

Abstract
Objective.
The objective of the current project was to determine the feasibility of using 3D printed technology to facilitate reminiscence-related activities for persons with memory loss (PWMLs).
Methods.
A parallel convergent mixed methods design was used. Fifteen PWMLs, 13 family members, and 6 staff members participated in two residential long-term care facilities. Participants were observed and interviewed initially, during a 2-week reminiscence session, and again during a 1-month reminiscence session. Staff participants also completed a 1-month focus group, and staff and family members were administered a 3D printing review checklist at 1-month.
Results.
The integrated qualitative and quantitative data strongly suggested that PWMLs enjoyed using the 3D objects, were engaged while doing so, and appeared to value the objects due to their personalized nature. The use of 3D printed objects also appeared to encourage family involvement as well as family and staff interactions with PWMLs. Barriers to use included memory impairment and behavioral issues.
Conclusions.
The use of 3D printed objects could provide an easy-to-use, well-received, person-centered approach that augments current reminiscence strategies for PWMLs.
Keywords: Memory loss, Dementia, Alzheimer’s disease, 3D printing, Reminiscence, Mixed methods, Non-pharmacological therapies
INTRODUCTION
Alzheimer’s disease or related dementias affected over 46.8 million people worldwide in 2015 [1]. Given Alzheimer’s disease and related dementias’ complex neuropathology, extensive healthcare and social costs, and moderately effective pharmacological treatments, the identification of viable non-pharmacological approaches is urgent. Non-pharmacological approaches range from exercise to creative therapies and harbor the potential to offer tailored, person-centered dementia care. Person-centered dementia care honors and respects the unique needs and interests of the person with memory loss (PWML), relying on PWMLs’ strengths and engaging her/him in activities of interest [2,3]. Among non-pharmacological treatments thought to embody person-centered care is reminiscence therapy (RT) and related activities. Reminiscence therapy involves the prompting of past memories, typically with artifacts such as old photographs or music that are familiar and important to the PWML. Engaging the PWML via RT may foster their verbal engagement and social involvement through the recollection of past memories and significant life experiences [4,5].
There is potential to augment the benefits of RT with digital audio or image technology [6]. However, there is no existing research on the feasibility and utility of more advanced technologies, such as 3D printing, to help facilitate RT for persons with dementia. The current project is the first of its kind to determine the feasibility of using 3D printed technology to produce replicas of objects that hold personal significance and meaning to PWMLs in order to facilitate reminiscence-related activities.
Background
Reminiscence therapy originated from the work of Robert Butler, who outlined the importance of life review as a form of therapy [7]. In RT the person recalls and discusses important events in her or his life with another person or in a group setting. Reminiscence therapy is often delivered by professional or family caregivers [2]. This approach is particularly useful for PWMLs, since memories from childhood and early adulthood stay relatively intact until the later stages of dementia. Studies of RT have suggested benefits for PWMLs, including improved cognitive skills, levels of engagement, and well-being in addition to decreased depressive symptoms, anxiety, and agitation [8–12]. However, the methodological quality of such research is heterogeneous; several studies and meta-analyses indicate that RT has no effect on depression or cognitive skills, and there exist few controlled evaluations that include sufficient sample sizes [4,12,13].
A core component of RT with PWMLs involves the prompting of past memories with artifacts relevant to the individual, including photographs or music [4]. This essential function of RT is now facilitated with a variety of technologies. For example, digital photographs, accessible and commercially available online games, and multimedia interventions have been implemented and in some instances systematically examined for their potential to facilitate reminiscence for PWMLs [4,6,14]. In general, the use of technology appears to hold promise in augmenting and contributing to more successful reminiscence experiences for PWMLs. The technological aids used in RT sessions typically consist of 2-dimensional photographs or music familiar to the PWML that are sometimes downloaded onto a computer or tablet device [4,14]. Three dimensional (3D) printed objects may provide a novel and effective medium for RT that could offer robust memory stimulation and opportunities for engagement via a tactile sensory experience [14–18]. In addition, generating a personalized 3D-printed object that not only has emotional salience for the PWML but actually “exists” and is owned by the PWML could further enhance the reminiscence experience [4,19].
Research focus
To our knowledge there is no literature available that considers the use of 3D objects to facilitate reminiscence for PWMLs (a PubMed search using the key words “3D printing and Alzheimer’s” and “3D printing and dementia” yielded no publications on this topic). As RT has potential benefits in reducing depressive symptoms and offering cognitive stimulation for PWMLs, incorporation of a 3-dimensional, personalized, physical object of importance to a PWML may operate to facilitate such outcomes alongside standard reminiscence activities [10,14]. The goal of the current study was to test the feasibility of 3D printing to create a variety of replicas and small-scale models that individuals in various stages of dementia could recognize and relate to their personal past. Specifically, the present study sought to determine whether 3D printed technology is capable of creating objects for use in reminiscence activities and whether the use of these objects stimulate a positive, autobiographical reminiscence experience for PWMLs, their family members, and professional care staff.
METHODS
Design and sample
To fully examine the feasibility and utility of 3D printing objects for PWMLs, their family members, and staff, a parallel convergent mixed methods design (QUAL + quan) was used [20,21]. A mixed methods design was employed because the quantitative data would provide broad descriptive data as to the extent of perceived utility and feasibility of 3D printing for reminiscence. Incorporating various forms of qualitative data (e.g., field notes, semi-structured interviews) helped expand upon the quantitative data by examining the reasons why or how PWMLs, family members, and staff felt 3D printing was useful in helping to stimulate reminiscence. In addition, the use of qualitative data collection techniques offered PWMLs the opportunity to share their “voices” in the analysis of feasibility and utility. As noted in the QUAL + quan notation, the priority in this particular design is given to the qualitative strand, with the quantitative strand offering broader description of the feasibility and utility of 3D printing objects. Further information on the timing and data elements of the qualitative and quantitative study strands are illustrated in Figure 1. The “mixing,” or integration of the qualitative and quantitative data in the current study occurred when simultaneously interpreting, analyzing, and comparing the data from both strands in the Results section.
Figure 1.
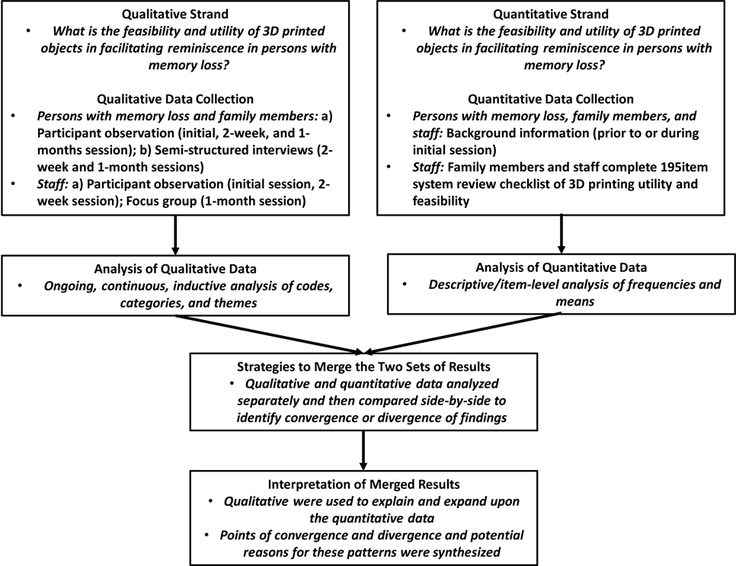
Parallel Convergent Mixed Methods Design.
