

Abstract
The purpose of this scoping review was to survey the most recent (10 years) estimating of needed human resource in health-care organization by Workload Indicators of Staffing Need (WISN) method literature to understand themes and research avenues that may be helpful and beneficial to estimating of needed staff in health-care organizations. Our search strategy was based on using search engines such as Medline, Google Scholar, Scopus, and PubMed as well publications such as Elsevier, Emerald, ProQuest, and Springer. Finally, 31 articles extract for scoping review. Scoping review findings emerge in four key points that mentioned as follow: Service delivery time, Geographical features, Workload, and Supply and Demand. Furthermore, the strengths and weakness of WISN extracted from literature. As conclusion, the WISN method is applicable to any health-care organization, and of course, in smaller institutions, it can be done more quickly and efficiently. Where shortages of staff were identified using WISN, and if increasing the number of employees was impossible, we could use the task shifting. WISN can be used to calculate the required human resources for future models based on some assumptions such as the results of staff training, demographic changes, and disease profiles and staff turnover.
Keywords: Health staff, health-care centers, hospitals, workload indicator of staffing need, workload estimation
Introduction
Nowadays, most developed and even developing countries are facing increasing need for trained health-care facilities such as hospitals, emergency departments, and other health services centers. Providing diverse and complicated health services will require more human resources.[1] Human resources play a main role in providing optimal health services to the community, and in fact, are critical factors affecting the effectiveness and efficiency of health systems.[2] But in recent years, increasing demand for high-quality health services has led to an increased pressure on human resources planners to allocate the optimal number of health workers in different businesses and different geographic areas, and simultaneously, promote the desirable population coverage.[3] Human resource allocation in wrong numbers or wrong proportions or inappropriate geographic areas can lead to a bad effect on the quality of service provision, an increased dissatisfaction among customers, and even staff. Ultimately, it can be an obstacle to the achievement of the organization's main goals.[4] Hence, it seemed that the essential need of health organizations is to estimate the optimal number of employees to ensure effective and efficient use of limited resources.[5]
On the other hand, workforce, as the most important resource in provision of health care, account for the largest part in the health sector's expenditures, therefore, in most developed countries, the issue of human resource planning (HRP) has been paid lots of attention. The core of HRP is to estimate and predict the number and types of human resources needed to achieve the organization's goals. Neglect of HRP leads to many problems, such as shortage or surplus of workforce, unequal distribution of workforce, severe shortage of staff in rural or deprive region, inappropriate applying staff, nonproductive employees, and so on in the organization.[6,7] Therefore, an objective estimation of staff is the most efficient, effective, and acceptable step on human resource management that will facilitate the achievement of fair and desirable health-care goals. However, for years, it has become possible to achieve a rational approach to allocate appropriate levels of human resources to health centers.[8] In recent decades, developing countries have used demographic ratios to estimation of their staff needed, which often result in excessive workforce in some place and a reduction in other place. In the late 1990s, the World Health Organization (WHO) provided the Workload Indicator of Staffing Need (WISN) methodology for estimating the needed staff. This method is based on a human resource management tool regarding the actual work done by the staff. Using the workload indicator to determine the required human resources will lead to the establishment of a new evidence-based workforce norm.[6] Some concerns and critics on this methodology have been aroused during application of WISN; so, this methodology needs to be reviewed broadly after more than four decades.
At scoping review the main goal is to achieve a deep insight of subject by literature review not the critique of previous studies and ranking them in the range of the best and worst conducted studies. Therefore, reviewing the studies were.
Hence, the aim of this study is to scoping review of the recent 10-year studies on the WISN as a tool or model for estimating human resources needed to provide desirable services using the proposed method by WHO's based on actual workload in health-care organizations and in different countries in order to identify the strengths and weaknesses of the methodology and propose the solution for limitations.
Background
WISN is based on the actual workload performed by the staff and the standard (time) activity for each component of the work. This principle has long been used in business. In the health sector, however, it was not applying until the late 1990s, when the WISN method was used in a number of countries. The manual of WISN is a revision of version that was prepared by Peter Shipp and published by the WHO in 1998. This method is an easy to use operational tool for estimating and forecasting the human resources required in HRP.[9]
What is the Workload Indicator of Staffing Need?
