

Abstract
Maxillary lateral incisors are most common teeth to be found missing. They also are the most common teeth that need esthetic replacement. A 23-year-old female patient with missing maxillary lateral incisors was treated orthodontically: laterals were replaced with implants. Challenges while doing this case are discussed in the following case report.
Key words: Congenitally missing laterals, Interdisciplinary orthodontics, Implants
Introduction
Missing maxillary lateral incisor, being in the esthetic region needs multidisciplinary approach; even if they are missing unilaterally or bilaterally.1 In this situation one treatment option is to open space for the prosthetic replacement of the missing lateral incisor and other is to close the space and use canine as substitution. Whether to close the space or to open the space for replacing missing lateral incisor depends on many parameters like; type of malocclusion, facial type, arch length tooth size discrepancy, smile line, canine morphology, ridge thickness, and finally patient’s expectation from the treatment and cooperation for the treatment are of utmost importance.2
Congenitally missing teeth affect jaw growth. Woodworth et al. stated that patients with bilateral congenital absence of maxillary lateral incisors showed a Class III tendency and the upper and lower anterior and posterior face heights were significantly less than normal.3 Kreczi et al. also found connection between agenesis of teeth and sagittal development of jaw. Reduction of the lower anterior facial height, retrognathism of jaw and increased overbite were most consistent findings.4
In case of unilateral tooth agenesis, space opening is often preferred to improve the aesthetics of patients and preserve smile symmetry. On the other hand, in case of bilateral agenesis, space closure and space opening both are possible.5-8 For crowded arches space closure is more appropriate but for spaced dentition, opening the space and replacing it with prosthesis is advisable. Space opening and prosthetic replacement is better in toothy smile. Gingival margin contouring should also be done if patient has gummy smile.1
Occlusal relationship of anteriors should be taken into account. Decreased overjet and increased overbite will be improved by space opening mechanics, while increased overjet and decreased overbite may benefit from space closure.2 Patients having arch length tooth size discrepancy can be evaluated by Bolton’s analysis for determining space required to replace laterals.9 In arches with class II malocclusion and crowding with slightly convex or straight profile, space can be closed and canines can be substituted as laterals.10 But in cases with class I or III pattern, low angle, reduced overjet and deep bite, opening the space for replacing lateral incisors is advisable. This replacement can be with implant retained crown or prosthetic bridge.2 Case discussed here show underdeveloped maxilla and mandible, presenting clinically as reduced overjet and increased overbite. After patient’s consent, treatment plan of opening the space and filing it with prosthetic replacement for congenitally missing lateral incisors was decided. Canine substitution was not possible in this case as patient was having reduced maxillary jaw length, class III facial pattern, low FMA angle and reduced overjet (Figure 1).
Figure 1.
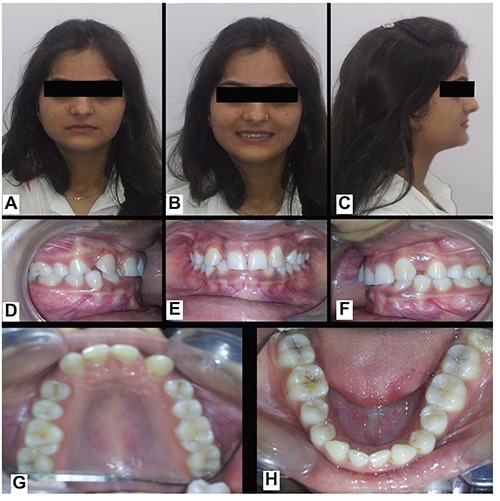
Pre-treatment photographs. (A) extraoral front view; (B) extraoral smiling view; (C) extraoral profile view; (D) right lateral view of dentition; (E) in occlusion front view of dentition; (F) left lateral view of dentition; (G) occlusal view of maxillary arch; (H) occlusal view of mandibular arch.
