

Supplemental Digital Content is available in the text
Keywords: limb lengthening, osteomyelitis, tibial hemimelia
Abstract
Rationale:
Tibial hemimelia is known as a rare congenital lower limb deficiency. It has been classified into different types based on Jones classification, and the traditional treatment of tibial hemimelia is amputation. Here we present a variant and unclassified case of tibial hemimelia, which was caused by osteomyelitis. And the lower limb with tibial hemimelia was salvaged by asymmetric limb lengthening.
Patient concerns:
19-year-old girl had the shortened and curved left lower extremity with walking abnormalities.
Diagnosis:
The patient's deformity was caused by osteomyelitis of tibia occurred when she was 18 month old. The tibial shaft was absent, while the proximal and distal tibia was present but was hypoplastic with radiographic analysis. The fibula was hypertrophied and curved like the capital letter C. The leg length discrepancy (LLD), mostly coming from the left lower leg, was 22 cm.
Interventions:
We were able to salvage the limb successfully by 5 operations, including releasing soft tissue, fusing the proximal tibiofibular joint, fibular osteotomy, femur lengthening, and fibular lengthening.
Outcomes:
The whole treatment time for the patient was 3 years and 2 months, and she was followed up for 5 years afterward. The length of femur lengthening and fibula lengthening during the reconstruction were 7.8 cm and 11 cm, respectively. Most of the deformities were corrected, except that the left lower limb was still 2 cm shorter than the contralateral limb, and the 34 mm of mechanical axis deviation (MAD) of left lower limb remained. The reason why the patient's lower limbs were asymmetric was that the femur and fibular lengthening were performed within the affected limb only. Overall, the patient was very satisfied with her asymmetric limbs and its function after surgeries.
Lessons:
The LLD in this case mainly came from tibial hemimelia. However, the fibula was unable to be lengthened to 22 cm during the lower leg distraction process because of blood flow disturbance. We could only lengthen the femur to salvage the limb in this situation. Even though the patient still had a few residual deformities and a pair of asymmetric lower limbs, she was satisfied with the function and appearance of the reconstructed limb. Therefore, the lower limb with tibial hemimelia can be salvaged by asymmetric limb lengthening in special cases.
1. Introduction
Tibial hemimelia, known as the congenital lower limb deficiency, is a very rare anomaly with an incidence of approximately 1 in 1 million live births.[1] It is characterized by deficiency of tibia with relatively intact fibula and marked shortening of the involved extremity with a severe equinovarus deformity.[2] It was a great challenge for the orthopedic surgeons to correct the deformities of the knee, ankle, foot, and the shortened, dysplastic, or absent tibia completely. Early ablative procedures for tibial hemimelia have been proposed in some literature; however, this approach is not well accepted in many cultures, especially in many Eastern countries.[3] For several decades, surgeons used the distraction osteogenesis principles in both bone and soft tissue to increase the expectancy of a functional extremity, even in difficult tibial hemimelia cases.[3,4]
The patient who suffered from tibial hemimelia in this article was caused by osteomyelitis, but not congenital deficiency. Therefore, the deformity in this case of tibial hemimelia could not be classified by any of the present existing systems, such as Jones,[5] Weber,[7] or Paley[6] classification. We used an unconventional method to reconstruct and correct the deficient leg rather than amputation. The novelty of our study is that very few similar cases with satisfactory outcome have been reported before this study.
2. Case report
A 19-year-old girl was born without any congenital deformity. Her parents are healthy and non-consanguineous, and her only elder sister is normal. When she was 18-month-old, she suffered from repeated fever, and her left lower leg ulcer appeared after then. The wound was cured by Chinese medicine patches when she was 3. According to her previous medical history, we can deduce her diagnosis at that time was acute hematogenic osteomyelitis of left lower leg. As she was growing up, the shortening and deformity of her left lower leg became obvious. She could walk without crutches, but it was very difficult for her to walk since she had to crouch down and straight up to exchange the supporting leg of length discrepancy for every step. She was very eager to walk upright by her own leg rather than amputating.