The WISN approach is a human resource management tool for:
Assessing the workload of staff.
Determining the number of staffing need based on the actual workload.[10]
The Main Features of Workload Indicator of Staffing Need Method
Easy to use; using the information that has been collected and available in the past year
Applicable for decision-making on the supply and distribution of workforce
Acceptable for health-care managers in terms of technical principles
A realistic approach that its outcome use to budgeting and resource allocation.[11]
The WISN calculation is based on the type of services and the complexity of care delivery in different centers. Two types of results differences and ratiosare provided by the WISN method.[12] The difference between the actual number of staff with calculated number which indicates the level of deficiency or excessive staff is the result of the using WISN. The actual staff ratio, compared with the required staff, represents the pressure on personnel.[13]
The strength of the WISN method is the calculation basis on actual work that has made it a completely objective tool for determining the desirable level of human resources. On the other hand, applying WISN lead to efficient use of resources and improve the quality of services.[14,15]
Methods
In the recent years, many studies have been done on the WISN as a methodology, model, or tool for estimating staff needed. Due to a large number of articles in this issue, the search strategy was limited to the period of 10 years from 2007 to 2017 [inclusion and exclusion criteria mentioned in Table 1]. All articles that their method was WISN were chosen to including to the study. Keywords consist of workload, WISN, health-care staff, health centers, and hospitals [search strategy mentioned in Table 2].
Table 1.
Inclusion and exclusion criteria
| Criterion | Inclusion | Exclusion |
|---|---|---|
| Time period | January 2007 and February 2017 | Any study outside these dates |
| Language | English and Persian | Non-English |
| Kind of organization | Hospitals and health centers and health-care organization | No reference to l health-care organization |
| Tool | WISN | Any study without this method |
| Population and sample | All kind of health-care organization (clinical and nonclinical) | Personnel that working in other organization |
WISN=Workload indicator of staffing need
Table 2.
Search terms and strategies
| SPIDER tool 1 | Search term |
|---|---|
| S | Hospital or clinic or hospice or (health and organization or center) |
| PI | Estimate or assess or calculate or survey and (work or volume and work) and Man or work or labor and (power or force) or employee or personnel or staff and WISN OR workload indicator of staffing need |
| D/E/R | “Qualitative” OR “quantitative” OR “mixed method” OR “case study” OR “cohort study” OR “quality assurance” |
WISN=Workload indicator of staffing need
The databases that were used for search included Medline, Google Scholar, Scopus, and PubMed as well publications such as Elsevier, Emerald, ProQuest, and Springer. The search result was the extraction of 367 articles that after omitting the repeated and nonEnglish articles, 99 eligible articles (regarding to including criteria) were chosen. Our scoping review, focus on health-care workers, workload, and estimate of staffing need, so articles that were not eligible exclude from the study. Furthermore, because of concentrate on the main aim of the study, some study that their objectives were about high workload hazards and its correlation with increasing human error, staff, and patient's dissatisfaction were excluded. Studies that applying WISN but not in health-care organizations were excluded. After screening removal of duplicates, and addition of snowball studies, 31 empirical articles were selected for inclusion and concepts analyses. [Summarizing the selection process drawn up Figure 1].
Figure 1.
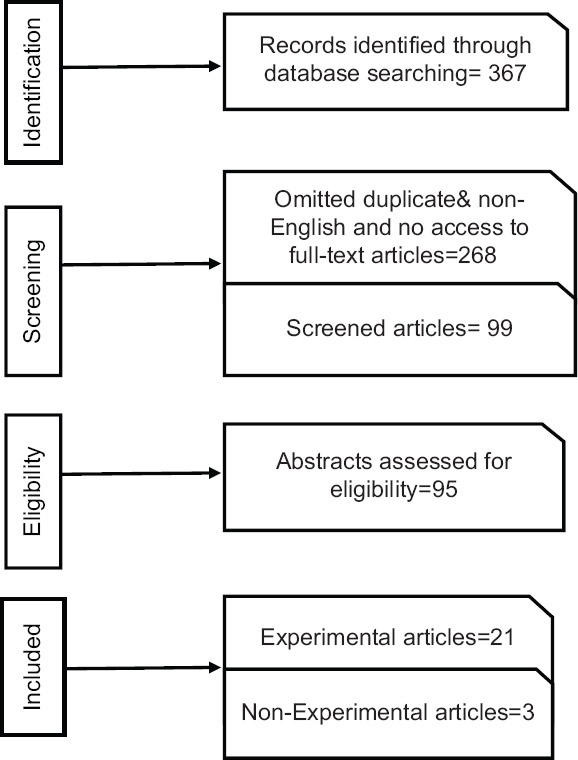
Preferred reporting items for systematic reviews and meta-analyses flow diagram
After ultimate review, chosen articles assessed by matrix method that is an approach for organizing, critical, and analyzing articles. A scoping review aim is achieving the broad vision to one issue not for put critical comment on the best articles. Hence, researchers review the articles away from criticism.
