

Abstract
Background
To improve access to surgical service and to reduce neonatal mortality Ethiopia implemented surgical task shifting to nonphysician surgeons (NPSs). We aim at assessing surgical outcomes between NPSs and physician surgeons working in two hospitals.
Methods
We collected data from two hospitals on 474 maternal medical records. Completed maternal medical records were included in this study. Data were entered into Epi Info version 7 and analyzed by SPSS version 20 software. Both descriptive and inferential statistics were done. If the 95% confidence interval values exclude the null value, the factor was considered as a significant factor.
Result
Totally, 3429 mothers delivered in two hospitals. Of them, 840 (24.5%) delivered by caesarian section (CS), but 474 mothers' records meet the inclusion criteria included in this study. Of 474 CS deliveries, the majority (82%) of them were performed by NPS. Maternal or fetal emergency conditions were the main reasons (92.0%, n=436) for CS. Task shifting does not affect immediate newborn outcomes (ARR, 1.24 (0.55, 2.78)), but duration of hospitalization (ARR: 4 (2.3, 7.5)), condition of the fetus during admission (ARR: 5.22 (2.9, 9.2)), and type of anesthesia used (ARR: 0.2 (0.1, 0.4)) significantly determine the outcome.
Conclusion
Surgical task shifting to NPS does not affect the immediate newborn outcome. But general anesthesia is one of the major factors that affects the outcome.
1. Introduction
Surgical care task shifting to nonphysicians is a common practice in most developing countries [1]. Ethiopia implemented task shifting to NPSs, (they are BSc health officers or BSc nurses plus a 4-year training on integrated emergency surgery and obstetrics) to overcome the dire shortage of physicians, to improve access to medical and surgical care service, and to reduce maternal and neonatal mortality [2–6].
Neonatal mortality is one of the major health problems of Ethiopia. Surgical task shifting is an intervention supposed to reduce the rate of neonatal mortality [7–9]. Emergency Obstetric and Newborn Care (EmONC) is another strategy to reduce neonatal mortality [10]. EmONC is best implemented in developing countries through surgical task shifting. There is evidence from different countries on significant reduction of neonatal mortality due to EmONC implementation [7, 11]. This is because surgical intervention of EmONC creates a window to save the life of both mother and fetus due to emergency conditions during pregnancy. An emergency condition is a major reason for CS [12–18].
Different scholars reveal that there is an improvement on access to CS service and reduction of neonatal mortality after implementation of surgical task shifting [1, 12–14, 19]. There are findings from Ethiopia that assess the quality of CS service and its rate; but this research assesses the effect of surgical task shifting on neonatal birth outcomes [12, 15, 16, 20, 21].
2. Methods and Materials
A retrospective cohort study design was used to assess the rate of CS delivery and the relationship between NPS and CS outcomes. Data were collected from July 1 to 30, 2017. The study was conducted in Arba Minch General Hospital and Sawla District Hospital. These hospitals were selected because they qualify Comprehensive EmONC standard [20].
Mothers who gave birth by CS from July 2015 to June 2016 and all those who meet inclusion criteria (fully recorded medical record, mothers who give birth after arrival to the hospital, and both the mother and fetus are alive at the time of arrival to the hospitals) were included in this study. Data were collected by data abstraction tools adopted from averting maternal death and disability program module [10]. We collected data on the condition of mother and fetus during admission, who conducts CS, different tasks done during the procedure, and status of the newborn until the time of discharge. Experienced midwives and anesthetists were used to collect data after attending one-day training on how to collect the data. Ethical clearance was obtained from the South Region Health Research Ethics Review Committee.
Data were entered into Epi Info version 7 and analyzed using SPSS version 20. We did both descriptive and analytic statistics. Initially, binary logistic regression was performed to assess the association between each exposure and outcome variables. During bivariate analysis, variables with P value 0.2 were considered for multivariate binary logistic regression. When 95% confidence interval values exclude null value the factors considered as a significant factor. The immediate newborn outcome was categorized into good and bad. The good outcome means when the newborn is alive during birth without distress, and bad outcome means when there is a prenatal death or lives birth with distress.
3. Results and Discussion
3.1. Results
3.1.1. Participants in the Study
Totally, 3429 deliveries were attended in two hospitals, and of them 840 (24.5%) were delivered by CS. But only 474 mothers who fulfilled the inclusion criteria were included in this study (Figure 1).
Figure 1.