The University of Minnesota Institutional Review Board approved the conduct of this study (IRB #1507S76666). Staff who volunteered to participate and facilitate the use of the 3D printing objects for PWMLs and their family members provided written informed consent and participated in an initial 30–45 minute tutorial session (see below; n = 6). Following the staff tutorial session, participating staff identified residents with memory loss and their family members (and/or their legally authorized representatives) and described the study. Participating staff also received permission from interested family members for the graduate research assistants (AG and SR) to contact them regarding enrollment in the study. Inclusion criteria for persons with memory loss (PWMLs) were as follows: (1) a diagnosis of Alzheimer’s disease or a related dementia; and (2) a willingness to use the 3D objects with PWMLs. Once permission was obtained, the graduate research assistant secured informed consent from the family member and/or legally authorized representative and then met with the PWML to review the study procedures, conduct a brief memory assessment (the Saint Louis University Mental Status Examination/SLUMS) [22] and obtain verbal assent from the PWML prior to the identification of selected objects to print.
A total of 15 PWMLs participated in the research procedures as well as 13 family members who agreed to use the 3D objects with the PWML and 6 staff members (see Table 1 for sample characteristics).
Table 1.
Background Characteristics: Persons with Memory Loss, Family Members, and Staff
| PWMLs (n = 15) |
Family Members (n = 18)a |
Staff (n = 6) |
||||
|---|---|---|---|---|---|---|
| Variable |
Mean
(SD) |
% |
Mean
(SD) |
% |
Mean
(SD) |
% |
| Age | 86.13 (9.89) |
60.38 (10.01) |
44.00 (15.60) |
|||
| Female | 60.0% | 61.1% | 100.0% | |||
| Ethnicity: Not Hispanic/Latino | 93.3% | 100.0% | 100.0% | |||
| Race: White | 100.0% | 100.0% | 100.0% | |||
| Married/Living with partner | 13.3% | 58.8% | 66.7% | |||
| Employed full time | - | 50.0% | ||||
| Average hours worked per week (staff only) | 32.33 | |||||
| per week (staff only) | (11.89) | |||||
| Living children | 3.14 (2.60) |
2.35 (2.26) |
- | |||
| Highest level of education: High school or greater |
100% | 5.06 (1.20) |
6.67 (0.82) |
|||
| Household income: Under $29,999 annually |
66.7% | 8.67 (1.23) |
- | |||
| Did PWML ever visit the doctor for memory concerns |
- | 66.7% | - | |||
| Time since first doctor visit for memory concerns (in years) |
5.73 (5.95) |
- | - | |||
| Diagnosis: Alzheimer’s disease or dementia |
53.6% | - | - | |||
| No diagnosis reported | 40.0% | - | - | |||
| St. Louis University Mental Status score |
8.47 (5.78) |
|||||
| Length of stay (in months) |
22.27 (29.12) |
- | - | |||
| Time since memory symptoms first recognized (in years) |
- | 5.15 (4.91) |
- | |||
| Kin relationship to PWML: Adult child |
- | 100.0% | - | |||
| Family member ever provided help to PWML due to memory loss |
- | 70.6% | - | |||
| Family member is primary caregiver of PWML |
- | 52.9% | - | |||
| Duration of care to PWML (in months) |
- | 82.67 (87.50) |
- | |||
| Length of employment at current facility (in months) |
- | - | 97.16 (122.16) |
|||
NOTE: PWML = person with memory loss
Nineteen family members completed a consent and background form for their relative, but only thirteen participated in subsequent research procedures and completed a system review checklist; 3 PWMLs resided in a nursing home unit and 12 in an assisted living/nursing home memory care unit
Ethical considerations
Obtaining informed consent from PWMLs was approached as an ongoing process between PWMLs, staff, family members, and the graduate research assistants (e.g., see http://www.irb.umn.edu/toolkit.html). This process was designed to uphold ethical principles of beneficence and autonomy, honoring the PWML’s rights to make decisions as well as protect their safety and wellbeing. The ethical protocol for obtaining informed consent included explicit discussion of participants’ rights and offering adequate information for them to make informed choices about entering and continuing in the study. Specifically, the consent process included: a) proxy consent via the family member/legally authorized representative; and b) verbal assent on behalf of the PWML. Family members/legally authorized representatives had to complete proxy consent and all PWMLs had to provide verbal assent in order to participate. The consent and verbal assent process also provided assurances to participants that the records of the study were kept private, and that all information provided was confidential and maintained in a secure manner by the researchers. The initial informed consent meeting also included an opportunity for the PWML to ask questions and receive answers about the study and their involvement, a discussion of the nature and anticipated course of the study, and the potential for involvement of family members and staff in these meetings. This was facilitated by family members and staff, who at times would ask questions on behalf of the PWML to ensure that their questions would be answered. The voluntary nature of the study was emphasized, and each of the following meetings included reminders for the PWML of their involvement in the study and an ongoing discussion of their rights as participants and to make autonomous decisions about continuing in the study. Participants could withdraw from the study by expressing to staff, family members, or the graduate research assistants that they no longer wished to participate. No participant chose to withdraw during the study, and often participants expressed gratitude for the opportunity to share their stories with others and stated that they looked forward to meeting again. In instances when participants were sleeping or were involved in other activities during scheduled meetings, the PWML was given information about the study and reminders of their previous involvement by graduate research assistants, family members, or staff. They could then choose to participate at that time, choose another time, or forego the meeting and withdraw completely. In each of these instances, the participant either chose to participate in place of their current activity such as sleeping or watching television, or a new time was negotiated per the PWML’s schedule.
3D printing and reminiscence procedure
To initiate the project, the project directors (TP and DK), the reminiscence coordinator (KJ), and the two graduate research assistants (AG, SR) conducted two 30–45 minute tutorials with staff involved in the project in two residential long-term care settings in the Minneapolis/St. Paul metropolitan area (one is a nursing home and assisted living facility, the other is an independent living and assisted living setting). These initial staff sessions included a discussion of how 3D printing works and could be helpful to PWMLs as well as an overview of research procedures. One month following the initial staff tutorial, the graduate research assistants conducted a focus group/semi-structured interview with staff participating at the two residential long-term care facilities involved in this project. The open-ended questions were designed to determine whether the 3D objects were or were not easy for PWMLs and family members to use and whether the objects were helpful or not to PWMLs.
Several weeks following the initial staff tutorial, the reminiscence coordinator (KJ) and one of the graduate research assistants (AG or SR) initially met with each participating PWML and/or a family member or staff person. This initial meeting facilitated reminiscence in PWMLs and the identification of potential objects, and was based on Butler’s seminal work and additional reminiscence guides (see the Life Interview Manual in the Online Supplemental Material) [7,23–27].