Description of Studies
Ultimately, 31 articles that their aim were estimating of needed workforce by WISN in health organization chosen for content analyze.
Table 3 is a summary of extracted articles base on country, population, year, and their aim. 12 studies was done in Africa (Tanzania, Namibia, Burkina Faso, and Uganda), 4 studies in India, 4 in Indonesia, 3 in Iran, and 1 in Turkey, Pakistan, Bangladesh, Bengal, Finland, and Brazil. 3 of 31 was qualitative study and others were carried out by cross-sectional method. Out of 31 studies that ultimately remain for the analysis of data, 10 of them in hospitals and on different clinical or nonclinical staff was done. The studies target population were nurses,[16,17,18,19,20,21,22,23] physicians and pharmacists,[24] laboratory staff,[25] anesthesiologists,[15,26] and hospital cooks.[27]
Table 3.
List of final sources and detail
| Row | Authors/country/year | Aim/population/research place |
|---|---|---|
| 1 | Burmen et al./Southern Kenya/2017 | Estimates of the optimal number of physicians for providing care and counseling services for AIDS in the referral hospital and training center by WISN |
| 2 | Ernawati et al./India/2017 | To analyze the real needs of nurses on staff workload indicators need (WISN) |
| 3 | Jocom et al./Indonesia/2017 | To identify the number of needed cooks in the hospital using WISN |
| 4 | Kumar et al./India/2016 | Calculating the workload of anesthesiologists and nurses in emergency operations in hospitals based on WISN |
| 5 | Kayani et al./Pakistan/2016 | Estimating the work pressure of lady health worker in health center using WISN |
| 6 | Bonfim et al./Brazil/2016 | Confirmation of the use of WISN in predicting nurse staff requirements in family health centers |
| 7 | Nayebi et al./Iran/2016 | To estimate the required number of nursing staff for an emergency department of a general training hospital |
| 8 | Liljano et al./Finland/2016 | Determining optimal number of nursing resources in relation to function |
| 9 | Mollahaliloğlu et al./Turkey/2015 | Determine the need for a family physician in health center in Turkey using WISN |
| 10 | Napirah and Sulistiani Indonesia/2015 | The estimation of optimal number of needing laboratory staff in the laboratory at Hospital based on WISN |
| 11 | Mugisha/Uganda/2015 | Use WISN to determine the need for clinical staff at hospital, Uganda |
| 12 | Di puskesmas skd/Indonesia/2015 | Estimating needed number of physicians in public health centers by WISN |
| 13 | Namaganda/Uganda/2015 | Estimating needed number of five cadres (nursing assistants, nurses, midwives, clinical officers, doctors at public health facilities by WISN) |
| 14 | Govule/Uganda/2015 | Estimating needed number of six cadres, namely, medical officers medical clinical officers, nurses, midwives, laboratory staff, and nursing assistants at hospital by WISN |
| 15 | Dharmayuda A/South Africa/2015 | Estimating the needed number of Physicians at health center by WISN |
| 16 | Ly et al./Burkino Faso/2014 | Measuring the capacity of maternal health-care services of reference hospitals to cope with the demand for health services by WISN |
| 17 | Shivam et al./East Bengal/2014 | Planning for needed nurse for rural Bengal hospitals, using WISN |
| 18 | Abdideh et al./Iran/2014 | Formulation of the ratio of the family physician in health-care center to the population based on WISN |
| 19 | McQuide et al./Namibia/2013 | To develop new evidence-based norms of physicians and nurses and pharmacist aid para clinics in hospital by WISN |
| 20 | Das et al./India/2013 | Estimation of needed nurses in maternal ward of hospital |
