

Abstract
Background:
Music engagement (the active making of music, e.g., music lessons and ensembles) is a common part of educational and community experiences. Music making typically involves listening to and production of rapidly changing combinations of pitch, timbre, and rhythm, which can be challenging for cochlear implant (CI) recipients, given that pitch and timbre are poorly conveyed through the CI. Pediatric CI users have variable patterns of music engagement, but some have achieved, sustained participation despite the degraded CI signal. What factors contribute to their persistence in these demanding listening situations? Our study examined a cohort of pediatric CI recipients from our center to better understand those perceptual and experiential factors most influential in relation to music engagement.
Method:
Regressions and correlations were run for measures of pitch and speech perception, hearing history, familial involvement in music, personal importance of music, and extent of music engagement (years in music lessons; general involvement in music).
Results:
Pitch ranking accuracy was a significant predictor of sustained participation in music lessons (p=.0019), and sustained involvement in music (p=.0038), as well as performance on CNC words (p=−.0060) and phonemes (p=−.0174). Extent of familial involvement in music at the time of testing was significantly predictive of the user’s musical engagement (p. =.0007). Personal importance of music was not predicted by or significantly correlated with, any of the variables investigated.
Conclusion:
Better pitch perception was associated with sustained involvement in music lessons as well as better speech perception. However, familial involvement in music was of greater impact for sustained music engagement. Judicious choice of musical instrument also influenced persistence. The positive impact of familial involvement indicates that perceptual limitations associated with CI processing do not present insurmountable barriers to music engagement. Because music engagement provides normalizing social involvement and challenging auditory practice, the impact of parental involvement has implications for counseling parents of CI users.
Over the past three decades, considerable research has been conducted regarding pediatric cochlear implant (CI) outcomes related to speech and language. A more modest body of research exists regarding their perception and enjoyment of music. The majority of these studies have enrolled school-aged children (~age 7–17), and most studies focus on perception of structural features (for review see Gfeller, 20161; Trehub, Vongpaisal, Nakata, 20092;Stabej, Smid, Gros, Zargi, Kosir, Vatovec, 2012 3). Pediatric CI users, as a group, have poor pitch and timbre perception compared with normal hearing (NH) peers,1 though individual outcomes are highly variable. Still fewer studies have examined the long-term involvement in music engagement by pediatric CI users who have grown up using electric hearing and who have reached adolescence or young adulthood. Music engagement for purposes of this paper refers to the personal importance of music within one’s life and/or extent of involvement in music making in lessons, ensembles, etc.1,4–6
While research indicates different patterns of musical engagement among pediatric CI users,1,4,5 the influence of various factors on engagement is little understood. Given the degraded representation of musical sounds (especially pitch and timbre) conveyed by CIs, is there a strong relationship between perceptual accuracy, personal importance of music, and active engagement? Do other factors, such as hearing history or familial involvement influence music engagement? This study attempts to answer these questions.
Though CIs have been designed primarily to support speech recognition and language development, music engagement outcomes remain interesting because they provide insights into how effectively CI recipients are able to function during challenging, spectrally complex auditory tasks. This is in part due to the technical characteristics of CIs. Conventional CIs transmit the temporal envelope of the signal; the fine structure of the signal is poorly represented. This signal is sufficient for speech in quiet and for conveyance of rhythmic components of music (e.g., rhythm patterns, tempo, beat), but is much less satisfactory for complex listening like speech in noise and enjoying several key features of music, particularly pitch (see reviews by Looi, et al7 and Limb & Roy 8). Thus, music engagement outcomes provide insights into how effectively CI recipients are able to function in challenging spectrally complex auditory tasks. It is not surprising that as a group, CI users’ pitch and timbre perception is significantly poorer than NH peers.1,4,7–12 Interestingly, there is considerable variability; some CI users have remarkably good pitch perception. Perhaps more surprising is the lack of clear correlations between perception and enjoyment reported in studies of adult CI users.9,11,13 For adult CI users, perceptual accuracy is not a strong predictor of music enjoyment; even less is understood regarding perception and enjoyment in pediatric CI users. Furthermore, generalizations to pediatric populations from adult studies on enjoyment or personal importance of music are problematic given differences in auditory development. Pediatric users’ perception of music has developed largely through electric hearing, while postlingually deaf adults have mapped perception of sounds through a CI onto their memory of the sound of acoustic hearing.1 Still less is understood regarding active making of music, referred to in this paper as music engagement.
