

Abstract
Surgical repair of the hip is considered an extremely painful procedure. Managing pain in this surgery is challenging even with several available options, each with limitations. Erector spinae plane (ESP) block is a novel technique that has been used in different types of surgery, with promising results. Herein, we describe a case of a successful ESP block for pediatric hip surgery. In the future, ESP block could be an alternative technique for providing effective analgesia.
Keywords: Analgesia, Child, Erector spinae plane block, Hip surgery
Surgical repair of the hip can be extremely painful and is associated with considerable postoperative pain in children despite the use of systemic opioids. These patients may benefit from neuraxial analgesia in adjunction with general anesthesia. The reported advantages of this technique include decreased opiate exposure, decreased time in the post-anesthesia recovery room, decreased hospital stay, and increased satisfaction of the patient. However, the considerably high rate of adverse effects of this technique limits its use in children [1,2]. Of the adverse effects, hypotension, postoperative nausea and vomiting, urinary retention, excessive motor block, and pruritus are the most frequently observed. Regional anesthetic techniques would seem a better choice for improving acute pain management in these patients, with fewer adverse effects. Herein, we describe our experience with erector spinae plane (ESP) block, an effective novel technique of regional anesthesia for pediatric hip surgery.
Case Report
Parental informed consent for publication was obtained. A 4-year-old female patient (weight 15 kg, American Society of Anesthesiologists physical status I) was scheduled for surgical treatment of developmental dysplasia of the right hip under general anesthesia. She was monitored continuously with electrocardiography, pulse oximetry, noninvasive blood pressure measurement, and body temperature determination. After anesthetic induction with propofol and vecuronium, a 4.5-mm orotracheal tube was easily inserted into the trachea. Controlled ventilation was administered with 50% oxygen in air, and anesthesia was maintained using sevoflurane. An ultrasound-guided ESP block was performed with the patient lying on her left side and the surgical side on the top. After skin disinfection, sterile draping was placed and the ultrasound probe was sheathed. The level of the block was the transverse process of L2. The block was performed using a 9–12 MHz linear probe (LOGIQeⓇ, GE Healthcare, USA), which was placed in a parasagittal plane 1 cm from the posterior midline. The deep plane to the erector spinae muscle (ESM) was identified, and a 22 G, 50 mm insulated needle (Sonoplex StimⓇ, Pajunk, Germany) was inserted craniocaudally in plane between the transverse process and the fascia of the ESM (Fig. 1). After negative aspiration, 0.3 ml/kg of 0.25% bupivacaine was injected to confirm the correct position by visualizing the solution lifting the ESM off the transverse process (Supplementary Video 1). Spread of local anesthetic between the L1 and L4 transverse processes was thereafter visually tracked with the transducer. Surgical incision was performed after 20 min and the surgery lasted 2.5 h, during which the hemodynamic state of the patient remained stable, with excellent pain control under minimal anesthetic requirements. Changes in blood pressure and heart rate did not exceed 10% of the baseline (recorded at anesthetic induction). Intraoperatively, no systemic analgesics were needed apart from the scheduled acetaminophen administered 30 min before the end of the surgery. The patient was extubated, and emergence from anesthesia was uneventful. She had a maximum FLACC (face, legs, activity, cry, consolability) scale score of 1 in 24 h with 15 mg/kg acetaminophen administered every 6 h. On the second day of surgery, a pain score of 3 on the FLACC scale was noted, which was controlled with nonsteroidal anti-inflammatory drugs, leading to a reduction in the FLACC scale score to 1 without further need for opioid analgesics.
Fig. 1.
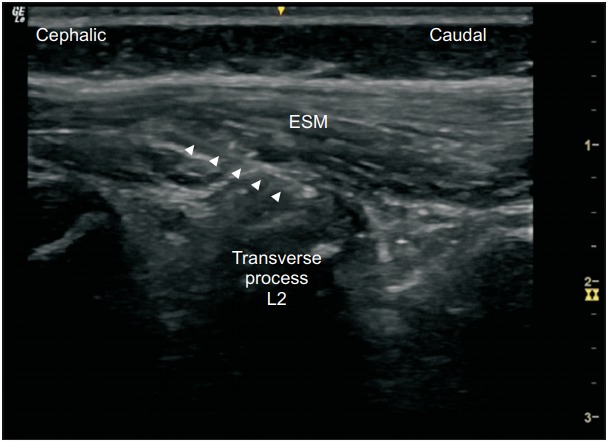
Ultrasound image showing the needle (arrow head) on top of the transverse process of L2. ESM: erector spinae muscle.