| 21 | Naznin et al./Nepal, India, Bangladesh/2013 | To determine the needed physicians at the primary health-care center for recognition Leishmanial |
| 22 | Doulati et al./Iran/2013 | Workforce approximation in health houses in Iran‘s villages |
| 23 | Mbwele, et al./Kilimanjaro, Tanzania/2012 | Assessing the quality of neonatal care at the hospital based on number of physicians and nurses by WISN |
| 24 | Hagopian et al./India/2011 | Use WISN to calculate the need for health staff to provide mothers and children care services in health center |
| 25 | Daviaud and Chopra/South of Africa/2008 | To determine health workers needs in health-care centers using WISN |
| 26 | Nyamtema et al./Tanzania/2008 | Estimating needed maternal healthcare worker for maternity hospital |
| 27 | Mugisha and Namaganda/North of Uganda/2008 | Using WISN to determine the needed nurses in a hospital |
| 28 | Musau et al./Kenya/2008 | Estimating needed number of all cadres of workers in the tertiary hospital |
| Qualitative study | ||
| 29 | Endsley et al./2017/qualtive study | Improvement on human resource planning capacity of a hospital in Karangasem through workload indicators of staffing need software application training |
| 30 | Nopiyani et al./2017/qualtive study | A scoping review of acute care, community health, and mental health nursing workload literature |
| 31 | Tabatabaee/2017/qualtive study | What features should be included for success in nurse staffing norm in Iran hospitals? |
WISN=Workload Indicators of Staffing Need
Thirteen study in primary health-care centers on target groups such as maternal health-care providers,[28] female family health-care worker,[29] general and family practitioners,[30,31,24] family health-care worker in rural areas,[32] mother and child care workers,[33,34] nurses of health-care centers,[35] doctors for caring AIDS, and leishmanial.[24,36,37] Three studies were nonempirical and done by systematic or scoping review.[38,39,40] In all 23 experimental studies, researchers estimate staffing need for one occupational field except six below-mentioned studies.[11,15,25,41,42,43]
Result
Scoping review findings emerge in four key points that should be considered when applying WISN:
Service delivery time Usually, referrals in the evening and night shifts are gradually reduced and the workload is less than the shift in the morning. Therefore, the number of employees required in the afternoon and night shifts compared with the shift in the morning is less[16,25]
Geographical features: In some countries, there is a large difference between urban and rural areas in terms of demand for work. Employees usually have a strong willingness to serve in cities because the motivation of employees to serve in rural areas and outback centers with very limited facilities are very low.[35] Furthermore, the workload in rural area may be affected by the topography, the climate, and population density in the area[42]
Workload: Typically, auxiliary and nonspecialist employees tend to participate in less challenging and complex works. Therefore, in challenging and complicated tasks, shortages of staff lead to high workload and consequently lower quality[21,27,43]
-
Supply and demand: Shortage of supply and demand, poor services, poor communication, and inappropriate location of centers are important factors that limit the amount of services delivery[24,42]
In addition to the above-mentioned points, the strengths and weaknesses of the WISN, as well as suggestions for solving the problems, were also extracted and summarized briefly below.
