

Abstract
Context:
Hair is said to gray prematurely when a minimum of five gray hairs occurs before the age of 20 in fair skinned, 25 in Asians, and 30 in Africans. It may be genetically associated with autoimmune syndromes or certain environmental factors.
Aims:
The aim of this study was to evaluate the serum level of iron, copper, and calcium and to assess their role in premature hair graying.
Subjects and Methods:
This study was carried out on 60 patients with premature hair graying (PHG) and 30 age- and sex-matched healthy individuals served as a control group. The severity of PHG was assessed by the hair whitening scoring system. Serum iron, copper, and calcium concentrations were measured using Beckman Coulter instrument and spectrophotometric method.
Results:
There was a reduction in serum levels of iron, copper, and calcium in patients with PHG in comparison with controls. There was a statistically negative significant correlation between the severity of PHG and serum iron and calcium levels. There was a negative nonsignificant correlation between body mass index and serum iron, copper, and calcium levels.
Conclusions:
Serum iron, copper, and calcium levels were reduced in association with PHG and correlated with its severity. Premature graying may be an indicator that hair is not getting enough nutrients and minerals, and supplementation with these trace elements might reverse and is expected to prevent progression of canities; however, further studies are needed to find the underlying mechanism of this relationship.
Key words: Calcium, copper, iron, premature hair graying, trace elements
INTRODUCTION
Hair pigmentation is one of the most conspicuous phenotypes of humans.[1] The biological process of gray hair appears to be associated with the progressive loss of pigment-producing cells.[2] Hair is said to gray prematurely when it occurs before the age of 20 in fair skinned, 25 in Asians, and 30 in Africans.[3] Although hair graying or canities is a common process occurring in people as their age, an unknown percentage of individuals experiences premature graying from familial inheritance or pathologic conditions.[4]
Premature hair graying has been shown to be associated with various autoimmune disorders such as vitiligo, pernicious anemia, thyroid diseases, and premature aging syndromes such as Werner's syndrome. Furthermore, studies have shown a role for environmental factors such as ultraviolet light, climate, smoking, drugs, trace elements, and nutritional deficiencies in the pathogenesis of premature graying.[5,6]
Trace element deficiencies lead to a spectrum of clinical manifestations especially in skin and hair. Pigmentary changes and hair loss are important manifestations of deficiency states. Iron and copper have been shown to affect hair growth and pigmentation. It has also been hypothesized that the premature graying is associated with osteopenia indicating a probable role for vitamin D3 and calcium.[7]
The present study was aimed to evaluate the serum level of iron, copper, and calcium and to assess their role in premature hair graying.
SUBJECTS AND METHODS
This study included 90 individuals were collected from the Outpatient Clinic of Dermatology and Venereology Department during the period from January to December 2016. The study included 60 patients with premature hair graying (<30 years old and have a minimum of five gray hair fibers), and 30 healthy persons of matched age and sex served as controls. The study was approved by the Research Ethics Committee of Faculty of Medicine, Tanta University. All participants signed on informed consent before the participation in the study. Patients who were excluded from the study included those with any systemic or dermatological diseases that might affect the results such as coronary artery disease and vitiligo. Patients who had received any drugs that may cause bleaching of hair as chloroquine.
Complete history taking and thorough general and dermatological examinations were done for every patient including the body mass index (BMI).
Severity of hair graying was assessed according to hair whitening score (HWS);[8] HWS 1 (Trace): <25%, HWS 2 (Mild): 25%–<50%, HWS 3 (Moderate): 50%–<75%, HWS 4 (Manifest): 75%–<100%, and HWS 5 (Complete): 100%. Location of gray hair, the scalp was divided into five areas (frontal region, two temporal regions, vertex, and occipital region). Texture and diameter of gray hair fibers were also assessed.
