

Abstract
Objective
To determine if ethnic disparities exist with regard to the risk of injury and injury outcomes among elderly hospitalized casualties in Israel.
Methods
A retrospective study based on data from the Israeli National Trauma Registry between 2008 and 2017. Data included demographic, injury and hospitalization characteristics. Descriptive statistics and adjusted logistic regression were used to examine the differences between Jewish and Arab casualties, aged 65 and older.
Result
The study included 96,795 casualties. The proportion of elderly hospitalized casualties was 2.8 times greater than their proportion in the population (3.1 times greater among Jews and 2.1 times among Arabs). In comparison to Arabs, Jews suffered from a greater percentage of head injuries (10.5 and 8.9%, respectively for Jews and Arabs p < .001), but fewer extremity injuries (46.7% vs. 48.0% respectively for Jews and Arabs p < .05). Among severe/critical casualties and among casualties with severe head injuries, Arabs were more likely to be transported to the hospital in a private car (27% vs. 21% respectively for Arabs and Jews p < .001; 30.5% vs. 23.3% respectively for Arabs and Jews p < .001). Logistic regression analysis, adjusted for age, gender, injury severity, type of injury, type of trauma center and year of admission, shows that Jews, relative to Arabs, were more likely to be hospitalized for more than seven days, admitted to the intensive care unit (ICU) and to be discharged to a rehabilitation center (OR: 1.3, 1.3 and 2.4 respectively). No differences regarding surgery (OR: 0.95) or in-hospital mortality (OR: 0.99) were found.
Conclusions
Ethnic disparities between Jewish and Arab hospitalized casualties were observed with regard to hospital stay, ICU admission and rehabilitation transfer. However, no differences were found with regard to mortality and surgery. While the reported disparities may be due in part by cultural differences and accessibility, health policy decision makers should aim to reduce the gaps by optimizing the accessibility of ambulance and rehabilitation services as well as increasing awareness regarding the availability of these medical services among the Arab population.
Keywords: Injury, Seniors, Minority, Hospitalization, Rehabilitation
Introduction
The elderly population continues to expand, resulting in a greater number of geriatric patients being at risk for injury [1]. The increase of traumatic events involving the geriatric population is due to longer life expectancy, increasing activity and mobility, and a progressive improvement in quality of life [2]. In comparison to younger patients, outcomes following injury are significantly worse among the geriatric population, resulting in disproportionate healthcare utilization and expenditures. Disparities in the risk of injury and health outcomes between ethnic groups have been demonstrated in a number of countries around the world. Minority ethnic groups are often at higher risk than the majority of the population [3–8]. A recent study from the United States has demonstrated that trauma casualties among minority populations are clustered in hospitals with higher than expected mortality [9]. While injury research studying ethnic disparities has focused on the younger population, research of ethnic disparities among the elderly is lacking [10]. In addition, research among the non-American trauma patient population has been limited [11].
The majority of the elderly population in Israel is Jewish (79.3%) with an Arab minority (20.7%). Jews and Arabs differ in their language, religion, and culture. In comparison to the Jewish population, the Arab population in Israel has lower socioeconomic status, is younger, is more likely to live in rural areas and has a lower life expectancy [12]. Since 1995, Israel has a National Health Insurance Law which provides health-care services for all Israeli residents regardless of religion, ethnicity, and gender. That is to say, Arabs and Jews are equally eligible to receive health services. They are treated in the same hospitals with the same health-care teams [13]. According to the Israeli Central Bureau of Statistics, the proportion of persons aged 65 and above in the entire population will increase from 10.6% at the end of 2013 to 14.6% at the end of 2035 [14, 15]. In the present study persons aged 65 and above are defined as elderly.
The objective of this study is to examine the risk of injury and health outcomes between ethnic groups, among hospitalized casualties, aged 65 and above.
Methods
Data resources
A retrospective study was performed which included all hospitalized casualties, aged 65 and above, who were recorded in the Israeli National Trauma Registry during a ten year period (1 January 2008 through 31 December 2017). During the study period up to 20 trauma centers (of 24 in Israel) participated in the Trauma Registry (all six Level Ι trauma centers and 14 Level ΙΙ trauma centers). All hospitals participating in the registry during the study period were included in the study. The Trauma Registry includes all injured trauma patients with an ICD-9-CM (International Classification of Diseases, Ninth Revision) diagnosis code of 800–959.9 who were hospitalized, including those who died in the emergency department, or discharged to another hospital following injury. The Trauma Registry does not include casualties who died at the scene of the event or on the way to the hospital, persons who were not hospitalized, or who were admitted 72 h or more after the event. All Jewish and Arab citizens of Israel, aged 65 and above, who were hospitalized due to an injury were included in this study. Foreign workers, tourists and unknown ethnicity were excluded (3%).