Strengths of Workload Indicator of Staffing Need
-
Saving costs, simplicity, and comprehensiveness of approach: Since the calculation in the WISN method is done using available data, so it is a simple method for estimating the staffing need. WISN results can be used to policy-making for allocating workforce.[16] Using WISN, researchers can measure the workload that employees experience throughout the day. For example, it is not far from mind that workload is different in the first and second visits or when do by professional nurse or novice one but WISN, by combining these statistics and taking into account all aspects, gives a combined number of required staff. WISN is a dynamic and useful tool for delivering workload to regional, provincial, and national managers and policy-makers that can be used to improve the equity of distribution of health workers within or among similar types of health centers[11,29]
- Practical and realistic method: WISN is based on actual workload, for this reason is much more objective and more favorable than other approaches.[23,27] The benefits of this method are the use of real workload, which its realistic results can be used to allocate human resources and budgeting optimally. It is also applicable to all levels of health-care services for specific types of employees and even for a specific type of services[11,32]
- Forecasting the staffing need: The results of the WISN can be used to review existing human resources, improve the equality of staff distribution between regions and centers, ensure that staff with needed skills and knowledge are available at each level, and estimate the needed staff for newly established places. On the other hand, WISN findings can be used to compare employees in similar health-care organizations in one area or to compare staff from different cadres among different types of organization or areas. In fact, the real benefit of WISN is an opportunity that gives policy-makers to anticipate impact of their decision on human resources before implementing them. The WISN makes it possible to measure and balancing supply and demand of workforce in each organization[21,30]
- Helping to hold training courses for managers and decision-makers about estimation of staff based on real workload: WISN is applicable to all kind of staff. Literature review shows that the result of applying customized WISN can used to improve the distribution of staff among different regions, providing the essential information for training plans, and allocation of staff among different regions.[25]
Prioritization: WISN is a useful method for evaluating priorities, to address the workload of employees, or to maximize the power of decision-makers to HR allocation. WISN's simplicity turned it to an attractive and understandable way to judge about HRP. Another benefit of WISN, possibility of use in any health-care organization and understandable for all level of managers, even those with little-specialized information[37]
Participation of managers: The WISN cannot be right tool unless support strongly by managers.[20] On the other hand, WISN cannot be used lonely for decision about distribution of staff. For example, in areas such as African countries, where geographical conditions are crucial for the survival of workforce, supportive management, and informed HRP could lead to a fair distribution of human resources.[42]
Weakness of Workload Indicator of Staffing Need
Nongeneralizability: The time needed to services delivery may be affected by topography, climate, and population densities of each area. These effects may vary greatly from one region to another and will have significant effects on the calculation of needed staffing. For this reason, the results obtained from WISN cannot be generalized to other regions due to the difference in area conditions[27,31]
The impact of wrong decision-making in the results of WISN: The great difference between the needed staff in different levels of organizations, indicates that managers have a significant role in increasing equality and consequently efficiency by allocating optimal workforce at the organizations. In some organization, the lack of facilities leads to reduced workload, compulsory, so WISN calculations show less needed staff and this defective cycle repeat continually. In other words, the available statistics are lower than the level that should exist and lead to a lower estimate of human resources than the actual number required
The effect of changing health environment on WISN outcomes: Given the changing environment and its impact on health programs, such as emerge new tasks and services should be considered in the calculation of human resources and the norm obtained should be reviewed as far as possible.[34]
Discussion
A scoping review of studies on the WISN can provide useful and valuable information to those interested in this method. According to the results obtained from the review of the studies, some points that should be considered when applying the WISN method are as below:
Due to the use of the previous year's statistics in computation, the calculations may not be conforming to the facts of the current year. Therefore, it is suggested that the calculations for the current year, using possible changes in the workload, be reevaluated, or changes are considered in calculation by percentage subtract or add to the statistics.[20,32]
Held training course for familiar with WISN for new user before implementing it: Due to the newness of the WISN methodology, many employees still do not have enough familiarity with the basic principles and concepts of this method, so it may not be possible for researchers to provide the correct information due to lack of sufficient knowledge in this field, which can lead to mistakes in calculations.[16,37,43]
Taking into account the work shift, the geographical area in terms of demographic characteristics, deprived and remote areas, and specific diseases of the region, local people's customs, and other factors that leads to more or less favorable benefits of each health center's health services while using WISN.
In the case of the implementation of new human resource allocation policies, including the use of job turnover, the results obtained from the WISN calculations must be recalculated
Considering the weakness of human resource management which can have a huge impact on the shortage or surplus of workforce in some organizations[17,20,43]
In the case of the training organizations, the work that doing by the students and interns to the clients should be considered in the calculation of the staffing need[18,29]
Use combined statistics to calculate staffing need: Given the fact that the time needed for the first visit (need time to take medical history or some essential information) can be different from other visits, it is better to use the average time of services.[27]
Conclusion
Concerns about fair distribution of workforce within and between service institutions rank high in seeking how best to respond to challenges. The health workers who actually deliver health services are the most precious and least readily available resource in a health system. Managers at national and local levels struggle daily with how to manage them and simultaneously increase their effectiveness, in this way they can achieve a more just distribution of workload and productivity.