Music engagement occurs within an environment of ongoing, rapidly changing, spectrally complex combinations of pitch, timbre, rhythm, and loudness.14 Active music listening and production are arguably more demanding than speech recognition, given the technical characteristics of CIs that present degraded representation of pitch and timbre. Typically, greater precision in listening and production (playing music) are required as students progress from music classes and lessons from elementary to senior high school. Even NH people must practice skills such as matching pitch to other musicians, producing a good tone quality, or making fine pitch changes with finger positions (i.e., playing a violin) or embouchure (i.e., playing a trumpet). However, these tasks are particularly difficult for many CI users. Anyone who has successfully engaged in music ensembles or lessons over many years is likely to have developed impressive capability for responding to complex auditory input.14–16 At present, it is unknown whether pitch perception is a significant predictive factor in music engagement. Better understanding the factors that impact successful navigation of these auditory demands may reveal clinically relevant strategies for overall CI benefit.
Beyond perceptual accuracy, normalization within social and educational experiences is another important aspects of CI use. Studies such as those of Punch and Hyde17 and Wheeler, Archbold, Gregory and Skipp18 have identified various aspects of community and educational settings that contribute to or reduce integration and quality of life; however, engagement in music has been beyond the scope of those articles; little is known. Better understanding of engagement in music is highly relevant to understanding social integration, given that for many NH adolescents, music is a key aspect of social life.19 In fact many NH children participate in music lessons and ensembles as part of typical educational curricula, community experiences, and life enrichment.20 This study examines whether children with CIs partake in these normalizing events that rely so heavily upon audition and whether there are particular factors that facilitate engagement and more complete integration in these life experiences. Better understanding of supportive influences could inform individual educational plans and counseling of CI users and families.
In addition to social integration associated with music engagement, research has suggested there are shared processing requirements for some aspects of speech and music. Neuroscientists speculate music training may have benefits not only for music perception but speech perception as well, at least for NH children.1,15,21–23 This has led to speculation that music training may have therapeutic benefits for children who have communication disorders;22,24 to date, the relationship between music training and speech perception of pediatric CI users is unclear.1,21 Consequently, the relationships between music perception, engagement, and speech perception are of theoretical and clinical interest.
These issues formulate the basis for this study, which examines factors that influence music engagement of pediatric CI users in highly demanding and complex listening experiences that are poorly matched to the technical features of CIs. To better understand the relationship among potentially influential factors, this retrospective examination of a cohort of pediatric CI recipients from our center, was conducted with the primary aim of better understanding the relationship between perceptual and experiential factors and long-term engagement in music. This involved the following three sub-questions:
To what extent does perceptual accuracy for pitch predict active engagement in music and personal importance of music to pediatric CI users?
What are the relationships among demographics (e.g., age, length of CI use, etc.) and experiential factors (familial involvement in music) with music engagement?
What are the relationships between pitch perception, music engagement, and speech perception?
Method
To answer these questions, we completed a retrospective examination of patient records of (a) demographics (e.g., age, gender), (b) hearing history (age of onset, age when implanted, months of CI use), (c) perceptual accuracy for complex pitch ranking,25 (d) questionnaire items examining the role of music within the CI user’s family,26 (e) items from the Iowa Pediatric Music Questionnaire (IPMQ) quantifying engagement in music (music classes, ensembles, etc.), as well as a subset specifying duration and type of musical instrument played (some which have greater demands for pitch perception than others),5 and (f) measures of speech perception (CNC words and phonemes27).
Participants
Participants included 76 pediatric CI users who were enrolled in our center between 1998 and 2017, who were implanted before age 18, and who had reached age 12 by the time of testing for this study. To reflect patterns of persistence in music engagement (e.g., lessons, ensembles, classes), we set a lower age limit of 12 years or older at time of testing. By setting this limit, we hoped to capture ongoing music experiences, such as general music education offered from kindergarten through 6th grade in the United States. Additionally, many music lessons or band programs in U.S. schools begin between the ages of kindergarten (e.g., Suzuki programs) and middle elementary school (around 4th or 5th grade). Persistence in music lessons or ensembles generally involves increasing precision of musical skills; furthermore, involvement in junior high or high school is more likely to involve personal choice as well as parental expectation.26 The range of ages at time of testing was 12.02 to 22.81 years with a mean age of 15.15 years (SD= 2.0).