Data reported in the Registry is recorded by trauma registrars at each trauma center under the supervision of the trauma director and coordinator. Electronic files are transferred to the National Center for Trauma and Emergency Medicine Research, where quality assurance is carried out prior analyzing of data. The data in the Israel Trauma Registry is anonymous. The study received the approval of the ethical committee number 5138-18SMC.
Measurements
The Registry includes demographic information, injury characteristics, hospital utilization, and disposition of each injured hospitalized patient. Ethnicity was categorized as Jews and Arabs. Injury Severity Score (ISS) was classified; 1–8 (minor), 9–14 (moderate), 16–24 (severe) and 25–75 (critical). Hospital length of stay (LOS) was categorized as < 7 and ≥ 7 days and admissions to the intensive care unit (ICU) were categorized as 0 and ≥ 1 days.
Statistical analysis
SAS statistical software was used for data analysis and for comparison between the two ethnic groups. Statistical analysis included conventional tests such as χ2-tests and Fischer’s exact test for categorical data. The prevalence of injury hospitalization per 100 citizens was calculated among Jews and Arabs. Population size in each age group was based on the Israel Central Bureau of Statistics [15].
Multivariate logistic regression analysis was performed to calculate the odds of Jews relative to Arabs (odds ratios), undergoing surgical procedures, hospital LOS (cut-off ≥7), ICU stay, rehabilitation transfer and death; adjusted for age, gender, ISS and year of admission. Possible interactive effects were assessed for each model. A value of p < .05 was considered to be statistically significant.
Results
Prevalence of hospitalization due to injury
Between 2008 and 2017, 96,795 casualties, aged 65 and above, were hospitalized due to injury, representing 28.0% of all casualties in the registry (38.7% among Jews and 9.5% among Arabs). The overall prevalence of hospitalization due to injury among ages 65 and above was approximately 12.5 per 1000 citizens (based on the Central Bureau of Statistics, population distribution in 2016). Among Arabs the prevalence was greater (13.4/1000) than among Jews (12.4/1000) (Table 1). Since the age distribution between Jews and Arabs differs, we calculated the prevalence by age group for each population group (Table 2). In 2016, the prevalence of hospitalization due to injury for ages 65–79 was higher among Arabs compared to Jews, (p < .05) with no significant differences among the age group 80+ (Fig. 1). The proportion of hospitalized casualties aged 65 and above (31.0%) was 2.8 times greater than their proportion in the population (11.2%). The proportion of hospitalized elderly Arabs increased significantly during the study period, from 7.3% in 2008 to 10.4% in 2017 (Fig. 2).
Table 1.
Population, number and percent of hospitalized casualties age 65+ by ethnicity, in 2016
| Total | Jews | Arabs | |
|---|---|---|---|
| Population | |||
| Total | 8,546,000 | 6,768,500 | 1,775,000 |
| Age 65+ | 958,600 | 879,100 | 79,600 |
| Percent from the entire population | 11.2% | 13.0% | 4.5% |
| Hospitalized casualties | |||
| Total | 38,546 | 27,434 | 11,112 |
| Age 65+ | 11,967 | 10,897 | 1070 |
| Percent from the entire hospitalized casualties1 | 31.0% | 39.7% | 9.6% |
| Rate per 1000 population2 | 12.5 | 12.4 | 13.4 |
1Calculation was based on: (Number of hospitalized casualyties Age 65+/ Number of hospitalized casualties) *100
2Calculation was based on: (Number of hospitalized casualties Age 65+/ Number of population age 65+) *1000
Table 2.
Characteristics of hospitalized casualties aged 65+ by ethnicity, 2008–2017
| Total | Jews | Arab | p-value | |
|---|---|---|---|---|
| Total | 96,795 (100%) | 88,836 (91.8%) | 7959 (8.2%) | |
| Gender | ||||
| Female | 63.7 | 64.4 | 55.9 | <.0001 |
| Age | ||||
| 65–74 | 27.8 | 26.1 | 46.8 | <.0001 |
| 75–84 | 40.6 | 41.0 | 36.8 | |
| 85+ | 31.6 | 32.9 | 16.4 | |
Fig. 1.