As mentioned above, the WISN is one of the most popular methods that recently apply for determination of needed staff in various organizations. Some practical tips have been extracted from the literature review, which is briefly summarized below:
The WISN method is applicable to any health-care organization, and of course, in smaller institutions, it can be done more quickly and efficiently. In large and advanced institutions could be applied to sub-elements of organization, such as a ward in tertiary hospital.[16]
WISN results can be used to HRP as well as to be applicable for estimating the needed budget for HRP[25]
Where shortages of staff were identified using WISN and if increasing the number of employees was impossible, we could use the task shifting[11,31]
WISN can be used to calculate the required human resources for future models based on some assumptions such as the results of staff training, demographic changes, and disease profiles and staff turnover. It is suggested that the WISN calculations be updated every 2 or 3 years, but by taking into account the cost-effectiveness of this revision. The components of work should be reviewed every 5 or 6 years to ensure that current operating standards are up-to-date and changes made over time, for example, if an organization uses a policy of staff turnover, or added a new task, the WISN should be recalculated.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We are immensely grateful to Dr. Vahid Rasi for his useful comments on an earlier version of the manuscript. We also thank Dr. Kamal Gholipour for his kindly assistance in summarizing the study and editing of the final text.
References
- 1.Kakuma R, Minas H, van Ginneken N, Dal Poz MR, Desiraju K, Morris JE, et al. Human resources for mental health care: Current situation and strategies for action. Lancet. 2011;378:1654–63. doi: 10.1016/S0140-6736(11)61093-3. [DOI] [PubMed] [Google Scholar]
- 2.Boxall P, Purcell J. UK: Palgrave Macmillan; 2011. Strategy and Human Resource Management., Mrtin S Press LLC. [Google Scholar]
- 3.Berman EM, Bowman JS, West JP, Van Wart MR. 4th Edition. London, United Kingdom: 2012. Human Resource Management in Public Service: Paradoxes, Processes, and Problems. [Google Scholar]
- 4.Bahadori M, Ravangard R, Raadabadi M, Mosavi SM, Gholami Fesharaki M, Mehrabian F, et al. Factors affecting Intensive Care Units nursing workload. Iran Red Crescent Med J. 2014;16:e20072. doi: 10.5812/ircmj.20072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zangane M, Omrani A, Shahabi M, Alikhani M, Gharlipour Z, Imanzad M. The nurse manpower distribution at state hospitals of Iran by Lorenz Curve and Gini index during 2001-2006. Sci J Ilam Univ Med Sci. 2013;21:174–81. [Google Scholar]
- 6.Clements A, Halton K, Graves N, Pettitt A, Morton A, Looke D, et al. Overcrowding and understaffing in modern health-care systems: Key determinants in meticillin-resistant Staphylococcus aureus transmission. Lancet Infect Dis. 2008;8:427–34. doi: 10.1016/S1473-3099(08)70151-8. [DOI] [PubMed] [Google Scholar]
- 7.Van Bogaert P, Clarke S, Willems R, Mondelaers M. Nurse practice environment, workload, burnout, job outcomes, and quality of care in psychiatric hospitals: A structural equation model approach. J Adv Nurs. 2013;69:1515–24. doi: 10.1111/jan.12010. [DOI] [PubMed] [Google Scholar]
- 8.Neuraz A, Guérin C, Payet C, Polazzi S, Aubrun F, Dailler F, et al. Patient mortality is associated with staff resources and workload in the ICU: A multicenter observational study. Crit Care Med. 2015;43:1587–94. doi: 10.1097/CCM.0000000000001015. [DOI] [PubMed] [Google Scholar]
- 9.World Health Organization. Applying the WISN Method in Practice: Case Studies from Indonesia, Mozambique and Uganda. World Health Organization. 2010 [Google Scholar]
- 10.World Health Organization. Models and Tools for Health Workforce Planning and Projections. World Health Organization. 2010 [Google Scholar]