Participants used the following devices: Cochlear (N=73) [CI22 (21), CI24M (16), Contour/CI24R (11), Freedom (8), CI512 (1), L24 (5), CI422 (1), bilateral combinations-Cochlear (11)]; Advanced Bionics (N=3) [90K]. Signal processing schemes included: SPEAK (24), ACE (48), HiACE (1), HiRes (1), HiRes-S (1), HiRes-P (1). Onset of deafness ranged from congenital to 15.17 years (M= 17.3 months, SD=34.4); 65 had onset before age 3 and 7 had onset > 90 months of age. The age of implantation ranged from 0.9 to 16.1 years (M=6.21, SD= 4.16); 47 were implanted before age 3 and 29 after. Length of CI use ranged from 5.9 to 216.7 months (M=107.2, SD=49.5); 11 of the group used bilateral CIs, while 13 used hearing aids.
As these demographics indicate, the vast majority of the cohort used a Cochlear device, with either SPEAK or ACE processing schemes. MAP parameters varied, but age-appropriate methods were used to establish T- and C-levels. ECAP and ESRT thresholds were used as necessary to corroborate MAP levels. Programming was conducted with an end goal of speech and language development. No special or individualized mapping was used to optimize music perception. Furthermore, prior research with group data has not yet confirmed consistent and predictable improvement in pitch perception as a function of specific programming, consequently, individual variations in MAP parameters were not specifically examined as part of the analyses.7,8
Measures:
Complex Pitch Ranking Test (CPRT).
While various measures can reflect music perception, we focused on perception of pitch because (a) pitch is a particularly salient feature in the melodies and harmonies of western music (required for producing, matching, and tuning, which are important aspects of playing many musical instruments or singing in ensembles), and (b) pitch resolution of CI users is known to be significantly different from that of NH children.1 The threshold for CPRT was collected through an adaptive test in which the individual achieved 75% accuracy over 12 presentations at each interval to determine the smallest interval to accurately conclude which of two tones was higher. The smallest possible pitch change was one semitone (smallest pitch change on the piano and within western musical scales); the largest was 24 semitones—a two-octave pitch change. A smaller threshold indicates better pitch perception.25 Prior studies indicate that CI recipients are not significantly different from NH listeners on perception of rhythm, 8,28,29 consequently rhythm perception was not examined in this study.
Attitudes toward and engagement in music.
Information about personal importance of music (PIM) and active engagement (ME) (e.g., lessons, classes, ensembles) was gathered through two questionnaires completed by the CI user. The Familial Music Engagement Questionnaire (FMEQ) asked pediatric CI users to indicate the PIM in their life (rating 1 to 4). They also answered questions yielding scores of the extent of familial musical involvement while growing up (FAM-GU) and currently—that is, at the time of testing (FAM-C).26 Because most of the CI recipients were prelingually deaf at an age younger than typical enrollment in music instruction, information regarding music instruction prior to CI use was not measured.
The IPMQ quantified music involvement in classes and ensembles over time to yield an overall ME score. A subscale of the ME scores quantified duration of music lesson (DML) (based upon 1-year units). Typically, the longer the DML, the greater the demands for listening to and producing notes in tune with appropriate sound quality, particularly for wind, string, and brass instruments or singing. However, there are differing demands depending upon the instrument played. For example, playing the violin requires ongoing fingering adjustments to play pitches in tune; piano and most percussion instruments do not. To determine the auditory demands of the chosen instrument(s), participants listed the name(s) of instrument(s) they had played, and length of time.5 Persistence in DML over years suggests more effective processing of sound or effective accommodations to overcome challenging listening tasks.
Demographic data.
Demographic and hearing history data included: age at time of testing (AGE-T), onset of deafness (ONSET), age of implantation (AGE-I), and length of device use (LoU).
Speech measures:
Speech measures included the CNC phonemes and CNC words in quiet.27 These were selected because most pediatric CI patients in our center completed these tests during annual visits. Higher scores indicate better speech perception.
Analyses:
Because prior studies have failed to show significant differences in pitch perception based upon specific signal processors or internal arrays1,7,8 and our sample consisted predominately of two particular devices and strategies, we did not evaluate differences based upon those variables.
Using regressions and correlations, we examined the relationships between perceptual accuracy for CPRT, CNC words and phonemes, and the following factors: (a) PIM, (b) FAM-GU and FAM-C, (c) ME, DML, and (e) AGE-T, ONSET, AGE-I, and LoU (in months).
To examine the distribution of outcomes for this sample in relation to CPRT, we divided the sample by tertiles of high (Group 1: 24 to 17 semitones), middle (Group 2: 16 to 9 semitones), and low (Group 3: 8 to 1 semitone) thresholds for pitch ranking. Low thresholds indicate better perception (see figure 1). Unsurprisingly, given prior research on pitch perception of CI users7, the pitch perception did not reflect a normal distribution, thus, the tertiles, which were based upon the CPRT score were not equal in size. We then examined the distribution of the following variables as a function of assigned tertile: PIM (see figure 2); ME (see figure 3); and DML (one year units) (figure 4).