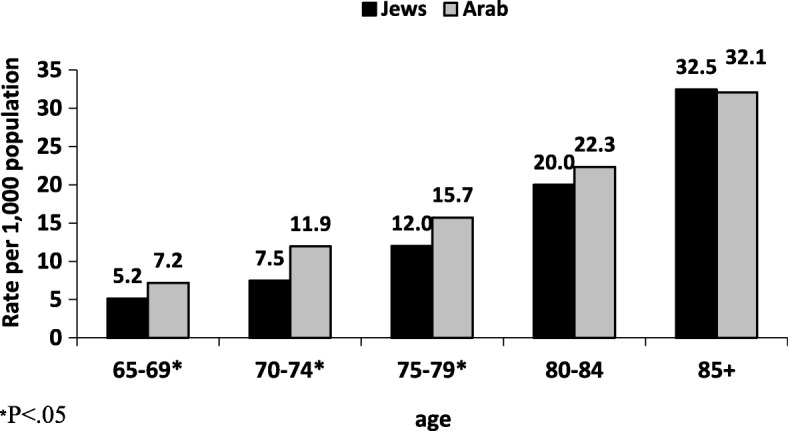
Prevalence of injury hospitalization per 1000 citizens, within each age group by ethnicity, in 2016
Fig. 2.

Hospitalized casualties aged 65+ by ethnicity, 2008–2017. Mantel-Haenszel chi-squre p.value<.0001
Population characteristics
Arab elderly represent 8.2% of elderly hospitalized casualties and 8.1% of severe/critical injuries. A higher percentage of hospitalizations were reported among Jewish women, in comparison to Arab women (64.4% vs. 55.9%, respectively, p < .0001). The Jewish population in Israel is older than the Arab population and similarly, the hospitalized casualties were older; casualties aged 75 and above constitute 73.9% of the Jewish casualties compared to 53.2% among Arab casualties (p < .0001). Jews, compared to Arabs, had a higher percentage of head injuries (10.5% vs. 8.9% respectively p < .001), but suffered from fewer lower extremity injuries, with the most significant difference being among the very old, aged 85+ (56.6% vs. 67.2% respectively for Jews and Arabs p < .001) (Table 3).
Table 3.
Characteristics of hospitalized casualties aged 65+ by ethnicity and age group, 2008–2017
| Total | Ages 65–74 | Ages 75–84 | Ages 85+ | |||||
|---|---|---|---|---|---|---|---|---|
| Jew N = 88,836 |
Arab N = 7959 |
Jew n = 23,198 |
Arab n = 3725 |
Jew n = 36,374 |
Arab n = 2928 |
Jew n = 29,264 |
Arab n = 1306 |
|
| Cause of injury | ||||||||
| Road accidents | 9.2*** | 10.8 | 17.5*** | 14.7 | 8.7*** | 9.0 | 3.3 | 3.9 |
| Falls | 86.8 | 82.0 | 74.1 | 74.1 | 88.2 | 86.6 | 95.0 | 94.3 |
| Othera | 4.0 | 7.2 | 8.4 | 11.2 | 3.1 | 4.4 | 1.7 | 1.8 |
| ISS | ||||||||
| Mild | 36.5 | 36.8 | 47.7* | 47.0 | 35.1*** | 30.2 | 29.6*** | 22.5 |
| Moderate | 54.0 | 53.9 | 41.9 | 43.7 | 55.2 | 59.2 | 62.0 | 71.0 |
| Severe & Critical | 9.5 | 9.3 | 10.4 | 9.3 | 9.7 | 10.6 | 8.4 | 6.5 |
| Injured body region (AIS3+) | ||||||||
| Head | 10.5*** | 8.9 | 10.4*** | 8.4 | 11.2 | 10.3 | 9.8** | 7.3 |
| Face | 0.1 | 0.1 | 0.3 | 0.1 | 0.1 | 0.03 | 0.1 | 0.1 |
| Thorax | 3.8*** | 4.6 | 5.8 | 5.9 | 3.6 | 4.0 | 2.6 | 2.4 |
| Abdomen | 0.7 | 0.8 | 1.0 | 0.8 | 0.6* | 1.0 | 0.4 | 0.3 |
| Spine | 0.9 | 0.8 | 1.3 | 1.0 | 0.9 | 0.7 | 0.7 | 0.6 |
| Upper extremity | 2.5** | 2.0 | 4.1*** | 2.6 | 2.4* | 1.6 | 1.4 | 1.1 |
| Lower extremity | 46.7* | 48.0 | 32.2*** | 36.3 | 47.9*** | 54.4 | 56.6*** | 67.2 |
| ICU (1+ days) | 5.3*** | 6.2 | 6.0 | 5.9 | 5.5** | 6.9 | 4.5 | 5.4 |
| Undergone surgery | 53.1*** | 55.0 | 50.3 | 49.7 | 53.0*** | 58.2 | 55.5 | 62.9 |
| LOS (7+ days) | 36.5*** | 29.4 | 29.9*** | 26.4 | 37.2*** | 32.5 | 40.8*** | 31.3 |
| Rehabilitation | 34.7*** | 18.0 | 24.7*** | 14.9 | 37.2*** | 20.6 | 39.4*** | 21.0 |
| Inpatient mortality | 3.2* | 2.7 | 1.8 | 1.7 | 2.9* | 3.6 | 4.5* | 3.4 |
aOther include: burns, violence and unintentional injury
ISS Injury Severity Score, AIS Abbreviated injury score, ICU Intensive Care Unit, LOS Length of Stay in hospital
*p < .05 **p < .01 ***p < .001
Fall injuries