Models were then constructed by CAD Technology Center. CAD Technology Center features software, design tools, and 3D printing capabilities to efficiently produce the 3D printed objects used in this project. The first step in the printing process was to generate a 3D model of the object on a computer, based on the specifications provided during the initial meeting with the PWML, family member, and/or staff person. A custom model was drawn on a computer by a skilled designer, usually in less than three hours. The computer model was then sent to a 3D printer to print the object in full-color gypsum and was later retrieved by KJ to present to the PWML and/or a participating family member and staff person at follow-up sessions (see below). Figure 2 provides some examples of the objects printed for this project.
Figure 2.

Example 3D Printed Objects
Approximately two weeks following the initial review and identification of objects, KJ and one of the graduate research assistants met with the PWML as well as a participating staff person and/or family member to present the objects and conduct a semi-structured interview with the PWML and participating family member about their initial impressions of the helpfulness or lack thereof regarding the 3D objects (see Online Supplemental Material for the brief, semi-structured interview guide). The PWML, staff member, and family member were encouraged to use the 3D objects in any way they wished and as frequently as desired during and following the 2-week session. One-month following the initial tutorial session, a final meeting of the PWML, KJ and one of the graduate research assistants, and a participating staff person and/or family member took place. KJ reviewed the 3D object using reminiscence techniques built upon the previous sessions. The graduate research assistant made observational notes and conducted a final semi-structured interview with the PWML and a participating family member (see Online Supplemental Material for interview guide). A 3D printing review checklist was also administered to participating family members and staff persons to obtain information on how well the 3D objects were received by PWMLs, perceived benefits, and other aspects of perceived utility or lack thereof; this checklist was the source of empirical data in this mixed methods study.
All observational notes, interview sessions, and focus groups were digitally recorded and/or transcribed for subsequent qualitative analyses.
Data collection
Demographic/Background data
Immediately following informed consent procedures the family member for the PWML provided background information on the PWML and family member; similarly, staff members provided background information about themselves following informed consent (see Table 1).
3D printing review checklist
A 15-item, close-ended checklist was administered to family members and staff following the 1-month 3D object review session. The senior author (JEG) designed the checklist specifically for this project to assess perceptions of feasibility and utility of the 3D objects for PWMLs based on similar checklists administered in prior research (see Table 2 for items; α = .92) [6,28]. The item responses ranged from 1 = “strongly disagree” to 5 = “strongly agree.”
Table 2.
3D Printing Review Checklist of 3D Printed Objects and Reminiscence: Percent Agreed or Strongly Agreed (N = 18; n = 13 family members; n = 5 staff members)
|
Percent Agreed or Strongly
Agreed |
|
|---|---|
| 1. 3D printing was easy to use. | 94.5% |
| 2. The objects generated by 3D printing were well received by the person with memory loss. | 88.9% |
| 3. The person with memory loss enjoyed using 3D printing. | 76.5% |
| 4. The research team was helpful in showing me and the person with memory loss how to use 3D printing. | 94.5% |
| 5. After using 3D printing, I thought that the person with memory loss was more engaged and alert. | 72.3% |
| 6. 3D printing allowed me to interact more effectively with the person with memory loss. | 83.4% |
| 7. There are time constraints to me being able to use 3D printing. | 33.4% (27.8% disagreed or strongly disagreed) |
| 8. I would use the 3D printing again when communicating/interacting with the person with memory loss. | 83.4% |
| 9. The objects printed were clear and easy for the person with memory loss to use. | 100% |
| 10. The person with memory loss felt lost using 3D printing. | 0.0% (77.8% disagreed or strongly disagreed) |
| 11. I wish I would have known about 3D printing sooner. | 50.0% |
| 12. 3D printing provided the person with memory loss with enough objects and material to fully engage with. | 83.3% |
| 13. 3D printing helped the person with memory loss reminisce and remember the past better. | 83.3% |
| 14. 3D printing is very confusing to me. | 5.9% (88.3% disagreed or strongly disagreed) |
| 15. I would recommend 3D printing to others in a similar situation | 94.4% |
Data analysis
Qualitative data collection and analysis occurred simultaneously. Field notes and interview data were audiotaped and transcribed verbatim. Systematic reading and rereading of qualitative content was conducted by AG, SR, and JEG to develop an understanding of meanings in their conversational or observational contexts [29,30]. The senior author (JEG) open-coded each transcript [30–32]. Through repetition of this procedure and regular meetings between JEG, AG, and SR, a consensus perspective was achieved regarding coding categories and themes. The themes were developed to provide information to address the research questions of interest.
Qualitative analytic techniques described by Morse [31] were utilized via a qualitative data management and software program (nVivo) [33] to complete thematic analyses. The qualitative analytic approach allowed participants to construct meanings, perceptions, and behaviors from their own vantage points. Descriptive statistics (frequencies, means) were utilized to analyze family and staff members’ perceptions of the 3D objects’ functionality and utility derived from the 3D printing review checklists.
Integration of the qualitative and quantitative study strands was first achieved by generating a matrix of the themes identified in the various qualitative data elements (e.g., participant observation/field notes; semi-structured interviews; staff focus group). The descriptive empirical results of the 3D printing review checklist (i.e., item frequencies and means) were then compared to the organized themes to determine how and why the 3D objects’ were perceived as useful or acceptable to PWMLs, their family members, and participating staff [20].
RESULTS
Feasibility and utility of 3D objects
The qualitative analysis identified 4 principal themes (Benefits of 3D Printing; Recommendations to Enhance Feasibility and Utility; Resident Engagement in Study Process; and Reminiscence Process) along with 14 categories that demonstrated the feasibility and utility of 3D objects to facilitate reminiscence in PWMLs (see Table 3). These themes and categories are described below and, per the mixed methods analysis approach, compared alongside the descriptive empirical results of the 3D printing review checklist.
Table 3.
Themes and Categories: Participant Observation and Semi-Structured Interviews of Persons with Memory Loss, Family Members, and Staff Persons
| Theme | Category |
|---|---|
| Benefits of 3D Printing | |
| Helpfulness of objects | |
| Enhanced resident engagement | |
| Family and staff benefit | |
| Lack of benefits | |
|
Recommendations to Enhance
Feasibility and Utility |
|
| Enhancing staff coordination and engagement |
|
| Improving reminiscence process | |
| Group discussion of objects | |
| Resident Engagement in Study Process | |
| Resident emotional status | |
| Resident environment | |
| Resident responsiveness during study activities |
|
| Reminiscence Process | |
| Object identification process | |
| Reaction to objects | |
| Participant engagement in 3D object- reminiscence process |
|
| 3D printing use was not for everyone | |
Benefits of 3D printing
A principal theme reflected the various benefits of 3D objects; representative categories included enhanced resident engagement; family and staff benefits; the overall helpfulness of the objects; and in some instances, the perceived lack of benefit of 3D objects and reminiscence.