During the physical examination, upper limbs and spine were unaffected, as well as the right lower extremity. The left side of hip was stable and normal in terms of range of motion. The knee was rigid and the range of movement was extension 0° and flexion 30°. There was a bowing with convexity laterally and the lower leg was externally rotated relative to the femoral condyle. Leg length discrepancy (LLD) was 22 cm, which was mostly from the left lower leg. The left foot was in a 45° equinovarus deformity but the foot shape was normal. The movement range of ankle was 90° extension and 15°plantar flexion (Fig. 1; Video 1).
Figure 1.

Pre-operative clinical view of left affected leg. The medial soft tissue of left lower leg was extremely contracted.
A radiograph (Fig. 2A and B) showed the pelvis tilted to the left severely. The left femoral condyles with mildly hypoplastic could not match the distal tibial plateau to form a normal articulated joint. Only 4.5 cm of the proximal tibia was present. The tibial shaft was absent, while the distal tibia was dysplastic and its length was about 7 cm. The fibula was hypertrophied and curved, with proximal migration of fibular head. There was a proximal subluxation of the fibula at the knee. In the ankle, the tibiotalar joint was also hypoplastic but the matching relationship of joint appeared to be nearly normal. However, the lateral malleolus was thickened and the distal tibiofibular joint was abnormal.
Figure 2.

(A, B) Pre-operative X-Ray film of the affected leg.
Since the circle external fixator was not accessible to our hospital in 2009, we used the Hoffmann II External Fixation System to correct the deformity at that time. Three-stage treatment was designed in our initial plan. In the first stage, we intended to straighten the bowing lower leg as much as possible. Subsequently, the shortened lower leg would be prolonged to the same length of the contralateral side in the second stage. The third stage was the fibula centralization to replace the missing tibial shaft.[5–9]
The first stage treatment was also conducted separately in sequential steps. During the first operation, we found that the disturbance of blood supply in deformity leg would occur if the contracted medial soft tissue was released too much. Therefore, we used the combined external fixator to distract the contractures of medial soft tissue gradually (Fig. 3). However, the patient still suffered from severe pain caused by the disturbance of blood supply during the process of distraction. One month later, the dislocated fibular head was pulled down and fused with the proximal tibia by 2 screws; the fibular osteotomy was also performed to correct the hypertrophied and curved fibula (Fig. 4).
Figure 3.
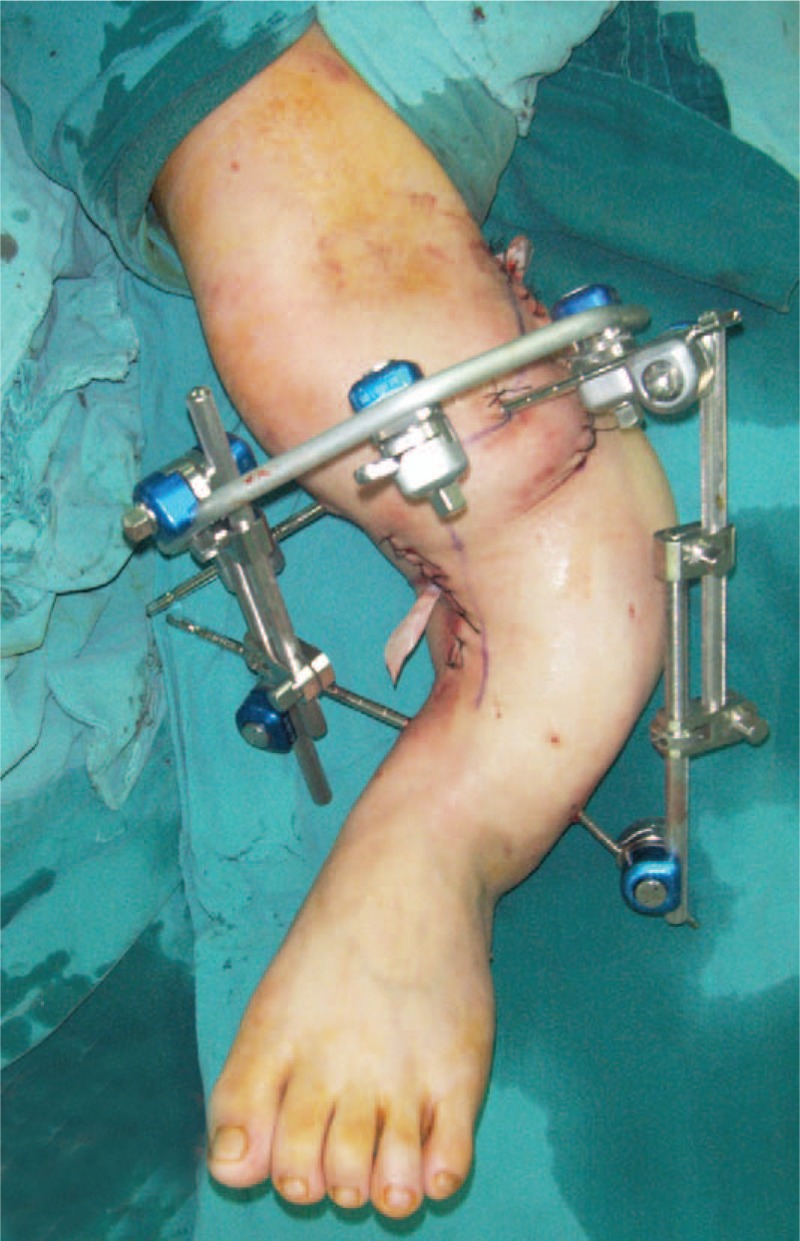
The first operation to release the medial soft tissue of left lower leg.