Falls were the leading cause of injury among elderly casualties, constituting 86.8% of the hospitalizations among Jews and 82.0% among Arab casualties. Age stratified results showed that among elderly aged 75–84, a greater percentage of Jews were hospitalized with a fall injury in comparison to Arabs (88.2% vs 86.6% respectively) (Table 3). The majority of falls, 78.6% among Jews and 72.5% among Arabs, occurred on a level surface, p < .0001. While ground level falls were more frequent among Jews, falls from height were more frequent among Arabs compared to Jews (22.8% vs. 17.9%, respectively, p < .0001). Among casualties hospitalized due to a fall, extremities were the most common part of the body injured, 70.7% of the casualties sustained extremities injuries, in both ethnic groups.
Road traffic injuries
Road traffic injuries (RTI) constituted 9.2% of the hospitalizations among Jewish casualties compared to 10.8% among Arab casualties, p < .0001. Among elderly, aged 65–74, Jews were more likely than Arabs to be hospitalized due to a RTI (17.5% vs. 14.7% respectively for Jews and Arabs). In contrast, among elderly ages 75 and above the percentage of hospitalized Arabs due to a RTI was greater (Table 3). Among traffic related casualties, pedestrians were at greatest risk with Jews sustaining more pedestrian related injuries than Arabs (40.7% vs. 32.5%, p < .001). Among Arabs, the proportion of vehicle driver casualties was 1.6 times greater in comparison to Jews (34.8% vs. 21.5%, p < .001). Although Arab age 65 and above represent about 5% of the Arab population, among driver casualties they represent 14.6%. Only among vehicle drivers Arabs casualties had more severe and critical injuries (ISS 16+) compared to Jews (24.8% vs. 19.5% respectively, p = 0.04).
Utilization of resources and discharge
Among severe/critical casualties and among casualties with severe head injuries, Arabs were more likely than Jews to be transported to the hospital by private car (27.3% vs. 21.1% respectively p < .001; 30.5% vs. 23.3% respectively p < .001), Data not presented. Over half of casualties underwent surgery, in both ethnic groups. Jews, compared to Arabs, underwent more head surgeries (2.0% vs. 1.2% respectively, p < .0001). Multivariate regression analyses, adjusted to age, gender, ISS type of injury, type of trauma center and year of hospitalization, were used to explore the effect of ethnicity on hospitalization characteristics and inpatient mortality (Table 4). The odds of being admitted to the ICU and being hospitalized for more than a week was greater for Jewish elderly compared with Arab elderly (OR 1.3 95%CI 1.192–1.326) However, it should be noted that differences in ICU admissions and LOS were found only among casualties not diagnosed with a head injury. Among elderly suffering from a head injury, no differences in ICU admissions or LOS were found between the two ethnic groups. Jews were 2.4 more likely to be discharged to a rehabilitation center in comparison to Arabs (2.4 OR 95%CI 2.224–2.525). There was no significant difference between the two ethnic groups in undergoing overall surgical procedures and inpatient mortality.
Table 4.