During the 1-month observational and interview sessions, PWMLs and participating family members frequently emphasized how various aspects of the objects and associated reminiscence activities were helpful. For example, the ability to touch and feel the object was linked to stimulation on the part of PWMLs:
“I don’t know. I think there’s something to touching it...and feeling it, and holding it. Cause everybody wanted to hold the little tricycle. And everybody wanted to <touch> the wheels and move the <handles>—you know. I wanted to too. (laughter)...Yeah. I would go with that, because we do different things with pictures and stuff. And that’s ok. But having that object. Then they could pass it on, and you know, and like did you notice this? And, yeah, it’s something there in their hands. I do think the 3-D might be just a little bit better than just a picture. I mean, it may not feel the same, but yet they—they’re feeling it. They’re touching it. And I think something there is jogging memory.” (Final staff focus group)
Semi-structured interviews also suggested that PWMLs and family members felt that having the objects present made the PWML happy:
AG: Did you like those <the 3D objects>? Do you think they helped?
Family member: The piano
PWML: Oh yes.
AG: What do you like about the piano and the house?
PWML: Well, they play beautiful music . Three men stayed in the house next to ours, and they played music really good. All the time. Really good.
AG: That would be a lot of fun.
PWML: Yeah. I wished they—maybe I’ll ask them if they still play some of those old time songs, just for the heck of it. You’ll learn how to play too.
Family member: Oh yeah. #
PWML: Tomorrow it’s her turn. (laughter)
AG: Do you think, apart from the focus is there anything else that the objects have helped with?
Family member: I think it’s maybe—she’s got some happiness from it. Because she’s thinking of the good things too. That made her happy.
PWML: They were playing a song that you could dance to.
(1-month semi-structured interview)
Another category was the engagement on the part of PWMLs when using the 3D objects:
Family member: I was interested when (name of PWML) showed it to me, because she has such great memories of—
PWML: Oh yeah.
Family member: This, and I think if you just even have that trigger you might think of something new—and I have to say that probably since they’ve moved here, I’ve probably heard a lot of different stories from the days when you were growing up, or from in town, or from when you first got married and things like that, because probably the busyness of other life you just didn’t get to it. And now when we’re here, I think we just have more time to talk. And so I thought, if this is something that triggers some new memories, or things that you know, you just didn’t think about that often—
PWML: Yeah.
Family member: And now she’s talking to us about it. I felt that’s been really fun, you know, hearing stories about both of you guys when you were growing up. So, I wasn’t ever really thinking about it as it would necessarily solve anything, but I think that it was only—could only probably help.
(1-month semi-structured interview)
“(Name of PWML) was sitting up with other residents. Before he went into the TV room the nursing staff were telling us that he has since been more outgoing with other residents and with care staff. Every morning they drop by his room for Trivia questions, and in the past he never answered them or told them to go away, and now he likes to sit and chat. I thought that was a really interesting piece, that maybe the reminiscence has gotten him more outgoing and more willing to share his stories and his knowledge with others.” (1-month session field notes)
In addition to the 3D objects and reminiscence activities potentially resulting in resident engagement, family and staff also mentioned other benefits of the 3D objects:
“I would say just being able to interact more with that resident or having something to talk about with them. You know, depending on the family and how involved they are. Some struggle with, well what do we talk to dad about? You know, he doesn’t remember who we—you know?...So I’d say from that aspect it just gave them something to talk about with the resident, or can in the future give them something to talk about with the residents. And just, I mean, I think it would be a benefit as a family member to see my loved one light up when they saw the object for the first time, or were able to tell stories from their past.” (Final staff focus group)
“Yeah, I do think they’ve helped. He’s recalled much more than we’ve ever talked about before...Yeah. Even learning about breeding, when you had the puppies...Yeah. I didn’t know that.” (1-month semi-structured interview session)
“Doing the couple of group discussions that they did was very helpful in thinking of other activities they could do for people with memory loss. You know, doing the object share activity was really great and caused some people to open up a lot more than they had and just prompted other memories often.” (Final staff focus group field notes)
“We, as a facility, loved the project...So I think it was an awesome project. So glad that we participated, and hopefully can continue.” (Final staff member semi-structured interview)
These data aligned with a number of empirical items on the 3D printing review checklist; close to and over ¾ of family and staff reported that the PWML was more engaged after using and reviewing the 3D objects (72.3%) and that the 3D objects allowed family and staff members to interact more effectively with the PWML (83.4%). Similarly, over ¾ of family and staff (76.5%) agreed or strongly agreed that PWMLs enjoyed the 3D objects. More than 80% of family and staff members emphasized that the 3D objects helped PMWLs reminisce and remember the past more effectively (83.3%).
Although a considerable number of PWMLs seemed highly enthused about how the 3D objects stimulated reminiscence, some of the qualitative data implied concerns related to “triggering negative memories.” Although PWMLs would mention loss when viewing an object (e.g., a house burning or sold; a pet dying), the expressed concerns related to these memories did not seem to manifest negative reactions or behaviors among PWMLs:
“Yeah, I don’t know of any neg—I know some of the family members were concerned when I spoke to them initially they were concerned that having someone—bringing an object in of any sort might bring back negative memories. But I don’t think that anybody experienced that.” (Final staff focus group)
The qualified negative reactions to 3D objects and reminiscence were echoed in the system review checklist; for example, only 1/3 (33.4%) of family members and staff agreed or strongly agreed that there were time constraints when using 3D printing (an important consideration, as issues related to staff and family availability to engage in interventions are often noted as barriers when attempting to implement other long-term care interventions) [34]. No family members or staff (0.0%; 77.8% strongly disagreed or disagreed) felt that the PWML was “lost” using the 3D objects, which is also a critical feature when implementing a reminiscence intervention for persons in various stages of dementia. Similarly, very few (5.9%) family and staff members indicated that the 3D object and reminiscence process was confusing (88.3% strongly disagreed and disagreed with this statement). To provide further support, over 80% of family members and staff (83.4%) would use the 3D objects again when communicating and interacting with the PWML in the future and almost all would recommend the 3D object and reminiscence process to others in a similar situation (94.4%; although it is important to note that only half of family members and staff strongly agreed or agreed that they wished they would have known about the 3D objects sooner).
Recommendations to enhance utility and feasibility
Recommendations, particularly from staff members, provided a roadmap to further improve and refine the use of 3D objects to promote reminiscence for PWMLs. Categories identified in this theme included enhancing staff coordination and engagement; improving the reminiscence process; and group discussion of objects.