Discussion
First described by Forero et al. [3], the ESP block is a novel block in which a local anesthetic is deposited between the ESM and the underlying transverse process. It is a simpler technique than the ultrasound-guided paravertebral block, which is considered technically challenging, time consuming, and associated with important risks. Less technical expertise is required for the ESP block as the sonographic leading points are easily visualized. This method is also rather safe because the site of injection is far from the pleura, neuraxial structures, and major vascular structures. Furthermore, the craniocaudal spread of local anesthetic along the fascial plane underlying the ESM permits extensive, and thus multiple, dermatomal coverage from a single injection site [3]. The local anesthetic also penetrates anteriorly through the intertransverse connective tissue, gaining indirect access to the paravertebral space where it can potentially block the dorsal and ventral rami of the spinal nerves [3]. It may also block the sympathetic nerve fibers [4]. This block has been shown to be effective in providing thoracic analgesia when performed at the T5 level [5] and extensive somatic and visceral abdominal analgesia when performed at the T7-9 level [4].
The use of the ESP block is limited to the thoracic region in the pediatric population, with only a few reports (Table 1). It has been reported to provide effective postoperative analgesia for thoracic surgeries [6–10], nephrectomy [11], inguinal hernia repair [12], and laparoscopic cholecystectomy operations [13] in children. To our knowledge, ESP block performed in the lumbar region has not been reported in children.
Table 1.
Published Cases of Erector Spinae Plane Block in the Pediatric Population
| Title | Age | Indication | Level | LA and concentration | Volume | Spread of LA |
|---|---|---|---|---|---|---|
| Munoz et al. [6] | 7 yr | Tumor of the 11th right rib | T8 | Bupivacaine 0.5% | 14 ml (weight NP) | T5-T11 |
| De la Cuadra-Fontaine et al. [7] | 3 yr | Open thoracic surgery | T9 | Levo-bupivacaine 0.25% | 0.6 ml/kg | NP |
| Hernandez et al. [8] | 3 yr | Paraspinal thoracic lipoma | T1 | Bupivacaine 0.25% and lidocaine 1% | 0.2 ml/kg | NP |
| Ueshima and Otake [9] | 6 yr | Funnel chest | T6 (bilateral block) | Levo-bupivacaine 0.25% | 0.6 ml/kg into each side | NP |
| 8 yr | Funnel chest | T6 (bilateral block) | ||||
| Kaplan et al. [10] | 7 months | Left upper lobectomy | T6 | Ropivacaine 0.2% | 0.3 ml/kg | T3-T10 |
| Aksu and Gurkan [11] | 7 yr | Nephrectomy | T12 | Bupivacaine 0.25% | 0.5 ml/kg | NP |
| 6 months | Nephrectomy | T12 | ||||
| Hernandez et al. [12] | 2 months | Inguinal hernia | T6 | Bupivacaine 0.25% and lidocaine 1% | 0.4 ml/kg | T4-L1 |
| Thomas and Tulgar [13] | 11 yr | Laparoscopic cholecystectomy | T9 | Bupivacaine 0.25% | 0.6 ml/kg | NP |
| Present case | 4 yr | Developmental dysplasia of the hip | L2 | Bupivacaine 0.25% | 0.3 ml/kg | L1-L4 |
LA: local anesthetic, NP: not precise.
Tulgar et al. [14] reported a successful ultrasound-guided ESP block performed at the L4 transverse process level for postoperative analgesia in adult patients undergoing hip and proximal femur surgeries. Computed tomographic imaging performed after the ESP block showed contrast material spreading along the lumbar plexus from the T12 to S1 vertebrae, confirming the hypothesis that the local anesthetic would spread similar to that in an ESP block performed at the thoracal levels. Similarly, the present report suggests that lumbar ESP block performed at the L2 level could provide effective postoperative analgesia for pediatric hip surgery. Furthermore, it suggests that ultrasound-guided ESP block could be the sole method for intraoperative analgesia, thus obviating opioid usage.
To date, there are no recommendations about the optimal dose of local anesthetic for use in an ESP block in children. In some previous reports, relatively smaller volumes of local anesthetic or similar volumes and concentrations as reported in this case were used. Hernandez et al. [12] used a volume of 0.2 ml/kg of 0.25% bupivacaine to perform an ESP block for inguinal hernia repair in a 2-month-old male patient. They also reported that they were able to achieve adequate anesthetic spread and analgesia with a volume of 0.2–0.3 ml/kg in other pediatric patients undergoing thoracic surgery. Kaplan et al. [10] reported the successful use of a modest amount of local anesthetic with an approximately 0.3 ml/kg bolus in an infant weighing 7 kg. Future studies on the optimal local anesthetic volume and concentration when performing ESP block in children would be useful to practitioners and to further enhance the understanding of this useful block.