Odds Ratio (OR) of Jews relative to Arabs by hospitalization characteristics and inpatient mortality; 2008–2017
| Model | dependent variable | ORa (Jews/Arabs) | 95% Confidence intervals | p-value |
|---|---|---|---|---|
| 1 | Surgery | 0.95 | 0.896–1.007 | .086 |
| 2 | ICU | 1.27 | 1.140–1.422 | <.0001 |
| 3 | LOS 7+ | 1.26 | 1.192–1.326 | < .0001 |
| 4 | Rehabilitation | 2.37 | 2.224–2.525 | < .0001 |
| 5 | Mortality | 0.99 | 0.854–1.149 | .902 |
aAdjusted for age (continuous variable), gender, Injury severity score - 3 groups (1–8, 9–14, 16–75), type of injury, type of trauma center and year of hospitalization for all models
ICU Intensive Care Unit, LOS Length of Stay in hospital
Discussion
The present study not only characterizes injuries and hospital resource utilization among elderly casualties during the last decade in Israel, but also focuses on the differences between Jews and Arabs. The results show that the proportion of hospitalized casualties aged 65 and above among all hospitalized casualties was 2.8 times greater than their proportion in the overall Israeli population. The data presented illustrates the similarities and differences between Jews and Arabs regarding injury related hospitalizations. No significant differences between the two ethnic groups were found with regard to mortality or undergoing surgery. However, Jews, in comparison to Arabs, were more likely to have longer hospital stays,, to be admitted to the ICU and to be discharged to a rehabilitation center. Our results are in partial discrepancy with other international findings which find that there are disparities in the risk of injury and health outcomes between ethnic groups [3, 5–8, 16].These disparities may be attributed to cultural, safety and behavioral differences [17].
It was found that the disparities in the risk of hospitalization due to injury between Jews and Arabs are age-dependent. The risk of injury related hospitalizations was greater among Arabs compared to Jews, up to age 79. Previous research, which studied the relationship between socio-economic status and injury in Israel, found that in every socioeconomic cluster, the risk of hospitalization due to injury is higher among Arabs compared to Jews, even after adjusting for age [18]. While the Arab elderly are much younger than the Jewish elderly, they are more disabled [19]. The percentage of Arab elderly who are disabled and need help with activities of daily living is twofold that of Jewish elderly (30% vs. 14%, respectively). In addition, about one-quarter of the Arab elderly living in the community are homebound, compared to 12% among Jewish elderly [19].
Hicks et al. [10] documented that disparities in survival after injury exist between white and black patients depending on their age group. Younger white patients have better outcomes after injury than younger black patients, while older black patients have better outcomes than older white patients. Commonly posited explanation for these age-dependent disparities is the insurance status, availability of Medicare, and consequently, better access to pre injury medical care, in the older population. However, in Israel the National Health Insurance Law provides health-care services for all Israeli residents regardless of religion, ethnicity, and gender. Therefore, Arabs and Jews are equally eligible to receive health services.
Although the proportion of Arabs among elderly drivers (65+) in Israel is only 4.5% [20], we found that they represent 14.6% of vehicle drivers hospitalized due to road accidents. In addition, one in three elderly Arab vehicle drivers who were hospitalized due to a RTI suffered severe/critical injuries. These findings can be attributed to low quality of road infrastructure in Arab villages and towns, inadequate safety behaviors, and unlawful driving. Not only is road infrastructure inferior in Arab towns, but Arabs are more likely to drive in older vehicles and refrain from using safety accessories, such as seatbelts. [21, 22].
In our study several differences between Jewish and Arab elderly casualties were reported. Most notably, Arabs, in comparison to Jews, were far less likely to be discharged to a rehabilitation center (OR = 2.4). Other previous studies support our results that ethnic minorities are less likely to utilize rehabilitation facilities compared to the ethnic majority [3, 5]. For example, in the United States [5], ethnic minority patients are less likely to be placed in rehabilitation than non- Hispanic white patients, even after accounting for insurance status, suggesting existence of systematic inequalities in access. In addition, our previous study which compared Jewish and Arab children showed that Jewish casualties were more likely to be discharged to rehabilitation facilities than Arabs [3]. This fact can be attributed to various causes; including accessibility, culture and language. Residents living in the Northern district of Israel and in Jerusalem were reported to be 3–4 times less likely to receive inpatient rehabilitation compared to those living in the Center district [23]. Fifty percent and 17% of the Arab elderly live in the North district and Jerusalem, respectively, while only 9% live in the Center district [15].