Estimation of serum iron, copper, and calcium levels was done
5-cm venous blood samples were collected from patients and controls without adding the anticoagulants, and serum was separated by centrifugation at (4000 rpm) room temperature. Serum was separated immediately after centrifugation. Serum iron and calcium levels estimation were done using the Beckman Coulter AU System method.[9,10] Serum copper level estimation was done using the simple spectrophotometric method.[11]
Statistical presentation and analysis of the present study were conducted using the mean, standard deviation, Kruskal–Wallis test, Mann–Whitney test, Fisher's exact test and Monte Carlo test, ANOVA, Student's (unpaired-sample) t-test, and Chi-square test, and linear correlation coefficient by using SPSS statistical software 15.0 for windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic data of the patients are summarized in Table 1.
Table 1.
Distribution of the studied groups according to sex, age, duration, body mass index, residence, family history, and associated diseases
| Patients (n=60), n (%) |
Control (n=30), n (%) |
χ2 | P | |
|---|---|---|---|---|
| Sex | ||||
| Male | 26 (43.3) | 10 (33.3) | 0.417 | 0.519 |
| Female | 34 (56.7) | 20 (66.7) | ||
| Age (year) | ||||
| Childhood <11 | 2 (3.3) | 0 | 3.273 | 0.195 |
| Adolescence 11-20 | 10 (16.7) | 12 (40.0) | ||
| Young adults 20-40 | 48 (80.0) | 18 (60.0) | ||
| Duration (year) | ||||
| 1-4 | 38 (63.3) | |||
| 5-8 | 22 (36.7) | |||
| BMI | ||||
| Range | 20.6-37.1 | 19.5-32.35 | 3.25 | 0.078 |
| Mean±SD | 28.26±4.28 | 25.90±3.83 | ||
| Residence | ||||
| Rural | 34 (56.7) | 12 (40.0) | 1.112 | 0.292 |
| Urban | 26 (43.3) | 18 (60.0) | ||
| Family history | ||||
| Positive | 46 (76.7) | 0 | 23.523 | 0.001* |
| Negative | 14 (23.3) | 30 (100.0) | ||
| Associated diseases | ||||
| Hair problems | ||||
| Hair falling | 42 (70.0) | 14 (46.6) | 2.321 | 0.128 |
| Negative | 18 (30.0) | 16 (53.3) | ||
| Stress | ||||
| Positive | 32 (53.3) | 10 (33.3) | 1.612 | 0.205 |
| Negative | 28 (46.7) | 20 (66.6) |
*Significant – P≤0.05. SD – Standard deviation; BMI – Body mass index; SD – Standard deviation
In the studied patients' group with (PHG), there were 34 females (56.7%) and 26 males (43.3%) with the female: male ratio was 1.3:1. Their age ranged from 5 to 30 years. Two patients (3.3%) were < 11 years, 10 patients (16.7%) aged from 11 to 20 years, and 48 patients (80%) aged more than 20 years. In the control group, there were 20 females (66.66%) and 10 males (33.33%) and their age ranged from 14 to 30 years; 12 persons (40%) aged from 11 to 20 years and 18 persons (60%) aged more than 20 years. Comparison between the two studied groups according to sex and age revealed no statistically significant difference in between them (P = 0.519, 0.195, respectively).
There were 46 patients (76.7%) had positive family history of PHG, while 14 patients (23.3%) had negative family history. In control group, all (30) persons had negative family history. There was a statistically significant difference between the two groups regarding family history (P = 0.001*).
Premature hair graying was assessed by HWS score; there were 40 patients (66.6%) with HWS1 (trace severity), 6 patients (10%) with HWS 2 (mild severity), and 14 patients (23.3%) with HWS3 (moderate severity) Figures [1–3].
Figure 1.

Trace severity of premature hair graying (HWS 1), showing <25% white hair. HWS – Hair whitening score
Figure 3.