Participating staff members suggested several approaches to improve coordination between PWMLs, family members, and staff via the 3D objects, including a discussion booklet and a method to track which residents had which objects:
“As far as what would be helpful, the staff said it would be really great to have a discussion booklet with question examples on how to prompt reminiscence with these objects. Especially if the family doesn’t relay what the object is there for. If there could be a little [booklet] that was right underneath the object, or something that could kind of guide how they could talk about this object, instead of just saying, oh this is cool. Yeah. Then that would be very beneficial.” (Final staff focus group, field notes)
“Finally, [last] negative really was—it was really difficult to follow through and talk about the objects with the staff, because just timing was difficult, as well as, they weren’t really sure who had what objects all the time. So making sure that they knew where the objects were, and what the objects were, so that they could do the reminiscence, would be very helpful.” (Final staff focus group, field notes)
Although group engagement occurred informally in this project (see above), staff also recommended that this become more central to future implementation of printed 3D objects to promote reminiscence in their respective residential settings:
“Everyone liked the idea of group discussions with the objects. The daughter brought this up and stated, you know, if these objects could be used to meet other residents in the facility and discuss why this object is special to you, to the other residents in the facility, it could be a very beneficial group environment.” (Final staff focus group, field notes)
Engagement in study process
Another theme identified in the various qualitative data elements was PWMLs’ positive and negative engagement in study procedures. Categories that reflected this theme included resident emotional status, resident environment, and resident responsiveness during study activities. A number of quotes and field notes represented the theme of engagement in the study process; for example, the graduate research assistants often noted the affect of PWMLs during the various study procedures:
“When we went to (name of residential campus) we were told that we could meet with her in a meeting room that she had never been in. So we waited there for her, and her daughter brought her down in the wheelchair. When we all introduced ourselves she stated, why are you so happy? But she smiled and generally had a much better demeanor and a much brighter affect than she had the last time we met her...Overall, while she was very distractible—the last time we could barely get her to say a word. And so this was—she was remarkably more—just more upbeat and smiled a lot more, and talked much more.” (2-week session field notes)
The environment and physical surroundings of the PWML often played an important role when identifying appropriate 3D objects:
“She also had a lot of little mini-models from the Minnesota State Fair. I guess she has over 25 little bronze cast items. So we were thinking things related to the State Fair, or just knowing that she’s familiar with miniature models anyway, having a little cabin to go in that set would probably be something very special to her.” (Initial session field notes)
Further emphasis on the importance of the PMWL’s environment extended to some of the activities and planning that the long-term care setting engaged in; these environmental features helped to facilitate the identification and use of 3D objects for reminiscence and stimulation:
“And then, she also wanted us to know that every resident has a document created when they first move in, called Creating Wonderful Memories. And this is a document that tells about the resident’s past, especially things that they were very involved with, including volunteering, previous jobs, what they loved to do, family and friends, etc. And she also has information on good and bad triggers. She noted that there were a couple residents that had triggers that could cause a very emotional response, such as, one was very scared of dogs, one had a bad relationship with her husband. So those things could cause a bad trigger. So those are things to be aware of when we go in to figure out what 3D objects to use.” (Staff training session, field notes)
Responsiveness during study activities was also evident throughout the various research procedures; specifically, interviews and field notes suggested that as PWMLs and their family members progressed from the initial meeting to the introduction of objects to final interview sessions, participants seemed to enjoy their involvement and use of the 3D objects:
“It’s been fun...We’ve enjoyed it...Thank you...We’ve had a lot of fun.” (1-month session semi-structured interview)
The empirical data from the 3D printing review checklist (see Table 2) largely aligned with the qualitative data. For example, family members and staff were in strong agreement that the 3D objects were easy to use (94.5%). Moreover, almost all family members and staff agreed or strongly agreed that the research team (KJ, AG, and SR) was helpful when reviewing 3D objects and discussing them (94.5%).
Several aspects of the PWMLs’ environment made it difficult to fully utilize the 3D objects and reminisce effectively. In other instances PMWLs’ responsiveness was difficult to judge due to cognitive impairment or other issues:
“So this visit we didn’t get as much detail or as much reminiscence done as in previous visits, but it was still meaningful just to get a snapshot of where <the> participant is living and who he interacts with on a day to day basis. He said a lot of the residents aren’t interested in talking with him, or they don’t understand, or they can’t talk anymore. So I can understand that it might be lonely for him in the unit.” (1-month session field notes)
“She was very agreeable. I’m not sure if—at the time I wasn’t really sure if she actually liked doing those things, or nodded and smiled because they sounded like things that she would have done.” (Initial session field notes)
The reminiscence process
A theme that was identified and apparent throughout the various study procedures was the reminiscence process itself: this theme included categories related to how PWMLs and their family member identified objects (object identification process), PWMLs’ and family members’ reaction to objects (reaction to objects), participants’ level of engagement when reminiscing about 3D objects (participant engagement in 3D object-reminiscence process), and challenges to reminiscence (3D printing use was not for everyone).
The reminiscence process was observable immediately during the initial meeting with PWMLs. Objects selected ranged from pets to cabins to cars. The latter was a particularly popular choice for PWMLs (particularly automobile models from the 1950s) and often triggered memories for PWMLs:
“His guardian stated that when she was clearing out his house she found all these books. Apparently he (was) into a lot of different activities growing up. He enjoyed working on cars, he enjoyed fixing—his main job was fixing watches. When he was 18 he was stationed in Texas and Florida for the Air Force, guarding bombers. When we talked about cars—when we went into talking about cars, he said he could do it all, and really enjoyed fixing things. His favorite car was a Cadillac ‘51, blue. And Kari was able to find the car online, and the resident [clasped] his hands together and said, that’s it. And he was really excited about that. So I think that would be a really positive object to create. He stated, ‘I had it for a long time.’” (Initial session field notes)
Participants’ initially noted how beautiful and real the objects appeared:
“We showed her the object that we created, which was a small piano. And she said, well let me see that. Oh wow, it’s beautiful. This participant had such bright affect throughout our time when we were meeting with her. Since she played piano for a long time at St. Lawrence, the school that she attended and the church she attended, we thought the piano would be appropriate.” (2-week session field notes)
“As soon as we pulled out the objects, she stated, “Oh, how cute. This looks just like the house I grew up in...Regarding the dog <name here> she stated, “Oh my. That just about looks like her.” (2-week session field notes)
Data from the 3D printing review checklist supported the qualitative data; nearly 90% of family and staff reported that the objects generated by 3D printing were well-received by the PWML (88.9%). Similarly, family and staff were unanimous that the 3D objects were perceived as clear and easy to use for PWMLs (100%).
The presentation of objects was often followed by reminiscence on the part of the PWML and family member:
“And then, we went on to the Vikings football. There was a football that had a stand, and it actually came apart from the stand. And he joked several times about kicking it, or throwing it, but then went into how sad he was about the missed kick this past year. And he listed off many different players by name. And said, ‘They did good. Just not good enough.’” (2-week session field notes)
Both family and staff engagement in the reminiscence process appeared to facilitate the cognitive stimulation of PWMLs as well:
“But what was kind of interesting was when her son came in, and I went in to say hi, and I said have you seen this little cabin, this little mock-up of the cabin? And he pulled it down and he said, that’s incredible. It looks just like the cabin. It looks just like it. How do they do that? And then his mom would come back and say, well, it’s a little different. And he would say, well, it is a little different. And then they would start talking about the differences, and what was important about making sure that the stairs were just right....But it was so cool, because they must have spent an hour together talking about the cabin and all the fun times they had, and what it was like to have all the kids up there in the summer, and how her husband built it, and how he did that, and chopping down the trees. I mean they just went through the entire process together as a son and mother.” (Final staff focus group)
Staff encouraged residents to bring objects to group activities to discuss and share, which seemed to result in individual and group reminiscence:
“Well the one with the tricycle. I brought the cabin out one time when (name of PWML) was sitting out, and that generated a lot of discussion about going up north in the summers, and some people didn’t have cabins, but they had friends who had cabins. And camping, you know, talking about it. So, yeah. And even (name of PWML)’s son brought the cabin out one time that he was there and they kind of started talking about—. And then, if I remember right, we also launched into discussions about building your own home, or building your own place. Cause a lot of people in this generation did that.” (Final staff focus group)
These qualitative insights paralleled the empirical data collected on the 3D printing review checklist; over 80% (83.3%) agreed or strongly agreed that PWMLs were provided with a sufficient number of 3D objects to fully engage with.