In addition, there are vast differences in family relations and composition; Arab nuclear families in Israel usually occupy several households in the same village, which are proximate to each other. Children and grandchildren abound, and are actively involved in the lives of their parents and grandparents [19]. Arabs in Israel rated their culture as more tolerant toward their elders in comparison to Jews and spend more time with them [24]. In the Arab nuclear family, it is both expected and customary for the elderly to live at home and be cared for by family members Language barriers may also contribute to the differences. While the native language of the Arab population is Arabic, Hebrew is the official language in Israel. Due to communication barriers, elderly Arabs may prefer home care rather than residing in a rehabilitation facility with few Arab speaking professionals.
Another difference is the fact that among Arabs, a relatively high proportion of severe/critical casualties were transported by private car. This could be explained by the lack of ambulance availability in many Arab communities [25]. Moreover, in some of the Arab villages there is no exact address and it is difficult to direct the ambulance driver to a specific location. In addition, even though ambulance costs are often paid by health insurance, ambulance fees may be a deterrent. All of these reasons could contribute to the lack of ambulance use among Arabs.
Health policy decision makers and educators should aim to reduce the gaps between the two ethnic groups with regard to accessibility and availability of rehabilitation and ambulance services, as well as increase awareness regarding the availability and utilization of these pre and post hospital services.
Possible explanations for the differences in length of stay between Jews and Arabs may include geographic location and comorbidity. That is, maybe the longer length of hospital stay is due to preexisting conditions rather than the injury itself. In addition, since Arabs live in the periphery, they often arrive first at a level II trauma center after which are transferred to a Level I Trauma Center. Thus, the LOS may not reflect the total time of hospitalization. However, it should be reminded that among casualties suffering from head injuries, no differences in LOS or ICU were found between Jew and Arabs.
Implementing an in-depth study to explore the reasons contributing to disparities in health care utilization between Jews and Arabs is recommended. The outcomes of such a study will provide policy makers with evidence based data to reduce inequality between population groups.
Minority ethnic groups in the United State have a higher risk of mortality after injury than majority group [8, 9]. For example, African American and Hispanic casualties had higher odds ratio of death (1.17 and 1.47, respectively) compared to whites even after adjustment for demographic and injury severity variables [9]. In contrast, the outcomes of our study showed no significant differences between ethnic groups in inpatient mortality. Non-American studies support our results that ethnicity is not an independent predictor of trauma mortality outcomes [3, 11].
The first limitation of our study is that it includes only hospitalized casualties, as those who were discharged following treatment in the emergency department and those who died at scene of the accident or on the way to the hospital are not included. A second limitation is the lack of data regarding socioeconomic status. However, according to Goldman et al. factors other than socioeconomic differences are the cause for injury disparities between Jews and Arabs. A third limitation is the lack of data regarding distance from the scene of the accident to the hospital [26]. However, the INTR includes method of evacuation and transfer to the hospital, thus providing information regarding prehospital medical treatments.
Conclusions
The outcomes of this study show that injury among the elderly is a burden to the health system. Since differences in injury characteristics, hospital utilization and discharge exist between Jewish and Arab elderly in Israel, it is vital that prevention programs be developed and adapted to meet the needs of each population group. Policy makers should increase the awareness among the Arab community of the available medical and rehabilitation services for the elderly population. In addition, decision makers in public health should use these results to optimize the allocation of pre and post hospital emergency care.
Acknowledgements
The authors wish to thank the Israel Trauma Group for their responsibility for the data completing. The Trauma Group include: H. Bahouth, A. Becker, A. Hadary, I. Jeroukhimov, M. Karawani, B. Kessel, Y. Klein, G. Lin, O. Merin, B. Miklush, Y. Mnouskin, A. Rivkind, G. Shaked, G. Sibak, D. Soffer, M. Stein and M. Wais. H Pharan. I. Garbetzev.
Funding
None.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due hospitalization privacy but are available from the corresponding author on reasonable request.
Financial disclosure
The authors have no financial relationships relevant to this article to disclose.
Potential conflicts of interest
The authors have no conflicts of interest relevant to this article to disclose.
Abbreviations
- ICD
International classification of diseases
- ICU
Intensive care unit
- ISS
Injury severity score
- LOS
Length of stay
- SMC
Sheba medical center
Authors’ contributions
NAR and NY conceived and designed the study, analyzed the data and wrote the manuscript. MST conceived and designed the study, analyzed the data and reviewed and revised the manuscript. IR and KP conceived and designed the study, reviewed and revised the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The research receive the approval of the Sheba medical Center Helsinky committee 5138–18-SMC. The research is based on anonymous registry, there for consent to participant was not mandatory.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Nura Abdel-Rahman, Email: nuranader@gmail.com.
Nechemia Yoffe, Email: maylev90@gmail.com.
