

Abstract
Primary sclerosing cholangitis (PSC) is a rare but prominent fibroinflammatory cholangiopathy which can affect individuals of essentially any age. It carries a median survival of 15-20 years, regardless of age at diagnosis, and is a foremost risk factor for cholangiocarcinoma. Given the chronic and progressive nature of PSC, its inherent risk for biliary tract and other complications, and the paucity of effective pharmacotherapies, endoscopy plays a major role in the care of many patients with this disorder. In this review, we discuss the endoscopic management of PSC, including established and evolving approaches to the diagnosis and treatment of its benign as well as malignant sequelae. Owing to the rarity of PSC and dearth of high-quality evidence, we propose pragmatic approaches based on both currently available data and expert opinion.
Keywords: Bile duct diseases, Cholangiocarcinoma, Inflammatory bowel disease, Endoscopic retrograde cholangiopancreatography, Biopsy, Primary sclerosing cholangitis
Core tip: Primary sclerosing cholangitis is a chronic, inflammatory condition of the biliary tract associated with several biliary and extrabiliary complications requiring endoscopic evaluation, treatment, and surveillance.
INTRODUCTION
Primary sclerosing cholangitis (PSC) is a chronic, progressive cholestatic disease of unknown pathogenesis that is characterized by inflammation and stricturing of the biliary system. The incidence of PSC worldwide is heterogeneous, with studies reporting prevalence rates ranging from as low as nearly 0 to as high as 14 patients per 100000 individuals, depending on which region is studied[1,2]. The mean age at the time of diagnosis of PSC is approximately 40 years old, and 60% of patients diagnosed with PSC are male[3]. Notably, PSC is associated with inflammatory bowel disease (IBD); indeed, roughly 70% of patients diagnosed with PSC are at some point in their lives also diagnosed with IBD (before, contemporaneous with, or after the diagnosis of PSC), though this too is geoepidemiologically variable[4].
Although many patients with PSC are asymptomatic at the time of diagnosis, the long-term consequences of PSC can be severe and even lethal. The median liver transplantation-free survival for patients with PSC is approximately 15-20 years[5]. The shortened survival is in large part related to the fact that PSC is a mutagenic condition associated with several different malignancies including cholangiocarcinoma (CCA), gallbladder carcinoma, colorectal cancer, and hepatocellular carcinoma, among others. The chronic parenchymal inflammation associated with PSC over time also leads to the development of liver cirrhosis, which although a precursor for hepatocecullar carcinoma, is not required for the development of other malignancies.
Despite years of research, there remains an absence of pharmacologic therapies to safely and effectively stem the inflammatory cascade driven by PSC that results in biliary strictures and the development of malignant complications. Therefore, physicians often have to rely on endoscopy to help manage patients during the PSC disease course. This review focuses on the role of biliary as well as luminal endoscopy in the diagnosis, management, and surveillance of PSC and its complications.
DIAGNOSIS OF PSC
Approximately 50% of patients diagnosed with PSC are initially asymptomatic; therefore, clinicians must maintain an index of suspicion that their patient may have PSC if characteristic abnormalities are discovered in laboratory, imaging, cholangiographic, and histologic studies[6]. At the time of diagnosis, patients with PSC are often found to have chronically elevated serum liver tests with a cholestatic pattern of liver injury. Cholangiography will usually demonstrate diffuse intrahepatic and/or extrahepatic biliary ductal irregularities characterized by areas of alternating stricture and dilation, though a small subset of patients with PSC (approximately 10%) will have a negative cholangiogram, a phenotypic variant of PSC referred to as “small duct PSC”. Liver biopsy in patients with PSC typically shows evidence of periductal fibrosis, chronic nonsuppurative cholangitis, and ductular reaction, though classic “onion skin” features are not commonly seen on biopsy specimens. Notably, with the exception of small duct PSC and rare instances, clinicians often can rely on cholangiographic and serum laboratory data to establish a diagnosis of PSC, i.e., without obtaining a liver biopsy.
From a historical perspective, direct cholangiography by endoscopic retrograde cholangiography (ERC) was first described in the early 1970s and, for years, had a central role in a clinician’s diagnostic approach to PSC[7]. Prior to the development of ERC, PSC was rarely diagnosed due in large part to the inability to reliably image the biliary tree. ERC in PSC demonstrates a classic “beads on a string” appearance of the intrahepatic and extrahepatic ducts, representing diffuse ductal stricturing alternating with proximal ductal dilation. The use of ERC for the diagnosis of PSC shed light on the different phenotypic variants of the disease (Table 1). For example, it permitted the recognition that there are patients with PSC with solely intrahepatic strictures, solely extrahepatic strictures or, in some cases, both intrahepatic and extrahepatic strictures. The classification of the different phenotypic variants by cholangiography and liver biopsy is key as each variant demands its own nuanced diagnostic and management approach.