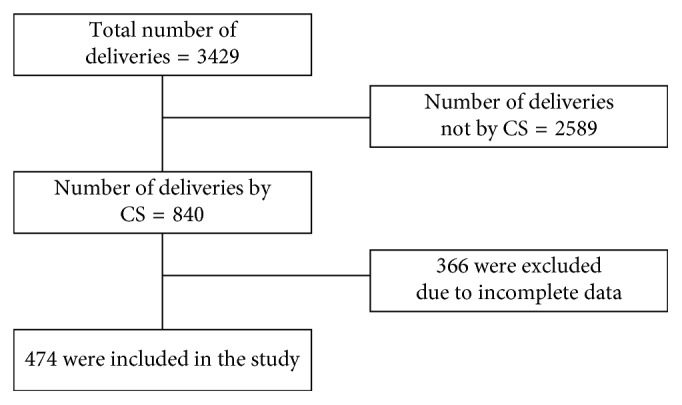
Schematic presentation of sampling procedure at selected health institutions, July 2015–June 2016 (n=474).
3.1.2. Characteristics of Mothers
From the total population, the majority (58%) of mothers were in the age group between 15 and 25: 189 (39.5%) mothers were nulliparous (not given birth before), and 64 (13.5%) mothers have more than 5 children. Greater than 60% of mothers were rural by residence, and 222 (48.2%) mothers come to hospital referred from rural health centers. At the time of admission, 159 (33.5%) mothers and 157 (33.1%) fetuses had an unstable vital sign. Only 152 (32.1%) mothers' medical registrations have data on the time interval from decision to perform CS to actual incision time.
3.1.3. Indications for Cesarean Section
Of the 474 CS deliveries, 436 (92%) were performed because of emergency conditions. But 85% of CS were due to cephalopelvic disproportion (CPD), fetal distress, malpresentation, previous CS scar, multiple gestation, and antipartum hemorrhage; 131 (28%), 102 (21%), 67 (14%), 43 (9%), 36 (8%), and 25 (5%), respectively (Figure 2).
Figure 2.
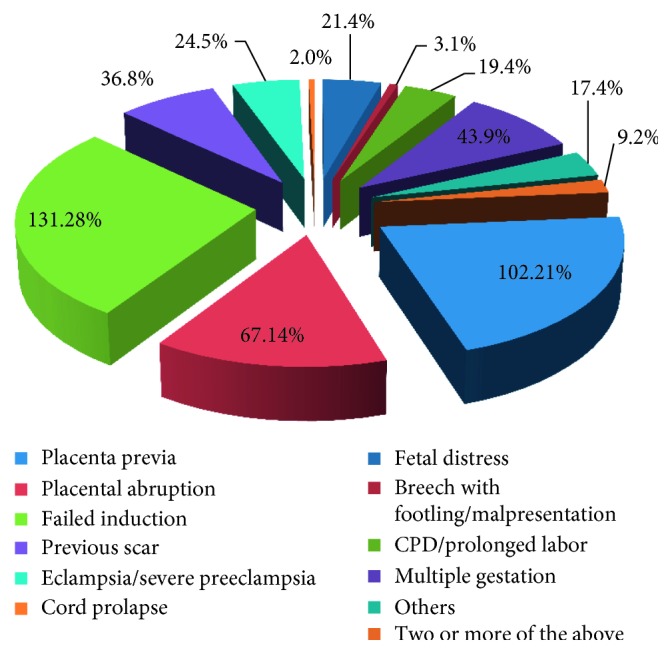
Indications for cesarean section at selected health institutions, July 2015–June 2016 (n=474).
Often, spinal anesthesia and lower uterine segment transverse CS were used in 379 (79.1%) and 464 (96.9%) mothers, respectively. The majority (82%) of procedures were performed by nonphysician surgeons. The average time of the procedure was 51 (SD 18.62) minutes (Figure 3).
Figure 3.
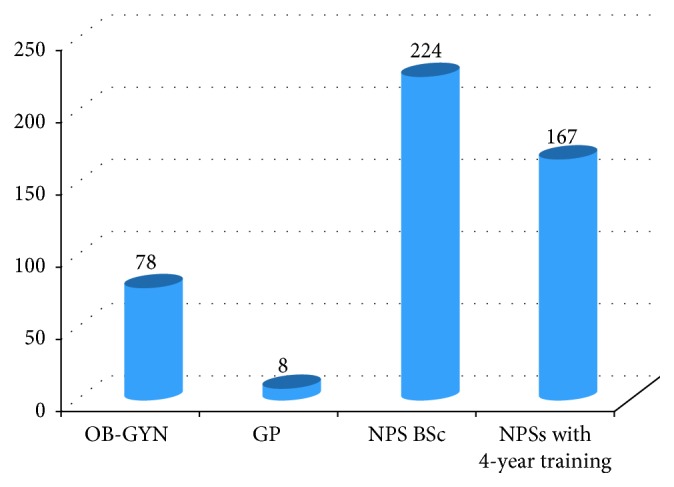
Types of staff members that performed the cesarean section in two hospitals, July 2015–June 2016 (n=474).