Figure 1.
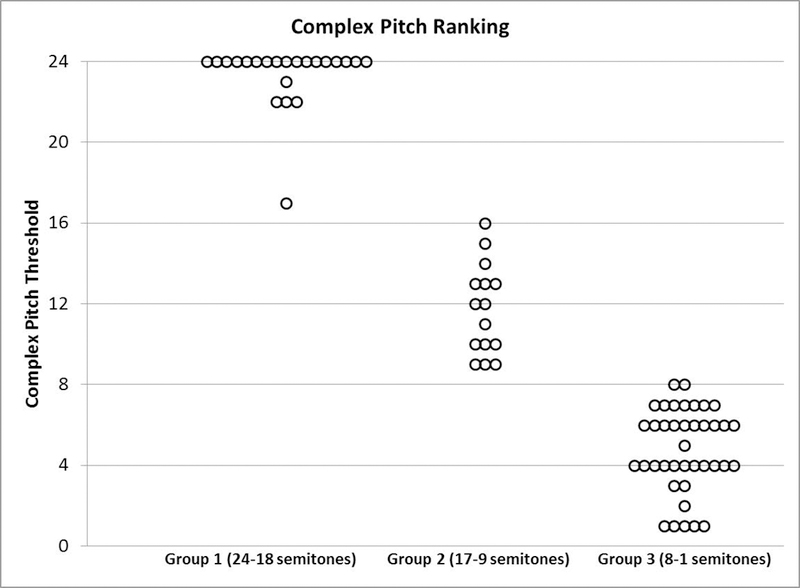
Distribution of CPRT scores by group, where lower scores indicate more accuracy on perception.
Figure 2.
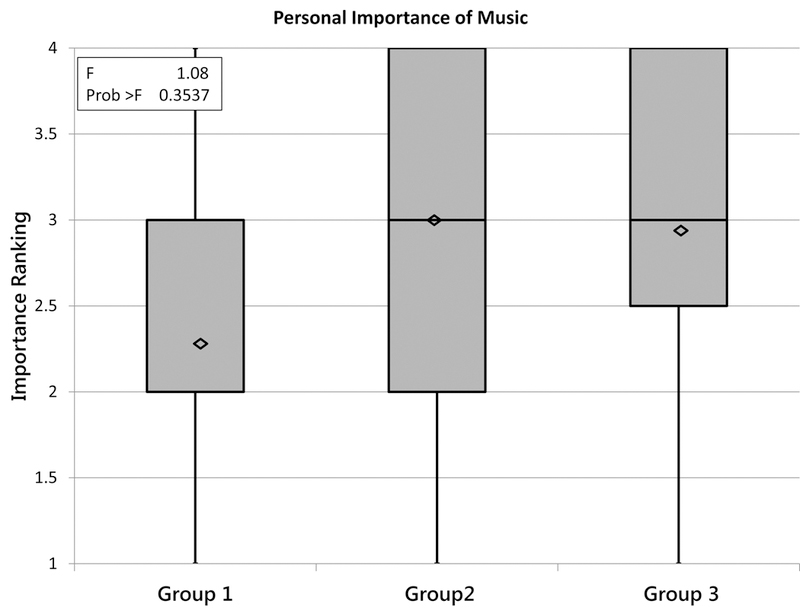
Distribution of Personal Importance of Music (PIM) (ranking 1 to 4) as a function of CPRT group tertile membership. No significant difference was found between the groups.
Figure 3.
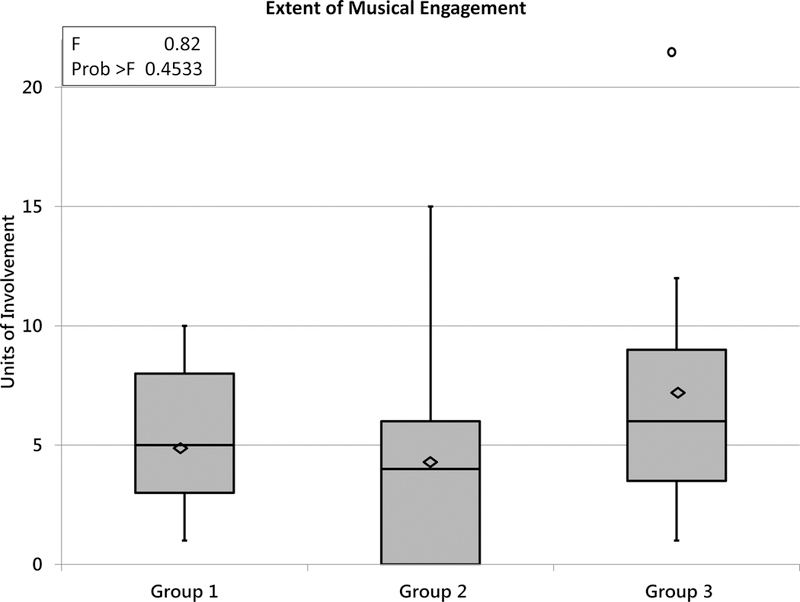
Distribution of total music involvement (ME) as a function of group. No significant difference was found between groups.