Table 1.
Phenotypic variants of primary sclerosing cholangitis
| Phenotype | Cholangiographic features | Liver histology features |
| Classic PSC | Multifocal intrahepatic and extrahepatic strictures and resultant upstream (i.e., proximal) ductal dilation | Typical findings of PSC (e.g., non-suppurative paucicellular cholangitis, periductal fibrosis, ductular reaction, and ductopenia) |
| Intrahepatic PSC | Multifocal intrahepatic strictures and resultant upstream (i.e., proximal) segmental ductal dilation | Typical findings of PSC |
| Extrahepatic PSC | Extrahepatic only strictures and resultant upstream (i.e., proximal) ductal dilation | Non-diagnostic or non-specific features of cholestasis, particularly in early stage disease |
| Small-duct PSC | Normal | Typical findings of PSC |
All of the above phenotypes will generally have a cholestatic serum biochemical profile, though a small minority of patients can have normal serum liver tests. PSC: Primary sclerosing cholangitis.
In the past decade, for patients with suspected PSC, there has been a shift from ERC to a non-invasive diagnostic option-magnetic resonance cholangiopancreatography (MRCP). MRCP uses heavily T2-weighted image sequences to highlight the biliary system and is useful for the diagnosis of several different biliary disorders such as choledocholithiasis, CCA, and sclerosing cholangitis (including PSC). Technologic advancements (such as ultrafast T2-weighted imaging sequences and three-dimensional reconstruction via maximum intensity progression) have amplified the role of MRCP in the diagnosis of PSC[8]. Compared to ERC, MRCP allows for better visualization of smaller, proximal branches of intrahepatic ducts and, therefore, may be a superior modality for the diagnosis of PSC phenotypes that do not primarily involve the extrahepatic and/or perihilar ducts[9]. Over the last two decades, meta-analyses and cost-effectiveness studies have demonstrated that MRCP is at least equivalent to ERC as the initial modality to provide cholangiographic evidence of PSC[10,11].
Although the role of ERC in the initial diagnostic approach to PSC is diminishing, there are scenarios where ERC may be required. For example, in instances where MRCP is negative in the diagnosis of patients with a high pre-test probability of PSC based on other clinical features, ERC is a reasonable next step. ERC is also appropriate for patients who cannot tolerate MRCP due to contraindications (such as non-MRI compatible implanted cardiac devices) or issues such as respiratory illness (with inability to breath hold) or metallic foreign bodies that can cause image artifacts or safety concerns.
ENDOSCOPY FOR EXTRABILIARY SURVEILLANCE OF PSC
Once the diagnosis of PSC is established, the role of endoscopy expands. While the majority of this review will focus on the role of biliary endoscopy in the surveillance and management of PSC and its complications, it is also important to consider the extrabiliary role of endoscopy in PSC (Figure 1). As mentioned earlier, the majority of patients with PSC are found to have underlying IBD. Therefore, it is recommended that patients undergo a colonoscopy to evaluate for possible IBD once a diagnosis of PSC has been established. Concomitant PSC in patients with IBD has been shown to be an independent risk factor for the development of colorectal cancer, therefore it is recommended that colonoscopies be performed annually as part of dysplasia surveillance in these patients[12-16].
Figure 1.

Overview of endoscopic surveillance of primary sclerosing cholangitis. AASLD: American Association for the Study of Liver Diseases; CA 19-9: Carbohydrate antigen 19-9 serum tumor marker; EGD: Esophagogastroduodenoscopy; PSC: Primary sclerosing cholangitis; PSC-IBD: Inflammatory bowel disease co-existing with primary sclerosing cholangitis.
During dysplasia surveillance for patients with IBD, it is recommended that endoscopists obtain four quadrant biopsies sequentially while withdrawing the colonoscope after cecal intubation is achieved[17]. Recently, however, researchers have raised questions about the appropriateness of this approach given concerns that the majority of the colon is left unsampled[18]. Research has since focused on the possible benefits of chromoendoscopy for dysplasia surveillance in IBD patients (Figure 2). A recent meta-analysis demonstrated that chromoendoscopy had a dysplasia detection rate of 7% compared to 5.1% in the traditional random biopsy cohort. Future studies are needed to demonstrate a benefit to chromoendoscopy and its cost-effectiveness in PSC-associated IBD and are likely to produce clinically meaningful results that would change our approach to dysplasia surveillance for these patients[19].