Considering patient’s age (23 years) and longevity of prosthetic replacement, implant supported crown was advised by implantologist. For implant retained crown Savarrio et al. has given few factors which help in preparation of implant site. These factors are: smile line and gingival contour, height and width of bone at the implant site, radiographic assessment of bone quality, volume and anatomy, interocclusal space, root position of the teeth adjacent to the implant site, local gingival thickness and architecture, width, and form of the adjacent teeth, amount of incisal wear of the adjacent teeth, presence of parafunctional activity and occlusal forces, probing depths and marginal gingival position in relation to the cementoenamel junction.1
In many ways this case was difficult to finish. As interdental, interocclusal and interradicular spaces were less than needed and it was challenge for our team. Creating space faciolingually is easy with ridge augmentation. But creating interradicular space was tough with less tooth material and small jaw sizes.
Case Report
Diagnosis and treatment planning
A 23-year-old female patient came with a chief complaint of gap in front teeth. On examination, it was discovered that her both upper and lower lateral incisors were congenitally missing bilaterally. According to a literature review by Rakhshan, prevalence of congenitally missing teeth in both the arches is negligible.11,12 In the previous researches, it was found that absence of maxillary lateral incisors may be only one manifestation of a complex, multifactorial, craniofacial anomaly.13 It has been reported that the absence of lateral incisors may include a higher incidence of absence of other teeth, more frequent impactions, and tooth size discrepancies in both arches.14 In the case shown here, no other craniofacial anomaly was found on examination. Patient’s lower two incisors (31 and 41) and upper right third molar (18) were missing along with upper lateral incisors. Remaining three third molars (i.e. 28, 38 and 48) were partially impacted. Both jaws were retrognathic and decreased in length on cephalometric evaluation. Though patient was having Angle’s class I molar relationship, she was having low angle pattern, short facial type and horizontal growth pattern on cephalometric analysis, decreased overjet and deep bite intraorally.
Leveling and aligning of both upper and lower arches, bite opening and space opening for missing lateral incisor was the treatment plan decided. Patient agreed for implant supported crown for lateral incisor. So to create space for implant fixture was added in treatment objectives.
Teeth were bonded with 022” MBT prescription orthodontic fixed appliance. Leveling and aligning was achieved with 0.016” Niti followed by 0.019 X 0.025” NiTi wire. Space was created for upper lateral incisors by retraction of canines and slight protraction of incisors. Space analysis showed decreased arch length as both upper and lower jaws were having reduced length. Open coil spring was given to open the space between canines and central incisors bilaterally.
Treatment progress
Because of small jaw size, space opening seemed difficult. Proximal stripping of total 2 mm with canine, first premolar and second premolar was planned and carried out. For caries prevention fluoride application was done. Spaces created by proximal stripping were closed with elastomeric chain on round 0.018” Stainless steel archwire. Slight torque to central incisors was given with 0.019 X 0.025” TMA wire. As mentioned above, one of the goals of ortho dontic treatment was to achieve sufficient bone between the roots to place the implant. For implant placement at lateral incisor place, interradicular space of at least 6-8 mm, facio-lingually 6 mm of ridge thickness and 10 mm of gingivo-incisal length of bone is needed.6 Torquing central incisors and proximal stripping gave enough space for implant placement. It was confirmed on cone beam computed tomography.
As ridge at bilaterally missing maxillary lateral incisors was narrow mesiodistally, decision was made to use a narrow diameter one piece, one stage implant. We used a 2.5 mm diameter and 13 mm length (Osstem implants) on both sides. Initial loading torque was of 35 Ncm and restored with provisional restoration after initial stability. After six months, once the implant was integrated and biological stability was achieved, permanent restorations cemented by zirconia crowns (Figure 2). Follow up was done in 1 month, six months and one year. In the last follow up visit after one year of loading implants everything was fine.
Figure 2.

Post-treatment photographs. (A) extraoral front view; (B) extraoral smiling view; (C) extraoral profile view; (D) right lateral view of dentition; (E) in occlusion front view of dentition; (F) left lateral view of dentition; (G) occlusal view of maxillary arch; (H) occlusal view of mandibular arch.