ESP block performed at the L2 level as an adjunct to general anesthesia may be effective in providing reliable surgical analgesia and satisfactory postoperative pain control in pediatric hip surgery. It could be a reasonable alternative for operators who are wary of other techniques owing to the high risks of complications and/or the requirement for advanced skills, especially in the pediatric population.
Supplementary Material
References
- 1.Lloyd-Thomas AR. Pain management in paediatric patients. Br J Anaesth. 1990;64:85–104. doi: 10.1093/bja/64.1.85. [DOI] [PubMed] [Google Scholar]
- 2.Lejus C, Surbled M, Schwoerer D, Renaudin M, Guillaud C, Berard L, et al. Postoperative epidural analgesia with bupivacaine and fentanyl: hourly pain assessment in 348 paediatric cases. Paediatr Anaesth. 2001;11:327–32. doi: 10.1046/j.1460-9592.2001.00659.x. [DOI] [PubMed] [Google Scholar]
- 3.Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41:621–7. doi: 10.1097/AAP.0000000000000451. [DOI] [PubMed] [Google Scholar]
- 4.Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesiain bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42:372–6. doi: 10.1097/AAP.0000000000000581. [DOI] [PubMed] [Google Scholar]
- 5.Forero M, Rajarathinam M, Adhikary S, Chin KJ. Continuous erector spinae plane block for rescue analgesia in thoracotomy after epidural failure: a case report. A A Case Rep. 2017;8:254–6. doi: 10.1213/XAA.0000000000000478. [DOI] [PubMed] [Google Scholar]
- 6.Muñoz F, Cubillos J, Bonilla AJ, Chin KJ. Erector spinae plane block for postoperative analgesia in pediatric oncological thoracic surgery. Can J Anaesth. 2017;64:880–2. doi: 10.1007/s12630-017-0894-0. [DOI] [PubMed] [Google Scholar]
- 7.De la Cuadra-Fontaine JC, Concha M, Vuletin F, Arancibia H. Continuous erector spinae plane block for thoracic surgery in a pediatricpatient. Paediatr Anaesth. 2018;28:74–5. doi: 10.1111/pan.13277. [DOI] [PubMed] [Google Scholar]
- 8.Hernandez MA, Palazzi L, Lapalma J, Forero M, Chin KJ. Erector spinae plane block for surgery of the posterior thoracic wall in a pediatric patient. Reg Anesth Pain Med. 2018;43:217–9. doi: 10.1097/AAP.0000000000000716. [DOI] [PubMed] [Google Scholar]
- 9.Ueshima H, Otake H. Clinical experiences of erector spinae plane block for children. J Clin Anesth. 2018;44:41. doi: 10.1016/j.jclinane.2017.10.021. [DOI] [PubMed] [Google Scholar]
- 10.Kaplan I, Jiao Y, AuBuchon JD, Moore RP. Continuous erector spinae plane catheter for analgesia after infantthoracotomy: a case report. A A Pract. 2018;11:250–2. doi: 10.1213/XAA.0000000000000799. [DOI] [PubMed] [Google Scholar]
- 11.Aksu C, Gürkan Y. Ultrasound guided erector spinae block for postoperative analgesia in pediatric nephrectomy surgeries. J Clin Anesth. 2018;45:35–6. doi: 10.1016/j.jclinane.2017.12.021. [DOI] [PubMed] [Google Scholar]
- 12.Hernandez MA, Palazzi L, Lapalma J, Cravero J. Erector spinae plane block for inguinal hernia repair in preterm infants. Paediatr Anaesth. 2018;28:298–9. doi: 10.1111/pan.13325. [DOI] [PubMed] [Google Scholar]
- 13.Thomas DT, Tulgar S. Ultrasound-guided erector spinae plane block in a child undergoing laparoscopic cholecystectomy. Cureus. 2018;10:e2241. doi: 10.7759/cureus.2241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tulgar S, Selvi O, Senturk O, Ermis MN, Cubuk R, Ozer Z. Clinical experiences of ultrasound-guided lumbar erector spinae plane block for hip joint and proximal femur surgeries. J Clin Anesth. 2018;47:5–6. doi: 10.1016/j.jclinane.2018.02.014. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.