Figure 2.
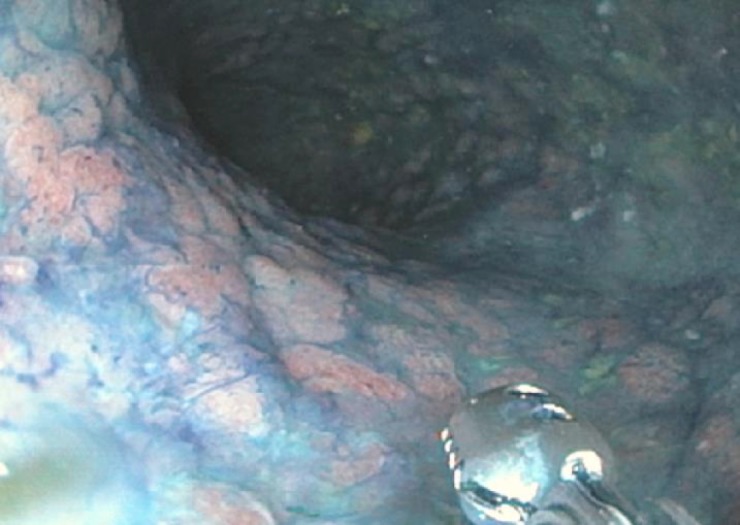
Example of the use of chromoendoscopy in a patient with primary sclerosing cholangitis. In this example, the colon was irrigated using a methylene blue solution. Targeted biopsies were obtained in a region of the sigmoid colon where decreased uptake of methylene blue revealed a diffusely flat, nodular region. Pathology revealed multifocal low-grade dysplasia requiring total proctocolectomy.
Upper gastrointestinal pathology, though not as commonly recognized, is also important to bear in mind in patients with PSC. Indeed, the hepatobiliary inflammation in PSC (akin to primary biliary cholangitis) can result in focal portal tract fibrosis resulting in portal hypertension before the development of widespread cirrhosis, thus rendering patients with PSC at risk for esophageal varices and other sequelae. In a large cohort study of 283 patients with PSC from the Mayo Clinic, 36% were found to have esophageal varices, the majority of which were moderate or large in size; of the patients found to have esophageal varices, 47% were identified as not having cirrhosis on liver biopsy[20]. Practice guidelines support performing esophagogastroduodenoscopy for variceal screening in patients with PSC who develop cirrhosis[21-23]. One area of controversy, however, is whether there is a role for variceal screening in patients with PSC without cirrhosis. At this time, guidelines limit variceal screening to only those with evidence of advanced liver fibrosis; however, clinicians should be aware of the possibility of varices in patients with PSC before the development of cirrhosis[23].
DIAGNOSIS AND MANAGEMENT OF DOMINANT STRICTURES
Due to the invasive nature and potential complications associated with ERC, it should generally be limited to instances where there is concern that patients have developed complications requiring intervention and/or tissue sampling, such as choledocholithiasis, acute cholangitis, or a dominant stricture. Development of a dominant stricture is a relatively common but also feared complication of the PSC disease course. Dominant strictures are loosely defined as extrahepatic strictures of less than or equal to 1.5 mm or intrahepatic strictures greater than or equal to 1.0 mm in diameter (Figure 3)[24]. Published reports suggest that 40%-58% of patients with PSC will develop a dominant stricture during their lifetime[24-26]. This is of particular importance as patients with PSC who develop dominant strictures have a mean survival of 14 years compared to 27 years in patients who do not develop dominant strictures[27]. Moreover, the presence of a dominant stricture is itself associated with an increased risk of developing CCA[27-29]. Clinicians should become concerned about the possibility of a dominant stricture (and the potential for underlying CCA) when a patient develops subacute worsening of right upper quadrant pain or laboratory abnormalities suggestive of worsening biliary obstruction, though in many cases, a dominant stricture is found (incidentally) during routine CCA surveillance, as discussed further below[30,31].
Figure 3.

Examples of dominant strictures (arrow) in primary sclerosing cholangitis patients as seen on magnetic resonance cholangiopancreatography (A) and on endoscopic retrograde cholangiography (B).
