguinal approach. At 1-year follow-up, the patient is able to walk, squat, and do routine activities without pain and fracture healed uneventfully.
Discussion:
Acetabulum fractures are known for their complex nature and difficulty in management. We have seen this challenging case of bilateral anterior column acetabulum fracture following RTA, which has not been reported earlier and managed with open reduction and internal fixation with excellent results.
Conclusion:
This is among the few reported cases of bilateral anterior column acetabulum fracture due to high-velocity injury following RTA. The pattern of injury clarifies the complexity of acetabular fractures and challenges associated with treating these injuries. Such injuries will be more common in future due to increasing incidence of high-velocity trauma.
Keywords: Bilateral acetabulum fracture, bilateral anterior column, acetabulum
Learning Point of the Article:
Complex injuries like this will be seen more frequently in future with rising incidence of high velocity injuries.
Introduction
Bilateral anterior column acetabulum fracture without any associated injury is very rare. Bilateral displaced acetabulum fractures have been reported earlier, but most of the cases in the literature are due to low-velocity injuries following seizures or severe osteoporosis [1, 2, 3, 4,5]. We have seen bilateral anterior column acetabulum fracture due to high-velocity injury following road traffic accident (RTA) in a young patient. These fractures are quite challenging in terms of complexity and treatment options. A similar case of bilateral anterior column acetabulum fracture with multiple other fractures has been reported earlier and managed using percutaneous screw fixation as the fracture was minimally displaced [6]. In our case, the patient is young with displaced fracture on both sides without any associated injury requiring open reduction and internal fixation (ORIF).
Case Report
A 28-year-old male presented to the emergency department following high-velocity RTA with severe pain in both hips and inability to stand and walk. He was stabilized hemodynamically and evaluated with radiographs of pelvis anteroposterior and spine, and found to have bilateral anterior column acetabulum fracture (Fig. 1). The patient was shifted to ward and further investigations were done in the form of Judet views for both hips and three-dimensional reconstruction computed tomography (Fig. 2 and 3) for definitive management. He was diagnosed with bilateral displaced anterior column acetabulum fracture requiring ORIF. The patient was operated in two sittings using ilioinguinal approach on both sides for ORIF with plating. Routine antibiotic and deep vein thrombosis prophylaxis along with indomethacin were given for heterotopic ossification. Procedure was uneventful, andthe patient did well postoperatively. Post-operative radiographs were done showing anatomical reduction with congruent joints (Fig. 4), following which physiotherapy was started for hip, knee, and ankle joints. Initial 6 weeks, the patient was kept non-weight-bearing and radiographs at the end of 6 weeks were good both for reduction and healing. Partial weight-bearing as tolerated with walking aid and muscle strengthening exercises for both hips started. At 3-month follow-up, radiographs revealed sign of union and the patient was allowed full weight-bearing and all routine activities as tolerated (Fig. 5). At 1-year follow-up, radiographs were done and fracture on both sides was well consolidated, and the patient is pain free, walking without any limp, no restriction of movements, and able to squat and sit crossed leg without any complications (Fig. 6).
Figure 1.

Anteroposteriorradiograph of pelvis showing bilateral displaced acetabulum fracture.
Figure 2.

(a and b) Judet obturator view radiograph of both hips showing displaced anterior column acetabulum fracture.
Figure 3.
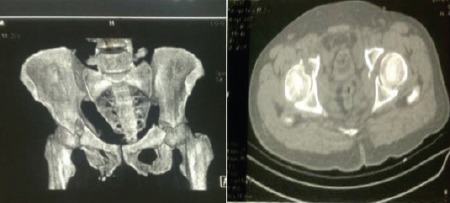
(a and b) Three-dimensionalreconstruction computed tomography images showing bilateral displaced anterior column acetabulum fracture
Figure 4.

(a, b, c) Post-operative pelvis anteroposterior and Judet view radiographs showing anatomical and congruent reduction of both fractures.
Figure 5.

A 1-year follow-up pelvis anteroposterior radiograph showing consolidation of fracture with anatomical reduction and congruent joints on both sides.
Figure 6.

Clinical images of the patient showing squatting and sitting crossed leg position without any problem.
Discussion
A displaced bilateral anterior column acetabular fracture following RTA in a young patient without any associated injury is very rare. All the existing reports of the bilateral acetabular fractures in the literature are following low-energy injuries resulting after epileptic seizures or in severely osteoporotic patients [1, 2, 3, 4, 5, 6]. Gupta et al. reported a case of high-energy traumatic injury causing displaced bilateral acetabular fractures which was associated with an open book injury of the pelvis and sacral fracture [7]. Vaishya et al. reported a case of bilateral anterior column fracture in a polytrauma patient which was minimally displaced and managed with percutaneous screw fixation. These injuries are challenging in terms of immediate as well as definitive management. Incidence of bilateral acetabulum fractures is increasing with the rise in high-velocity injuries. We report a case of high-velocity RTA with bilateral displaced anterior column acetabulum fracture without any associated injury managed with ORIF and excellent outcome at 1-year follow-up.
Conclusion
This is among the few reported cases of bilateral anterior column acetabulum fracture due to high-velocity injury following RTA. The pattern of injury clarifies the complexity of acetabulum fractures and challenges associated with treating these injuries. Patients do excellent as seen from this case if appropriately evaluated and managed without any complication.
Clinical Message.
With the rising incidence of high-velocity injuries, such presentations will be seen more often in the times ahead. For such complex case, we should evaluate well to plan for definitive management, and if we stick to this, we can achieve excellent-to-good outcome depending on the case.
Biography

Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that Informed consent of the patient is taken for publication of this case report
References
- 1.Aynaci O, Kerimoglu S, Ozturk C, Saracoglu M. Bilateral non-traumatic acetabular and femoral neck fractures due to pregnancy-associated osteoporosis. Arch Orthop Trauma Surg. 2008;128:313–6. doi: 10.1007/s00402-007-0439-z. [DOI] [PubMed] [Google Scholar]
- 2.Balcarek P, Dresing K, Walde TA, Tezval M, Stürmer KM. Myoclonus induced bilateral acetabular fracture dislocations. J Arthroplasty. 2009 Aug;24(5):826.e11–15. doi: 10.1016/j.arth.2008.05.030. [DOI] [PubMed] [Google Scholar]
- 3.Friedberg R, Buras J. Bilateral acetabular fractures associated seizure:A case report. Ann Emerg Med. 2005;46:260–2. doi: 10.1016/j.annemergmed.2005.03.009. [DOI] [PubMed] [Google Scholar]
- 4.Khalily C, Ilizaliturri VM, Jr, Lester DK. Bilateral pathologic fractures of the hip and acetabulum treated with cementless total hip arthroplasty. J Arthroplasty. 2002;17:664–6. doi: 10.1054/arth.2002.32703. [DOI] [PubMed] [Google Scholar]
- 5.Schachter AK, Roberts CS, Seligson D. Occult bilateral acetabular fractures associated with high-energy trauma and osteoporosis. J Orthop Trauma. 2003;17:386–9. doi: 10.1097/00005131-200305000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Vaishya R, Kumar R, Maharjan RR. Percutaneous fixation of bilateral anterior column acetabular fractures:A case report. Apollo Med. 2013;11:52–5. [Google Scholar]
- 7.Gupta RK, Kapoor S. Bilateral displaced acetabular fractures associated with an open book injury of pelvis and sacral fracture. J Clin Orthop Trauma. 2011;2:57–9. [Google Scholar]