Figure 4.
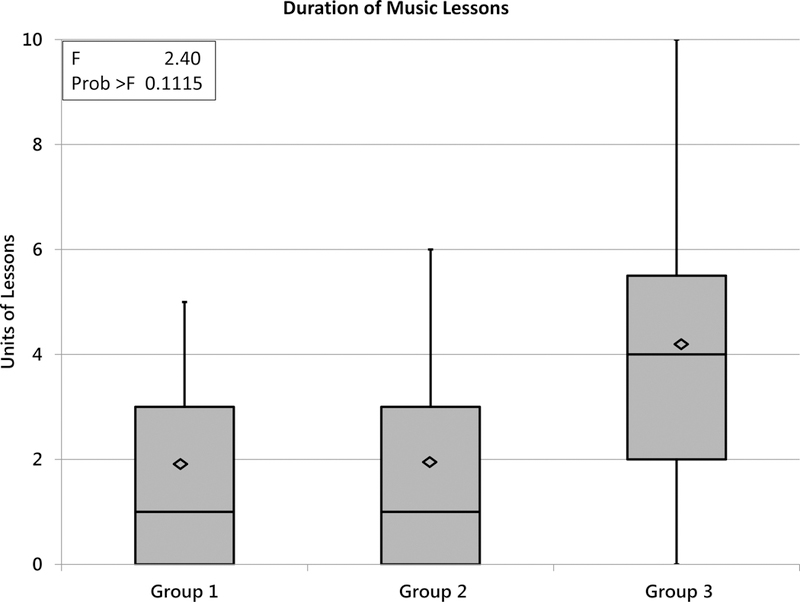
Distribution of duration of music lessons (DML) as a function of group membership. No significant difference was found among groups, but group 3 showed larger variability in duration than the other two groups.
To answer the first research sub-question, a correlation was performed between the continuous variables CPRT, ME and DML. Because PIM was a categorical variable, a regression model was run to evaluate how CPRT varies by PIM level where CPRT was the outcome variable and levels of PIM were the predictor variables.
To answer the second research sub-question, a regression model was used to evaluate how ME is related to predictor variables of demographics, familial involvement in music, and PIM. Continuous variables were the demographic variables: AGE-T, LoU, AGE-I, ONSET; categorical variables were family involvement in music growing up (FAM-GU) and current family involvement in music (FAM-C). A post hoc analysis was used to illustrate any differences in ME as a function of family involvement.
In relation to the third research sub-question, a regression was created to determine the extent that PIM, CPRT, and ME predicted CNC word and CNC phoneme speech perception scores. Backwards model selection was used to determine the final version of the regression models.
Results
Figure 1 shows the distribution of scores on CPRT: Group 1 (24 to 17), with higher (least accurate) thresholds on the left; Group 2 (16 to 9) in the middle; and Group 3 (8 to 1 semitone) with the lower (most accurate) thresholds to the right. The number and mean ages of the CI users within the CPRT tertiles were as follows: Group 1: n=22, Mean age 15.14 yrs.; group 2: n=16, Mean age 14.78 yrs.; Group 3: n=39, Mean age 15.3 yrs. A
Figures 2 through 4 present the distribution of scores for PIM, ME, and DML as a function of CPRT tertiles. Examination of these figures shows the variability of responses on each of these measures and indicates any significant differences on each variable as a function of CPRT tertiles.
Research question 1 examined the relations between CPRT and three forms of musical engagement: ME, DML, and PIM. CPRT showed significant, negative correlation with both ME (p=.0038) and DML (p=.0019). In other words, CI users with lower (better) pitch thresholds were more likely to persist in music lessons. Conversely, better pitch perception (CPRT) was not significantly correlated with participant’s ranking of the importance of music in their lives (PIM) (p=.1968).