Once patients become symptomatic (i.e., develop pruritus, jaundice, or cholangitis) or develop laboratory abnormalities consistent with worsening cholestasis and there is evidence that a dominant stricture has developed, endoscopic intervention with ERC is warranted. Once a dominant stricture has been identified, a key step (in addition to remediating the stricture) is to distinguish whether or not it is benign or malignant (i.e., CCA). In one retrospective study of 20 patients with PSC with new dominant stricture formation, 35% of the patients were found to have underlying malignancy[32]. Therefore, it is of critical importance to consider and rule out the possibility of malignancy when such strictures are identified. For diagnostic evaluation of dominant strictures, a newer technology, single-operator cholangioscopy (SOC), is available to provide targeted sampling under visual guidance. Currently, an indication for SOC is to provide a definitive diagnosis for any patients with indeterminate strictures following biliary brushing or random biopsies. The mean sensitivity of biliary biopsies of all indeterminate strictures via SOC for diagnosing underlying malignancy is 68%, which is slightly better than random brushings and biopsies (59% and 63%, respectively)[33-40]. For patients with PSC, one would expect that the diagnostic performance of SOC is even lower, therefore, the challenge of detecting underlying malignancy is even more difficult. One of the potential limitations of SOC in patients with PSC is that SOC catheters are large in diameters (measuring 10 french) and can be difficult to insert into and through stenosed areas of the biliary system. An important benefit of SOC, at least in theory, is that in addition to directed biopsies, SOC offers direct visualization of the biliary mucosa within dominant strictures and thereby provide valuable diagnostic information. Visualization and characterization of stricture phenotypes (through advanced techniques such as narrow band imaging and probe-based methodologies) could improve how we characterize these strictures in the future; however, at present, the role of SOC in the initial evaluation of dominant strictures is still being defined through ongoing studies[41].
Another important consideration when evaluating possible malignancy in PSC is the role of endoscopic ultrasound (EUS) and fine needle aspiration/core needle biopsy (FNA/FNB). If a patient has evidence of perihilar lymphadenopathy, endoscopists should be cautious, however, with transperitoneal sampling via EUS. Transperitoneal sampling of tumors or malignant lymph nodes carries a risk of microscopic seeding of malignant cells. In a study of 191 patients with unresectable Klatskin tumors, transperitoneal sampling was associated with peritoneal metastases in 83% of patients compared to 8% in those who did not have EUS-FNA/FNB[42]. Therefore, protocols of liver transplantation for patients with CCA exclude those who have undergone percutaneous or transperitoneal biopsies of suspected malignancy due to concern for microscopic seeding[43].
In the last decade, an emerging modality for the evaluation of indeterminate strictures is confocal laser endomicroscopy (CLE). CLE provides real-time information to endoscopists regarding microscopic tissue composition of the biliary subepithelium. After a contrast agent (e.g., fluorescein) is injected and used to stain the extracellular matrix of tissues, resultant high-contrast images allow for analysis of the subepithelial architecture of the target area and potential differentiation of neoplastic from benign tissue[44]. A study published in 2011 demonstrated that CLE had an accuracy of 81% for correctly diagnosing the underlying pathology of indeterminate strictures and was superior in diagnostic performance compared to ERCP with random brushings[45]. Specifically when used for patients with PSC with dominant strictures, CLE has been shown to be more sensitive for the detection of neoplastic tissue compared to traditional brushings or biopsies[46]. Further study of CLE will be necessary to validate the technique and support its use in the algorithm for evaluating dominant strictures.
While ruling out underlying malignancy in a patient with a dominant stricture, a contemporaneous step is to consider what therapeutic intervention to perform to relieve worsened biliary obstruction posed by the dominant stricture. Some researchers hypothesize that decreasing episodes of cholangitis and limiting inflammation secondary to dominant strictures via biliary interventions may decrease the risk of CCA in patients with PSC[29,47]. When an intervention for a dominant stricture is indicated, a frequent question faced by gastroenterologists, hepatologists, and endoscopists is what specific endoscopic intervention to pursue (i.e., stricture dilation or short-term stenting or both) (Figure 4). To help address this question, a randomized controlled trial was recently performed in 9 centers across Europe. In this study, patients were randomized to one of two groups - either balloon dilation alone or short-term stent placement for a maximum of 2 wk. Patients were then followed for 24 mo. The primary outcome of the study was cumulative recurrence-free patency of dominant strictures. The study was ended early after an interim analysis demonstrated futility and that there were significantly more treatment-related adverse events in the group that received short-term stenting. Specifically, the patients who received short-term stenting had higher rates of post-ERCP pancreatitis as well as acute cholangitis compared to the patients who had balloon dilation alone. But whether more tailored use of a stent for specific scenarios or use of a fully-covered self-expanding metallic stent would have resulted in more favorable outcomes with stenting is unknown. Further data are required to provide recommendations regarding whether patients should undergo balloon dilation without short-term stenting for first-line management of dominant strictures, potentially saving stenting for only those cases wherein balloon dilation alone does not result in improved biliary drainage[48].