Descriptive quantitative data and the themes, categories, and exemplar text derived from the qualitative data suggest the success and depth of the 3D object facilitation process. However, in several instances it was apparent that 3D printing did not work successfully for all participants. In particular, memory impairment, behavioral issues, and resulting communication issues hindered object identification and reminiscence:
AG: :..what do you like about these objects?
PWML: What do I like about this? I’ve never seen it before?
AG: Well, what do you like about it?
PWML: It’s just small. Just a toy.
AG: What is it?
PWML: It’s an accordion, I would say.
AG: Does it remind you of anything?
PWML: Hm?
AG: Does it remind you of playing the accordion?
PWML: Doesn’t remind me of that, but it reminds me of [working there?] . It is # an accordion, wasn’t it?
AG: Do you think this helps you at all?
PWML: What?
AG: Do you think it helps you just remembering playing the accordion?
PWML: I don’t know.
(1-month session semi-structured interview)
“When we first started off this morning one of the staff members whispered to us that <the> participant woke up very, very crabby this morning. Which was interesting, because she was one of…the most agreeable and engaging and friendly residents we’ve worked with thus far in the research project. So when we approached the resident and said hi, she didn’t say anything. She was in the middle of an exercise group, and everyone was seated in chairs or in wheelchairs around the exercise instructor. And the exercise instructor said, “There are some people here that want to see you and visit with you.” And (the) participant shot up from her chair and said, “I guess I’ll just do what anyone says, because no one care about me. I have no say in anything. Nobody even gives a damn.” So on her way out of the exercise activity room, she was pushing in a chair and slammed it up against the table, was walking very fast in front of KJ and I...” (it is important to note that following a conversation with the activity director of the facility, the PWML emerged from her room holding hands with the activity director and had stated that “she really, really wanted to talk to us and meet with us in the activity room…So she came out of her room, seemed completely engaging and fine and very kind and had a very open and calm demeanor, and was cracking jokes, and it didn’t seem apparent to KJ or I that she had any recollection that this had happened—with her outburst.”
(2-week session field notes)
DISCUSSION
The goal of this study was to determine the feasibility and utility of implementing 3D printed objects in reminiscence-based activities for PWMLs, family members, and professional care staff. The integrated qualitative and quantitative data strongly suggested that PWMLs enjoyed using the 3D objects, were engaged when interacting with the objects, and appeared to value the objects due to their personalized characteristics. The use of 3D printed objects also appeared to facilitate family involvement and family members’ and staff persons’ interactions with PWMLs. There were some challenges to using the objects, including PWMLs’ memory impairment and behavioral issues.
Many PWMLs offered positive initial reactions to the 3D objects. Persons with memory loss’ frequently noted that the objects were “beautiful” and appeared very real upon initial presentation, and family members felt that the objects were well-received by PWMLs in general. The unveiling of objects also tended to spark immediate memories. Many PWMLs asked to hold the object while they were speaking, as if to trace where events happened around the object or to point to areas of the object that were significant. Persons with memory loss were able to hold the focus of reminiscence in their hands, point to similarities and differences between the real object and the 3D object, and actively engage with others while interacting with the object [15]. For example, one PWML placed a replica of a camper on the table, and pointed to each window while explaining what happened in each area; the resident also moved their finger along the table to explain the location of a fire pit or where the PWML’s children played outside the camper. This example suggests that having an object to physically interact with, hold, move, and view from various angles holds particular potential as a reminiscence aid. In another example, the use of a 3D object appeared to enhance the reminiscence process while also viewing a picture simultaneously:
“When we showed a picture of the house, because we were able to find a picture online of the current house, both the participant and her husband used the objects to describe the locations of doors that couldn’t be seen in the pictures, and compared and contrasted.” (1-month session field notes)
Additional qualitative data inferred that it was less useful to compare whether pictures or 3D objects were more effective than the other; instead, using both in tandem enhanced the reminiscence experience:
“Then KJ brought out the…tablet and showed the participant Jane Arden paper dolls that she used to get in the paper. (The participant) brightened up looking at the paper doll photos and said, “I used to wait for the paper to come every day.” She was very perceptive and alert, and very expressive in her eyes and face. She continued to hold the piano, and touched along the keys while we were talking about the paper dolls” (2-week session field notes)
The reminiscence process was often initiated by identifying objects that were important to PWMLs and which they or their family felt would stimulate memories. Pets, cabins and cars were often selected. Previous studies have found that reminiscence helps to improve communication between PWMLs and their caregivers [35]. Similarly, when family members participated in reminiscence with PWMLs in the current study, PWMLs’ verbal engagement occurred as well. If staff or family members were present, they at times offered prompts or probing questions to help the PMWL recall a significant story or memory attached to a given 3D object. This engagement occasionally uncovered new information which family or staff had not known about prior to the use of 3D objects. In some instances, even when the objects were not exactly the same as the original, positive interactions between PWMLs and family members occurred when reviewing similarities and differences. Staff at one site noticed this dynamic during one facility group session, as a replica tricycle instigated discussion among group members for about twenty minutes as its wheels were a different color than the original tricycle. Similar to previous studies which found RT has the potential to increase autobiographical memory, social interaction, and staff knowledge of PWMLs [8,36], the level of PWMLs’ engagement was apparent when staff led informal group activities to discuss objects above and beyond the 2-week and 1-month individual reminiscence sessions. Staff members perceived additional engagement when allowing PMWLs to reminisce about their 3D objects in group activity sessions and then relate the object to common themes that other participating group members could discuss.
Context often drives behavior, and PWMLs’ environments appeared to facilitate or hinder their level of engagement in the study. Unfamiliar environments, disruptive noise levels, and visits by the research team with little warning had an adverse effect on residents’ reminiscence process. In contrast, PWMLs who reminisced in their rooms, in a familiar meeting room area, or with family members present typically contributed more verbally and elaborated to a greater extent on stories when compared to PWMLs in an unfamiliar setting or without family members present. Louder environments posed distractions, and residents at times would quietly narrate or comment on what was going on in their environment thereby losing focus on the reminiscence questions. Residents who were woken up suddenly from a nap or PWMLs who were not notified in advance of visitors typically took longer to respond to questions or appeared less talkative initially. Other challenges, including PWMLs’ memory impairment and behavioral issues, tended to stifle the reminiscence and stimulation process that often took place otherwise.