Figure 4.

The second operation of fusion the superior tibiofibular joint and fibular osteotomy.
Due to the blood supply disturbance in the first operation, we told the patient that her lower leg may not be corrected to the same length as the contralateral lower leg, and the alternative approach was lengthening the thigh to make both lower limbs equal length. The treatment time could be shortened with this approach since the femur lengthening could be performed before the bone healing of fibular osteotomy. The patient accepted our suggestion, and the femur was distracted 2-month postoperative of fibular osteotomy in the second stage (Fig. 5). After 6 months of the femur lengthening, the fibula was prolonged and the equinovarus deformity of foot was corrected at the same time (Fig. 6A and B). However, the patient suffered from severe pain again, due to the recurrence of blood supply disturbance during the process of lengthening. In this case, the continued lengthening of lower leg had to be ceased when the deformity leg was lengthened to 11 cm. But the left lower limb was still 2 cm shorter than the contralateral limb (Fig. 7A and B). Considering that the fibula would be transformed to inward and downward and be centralized as the tibial shaft, the shorten deformity would be remedied.
Figure 5.
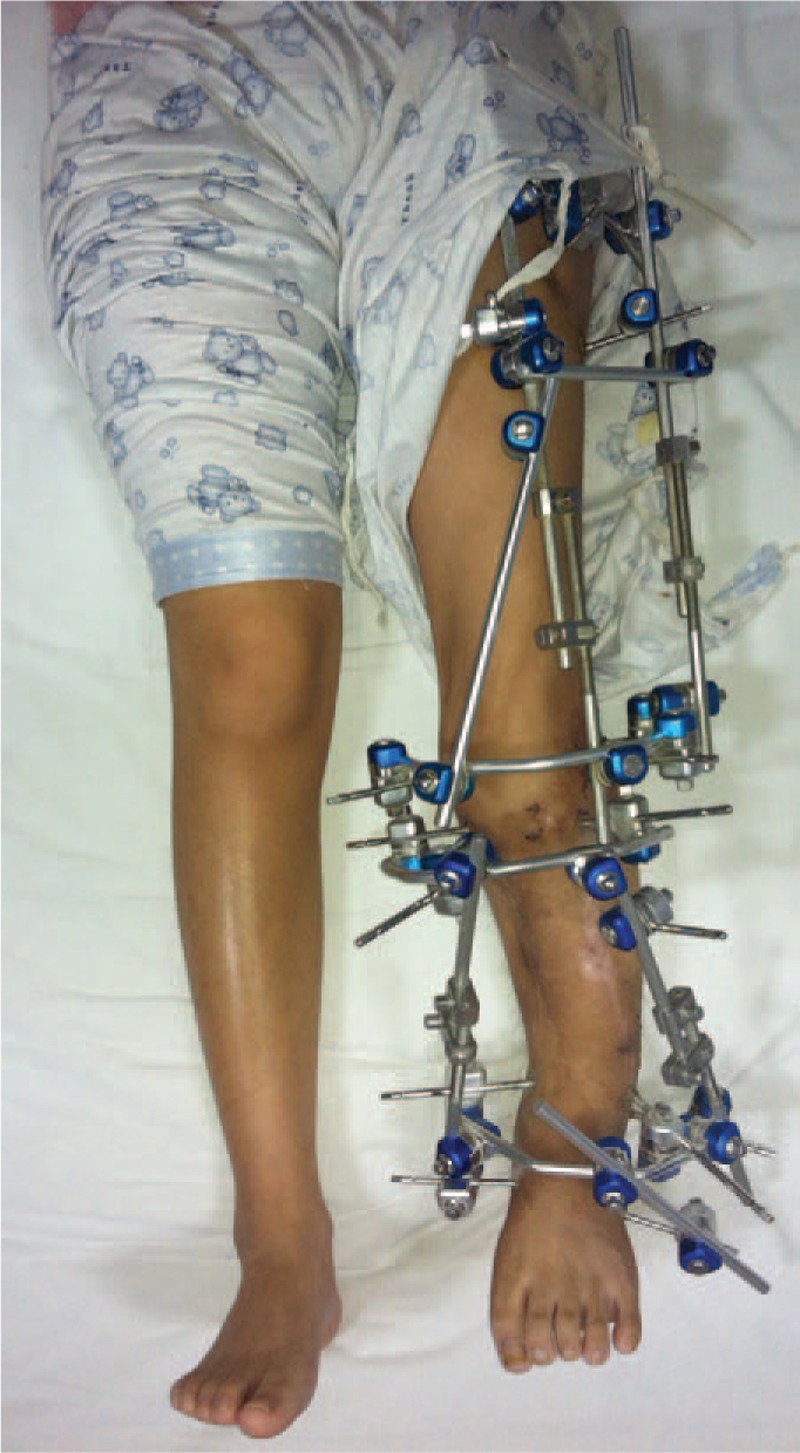
Clinical view with external fixator during the lengthening.
Figure 6.

Radiograph showing the bone regenerate in the (A) femur and (B) fibula.
Figure 7.

(A, B) Post-operative clinical view of 5 years follow-up.