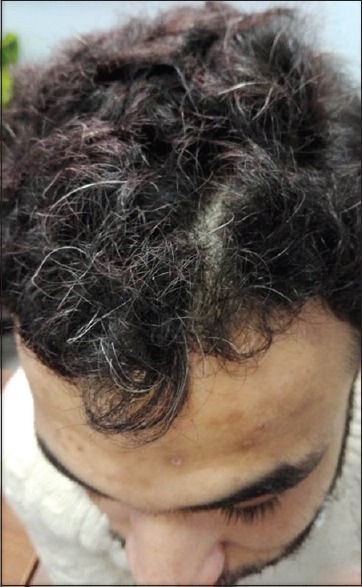
Moderate severity of premature hair graying (HWS 3), showing 50%–<75% white hair. HWS – Hair whitening score
Figure 2.

Mild severity of premature hair graying (HWS 2), showing 25%–<50% white hair. HWS – Hair whitening score
The serum level of iron in the patients with PHG ranged from 10 to 158 ug/dl with a mean of 78.77 ± 34.68 ug/dl. In the control group, it ranged from 33 to 161 ug/dl with a mean of 104.40 ± 46.50 ug/dl. There was a statistically significant decrease in the serum level of iron in the patients' group when compared to the control group (P = 0.046*).
The serum copper level in the patients with PHG ranged from 71.6 to 227.0 ug/dl with a mean of 126.22 ± 31.66 ug/dl while in control group, it ranged from 89.7 to 849 ug/dl with a mean of 195.76 ± 185.95 ug/dl. There was no statistically significant difference between the two studied groups regarding the serum level of copper (P = 0.098).
The serum level of calcium in the patients with PHG ranged from 7.9 to 11.2 mg/dl with a mean of 9.54 ± 0.71 mg/dl. In the control group, it ranged from 9.4 to 10.7 mg/dl with a mean of 9.95 ± 0.39 mg/dl. There was a statistically significant decrease in the serum level of calcium in patients' group when compared to control group (P = 0.045*) [Table 2].
Table 2.
Comparison between the two studied groups according to the serum level of iron, copper, and calcium
| Range | Mean±SD | t-test | P | |
|---|---|---|---|---|
| Iron | ||||
| Patients | 10-158 | 78.77±34.68 | 3.955 | 0.046* |
| Control | 33-161 | 104.40±46.50 | ||
| Copper | ||||
| Patients | 71.6-227.0 | 126.22±31.66 | 2.536 | 0.098 |
| Control | 89.7-849 | 195.76±185.95 | ||
| Calcium | ||||
| Patients | 7.9-11.2 | 9.54±0.71 | 4.256 | 0.045* |
| Control | 9.4-10.7 | 9.95±0.39 |
*Significant – P≤0.05. SD – Standard deviation
There was a statistically significant difference between the severity of PHG and serum iron and calcium levels (P = 0.021*, 0.002,* respectively). There was no statistically significant difference between the severity of PHG and serum copper level (P = 0.743) There was no statistically significant difference between the severity of PHG and BMI of the studied patients (P = 0.247) [Table 3].
Table 3.
Comparison between the serum level of iron, copper, calcium, and body mass index regarding the severity of premature hair graying in patient’s group
| HWS score | Serum iron | Serum copper | Serum calcium | BMI |
|---|---|---|---|---|
| Trace | ||||
| Range | 50-158 | 82.2-227 | 8.4-11.2 | 20.6-37.1 |
| Mean±SD | 89.35±32.12 | 139.27±32.35 | 9.82±0.53 | 27.32±4.27 |
| Mild | ||||
| Range | 24-135 | 85.5-173 | 8.9-9.7 | 25.52-33 |
| Mean±SD | 65.33±60.68 | 131.50±43.92 | 9.37±0.42 | 30.24±4.11 |
| Moderate | ||||
| Range | 10-84 | 71.6-148 | 7.9-9.8 | 21.48-33.2 |
| Mean±SD | 44.86±29.01 | 112.37±24.4 | 8.81±0.77 | 30.07±4.06 |
| t-test | 4.505 | 0.301 | 7.786 | 1.474 |
| P | 0.021* | 0.743 | 0.002* | 0.247 |
*Significant – P≤0.05. BMI – Body mass index; SD – Standard deviation; HWS – Hair whitening score
There was a negative significant correlation between the severity of PHG and serum iron level while there were nonsignificant correlations between serum iron level and either age, duration, or BMI. There were nonsignificant correlations between serum copper level and age, duration, severity, and BMI. There were negative significant correlations between serum calcium level and age, duration, and severity of PHG while there was no significant correlation between serum calcium level and BMI [Table 4].