Research question 2 examined the relations between participant demographics and three variables of musical engagement (ME). There was a significance in the model, with FAM-C predicting current participant ME (p=.0007); however, none of the demographic variables were significant predictors. Post hoc analysis of least square means showed an effect of FAM-C on involvement. Participants whose families were involved in music at the time of testing were significantly different from those whose families who were not at all involved (p=.0003) or minimally involved (p=.0005).
Research question 3 addressed recent speculation regarding the relations between processing requirements of music and speech. For CNC word scores, CPRT was a significant predictor of accuracy (p=.0060), but ME or DML were not. CPRT was also a significant predictor of outcomes on CNC phonemes (p=.0174).
Discussion
This study examined the impact of perceptual, demographic, and environmental factors on musical engagement of pediatric CI recipients. Prior studies on music and pediatric CI users have typically focused on understanding the relations between auditory development through electric hearing and the impact on perceptual accuracy for acoustic features such as pitch, duration, and timbre.1 Less is known regarding the interaction of hearing history, perceptual accuracy, and music engagement, or active music making, especially in pediatric CI users. While a small number of prior studies have highlighted the importance of familial involvement in promoting music engagement,26 previous studies have not examined multiple factors within a single study and a sizable cohort. This study was designed to better understand the relations among multiple variables that likely interact with music engagement.
The first variable we examined was pitch perception. While prior studies have focused on pitch in relation to melody recognition or music enjoyment, pitch accuracy is also relevant to music engagement. When playing most pitched musical instruments or while singing, pitches must be produced within normal interval ratios and in tune with an external pitch. Although NH children must also develop increasingly refined abilities to play in tune, persons with normal hearing can typically perceive pitch increments that are orders of magnitude smaller than those increments comprising musical scales, thus auditory perception is not a major impediment to music engagement. These perceptual skills are often taken for granted in ‘normal’ music making. In contrast, many pediatric CI users have significantly poorer pitch perception. Only a small proportion of CI users are able to rank pitches as small as 1 or 2 semitones, with others requiring as large as two octaves for reliable pitch ranking.1,5 In addition, there can be distortions in interval size from one note to the next.
Given the importance of pitch in western music, it is not surprising that CI users with better pitch perception were more likely to persist in music lessons. However, establishing a causal relationship between pitch perception and music engagement is far from straightforward. For example, one can argue that generally superior CI use (including better speech and pitch perception) could support more satisfactory and thus persistent engagement; an alternative hypothesis is that longer-term involvement in music may enhance pitch and thus music perception. One should also keep in mind, however, that many NH children, whose pitch perception is within normal perceptual ranges, do not choose to persist in music lessons for any number of reasons (lack of motivation, low family priority, poor instruction, etc.). Thus, pitch perception cannot fully account for music engagement patterns.
Furthermore, different forms of music engagement require different levels of precision in pitch perception. For example, instruments that require on-going adjustment of tuning, like the violin or trumpet, demand finer-grained pitch perception than non-pitched instruments like many percussion instruments. An examination of the instruments played by CI users in our cohort indicates they were more likely to persist in music lessons for 4 years or longer when they played instruments such as piano or percussion, which do not require on-going tuning of the instrument to external pitch in real time. Consequently, these findings suggest that judicious choice of musical instrument is a factor in supporting robust music engagement. In fact, some CI users reported they started lessons on one instrument (e.g., trumpet), but found pitch production so difficult they switched to an instrument that did not require ongoing turning (e.g., percussion). They subsequently succeeded after reducing the perceptual demands.
We found that length of CI use and maturity (age) did not predict greater musical engagement, but family involvement did. This is not surprising, given the logistics of enrolling in lessons as well as the psychosocial aspects of parental and sibling influence. A child in a household that values music is more likely to have regular exposure to music and encouragement to participate in music lessons, ensembles, and on-going practice. Practically, young children typically rely on parents for enrolling in, payment of, and transportation to music lessons and events. Parents often must encourage music practice for all children—not just children with CIs—at least up until the point when practice is motivated by more intrinsic rewards. A parent might also intercede when there are difficulties with the structure or interpersonal relationships during instruction.
In our study, one participant from a family of professional musicians was so highly motivated to develop ‘normal’ pitch perception that he practiced for hours developing alternative cues (e.g., feeling the beats of music, using visual tuners) to establish nearly ‘normal’ pitch perception, with a CPRT threshold at the lower limit of the test. Although he is an outlier, in his case, familial influence and his own love of music led him to dedicate tremendous amounts of time and effort required for focused training and refinement of pitch perception. He described music as being highly valued within his family, and thus, restoring music engagement post implantation was a strong personal goal for this young man. Other family members, like an admired older sibling engaged in music, can also be influential and highly motivating. In short, familial support of music engagement is important to most children, but may be of particular importance for children with CIs, given the myriad challenges associated with music making.