The proper rehabilitation exercises, such as movement of the knee and ankle joint, were performed during the procedure of lengthening. When the regenerated bone began to be mineralized, the patient can walk in part weight-bearing with the external fixator. After maturation of the regeneration, the fixator and the internals were removed. Since then, the patient recovered well from these operations and was reviewed every 6 months for 5 years. We had advised that she should undergo the operation of fibula centralization to correct the force line of lower limb with Taylor ring external fixator[6] at every follow-up visit. But the patient was satisfied with the outcomes of previous operations and refused our advice.
The data about surgical result and the follow-up outcome are as follow. The patient underwent 5 operations in the whole treatment time of 3 years and 2 months. The bone healing time of fibular osteotomy was 8 months. The lengthening procedure of femur had continued for 102 days, and the external fixator was applied for 663 days. The total lengthening of femur achieved during the reconstruction was 7.8 cm. The external fixator index of femur was 85 days/cm. It took 156 days to lengthen the fibula for 11 cm, and the external fixator was removed after 492 days, at which time the limb lengthening and bone consolidation were completed. The external fixator index of fibula was 44.7 days/cm. The left lower limb was still 2 cm shorter than the contralateral limb (Fig. 7A and B). Knee valgus angle was 7.22°, femoral angle was 93.36°, tibia angle was 80.36°, and the mechanical axis deviation (MAD) of left lower limb was 34 mm. (Figs. 8 and 9A) The knee function was extension 0° and flexion 40°. The active ROM of ankle was normal (Fig. 9A–D; Video 2).
Figure 8.

Post-operative Radiograph showing the MAD of affected lower limb. MAD = mechanical axis deviation.
Figures 9.

(A-D) The active ROM of the affected knee and ankle in the 5 years post-operative.