Table 4.
Correlations between the serum level of iron, copper, and calcium and clinical parameters (age, duration, severity, and body mass index) in patient’s group
| Iron | Copper | Calcium | ||||
|---|---|---|---|---|---|---|
| r | P | r | P | r | P | |
| Age | −0.116 | 0.540 | 0.023 | 0.905 | −0.495 | 0.005* |
| Duration | −0.291 | 0.119 | −0.193 | 0.307 | −0.620 | 0.001* |
| Severity | −0.453 | 0.012* | −0.194 | 0.305 | −0.635 | 0.001* |
| BMI | −0.198 | 0.294 | −0.070 | 0.712 | −0.219 | 0.245 |
*Significant – P≤0.05. BMI – Body mass index
DISCUSSION
Hair graying (or canities) is considered to be a natural age-associated feature.[12] Aging of hair comprises two important components, namely weathering of hair shaft and aging of hair follicle. Weathering of hair shaft involves degeneration of hair fiber that progresses from the root to the tip. Aging of hair follicle refers to reduced melanocyte function (known as graying) and decreased hair production.[6]
Oxidative stress related to mitochondrial DNA damage has been found to be high in gray hair follicles. Gray hair melanocytes with more vacuoles also support the role of oxidative stress with accumulation of reactive oxygen species in gray hair follicles. The relationship between oxidative stress and psychological disorders (emotional stress, anxiety, and depression), alcohol intake, and atherosclerosis has been reported.[9]
Although the primary cause of PHG is considered to be genetic, autoimmune disorders are also shown to be related to PHG. Few studies have also reported that environmental factors (such as ultraviolet light and climate), smoking, drugs, deficiencies of trace elements, and nutritional deficiencies also play a role in PHG.[5,6,13]
The aim of this work was to evaluate the serum level of iron, copper, and calcium and to assess their role in premature hair graying.
Regarding the family history of PHG, it was positive in 76.7% of the studied patients that may reflect the genetic background of the pathogenesis of PHG. This was in agreement with the study conducted by Bhramaramba et al., 2016[14] where positive family history was found in 50.4% of patients. Moreover, Bhat et al., 2016[15] found that 31 of patients (62%) had a positive family history.
History of stress was reported in 53.3% of the studied patients. This was in agreement with Bhramaramba et al., 2016[14] who reported that emotional/psychosocial stress (22%) was the second most common aggravating factor in their study.
As regards the severity of PHG in the studied patients according to HWS; there were 66.6% of patients had trace severity (HWS 1), 10% of patients had mild severity (HWS 2), and 23.3% of patients had moderate severity (HWS 3). This was similar to a previous study conducted by Bhramaramba et al., 2016[14] who reported that 50% of patients had mild, 23% had moderate, 16% had severe, and 6% had very severe PHG.
There was no statistically significant relationship between the severity of PHG and BMI of the studied patients. This matched with the results of a study done by Zayed et al., 2013[16] who reported that there was no significant association between PHG and BMI. On the other hand, Shin et al., 2015[17] found that PHG was significantly higher in the overweight and obese groups than in the normal weight group. They reported that obesity was correlated with severity of PHG.
In this study, the serum level of iron in the studied patients showed a statistically significant reduction in comparison to the control group which may suggest a role of iron in the etiopathogenesis of PHG. This finding was in agreement with that of Bhat et al., 2016[15] who performed a study on serum iron, ferritin, and calcium levels in premature canities, the serum levels of iron were found to be significantly low in their patients with premature canities.
It was reported that iron affects melanogenesis by the rearrangement of dopachrome to 5, 6– dihydroxyindoles and oxidative polymerization of 5, 6– dihydroxyindoles to melanin pigments.[14] Smith et al., 2004[18] provided evidence for the role of iron in the modulation of the activity of tyrosinase. It is reported that in a tautomerization reaction by dopachrome tautomerase, which is one of the later stages of melanin biosynthesis, the isomerization of dopachrome to 5,6-dihydroxyindole-2-carboxylic acid occurs. This enzyme is a metalloenzyme with ferrous in at its active site.