For 176 (37%) mothers, labor was managed by partograph, but 144 (82%) of them were completely filled. The average length of hospitalization was 5 (SD ± 2) days. Estimated average blood loss is 495 ml (SD ± 156). Of the total mothers undergone CS, only 33 (6.9%) mothers were blood transfused; 31 mothers transfusion were prescribed by NPSs.
3.1.4. Complication and Death
This study revealed 40 (8.4%) deaths and 33 (6.7%) complications, totally 73 (15.2%) bad immediate CS outcomes (Table 1).
Table 1.
Immediate newborn outcome of CS delivery from July 2015 up to June 2016.
| Factor | Number (%) | ||
|---|---|---|---|
| Outcome of newborn | Normal live birth | 401 | 83.7 |
| Live birth with distress | 32 | 6.7 | |
| Dead | 24 | 5.0 | |
| One or more death for twin | 16 | 3.3 | |
|
| |||
| Death | Stillbirth | 15 | 68.2 |
| Early neonatal death | 7 | 31.8 | |
|
| |||
| Primary cause of stillbirth | Asphyxia and trauma | 14 | 70 |
| Infection or pneumonia | 1 | 5 | |
| Trauma | 1 | 5 | |
| Other | 2 | 10 | |
| Unknown | 1 | 5 | |
| No information | 1 | 5 | |
3.1.5. Factors Determining Outcomes of CS Delivery
Other than the type of staff, time of hospitalization (ARR: 2.96, 95% CI (1.4, 6.26)), condition of the fetus during admission (ARR: 3.53 95% CI (1.97, 6.31)), and the type of anesthesia used for surgery (ARR: 4.19, 95% CI (2.26, 7.77)) significantly determined immediate CS birth outcomes (Table 2).
Table 2.
Factors affecting newborn outcome of cesarean delivery.
| Factor | Death/distress of newborn | COR (95% CI) | AOR (95% CI) | ||
|---|---|---|---|---|---|
| No | Yes | ||||
| Age | 15–25 | 238 | 37 | 1 | |
| 26–35 | 148 | 31 | 1.3 (0.8, 2.26) | ||
| > = 36 | 15 | 5 | 2.1 (0.7, 6.2) | ||
|
| |||||
| Residence | Urban | 157 | 14 | 1 | |
| Rural | 231 | 56 | 2.9 (1.5, 5.5) | ||
|
| |||||
| Parity | Nulliparous | 163 | 24 | 1 | |
| Primiparous | 103 | 13 | 0.8 (0.4, 1.7) | ||
| Multiparous | 88 | 19 | 1.46 (0.76, 2.8) | ||
| Grand multiparous | 47 | 17 | 2.31 (1.13, 4.7) | ||
|
| |||||
| Mother referred | No | 212 | 25 | 1 | |
| Yes | 173 | 47 | 2.4 (1.4, 4) | ||
|
| |||||
| Condition of fetus | Well | 289 | 26 | 1 | 1 |
| Any sign of complication | 110 | 47 | 4.9 (2.9, 8.4) | 3.53 (1.97, 6.31) | |
|
| |||||
| Condition of mother | Stable vital sign | 273 | 42 | 1 | |
| Critical | 124 | 31 | 1.7 (0.99, 2.8) | ||
|
| |||||
| Time on labour | Normal | 239 | 34 | 1 | |
| Prolonged | 114 | 33 | 2 (1.2, 3.4) | ||
|
| |||||
| Type of anesthesia | Spinal | 338 | 37 | 1 | 1 |
| General | 63 | 36 | 5.2 (3, 8.9) | 4.19 (2.26, 7.77) | |
|
| |||||
| CS classified | Emergency | 365 | 71 | 1 | |
| Elective | 27 | 1 | 5.1 (0.69, 38.7) | ||
|
| |||||
| Duration of procedure | ≤30 minute | 80 | 18 | 1 | |
| ≥30 minute | 321 | 55 | 0.68 (0.37, 1.23) | ||
|
| |||||
| Hospitalized date | ≤3 | 94 | 12 | 1 | 1 |
| ≥4 | 287 | 57 | 3.9 (2.2, 6.9) | 2.96 (1.40, 6.26) | |
|
| |||||
| Staff | Physician | 75 | 10 | 1 | 1 |
| Nonphysician | 325 | 63 | 1.4 (0.7, 2.9) | 1.24 (0.55, 2.78) | |
3.2. Discussion
This study reveals that the rate of CS, the rate of bad CS birth outcome, major indications for CS, the effect of surgical task shifting, and factors determine CS birth outcome. Incompleteness of maternal data registration imposes gap in the study, but strong association between factors and CS strengthens our findings.