- 11.Namaganda G, Oketcho V, Maniple E, Viadro C. Making the transition to workload-based staffing: Using the workload indicators of staffing need method in Uganda. Hum Resour Health. 2015;13:89. doi: 10.1186/s12960-015-0066-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.World Health Organization. Workload Indicators of Staffing Need. World Health Organization. 2010 [Google Scholar]
- 13.Kitanda J. Vol. 6. Department of Health Sciences of Uganda Martyrs University; 2008. Workload-Based Indicators of Staffing Need (WISN) for Health Tutors in Two Public Health Training Institutions in Uganda; pp. 16–30. [Google Scholar]
- 14.World Health Organization. Workload Indicators of Staffing Need (WISN): selected Country Implementation Experiences. World Health Organization. 2016 [Google Scholar]
- 15.Satish N. Gap analysis in staffing using workload indicators of staffing need method in a tertiary care teaching hospital. Int J Sci Res. 2015;4:376–7. [Google Scholar]
- 16.Das S, Manna N, Datta M, Sengupta D, Samsuzzaman M, Baur B, et al. A study to calculate the nursing staff requirement for the maternity ward medical of college hospital, Kolkata applying WISN method. IOSR J Dent Med Sci. 2013;8:1–7. [Google Scholar]
- 17.Mbwele B, Reddy E, Reyburn H. A rapid assessment of the quality of neonatal healthcare in Kilimanjaro region, Northeast Tanzania. BMC Pediatr. 2012;12:182. doi: 10.1186/1471-2431-12-182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mugisha JF, Namaganda G. Using the workload indicator of staffing needs (WISN) methodology to assess work pressure among the nursing staff of Lacor Hospital. Publisher: Department of Health Sciences of Uganda Martyrs University. Vol 6; Edisi 1; Hal 1-15. Health Policy and Development Journal, 2008. 6:1–15. [Google Scholar]
- 19.Ernawati NL, Nursalam N, Djuari L. The real need of nurses based on workload indicator staff need (Wisn) J Nurs. 2017;6:85–92. [Google Scholar]
- 20.Shivam S, Roy RN, Dasgupta S, Das Bhattacharyya K, Misra RN, Roy S, et al. Nursing personnel planning for rural hospitals in Burdwan district, West Bengal, India, using workload indicators of staffing needs. J Health Popul Nutr. 2014;32:658–64. [PMC free article] [PubMed] [Google Scholar]
- 21.Liljamo P, Lavander P, Kejonen P. Determining optimal nursing resources in university hospital nurse staffing. Nurs Inform. 2016;2016:3. [PubMed] [Google Scholar]
- 22.Nayebi BA, Mohebbifar R, Azimian J, Rafiei S. Estimating nursing staff requirement in an emergency department of a general training hospital: Application of Workload Indicators of Staffing Need (WISN) Int J Healthc Manage. 2017;17:1–6. [Google Scholar]
- 23.Desy A, Syawal S. Analisis Beban Kerja Dokter Umum Menggunakan Metode Workload Indicators of Staffing Need (WISN).Ilmiah Mahasiswa Kesehatan J. 2016;1:250–73. [Google Scholar]
- 24.Dharmayuda A. Workload analysis of doctors at puskesmas using workload indicators of staffing need in denpasar. Publ Health Prev Med Arch. 2015;3:20–6. [Google Scholar]
- 25.Napirah MR, Sulistiani AO. Analysis of the optimal number of staff needed using workload indicator of staffing needed (WISN) method in laboratory unit of public hospital anutapura palu. Public Health Indonesia. 2015;1:190–205. [Google Scholar]
- 26.Govule P, Mugisha JF, Katongole SP, Maniple E, Nanyingi M, Anguyo R. Application of workload indicators of staffing needs (WISN) in determining health workers’ requirements for Mityana general hospital, Uganda. Int J Public Health Res. 2015;3:254–63. [Google Scholar]
- 27.Jocom PA, Massie RG, Porotu’o JP. Kebutuhan riil tenaga pemasak di instalasi gizi dengan menggunakanmetode workload indicators of staffing need (WISN) di RSU Pancaran Kasih GMIM Manado. J Biomed. 2017;9:58–66. [Google Scholar]