With regard to the strong correlations between pitch and speech perception, accuracy in pitch perception was a significant predictor of accuracy in speech perception. This strong relationship may simply reflect that some CI users excel in general auditory perception, including more spectrally complex sounds. Based on speculation regarding underlying perceptual mechanisms,1 it is possible the ability to more accurately extract pitch from the signal is beneficial to speech perception as well as music engagement.30 While some studies suggest extended music training can enhance speech perception,22,24 these data did not demonstrate that more extensive music engagement was associated with enhanced speech outcomes. More study is required to test directly the hypothesis that music engagement can enhance speech perception.
While analyses of group data provide some insights into those factors that could be initial avenues for success in music engagement, our examination of individual cases was a reminder that life experiences and personality factors influence individuals in unique ways. For example, one CI user’s CPRT was 4 semitones. This is much larger than the smallest pitch changes in western musical scales, and the minute pitch changes required for ongoing tuning to produce pitches on the violin’s fret board. Nevertheless, she persisted with violin lessons for 5 years. When asked in an open-ended question how she felt about music, she wrote, “I can’t live without music.”
Another participant with CPRT thresholds of 12 semitones (the equivalent of an octave!) was raised in a family with minimal involvement in music. Yet, this individual took flute lessons for 6 years and wrote, “Music is my life! I could not survive without music.”
As these individual profiles indicate, perceptual accuracy cannot fully predict patterns of perception. Although better perceptual accuracy for pitch appears to be beneficial, it does not predict music engagement fully. In many instances, familial involvement in music is an important factor. While a relatively small proportion of this sample persisted with lessons longer than 4 years, it is impressive that approximately 66% of these CI users described music as personally important in their lives, despite the degraded representation of musical sounds.
The current study showed a stronger relationship between familial involvement and music engagement, than between pitch perception and music engagement, which is of both clinical and educational interest. For families who value music as an important part of culture and family life, encouragement can improve motivation and influence judicious choices for music engagement. Even those pediatric CI users with poorer pitch perception can, with familial support, have some level of success and persistence in music engagement. The limitations of CIs for conveying key features of music are not an insurmountable barrier to music participation and enjoyment. These data also indicate pediatric CI users can successfully engage in music, particularly if the family supports participation.
Acknowledgements:
This study was supported by grant 2 P50 DC00242 and 5T32DC000040-24 from the NIDCD, NIH. Many thanks to Helin G. Hernandez for assistance with set up of analytical programming.
Footnotes
Analyses comparing test outcomes of pre- and postlingual deaf participants did not reveal significant differences in music engagement or perception.
References
- 1.Gfeller K Music as Communication and Training for Children with Cochlear implants. In: Young N, Kirk K, eds. Pedatric Cochlear Implantation: Learning and the Brain New York, NY: Springer; 2016:313–328. [Google Scholar]
- 2.Trehub SE, Vongpaisal T, Nakata T. Music in the lives of deaf children with cochlear implants. Ann N Y Acad Sci 2009;1169:534–542. [DOI] [PubMed] [Google Scholar]
- 3.Stabej KK, Smid L, Gros A, Zargi M, Kosir A, Vatovec J. The music perception abilities of prelingually deaf children with cochlear implants. International journal of pediatric otorhinolaryngology 2012;76(10):1392–1400. [DOI] [PubMed] [Google Scholar]
- 4.Gfeller K, Driscoll V, Smith R, Scheperle C. The music experiences and attitudes of a first cohort of prelingually deaf adolescent and young adult cochlear implant recipients. Seminars in Hearing 2012;33(4):346–360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gfeller K, Witt SA, Spencer L, Stordahl J, Tomblin JB. Musical involvement and enjoyment of children using cochlear implants. Volta Review 1999;100(4):213. [Google Scholar]
- 6.Rocca C A different musical perspective: Improving outcomes in music through habilitation, education, and training for children with cochlear implants. Seminars in Hearing 2012;33:425. [Google Scholar]
- 7.Looi V, Gfeller K, Driscoll V. Music appreciation and training for cochlear implant recipients: A review. Seminars in Hearing 2012;33(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Limb CJ, Roy AT. Technological, biological, and acoustical constraints to music perception in cochlear implant users. Hearing research 2014;123(7). [DOI] [PubMed] [Google Scholar]
- 9.Drennan WR, Oleson JJ, Gfeller K, et al. Clinical evaluation of music perception, appraisal and experience in cochlear implant users. Int J Audiol 2015;54(2):114–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gfeller K Musical perception and aesthetic enjoyment of adult cochlear implant recipients: Interdisciplinary perspectives. Proceedings of Multidisciplinary Perspectives on Musicality: The Seashore Symposium. Bulletin of the Council for Research in Music Education 2000.