Maya Siman-Tov, Phone: 972-3-7731454, Email: mayasi@gertner.health.gov.il.
Irina Radomislensky, Email: irinar@gertner.health.gov.il.
Israel Trauma Group, Email: estish@gertner.health.gov.il
Kobi Peleg, Email: kobip@gertner.health.gov.il.
Israel Trauma Group:
H. Bahouth, A. Becker, A. Hadary, I. Jeroukhimov, M. Karawani, B. Kessel, Y. Klein, G. Lin, O. Merin, B. Miklush, Y. Mnouskin, A. Rivkind, G. Shaked, G. Sibak, D. Soffer, M. Stein, M. Wais, H. Pharan, and I. Garbetzev
References
- 1.Kozar RA, Arbabi S, Stein DM, et al. Injury in the aged: geriatric trauma care at the crossroads. J Trauma Acute Care Surg. 2015;78(6):1197–1209. doi: 10.1097/TA.0000000000000656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kuhne CA, Ruchholtz S, Kaiser GM, Nast-Kolb D. Mortality in severely injured elderly trauma patients--when does age become a risk factor? World J Surg. 2005;29(11):1476–1482. doi: 10.1007/s00268-005-7796-y. [DOI] [PubMed] [Google Scholar]
- 3.Abdel-Rahman N, Siman-Tov M, Israel Trauma Group. Peleg K. Ethnicity and road traffic injuries: differences between Jewish and Arab children in Israel. Ethn Health. 2013;18(4):391–401. doi: 10.1080/13557858.2012.754405. [DOI] [PubMed] [Google Scholar]
- 4.Schoenfeld AJ, Belmont PJ, Jr, See AA, Bader JO, Bono CM. Patient demographics, insurance status, race, and ethnicity as predictors of morbidity and race, and ethnicity as predictors of morbidity and mortality after spine trauma: a study using the National Trauma Data Bank. Spine J. 2013;13(12):1766–1773. doi: 10.1016/j.spinee.2013.03.024. [DOI] [PubMed] [Google Scholar]
- 5.Shafi S, de la Plata CM, Diaz-Arrastia R, et al. Ethnic disparities exist in trauma care. J Trauma. 2007;63:1138–1142. doi: 10.1097/TA.0b013e3181568cd4. [DOI] [PubMed] [Google Scholar]
- 6.Steinbach R, Green J, Edwards P, Grundy C. ‘Race’ or place? Explaining ethnic variations in childhood pedestrian injury rates in London. Health Place. 2010;16(1):34_42. doi: 10.1016/j.healthplace.2009.08.002. [DOI] [PubMed] [Google Scholar]
- 7.Campos-Outcalt D, Bay C, Dellapena A, Cota MK. Motor vehicle crash fatalities by race/ethnicity in Arizona, 1990_96. Injury Prev. 2003;9:251-6. [DOI] [PMC free article] [PubMed]
- 8.Arthur M, Hedges JR, Newgard CD, Diggs BS, Mullins RJ. Racial disparities in mortality among adults hospitalized after injury. Med Care. 2008;46:192–199. doi: 10.1097/MLR.0b013e31815b9d8e. [DOI] [PubMed] [Google Scholar]
- 9.Haider AH, Hashmi ZG, Zafar SN, Hui X, Schneider EB, Efron DT, Haut ER, Cooper LA, MacKenzie EJ, Cornwell EE., 3rd Minority trauma patients tend to cluster at trauma centers with worse-than-expected mortality: can this phenomenon help explain racial disparities in trauma outcomes? Ann Surg. 2013;258(4):572–579. doi: 10.1097/SLA.0b013e3182a50148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hicks CW, Hashmi ZG, Velopulos C, Efron DT, Schneider EB, Haut ER, Cornwell EE, 3rd, Haider AH. Association between race and age in survival after trauma. JAMA Surg. 2014;149(7):642–647. doi: 10.1001/jamasurg.2014.166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Leow JJ, Lim VW, Lingam P, Go KT, Teo LT. Ethnic disparities in trauma mortality outcomes. World J Surg. 2014;38(7):1694–1698. doi: 10.1007/s00268-014-2459-5. [DOI] [PubMed] [Google Scholar]
- 12.Central Bureau of Statistics (CBS). 2011. Statistical Abstract of Israel 2011. Available at: http://www.cbs.gov.il/reader/. Accessed 30 May 2018.