Discussion and Conclusions
Missing maxillary lateral incisors is most prevalent, costly and challenging dental anomaly. Missing tooth or teeth from esthetic region negatively affect patients’ confidence, social behavior, professional performance, and quality of life.12 So such patients need to be treated with careful management with multidisciplinary perspective. Desirable treatment results can be achieved with teamwork and patient’s compliance. 9 In the given case report, all treatment objectives were achieved. Molar and canine were settled in class I relationship with acceptable overjet and overbite relationship. Spaces opened to replace missing lateral incisors were substituted by implants. Implants do not need any alteration or removal of natural tooth material, so they are most conservative prosthetic replacement for missing teeth. Seeing the age of patient, implants were best option to maintain alveolar ridge and gingival health in esthetic area.
The results achieved were maintained during the retention period by means of a fixed 13 to 23 lingual retainer. Occlusal relationship and dental alignment were stable after one year follow up.
Funding Statement
Funding: none.
References
- 1.Savarrio L, McIntyre G. To open or to close space – that is the missing lateral incisor question. Dental Update 2005;32:16-25. [DOI] [PubMed] [Google Scholar]
- 2.Paduano S, Cioffi I, Rongo R, et al. Orthodontic management of congenitally missing maxillary lateral incisors: a case report. Case Rep Dentistry 2014: 731074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yuksel S, Ucem T. The effect of tooth agenesis on dentofacial structures. Eur J Orthod 1997;19:71-8. [DOI] [PubMed] [Google Scholar]
- 4.Kreczi A, Proff P, Reicheneder C, Faltermeier A. Effects of hypodontia on craniofacial structures and mandibular growth pattern. Head & Face Med 2011;7:23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rosa M, Zachrisson B. The space-closure alternative for missing maxillary lateral incisors: an update. J Clin Orthod 2010;44:540-61. [PubMed] [Google Scholar]
- 6.Richardson G, Russell K. Congenitally missing maxillary lateral incisors and orthodontic treatment considerations for the single-tooth implant. J Can Dent Assoc 2001;67:25-8. [PubMed] [Google Scholar]
- 7.Millar B, Taylor N. Lateral thinking: the management of missing upper lateral incisors. Br Dent J 1995;179:99-106. [DOI] [PubMed] [Google Scholar]
- 8.Argyropoulos E, Payne G. Techniques for improving orthodontic results in the treatment of missing maxillary lateral incisors – a case report with literature review. Am J Orthod 1988;94:150-65. [DOI] [PubMed] [Google Scholar]
- 9.Schmidt J. Treatment considerations for the congenitally missing maxillary lateral incisor. DE’s Breakthrough Clinical with Stacy Simmons Newsletter. 2015, 7th May. Available from: https://www.dentistryiq.com/articles/2015/05/treatment-considerations-for-thecongenitally-missing-maxillary-lateralincisor.html [Google Scholar]
- 10.Kokich V, Kinzer G. Managing congenitally missing lateral incisors, part 1: canine substitution. J Esthet Restor Dent 2005;17:1-6. [DOI] [PubMed] [Google Scholar]
- 11.Balshi T. Osseointegration and orthodontics: modern treatment for congenitally missing teeth. Int J Periodont Restor Dent 1993;13:495-5. [PubMed] [Google Scholar]
- 12.Rakhshan V. Congenitally missing teeth (hypodontia): a review of the literature concerning the etiology, prevalence, risk factors, patterns and treatment. Dent Res J 2015;12:1-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bot PL, Salmon D. Congenital defects of the upper lateral incisors (ULI): condition and measurements of the other teeth, measurements of the superior arch, head and face. Am J Phys Anthropol 1977;46:213-43. [DOI] [PubMed] [Google Scholar]
- 14.Ambekar A, Kangane S, Savant S, et al. Management of congenital missing unilateral maxillary lateral incisor treated with Begg’s mechanotherapy: a case report. IOSR J Dent and Med Sci 2015;14:7-10. [Google Scholar]