There was a negative significant correlation between the severity of PHG and serum iron level in the studied patients; whereas with increasing the severity of PHG, there was a more reduction in serum iron level. However, Bhat et al., 2016[15] reported that no correlation between mean iron level and severity of canities in their patients.
There was a nonsignificant reduction in the serum level of copper when compared with the control group. Furthermore, there was a negative nonsignificant correlation between the serum copper level and severity of PHG. This may be due to copper being able to act as both an antioxidant and a prooxidant. As an antioxidant, Cu scavenges or neutralize free radicals and may reduce or prevent some of the damage they cause.[19] This matched with Chakrabarty et al., 2016[6] who reported that there was no significant association between PHG and serum copper concentration while Naieni et al., 2012[5] reported that there was a significant association between PHG and low serum copper concentration. This may be due to that copper can play an important role in melanogenesis. One of the most important enzymes in these reactions is tyrosinase. Copper ions, which are required for tyrosinase activity, bind to the inner portion of tyrosinase.
The serum level of calcium showed a statistically significant reduction in the PHG patients' group in comparison to the control group. This was supported by Bhat et al., 2016[15] who reported that the serum level of calcium was found to be significantly lower in their patients with premature canities than control group. Furthermore, it matched with Bhat et al., 2013[13] who reported that serum calcium levels and vitamin D3 levels were significantly lower in patients with PHG.
Chakrabarty et al., 2016[6] disagreed with the previous results. They reported that there was no significant association between PHG and serum calcium concentration. It was reported that PHG has been linked to decreased bone mineral density as calcium is involved in some steps of melanogenesis.[20]
A negative significant correlation was found between the serum calcium level and severity of PHG in our studied patients; whereas with increasing in the severity of PHG, there was a more reduction in serum calcium level. While Bhat et al., 2016[15] reported that there was no correlation between serum calcium level and the severity of canities in their patients.
CONCLUSIONS
From these results, we concluded that serum iron, copper, and calcium levels were reduced in association with PHG and correlated with its severity. Premature graying may be an indicator that hair is not getting enough nutrients and minerals and supplementation with these trace elements might reverse and is expected to prevent progression of canities; however, further studies are needed to find the underlying mechanism of this relationship.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ito S, Wakamatsu K. Diversity of human hair pigmentation as studied by chemical analysis of eumelanin and pheomelanin. J Eur Acad Dermatol Venereol. 2011;25:1369–80. doi: 10.1111/j.1468-3083.2011.04278.x. [DOI] [PubMed] [Google Scholar]
- 2.Commo S, Gaillard O, Bernard BA. Human hair greying is linked to a specific depletion of hair follicle melanocytes affecting both the bulb and the outer root sheath. Br J Dermatol. 2004;150:435–43. doi: 10.1046/j.1365-2133.2004.05787.x. [DOI] [PubMed] [Google Scholar]
- 3.Trüeb RM. Pharmacologic interventions in aging hair. Clin Interv Aging. 2006;1:121–9. doi: 10.2147/ciia.2006.1.2.121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McEvoy B, Beleza S, Shriver MD. The genetic architecture of normal variation in human pigmentation: An evolutionary perspective and model. Hum Mol Genet. 2006;15(Spec No 2):R176–81. doi: 10.1093/hmg/ddl217. [DOI] [PubMed] [Google Scholar]