- 13.The National Health Insurance Law. Ministry of Health, Israel. 2012. https://www.health.gov.il/Subjects/UninsuredRights/HealthInsuranceLaw/Pages/default.aspx. Accessed 30 May 2018.
- 14.CBS. 2014. Selected Data for International Senior Citizen's Day http://www.cbs.gov.il/reader/newhodaot/hodaa_template_eng.html?hodaa=201411261. Accessed 10 May 2018.
- 15.CBS. 2017. Jerusalem. Table No. 2.19, population, by population group, religion, age and sex, district and sub-district. https://www.cbs.gov.il/he/subjects/Pages/%D7%90%D7%95%D7%9B%D7%9C%D7%95%D7%A1%D7%99%D7%99%D7%94-%D7%9C%D7%A4%D7%99-%D7%93%D7%AA-%D7%95%D7%A7%D7%91%D7%95%D7%A6%D7%AA-%D7%90%D7%95%D7%9B%D7%9C%D7%95%D7%A1%D7%99%D7%99%D7%94.aspx. Accessed 28 Oct 2018.
- 16.CBS. 2013. Jerusalem. Population, by population group, religion, age and sex, district and sub-district. Table No. 2.19. https://www.cbs.gov.il/he/subjects/Pages/%D7%90%D7%95%D7%9B%D7%9C%D7%95%D7%A1%D7%99%D7%99%D7%94-%D7%9C%D7%A4%D7%99-%D7%93%D7%AA-%D7%95%D7%A7%D7%91%D7%95%D7%A6%D7%AA-%D7%90%D7%95%D7%9B%D7%9C%D7%95%D7%A1%D7%99%D7%99%D7%94.aspx. Accessed 10 May 2018.
- 17.Ageing and Life Course Family and Community Health. World Health Organization. Global report on falls prevention in older age. 2007 http://www.who.int/ageing/publications/Falls_prevention7March.pdf?ua=1. Accessed 10 May 2018.
- 18.Frumkin H, Walker ED, Friedman-Jiménez G. Minority workers and communities. Occup Med. 1999;14(3):495–517. [PubMed] [Google Scholar]
- 19.Goldman S, Radomislensky I, Ziv A, ITG PK. The impact of neighborhood socioeconomic disparities on injury. Int J Public Health. 2018;63:855–863. doi: 10.1007/s00038-018-1119-1. [DOI] [PubMed] [Google Scholar]
- 20.Azaiza F, Brodsky J. The aging of Israel's Arab population: needs, existing responses, and dilemmas in the development of services for a society in transition. Isr Med Assoc J. 2003;5(5):383–386. [PubMed] [Google Scholar]
- 21.CBS. 2013. Jerusalem. Licenced to Drive. Table No. 3, Licenced to Drive, by Population Group, Sex, Age and Type of Vehicle They Are Licenced to Drive. https://www.cbs.gov.il/he/subjects/Pages/%D7%9E%D7%95%D7%A8%D7%A9%D7%99%D7%9D-%D7%9C%D7%A0%D7%94%D7%95%D7%92.aspx. Accessed 10 May 2018.
- 22.Moran M, Baron-Epel O, Assi N. Causes of road accidents as perceived by Arabs in Israel: a qualitative study. Transp Res F. 2010;13:377_387. doi: 10.1016/j.trf.2010.07.001. [DOI] [Google Scholar]
- 23.CBS. 2012. Jerusalem. Table No. 19, Private cars registered in cities by year of production. https://www.cbs.gov.il/he/Statistics/Pages/%D7%9E%D7%97%D7%95%D7%9C%D7%9C%D7%99%D7%9D/%D7%9E%D7%97%D7%95%D7%9C%D7%9C-%D7%A1%D7%93%D7%A8%D7%95%D7%AA.aspx. Accessed 30 May 2018.
- 24.Zucker I, Laxer I, Rasooli I, Han S, Cohen A, Shohat T. Regional gaps in the provision of inpatient rehabilitation services for the elderly in Israel: Results of a national survey. Isr J Health Policy Res. 2013;23(2):27. doi: 10.1186/2045-4015-2-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Peleg, K. 2005. Equality and Availability of Pre-hospital Emergency Services. Beersheva: Taub Center for Social Policy Studies in Israel.
- 26.Champion HR, Sacco WJ, Copes WS. Trauma Scoring. In: Feliciano DV, Moore EE, Mattox KL, editors. Trauma. 3rd ed. Stanford, CT: Appleton & Lange; 1995. p. 53–67.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due hospitalization privacy but are available from the corresponding author on reasonable request.