

Case
A 56-year-old Indian male, silversmith by occupation, presented with gradually progressive loss of vision in both eyes. Best-corrected visual acuity in the right eye was 6/9 and in the left eye was 6/60. Lid and adnexa were normal. In both eyes, conjunctiva had gray-black pigmentation of medial bulbar conjunctiva, which was more prominent at the medial canthal region. Cornea had diffuse confluent deposits at the level of Descemet's membrane [Fig. 1], which were seen as hyperreflective shadows in anterior segment optical coherence tomography (OCT). Lens showed nuclear sclerosis grade 2 with posterior subcapsular cataract in the right eye and near mature cataract in the left eye. Intraocular pressure, gonioscopic evaluation of angles, and specular microscopy were normal. Fundus evaluation was normal in the right eye while details in the left eye were not clear due to dense cataract. B scan in the left eye was normal. Upper and lower limbs showed slate-gray pigmentation along with pigmentation of nails [Fig. 2]. Serum silver levels were raised, 2.3 μg/ml (normal <2 μg/ml). After written informed consent, patient underwent left eye manual small incision cataract surgery, during which lens matter was collected and sent for histopathological evaluation. It showed evidence of diffuse deposits of silver which were confirmed using hematoxylin and eosin (H and E) stain and were refractable in dark field illumination [Fig. 3]. Post cataract surgery, patient underwent Humphrey's 30-2 visual field analysis, macular optical coherence tomography (OCT) and fundus fluorescein angiography (FFA), which were normal.
Figure 1.
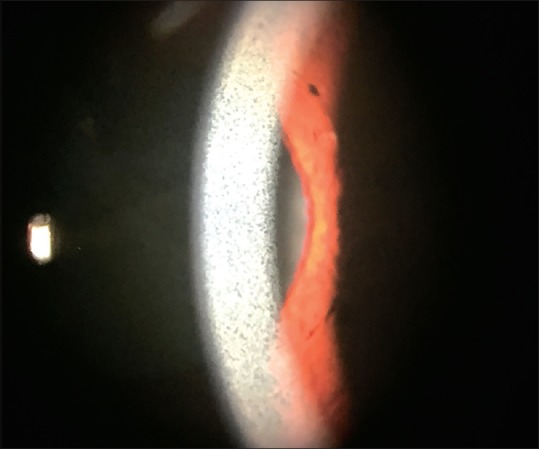
Slit lamp photograph showing diffuse deposits in the deeper layer of cornea
Figure 2.
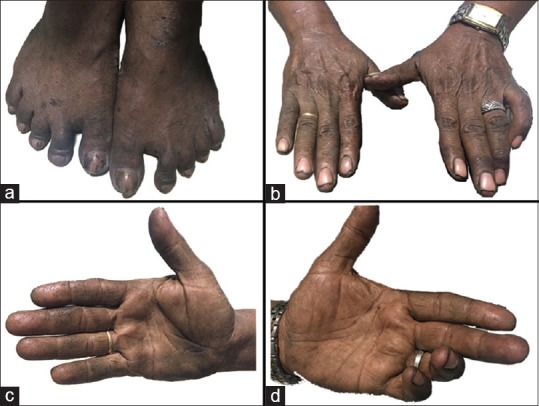
Pictures showing slate grey pigmentation of limbs and nails (a and b) and palmar surfaces of hands (c and d) which is presumed to be due to deposition of silver
Figure 3.
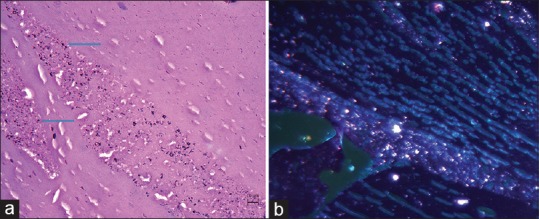
H and E (Hematoxylin and eosin) sections studied from the lens nucleus tissue (a) shows diffuse deposition of black granules (pointed by blue colored arrows) suggestive of silver particles which are refractable in dark field illumination (b)
Discussion
Silver deposits can be noted in the elastic fibers of the connective tissue and basement membranes including the eyelids, conjunctiva, lacrimal sac, lens, ciliary body, and Bruch's membrane. In cornea, deposits have been noted within Bowman's membrane, corneal stroma, and Descemet's membrane, causing its discoloration.[1,2,3,4] The presence of silver in a cataractous lens can be debated as silver deposits in senile cataract or cataract induced by silver deposits.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We would like to thank Dr. Shanthi R, Ocular pathologist, Aravind Eye Hospital, Anna Nagar, Madurai for doing histopathological evaluation of the lens matter.
References
- 1.Kamath Y, Sinha A. Ocular argyrosis in a jeweller. BMJ Case Rep 2013. doi: 10.1136/bcr-2013-009742. doi: 10.1136/bcr-2013-009742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pala G, Fronterré A, Scafa F, Scelsi M, Ceccuzzi R, Gentile E, et al. Ocular argyrosis in a silver craftsman. J Occup Health. 2008;50:521–4. doi: 10.1539/joh.n8001. [DOI] [PubMed] [Google Scholar]
- 3.Wadhera A, Fung M. Systemic argyria associated with ingestion of colloidal silver. Dermatol Online J. 2005;11:12. [PubMed] [Google Scholar]
- 4.Tendler I, Pulitzer MP, Roggli V, Abramson DH, Marr BP. Ocular argyrosis mimicking conjunctival melanoma. Cornea. 2017;36:747–8. doi: 10.1097/ICO.0000000000001191. [DOI] [PMC free article] [PubMed] [Google Scholar]