The rate of CS delivery (24.5%) obtained in this study is greater than the normal range set by WHO, which is between 5 and 15% and rates reported nationally and abroad [10, 12, 20–23]. Similar to different findings, high emergency conditions (92%) are the major reasons for CS delivery [13, 15, 22]. This shows that surgical task shifting is playing a great role in Ethiopia to reduce maternal and fetal mortality because the commonest emergency conditions, such as CPD, fetal distress, malpresentation, and antipartum hemorrhage, similar to findings from different countries [12, 13, 15, 17, 18], can lead to fetal or maternal mortality if they are not managed through surgical interventions. However, in order to reduce risk of surgery, the increasing rate of CS delivery needs deep investigation.
In Ethiopia and other countries where both surgeons and NPSs are active, NPSs are performing majority (82%) of CS procedures, [17, 19, 24–26]. This means NPSs contribute in saving the lives of mothers and fetuses during emergency conditions. Moreover, they make CS service more accessible to people in need. However, out of 73 (15%) bad CS birth outcomes, 63 (13%) of them were due to NPSs. But there is no statistically significant birth outcome difference between those performed by physicians and NPSs (AOR 1.24 (95% CI: 0.55, 2.78)). This is also similar to the finding from another part of Ethiopia [12]. But there are factors affecting CS birth outcome of children, such as using general anesthesia four times likely leads to bad newborn outcome than using spinal anesthesia (AOR 4.19, 95% CI: 2.26, 7.77); this is similar with findings from Tigray, Ethiopia [12], being hospitalized for four or more days is at risk to develop bad CS birth outcome (AOR 2.96, 95% CI: 1.40, 6.26), and moreover,fetus under the distress condition during admission was more at risk for bad CS outcome than fetus under well condition during admission (AOR 3.53, 95% CI: 1.97, 6.31); this finding is similar to a study finding from Malawi [14].
4. Conclusion
NPSs are dominant hand for saving the life of children of Ethiopia. Using spinal anesthesia and short-time hospitalization will improve CS birth outcomes.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Authors' Contributions
YT designed the study, supervised data collection, analyzed the data, and drafted the manuscript. TG participated in the design of the study and supervised data collection. MM reviewed the manuscript. HT supervised data collection and critically reviewed the manuscript. All authors read and approved the final manuscript.
References
- 1.Mullan F., Frehywot S. Non-physician clinicians in 47 sub-Saharan African countries. The Lancet. 2007;370(9605):2158–2163. doi: 10.1016/s0140-6736(07)60785-5. [DOI] [PubMed] [Google Scholar]
- 2.Berhan Y. Medical doctors profile in Ethiopia: production, attrition and retention. In memory of 100-years Ethiopian modern medicine and the new Ethiopian millennium. Ethiopian Medical Journal. 2008;46(1):1–77. [PubMed] [Google Scholar]
- 3.Mullan F. The metrics of the physician brain drain. New England Journal of Medicine. 2005;353(17):1810–1818. doi: 10.1056/nejmsa050004. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization. Working Together for Health: the World Health Report 2006. Geneva, Switzerland: World Health Organization; 2006. [Google Scholar]
- 5.Bergström S. Who will do the caesareans when there is no doctor? Finding creative solutions to the human resource crisis. BJOG: An International Journal of Obstetrics and Gynaecology. 2005;112(9):1168–1169. doi: 10.1111/j.1471-0528.2005.00719.x. [DOI] [PubMed] [Google Scholar]
- 6.Federal Democratic Republic of Ethiopia. Health Sector Development Program IV 2010/11–2014/15. New Delhi, India: Ministry of Health; 2010. [Google Scholar]
- 7.Hogan M. C., Foreman K. J., Naghavi M., et al. Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium development Goal 5. The Lancet. 2010;375(9726):1609–1623. doi: 10.1016/s0140-6736(10)60518-1. [DOI] [PubMed] [Google Scholar]
- 8.Yaya Y., Lindtjorn B. High maternal mortality in rural south-west Ethiopia: estimate by using the sisterhood method. BMC Pregnancy and Childbirth. 2012;12(1):p. 136. doi: 10.1186/1471-2393-12-136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Newborns: Reducing Mortality, 2016, http://www.who.int/entity/mediacentre/factsheets/fs333/en/