- 11.Gfeller K, Jiang D, Oleson J, Driscoll V, Knutson JF. Temporal stability of music perception and appraisal scores of adult cochlear implant recipients. Journal of the American Academy of Audiology 2010;21(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gfeller K, Jiang D, Oleson J, et al. The effects of musical and linguistic components in recognition of real-world musical excerpts by cochlear implant recipients and normal-hearing adults. Journal of Music Therapy 2012;49(1):68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wright R, Uchanski RM. Music perception and appraisal: cochlear implant users and simulated cochlear implant listening. J Am Acad Audiol 2012;23(5):350–365; quiz 379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Parbery-Clark A Musician enhancement for speech-in-noise. Ear and Hearing 2009;30(6):653–661. [DOI] [PubMed] [Google Scholar]
- 15.Patel AD. Why would musical training benefit the neural encoding of speech? The OPERA hypothesis. Frontiers in psychology 2011;2:142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gfeller K, Guthe E, Driscoll V, Brown CJ. A preliminary report of music-based training for adult cochlear implant users: Rationales and development. Cochlear Implants Int 2015;16 Suppl 3:S22–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Punch R, Hyde M. Social participation of children and adolescents with cochlear implants: A qualitative analysis of parent, teacher, and child interviews. Journal of Deaf Studies and Deaf Education 2011;16(4):474–493. [DOI] [PubMed] [Google Scholar]
- 18.Wheeler A, Archbold S, Gregory S, Skipp A. Cochlear implants: the young people’s perspective. Journal of Deaf Studies and Deaf Education 2007;12(3):303. [DOI] [PubMed] [Google Scholar]
- 19.Christenson PG, Roberts DF. It’s not only rock & roll: Popular music in the lives of adolescents Cresskill, NJ: Hampton Press; 1998. [Google Scholar]
- 20.Behne K-E. The development of” Musikerleben” in adolescence: How and why young people listen to musi. In: Deliège I, Sloboda J, eds. Perception and cognition of music Vol xvii Hove, England: Psychology Press/Erlbaum (UK) Taylor & Francis; 1997:461. [Google Scholar]
- 21.Gfeller K Music-based training for pediatric CI recipients: A systematic analysis of published studies. European Annals of Otorhinolaryngology, Head and Neck Diseases 2016;133:S50–S56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shahin AJ. Neurophysiological influence of musical training on speech perception. Frontiers in psychology 2011;2(126). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kraus N, Skoe E, Parbery-Clark A, Ashley R. Experience-induced malleability in neural encoding of pitch, timbre, and timing. Annals of the New York Academy of Sciences 2009;1169:543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wong PCM, Skoe E, Russo NM, Dees T, Kraus N. Musical experience shapes human brainstem encoding of linguistic pitch patterns. Nature neuroscience 2007;10:420–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gfeller K, Turner C, Mehr M, et al. Recognition of familiar melodies by adult cochlear implant recipients and normal-hearing adults. Cochlear Implants International 2002;3(1):29–53. [DOI] [PubMed] [Google Scholar]
- 26.Driscoll V, Gfeller K, Tan X, See RL, Cheng HY, Kanemitsu M. Family involvement in music impacts participation of children with cochlear implants in music education and music activities. Cochlear Implants International 2015;16(3):137–146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Peterson GE, Lehiste I. Revised CNC lists for auditory tests. Journal of Speech and Hearing Disorders 1962;27:62–70. [DOI] [PubMed] [Google Scholar]
- 28.Cooper WB, Tobey E, Loizou PC. Music perception by cochlear implant and normal hearing listeners as measured by the Montreal Battery for Evaluation of Amusia. Ear Hear 2008;29(4):618–626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Brockmeier SJ, Fitzgerald D, Searle O, et al. The MuSIC perception test: a novel battery for testing music perception of cochlear implant users. Cochlear Implants Int 2011;12(1):10–20. [DOI] [PubMed] [Google Scholar]
- 30.Won JH, Drennan WR, Rubinstein JT. Spectral-ripple resolution correlates with speech reception in noise in cochlear implant users. J Assoc Res Otolaryngol 2007;8(3):384–392. [DOI] [PMC free article] [PubMed] [Google Scholar]