- 28.Ly A, Kouanda S, Ridde V. Nursing and midwife staffing needs in maternity wards in Burkina Faso referral hospitals. Hum Resour Health. 2014;12(Suppl 1):S8. doi: 10.1186/1478-4491-12-S1-S8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kayani NS, Khalid SN, Kanwal S. A study to assess the workload of lady health workers in Khanpur UC, Pakistan by applying WHO's WISN method. Athens J Health. 2016;3:65–78. [Google Scholar]
- 30.Mollahaliloğlu S, Metin BC, Kosdak M, Üner S. Determination of family physician need with workload indicators of staffing need method in Turkey. Prevention. 2015;49:53. [Google Scholar]
- 31.Abdideh M, Jannati A, Asghari Jafarabadi M. Standard development of family physicians to the population defined by WISN. Bull Env Pharmacol Life Sci. 2014;3:89–96. [Google Scholar]
- 32.Doulati SP, Shahgoli JF, Jahanbin H, Kousha A, Tabrizi JS. The assessment of needed workload for manpower approximation in health houses in Iran's villages. Eur J Sci Res. 2013;114:139–48. [Google Scholar]
- 33.Hagopian A, Mohanty MK, Das A, House PJ. Applying WHO's ‘workforce indicators of staffing need’ (WISN) method to calculate the health worker requirements for India's maternal and child health service guarantees in Orissa state. Health Policy Plan. 2012;27:11–8. doi: 10.1093/heapol/czr007. [DOI] [PubMed] [Google Scholar]
- 34.Daviaud E, Chopra M. How much is not enough? Human resources requirements for primary health care: A case study from South Africa. Bull World Health Organ. 2008;86:46–51. doi: 10.2471/BLT.07.042283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bonfim D, Laus AM, Leal AE, Fugulin FM, Gaidzinski RR. Application of the workload indicators of staffing need method to predict nursing human resources at a family health service. Rev Lat Am Enfermagem. 2016;24:e2683. doi: 10.1590/1518-8345.1010.2683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Burmen B, Owuor N, Mitei P. An assessment of staffing needs at a hiv clinic in a Western Kenya using the WHO workload indicators of staffing need WISN, 2011. Hum Resour Health. 2017;15:9. doi: 10.1186/s12960-017-0186-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Naznin E, Kroeger A, Siddiqui NA, Sundar S, Malaviya P, Mondal D, et al. Human resource assessment for scaling up VL active case detection in Bangladesh, India and Nepal. Trop Med Int Health. 2013;18:734–42. doi: 10.1111/tmi.12124. [DOI] [PubMed] [Google Scholar]
- 38.Endsley P. School nurse workload: A scoping review of acute care, community health, and mental health nursing workload literature. J Sch Nurs. 2017;33:43–52. doi: 10.1177/1059840516681423. [DOI] [PubMed] [Google Scholar]
- 39.Nopiyani N, Suarjana I, Januraga P, Muliawan P. Improvement on human resource planning capacity of a hospital in karangasem through workload indicators of staffing need software application training. Udayana J Soc Sci Humanit. 2017:39–42. [Google Scholar]
- 40.Tabatabaee SS, Vafaee-Najar A, Amiresmaili MR, Nekoie-Moghadam M. Nurse staffing norm in Iran hospitals: What features should be included for success? Int J Prev Med. 2017;8:13. doi: 10.4103/2008-7802.201657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Willcox ML, Peersman W, Daou P, Diakité C, Bajunirwe F, Mubangizi V, et al. Human resources for primary health care in sub-Saharan Africa: Progress or stagnation? Hum Resour Health. 2015;13:76. doi: 10.1186/s12960-015-0073-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Nyamtema AS, Urassa DP, Massawe S, Massawe A, Lindmark G, Van Roosmalen J, et al. Staffing needs for quality perinatal care in Tanzania. Afr J Reprod Health. 2008;12:113–24. [PubMed] [Google Scholar]
- 43.McQuide PA, Kolehmainen-Aitken RL, Forster N. Applying the workload indicators of staffing need (WISN) method in Namibia: Challenges and implications for human resources for health policy. Hum Resour Health. 2013;11:64. doi: 10.1186/1478-4491-11-64. [DOI] [PMC free article] [PubMed] [Google Scholar]