3. Discussion
Tibial hemimelia, which was mostly known as the congenital deformity, is extremely rare.[1] However, our case caused by osteomyelitis during her childhood was quite distinct from the congenital tibial hemimelia. There are several classification systems for tibial hemimelia. The Jones classification,[5] published in 1978 and based on plain radiography findings, was the most widely accepted and used classification system. Our case neither conforms to any of the 4 types of Jones’ classification, nor the Weber- classification or Paley- classification. Shrivastava[10] present a variant of tibial hemimelia in 2009, which was very similar to our case. That case was a 9-year-old Asian boy who was diagnosed with tibial hemimelia when he was 1 week old, because of the absence of tibia shaft, fibular become hypertrophied, shortened and curved after loading the body weight. Since the patient walked on the lateral side of his equinovarus rather than the plantar side, the mechanical axis of lower limb deviated, in addition to the injury of the epiphysis of distal and proximal tibia resulted in the dysplasia of knee and ankle. As the result of the relatively overdeveloped proximal fibula comparing with the proximal tibia, the superior tibiofibular joint was malposition and the knee was rotational subluxation.
If we want to perform a corrective surgery to reconstruct the limb rather than amputation, all the deformity described above must be corrected as much as possible to achieve the plantigrade foot, stable and functioning knee joint, stable ankle joint, and leg length equality. We only had access to Hoffman external fixator to reconstruct the limb at that time, by which the deformities cannot be corrected in multiple planes.[11] Therefore, we had to divide the treatment into several steps. Firstly, the curved lower leg was straightened by releasing medial soft tissue, fusion the superior tibiofibular joint and the osteotomy of fibula. Only the straightened and shortened limb was suitable for being lengthened by the combined external fixator. If the ring external fixator can be used to correct the deformity, some surgical steps can be omitted and better results can be achieved, which was our shortcoming in this case.
The patient was an adult when she was treated, and the bone development was established and the deformity had existed for 18 years. Therefore, vascular crisis often occurred in the lower leg during the process of lengthening because of the severely contracted medial soft tissue. Eventually, the surgical plan had to be changed. The ipsilateral femur was distracted to achieve the equal length on both legs. Hence, we think that tibial hemimelia should be treated during childhood or adolescence.[5,7,8] The advantages are as follows:
-
1.
The degree of deformity is relatively gentle, and the limb reconstruction operation will be easier than its at adult age.
-
2.
It is beneficial for the development of the knee joint and ankle joint to restore the normal mechanical axis of lower limb as early as possible. As the consequence, the maximum joint function can be retained during growth period.
-
3.
The ability of bone regeneration in children is better than adult. That means the mineralization time in children after bone generation of distraction will be shorter than adults. Moreover, the time of fixation with external fixator can be shortened.
-
4.
Patients can return normal life much sooner and earlier, and the psychological effects caused by the deformity limb will be reduced.
Lengthening is associated with a certain number of complications: infection, poor quality osteogenesis, fracture after material ablation, stiffness, joint subluxation or dislocation, palsy, pain, psychological problems, disorder of blood supply, and material failure.[12] The left lower leg could only be lengthened to 11 cm in our report, but not the intended 22 cm to attain symmetrical and equal length lower limbs was owing to the pain and the disorder of blood supply in the deformity lower leg. The risk of complications from lengthening increases with distraction length.[13] Paley[14] mentioned that lengthening is limited by the soft tissues; hence, lengthening to 5 to 8 cm carries medium risk, and exceeding 8 cm increases risk substantially. We released the contractures of medial soft tissue first during treatment to reduce the risk of soft tissue complications. Moreover, the time of external fixator fixation was extended until the plain X-ray showed the regeneration callus were 3 or 4 continuous cortices of at least 2 mm thickness. Therefore, the patient had good quality of osteogenesis without any fracture after removal of the external fixator.
The asymmetry lengthening is the last resort to achieve the leg length equality. The non-physiological lengthening may associate with certain degrees of inconvenience to the patient's life, such as crouching down and sitting down in a special posture. Therefore, the asymmetry lengthening is only suitable in the condition that single lower leg or thigh distraction cannot reach the equal length of lower limbs, and the patient has a strong willingness to reconstruct and distract his limb. A similar case of asymmetry lengthening was reported in 2015.[15] A 4-year-old girl with a Jones type IA tibial hemimelia in the right lower extremity was reconstructed the tibial plateau with her ipsilateral and contralateral fibular heads. Limb length discrepancy was corrected with a femoral osteotomy and lengthening (total lengthening 13 cm). During 4-year follow-up, the limb was well aligned without significant length discrepancy and had good function knee. However, 4-year follow-up was not long enough for the asymmetry lengthening, and the result of longer term should still be evaluated. In our case, although the patient is satisfied with the current situation after the operations, the fibular centralization should be performed in future. Otherwise, the MAD of lower limb will accelerate the cartilage degeneration of the ipsilateral ankle, knee, and hip.