The feasibility and utility findings emphasize that 3D printing offers an important physical medium for PWMLs to share their memories and connect with family members and care staff. Persons with memory loss could turn and view objects from all angles, move and position objects as needed, and touch a given object when engaging in reminiscence activity. It appeared that this multisensory approach aided PWMLs’ abilities to access memories and represented a physical resource that allowed for connection with others [15]. Prior reviews and controlled studies have indicated that touch has the potential to reduce agitation and stress (as measured by cortisol levels) among persons with Alzheimer’s disease; the tactile properties of 3D objects may operate in a similar fashion [16–18]. The prompts and encouragements offered by family members and staff during reminiscence sessions were further facilitated by the presence of the 3D printed objects [5]. The objects also allowed PWMLs to have complete ownership over their stories and how they presented themselves in relation to the objects; this sense of ownership is an important aspect of person-centered dementia care [37]. Similarly, the 3D objects featured a high degree of personalization that makes this approach a novel and important technological advance when supplementing RT [4]. The potential benefits of 3D objects appeared to extend to group activity sessions, when other residents could understand what the PWML was describing via the physical presence of the object [6].
In addition to the challenges indicated above, there were several other study limitations. Time constraints were a concern, as some family members could not participate regularly in reminiscence sessions. As the mixed methods findings of this study infer, reminiscence with 3D objects is most beneficial when family members are present to facilitate storytelling and recollection. Further, independent initiation of reminiscence by PWMLs may be challenging given their cognitive impairments; instead, optimal use of 3D objects in residential long-term care would likely occur during structured activity (although it is important to note that the current study did not conduct informal observation of how PWMLs may have used or shared objects during unstructured time). We would argue that there are not necessarily time constraints to using 3D printed objects themselves (as their use by PWMLs, family members, or staff are anticipated to be largely self-initiated) but instead reflect the time pressures on staff to incorporate additional, formalized activities (such as reminiscence) into already busy schedules. Providing a picture or list of objects that could be inserted on a resident’s door or chart so that staff realize which objects belong to each resident could help to encourage further engagement with residents regarding their objects and their meaning to them. As the current study focused on feasibility and utility testing, no conclusions are possible regarding the efficacy of 3D printed objects in exerting clinically and statistically significant effects on key PWML, family member, and staff outcomes. Similarly, when participants (e.g., family, staff) indicated that the PWML was more “engaged,” it was in response to what the perceived engagement levels of PWMLs were prior to the project. However, these are retrospective reports. This sample lacked ethnic and racial diversity. As noted by staff, inclusion of questions or a guide that staff or visitors could use to help direct discussions of 3D objects may also allow for their more effective use.
There are practical implications of these results. A major clinical and policy initiative in residential and/or Alzheimer’s disease care is the shift towards person-centered care principles in order to increase quality of life for PWMLs. In particular, non-pharmacological interventions are thought to potentially benefit PWMLs’ quality of life by improving emotional, physical, and perhaps cognitive health [3]. Introduction of new interventions can be difficult to sustain due to the challenges of “changing the culture” of residential long-term care settings, funding, and staff availability [38]. Since 3D printed objects can be used flexibly (i.e., individually or within groups) and require little to no training to use, the integration of such objects into reminiscence or other therapeutic activities for PWMLs has high feasibility and translational potential.
CONCLUSIONS
The current study findings demonstrate that 3D printing technology has evolved so that objects can be made with high fidelity to provide a positive and individualized reminiscence experience. These objects may also be used with ease by PWMLs, family and staff to promote reminiscence of PWMLs’ autobiographical histories and promote discussion and communication between PWMLs, family members, and staff. Individualized prompts may aid in reminiscence [39], so the incorporation of 3D objects which are completely individualized to the PWML may increase the positive effects of reminiscence and begin to achieve the ultimate goal of person-centered care. Although further studies are needed to determine the scientific efficacy of 3D printed technology as a supplement to RT, the current study supports 3D printing as a feasible, potentially promising approach that can enhance dementia care.
Supplementary Material
ACKNOWLEDGMENTS
The authors would like to thank the residents, family members, and staff of Martin Luther Care Center in Bloomington, MN and Nine Mile Creek Senior Living in Bloomington, MN for their gracious contribution of time. The authors would also like to thank Gary Havey of Advanced Medical Electronics for his assistance.
This research was supported by R43 AG049548 from the National Institute on Aging to Moai Technologies (T. Plocher, Principal Investigator) and K02 AG029480 from the National Institute on Aging to the University of Minnesota (J. E. Gaugler, Principal Investigator). Ms. Johnson, Mr. Plocher, Mr. Havey and Dr. Klassen are paid employees of Moai Technologies, LLC.
Footnotes
DECLARATION OF INTEREST
REFERENCES
- [1].Alzheimer’s Disease International . World Alzhiemer report 2016. London, UK: Alzheimer’s Disease International; 2016. [Google Scholar]
- [2].Haupt M, Karger A, Janner M . Improvement of agitation and anxiety in demented patients after psychoeducative group intervention with their caregivers. Int J Geriatr Psychiatry 2000;15:1125–1129. [DOI] [PubMed] [Google Scholar]
- [3].Mitchell G, Agnelli J. Non-pharmacological approaches to alleviate distress in dementia care. Nurs Stand 2015;30:38–44. doi: 10.7748/ns.30.13.38.s45 [doi]. [DOI] [PubMed] [Google Scholar]
- [4].Lazar A, Thompson H, Demiris G. A systematic review of the use of technology for reminiscence therapy. Health Educ Behav 2014;41:51S–61S. doi: 10.1177/1090198114537067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Lancioni GE, Singh NN, O’Reilly MF, et al. A computer-aided program for helping patients with moderate Alzheimer’s disease engage in verbal reminiscence. Res Dev Disabil 2014;35:3026–3033. doi: 10.1016/j.ridd.2014.07.047 [doi]. [DOI] [PubMed] [Google Scholar]