- 5.Fatemi Naieni F, Ebrahimi B, Vakilian HR, Shahmoradi Z. Serum iron, zinc, and copper concentration in premature graying of hair. Biol Trace Elem Res. 2012;146:30–4. doi: 10.1007/s12011-011-9223-6. [DOI] [PubMed] [Google Scholar]
- 6.Chakrabarty S, Krishnappa PG, Gowda DG, Hiremath J. Factors associated with premature hair graying in a young Indian population. Int J Trichology. 2016;8:11–4. doi: 10.4103/0974-7753.179384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Heath ML, Sidbury R. Cutaneous manifestations of nutritional deficiency. Curr Opin Pediatr. 2006;18:417–22. doi: 10.1097/01.mop.0000236392.87203.cc. [DOI] [PubMed] [Google Scholar]
- 8.Tan SP, Weller RB. Sudden whitening of the hair in an 82-year-old woman: The 'overnight greying' phenomenon. Clin Exp Dermatol. 2012;37:458–9. doi: 10.1111/j.1365-2230.2011.04211.x. [DOI] [PubMed] [Google Scholar]
- 9.Akin Belli A, Etgu F, Ozbas Gok S, Kara B, Dogan G. Risk factors for premature hair graying in young Turkish adults. Pediatr Dermatol. 2016;33:438–42. doi: 10.1111/pde.12881. [DOI] [PubMed] [Google Scholar]
- 10.Hollfelder B, Blankenburg G, Wolfram LJ, Höcker H. Chemical and physical properties of pigmented and non-pigmented hair ('grey hair') Int J Cosmet Sci. 1995;17:87–9. doi: 10.1111/j.1467-2494.1995.tb00112.x. [DOI] [PubMed] [Google Scholar]
- 11.Daulatabad D, Singal A, Grover C, Sharma SB, Chhillar N. Assessment of oxidative stress in patients with premature canities. Int J Trichology. 2015;7:91–4. doi: 10.4103/0974-7753.167469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Goldberg LJ, Lenzy Y. Nutrition and hair. Clin Dermatol. 2010;28:412–9. doi: 10.1016/j.clindermatol.2010.03.038. [DOI] [PubMed] [Google Scholar]
- 13.Bhat RM, Sharma R, Pinto AC, Dandekeri S, Martis J. Epidemiological and investigative study of premature graying of hair in higher secondary and pre-university School children. Int J Trichology. 2013;5:17–21. doi: 10.4103/0974-7753.114706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bhramaramba TS, Sathyanarayana BD, Swaroop MR, Devaraj Y, Raghavendra JC, Dukkipati M, et al. A clinic-epidemiological study of premature canities of degree college students in the rural area. Int J Adv Case Rep. 2016;3:489–93. [Google Scholar]
- 15.Bhat YJ, Hassan I, Sajad P, Malik R, Majid S, Mubashir S, et al. Serum iron, ferritin and calcium levels in premature canities. Hair Ther Transplant. 2016;6:1–3. [Google Scholar]
- 16.Zayed AA, Shahait AD, Ayoub MN, Yousef AM. Smokers' hair: Does smoking cause premature hair graying? Indian Dermatol Online J. 2013;4:90–2. doi: 10.4103/2229-5178.110586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shin H, Ryu HH, Yoon J, Jo S, Jang S, Choi M, et al. Association of premature hair graying with family history, smoking, and obesity: A cross-sectional study. J Am Acad Dermatol. 2015;72:321–7. doi: 10.1016/j.jaad.2014.11.008. [DOI] [PubMed] [Google Scholar]
- 18.Smith DR, Spaulding DT, Glenn HM, Fuller BB. The relationship between Na(+)/H(+) exchanger expression and tyrosinase activity in human melanocytes. Exp Cell Res. 2004;298:521–34. doi: 10.1016/j.yexcr.2004.04.033. [DOI] [PubMed] [Google Scholar]
- 19.Davis CD. Low dietary copper increases fecal free radical production, fecal water alkaline phosphatase activity and cytotoxicity in healthy men. J Nutr. 2003;133:522–7. doi: 10.1093/jn/133.2.522. [DOI] [PubMed] [Google Scholar]
- 20.Orr-Walker BJ, Evans MC, Ames RW, Clearwater JM, Reid IR. Premature hair graying and bone mineral density. J Clin Endocrinol Metab. 1997;82:3580–3. doi: 10.1210/jcem.82.11.4338. [DOI] [PubMed] [Google Scholar]