- 10.World Health Organization. Monitoring Emergency Obstetric Care: A Handbook. Geneva, Switzerland: World Health Organization; 2009. [Google Scholar]
- 11.World Health Organization. Children: reducing mortality. 2016. http://www.who.int/mediacentre/factsheets/fs178/en/
- 12.Gessessew A., Barnabas G. A., Prata N., Weidert K. Task shifting and sharing in Tigray, Ethiopia, to achieve comprehensive emergency obstetric care. International Journal of Gynecology and Obstetrics. 2011;113(1):28–31. doi: 10.1016/j.ijgo.2010.10.023. [DOI] [PubMed] [Google Scholar]
- 13.Kim Y. M., Tappis H., Zainullah P., et al. Quality of caesarean delivery services and documentation in first-line referral facilities in Afghanistan: a chart review. BMC Pregnancy and Childbirth. 2012;12(1):p. 14. doi: 10.1186/1471-2393-12-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fenton P. M. W., Christopher J. M., Reynolds F. Caesarean section in Malawi: prospective study of early maternal and perinatal mortality. BMJ. 2003;327(7415):p. 587. doi: 10.1136/bmj.327.7415.587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fesseha N., Getachew A., Hiluf M., Gebrehiwot Y., Bailey P. A national review of cesarean delivery in Ethiopia. International Journal of Gynecology and Obstetrics. 2011;115(1):106–111. doi: 10.1016/j.ijgo.2011.07.011. [DOI] [PubMed] [Google Scholar]
- 16.Berhan Y., Ahmed A. Emergency obstetric performance with emphasis on operative delivery outcomes does it reflect on the quality of care? Ethiopian Journal of Health Development. 2004;18(2):p. 10. doi: 10.4314/ejhd.v18i2.9944. [DOI] [Google Scholar]
- 17.Chilopora G., Caetano P., Kamwendo F., Chimbiri A., Malunga E., Bergström S. Postoperative outcome of caesarean sections and other major emergency obstetric surgery by clinical officers and medical officers in Malawi. Human Resources for Health. 2007;15(17) doi: 10.1186/1478-4491-5-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kolawole A. O. D., Onwuhuafua P., Adesiyun G., Oguntayo A., Mohammed-Duro A. Audit of primary caesarean sections in nulliparae seen in ABUTH kaduna. Australian Journal of Basic and Applied Sciences. 2011;5(6):1088–1097. [Google Scholar]
- 19.Pereira C., Mbaruku G., Nzabuhakwa C., Bergstrom S., McCord C. Emergency obstetric surgery by non-physician clinicians in Tanzania. International Journal of Gynecology and Obstetrics. 2011;114(2):180–183. doi: 10.1016/j.ijgo.2011.05.004. [DOI] [PubMed] [Google Scholar]
- 20.Girma M., Yaya Y., Gebrehanna E., Berhane Y., Lindtjorn B. Lifesaving emergency obstetric services are inadequate in south-west Ethiopia: a formidable challenge to reducing maternal mortality in Ethiopia. BMC Health Services Research. 2013;13(1):p. 459. doi: 10.1186/1472-6963-13-459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ali Y. Analysis of caesarean delivery in Jimma Hospital, south-western Ethiopia. East African Medical Journal. 1995;72(1):p. 4. [PubMed] [Google Scholar]
- 22.Najam R., Sharma R. Maternal and fetal outcomes in elective and emergency caesarean sections at a teaching hospital in North India. A retrospective study. Journal of Advance Researches in Biological Sciences. 2013;5(1):5–9. [Google Scholar]
- 23.Central Statistical Agency (CSA) and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2016. [Google Scholar]
- 24.Kathryn C., Rosseel P., Gielis P., Ford N. Surgical task shifting in sub-Saharan Africa. PLoS Medicine. 2009;6(5) doi: 10.1371/journal.pmed.1000078.e1000078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McCord C., Mbaruku G., Pereira C., Nzabuhakwa C., Bergstrom S. The quality of emergency obstetrical surgery by assistant medical officers in Tanzanian district hospitals. Health Affairs. 2009;28(5):w876–w885. doi: 10.1377/hlthaff.28.5.w876. [DOI] [PubMed] [Google Scholar]
- 26.Pereira C., Cumbi A., Malalane R., et al. Meeting the need for emergency obstetric care in Mozambique: work performance and histories of medical doctors and assistant medical officers trained for surgery. BJOG: An International Journal of Obstetrics and Gynaecology. 2007;114(12):1530–1533. doi: 10.1111/j.1471-0528.2007.01489.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.