Statement: The case report was approved by the ethics committee of Zhongnan Hospital of Wuhan University (approval number: 2018046), and the patient signed informed consent to publication of her clinical details and/or clinical images.
Author contributions
Conceptualization: Li Yu, Guorong Yu, Guorong Wang.
Data curation: Li Yu, Guorong Yu, Kai Deng, Guorong Wang.
Formal analysis: Kai Deng.
Methodology: Li Yu, Guorong Yu, Guorong Wang.
Resources: Kai Deng.
Software: Li Yu.
Supervision: Guorong Yu, Guorong Wang.
Writing – original draft: Li Yu.
Writing – review & editing: Li Yu, Guorong Wang.
Supplementary Material
Supplementary Material
Footnotes
Abbreviations: LLD = leg length discrepancy, MAD = mechanical axis deviation.
The authors report no conflicts of interest.
Supplemental Digital Content is available for this article.
References
- [1].Fernandez-Palazzi F, Bendahan J, Rivas S. Congenital deficiency of the tibia: a report on 22 cases. J Pediatr Orthop B 1998;7:298–302. Review. [DOI] [PubMed] [Google Scholar]
- [2].Kalamchi A, Dawe RV. Congenital deficiency of the tibia. J Bone Joint Surg Br 1985;67:581–4. [DOI] [PubMed] [Google Scholar]
- [3].Hosny GA. Treatment of tibial hemimelia without amputation: preliminary report. J Pediatr Orthop B 2005;14:250–5. [DOI] [PubMed] [Google Scholar]
- [4].Balci Hİ, Sağlam Y, Bilgili F, et al. Preliminary report on amputation versus reconstruction in treatment of tibial hemimelia. Acta Orthop Traumatol Turc 2015;49:627–33. doi: 10.3944/AOTT.2015.15.0005. [DOI] [PubMed] [Google Scholar]
- [5].Jones D, Barnes J, Lloyd-Roberts GC. Congenital aplasia and dysplasia of the tibia with intact fibula. Classification and management. J Bone Joint Surg Br 1978;60:31–9. [DOI] [PubMed] [Google Scholar]
- [6].Weber M. New classification and score for tibial hemimelia. J Child Orthop 2008;2:169–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Paley D. Tibial hemimelia: new classification and reconstructive options. J Child Orthop 2016;10:529–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Wada A, Nakamura T, Urano N, et al. Foot centralization for tibial hemimelia. J Pediatr Orthop B 2015;24:147–53. doi: 10.1097/BPB.0000000000000149. [DOI] [PubMed] [Google Scholar]
- [9].Brown FW. Construction of a knee joint in congenital total absence of the tibia (paraxial hemimelia tibia): a preliminary report. J Bone Joint Surg Am 1965;47:695–704. [PubMed] [Google Scholar]
- [10].Shrivastava S, Nawghare S, Dulani R, et al. A rare variant of tibial hemimelia and its treatment. J Pediatr Orthop B 2009;18:220–4. doi: 10.1097/BPB.0b013e32832e4737. [DOI] [PubMed] [Google Scholar]
- [11].Schwechter EM, Swan KG. Raoul Hoffmann and his external fixator. J Bone Joint Surg Am 2007;89:672–8. [DOI] [PubMed] [Google Scholar]
- [12].Pejin Z. Femoral lengthening in children and adolescents. Orthop Traumatol Surg Res 2017;103(1S):S143–9. doi: 10.1016/j.otsr.2016.05.020. Epub 2017 Jan 16. Review. [DOI] [PubMed] [Google Scholar]
- [13].Yun AG, Severino R, Reinker K. Attempted limb lengthenings beyond twenty percent of the initial bone length: results and complications. J Pediatr Orthop 2000;20:151–9. [PubMed] [Google Scholar]
- [14].Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res 1990;250:81–104. [PubMed] [Google Scholar]
- [15].Cavadas PC, Thione A, Pérez-García A, et al. Microsurgical knee reconstruction in a type IA tibial hemimelia. J Plast Reconstr Aesthet Surg 2015;68:e63–66. doi: 10.1016/j.bjps.2014.12.018. Epub 2014 Dec 24. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.