- [6].Hamel AV, Sims TL, Klassen D, et al. Memory matters: A mixed-methods feasibility study of a mobile aid to stimulate reminiscence in individuals with memory loss. J Gerontol Nurs 2016;42:15–24. doi: 10.3928/00989134-20160201-04 [doi]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Butler RN. The life review: an interpretation of reminiscence in the aged. Psychiatry. 1963;26:65–76. [DOI] [PubMed] [Google Scholar]
- [8].Subramaniam P, Woods B. The impact of individual reminiscence therapy for people with dementia: systematic review. Expert Rev Neurother 2012;12:545–555. doi: 10.1586/ern.12.35;10.1586/ern.12.35. [DOI] [PubMed] [Google Scholar]
- [9].Bailey EM, Stevens AB, LaRocca MA, et al. A randomized controlled trial of a therapeutic intervention for nursing home residents with dementia and depressive symptoms. J Appl Gerontol 2016. doi: 0733464815627956 [pii]. [DOI] [PubMed] [Google Scholar]
- [10].Duru Aşiret G, Kapucu S. The effect of reminiscence therapy on cognition, depression, and activities of daily living for patients with Alzheimer disease. J Geriatr Psychiatry Neurol 2016;29:31–37. doi: 10.1177/0891988715598233 [doi]. [DOI] [PubMed] [Google Scholar]
- [11].Gonzalez J, Mayordomo T, Torres M, et al. Reminiscence and dementia: a therapeutic intervention. Int Psychogeriatr 2015;27:1731–1737. doi: 10.1017/S1041610215000344 [doi]. [DOI] [PubMed] [Google Scholar]
- [12].Huang HC, Chen YT, Chen PY, et al. Reminiscence therapy improves cognitive functions and reduces depressive symptoms in elderly people with dementia: a meta-analysis of randomized controlled trials. J Am Med Dir Assoc 2015;16:1087–1094. doi: 10.1016/j.jamda.2015.07.010 [doi]. [DOI] [PubMed] [Google Scholar]
- [13].Ito T, Meguro K, Akanuma K, et al. A randomized controlled trial of the group reminiscence approach in patients with vascular dementia. Dement Geriatr Cogn Disord 2007;24:48–54. doi: 000103631 [pii]. [DOI] [PubMed] [Google Scholar]
- [14].Boulay M, Benveniste S, Boespflug S, et al. A pilot usability study of MINWii, a music therapy game for demented patients. Technol Health Care 2011;19:233–246. doi: 10.3233/THC-2011-0628 [doi]. [DOI] [PubMed] [Google Scholar]
- [15].Sanchez A, Marante-Moar MP, Sarabia C, et al. Multisensory stimulation as an intervention strategy for elderly patients with severe dementia: a pilot randomized controlled trial. Am J Alzheimers Dis Other Demen 2016;31:341–350. doi: 10.1177/1533317515618801 [doi]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Millan-Calenti JC, Lorenzo-Lopez L, Alonso-Bua B, et al. Optimal nonpharmacological management of agitation in Alzheimer’s disease: challenges and solutions. Clin Interv Aging 2016;11:175–184. doi: 10.2147/CIA.S69484 [doi]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Hawranik P, Johnston P, Deatrich J. Therapeutic touch and agitation in individuals with Alzheimer’s disease. West J Nurs Res 2008;30:417–434. doi: 10.1177/0193945907305126 [doi]. [DOI] [PubMed] [Google Scholar]
- [18].Woods DL, Dimond M. The effect of therapeutic touch on agitated behavior and cortisol in persons with Alzheimer’s disease. Biol Res Nurs 2002;4:104–114. [DOI] [PubMed] [Google Scholar]
- [19].Baker R, Bell S, Baker E, et al. A randomized controlled trial of the effects of multi-sensory stimulation (MSS) for people with dementia. Br J Clin Psychol 2001;40:81–96. [DOI] [PubMed] [Google Scholar]
- [20].Creswell JW, Plano Clark VL. Designing and conducting mixed methods research. 2nd ed Thousand Oaks, CA: SAGE Publications, Inc.; 2010. [Google Scholar]
- [21].O’Cathain A, Murphy E, Nicholl J. The quality of mixed methods studies in health services research. J Health Serv Res Policy 2008;13:92–98. [DOI] [PubMed] [Google Scholar]
- [22].Tariq SH, Tumosa N, Chibnall JT, Perry MH 3rd, et al. Comparison of the Saint Louis university mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder: A pilot study. The American Journal of Geriatric Psychiatry 2006;14:900–10. [DOI] [PubMed] [Google Scholar]
- [23].Tariq SH, Tumosa N, Chibnall JT, Perry MH 3rd, et al. Comparison of the Saint Louis University Mental Status Examination and the Mini-Mental State Examination for detecting dementia and mild neurocognitive disorder--a pilot study. Am J Geriatr Psychiatry 2006;14:900–910. [DOI] [PubMed] [Google Scholar]
- [24].Gibson F The past in the present. Baltimore, MD: Health Professions Press; 2004. [Google Scholar]
- [25].Haight B, Gibson F. Burnside’s working with older adults. Sudbury, Massachusetts: Jones and Bartlett Publishers, Inc.; 2005. [Google Scholar]
- [26].Link AL. Group work with elders: 50 therapeutic exercises for reminiscence, validation, and remotivation Sarasota, FL: Professional Resource Press; 1997. [Google Scholar]
- [27].Sim R Reminiscence: Social and creative activities with older people in care. Bicester, Oxon, UK: Winslow Press Ltd; 1997. [Google Scholar]
- [28].Van Bogaert P, Van Grinsven R, Tolson D, et al. Effects of SolCos model-based individual reminiscence on older adults with mild to moderate dementia due to Alzheimer disease: a pilot study. J Am Med Dir Assoc 2013;14:528.e9–528.13. doi: 10.1016/j.jamda.2013.01.020 [doi]. [DOI] [PubMed] [Google Scholar]
- [29].Gaugler JE, Reese M, Tanler R. Care to Plan: an online tool that offers tailored support to dementia caregivers. Gerontologist 2016;56:1161–1174. doi: 10.1093/geront/gnv150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Strauss A, Corbin J. Basics of qualitative research: techniques and procedures for developing grounded theory. Thousand Oaks, CA: SAGE Publications, Inc.; 1998. [Google Scholar]
- [31].Morse JM, Niehaus L. Mixed method design: principle and procedures (developing qualitative inquiry). Walnut Creek, CA: Left Coast Press; 2009. [Google Scholar]
- [32].Morse JM, Field PA. Qualitative research methods for health professionals. Thousand Oaks, CA: SAGE Publications; 1995. [Google Scholar]
- [33].Luborsky MR. The identification and analysis of themes and patterns In: Gubrium JF, Sankar A, eds. Qualitative methods in aging research. Thousand Oaks, CA: Sage Publications; 1994:189–210. [Google Scholar]
- [34].QSR International Pty Ltd. NVivo qualitative data analysis software. Version 10. 2012. [Google Scholar]
- [35].Gaugler JE, Hobday JV, Robbins JC, Barclay MP. Direct care worker training to respond to the behavior of individuals with dementia: the CARES® dementia-related behavior online program. Gerontol Geriatr Med 2016;2:2333721415626888. doi: 2333721415626888 [pii]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Allen RS. The legacy project intervention to enhance meaningful family interactions: case examples. Clin Gerontol 2009;32:164–176. doi: 10.1080/07317110802677005 [doi]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Cotelli M, Manenti R, Zanetti O. Reminiscence therapy in dementia: a review. Maturitas. 2012;72:203–205. doi: 10.1016/j.maturitas.2012.04.008 [doi]. [DOI] [PubMed] [Google Scholar]
- [38].McEvoy P, Eden J, Plant R. Dementia communication using empathic curiosity. Nurs Times 2014;110:12–15. [PubMed] [Google Scholar]
- [39].Gaugler JE, Yu F, Davila HW, et al. Alzheimer’s disease and nursing homes. Health Aff 2014;33:650–657. doi: 10.1377/hlthaff.2013.1268 [doi]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Dempsey L, Murphy K, Cooney A, et al. Reminiscence in dementia: a concept analysis. Dementia 2014;13:176–192. doi: 10.1177/1471301212456277 [doi]. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.