Figure 4.

Examples of endoscopic management of a dominant stricture in a primary sclerosing cholangitis patient using balloon dilation (A) and short-term stenting (B).
ROLE OF ENDOSCOPY IN SURVEILLANCE FOR CCA
The development of CCA is ostensibly the most severe complication for patients with PSC. The cumulative 30-year risk of developing CCA in PSC is approximately 20%[5]. Treatment options for CCA are limited, as is reflected by the 5-year survival rate for patients following this diagnosis of less than 10%[49].
A multimodal approach is necessary to provide surveillance for CCA in patients with PSC. Currently, such an approach includes using annual serum laboratory testing and abdominal imaging (e.g., via MRCP) in addition to routine follow-up and labwork. The former would entail measurement of carbohydrate antigen 19-9 (CA 19-9), the only available biomarker for CCA (Figure 5). Choosing a CA 19-9 cutoff value of ≥ 20 U/mL improves sensitivity to nearly 100% at the cost of low specificity and accuracy (38% and 47%, respectively). Conversely, choosing a CA 19-9 threshold of ≥ 129 U/mL increases specificity, but at the cost of decreased sensitivity[50,51]. It is also important to not completely rely on CA 19-9, as 7% of the general population have a negative Lewis Antigen and, therefore, does not produce CA 19-9[52].
Figure 5.

Proposed surveillance algorithm for cholangiocarcinoma in patients with primary sclerosing cholangitis. CCA: Cholangiocarcinoma; US: Ultrasound; MRCP: Magnetic resonance cholangiopancreatography; CA 19-9: Carbohydrate antigen 19-9; ERC: Endoscopic retrograde cholaniography; FISH: Fluorescence in situ hybridization.
If the combination of imaging and serum biomarkers is suggestive of findings concerning for CCA, the role of endoscopy and, particularly, ERC is to provide additional diagnostic information to help make a formal (tissue) diagnosis. This can be done by obtaining biliary brushings for cytology (which can include fluorescence in situ hybridization), acquiring targeted biopsies via fluoroscopy and/or cholangiosopy, or by providing a visual assessment of the stricture using cholangioscopy[53-56].
In addition to surveillance for CCA, societal guidelines also recommend that patients receive screening for gallbladder cancer. In patients with PSC, the estimated (lifetime) incidence of gallbladder cancer ranges from 3%-14%. Thus, in addition to the screening recommendations above, patients should undergo abdominal ultrasound annually to assess for gallbladder polyps and other potentially (pre-)cancerous changes[57].
COMPLICATIONS OF ENDOSCOPY IN PATIENTS WITH PSC
As has been alluded to throughout this article, although endoscopy has a very important role in the management and surveillance of patients with PSC, gastroenterologists will try to limit endoscopic interventions (especially ERC) in patients with PSC due to concerns of causing complications. In 2009, a Mayo Clinic study compared the rate of complications of over 1000 patients with and without PSC undergoing ERC. This retrospective review demonstrated no significant difference in the overall rate of complications in patients with PSC and those without PSC; there was, however, a significantly higher rate of subsequent acute cholangitis in patients with PSC compared to those without PSC (4% vs 0.2%, respectively). A seemingly contributing factor to the development of cholangitis in patients with PSC was the length of the ERC procedure, as patients with PSC who developed cholangitis had an average procedure length of almost 90 min compared to 50 min in those who did not develop cholangitis[58].
Different therapeutic maneuvers during ERC have varying rates of complications. For example, in one prospective study of over 500 balloon dilations of dominant strictures in 96 patients, significant adverse events such as pancreatitis (2.2%), acute cholangitis (1.4%), and bile duct perforation (0.2%) occurred rarely[47]. As mentioned previously, however, a recent randomized controlled trial suggests that short-term stenting of dominant strictures appears to carry a higher risk profile compared to balloon dilation. Short term stenting was associated with a higher rate of acute cholangitis (12%) and post-ERC pancreatitis (24%). The overall rate of complications in patients randomized to a short-term stenting protocol compared to balloon dilation was also much higher (45.4% vs 6.7%)[48].
The hypothesis behind the increased rate of post-ERC pancreatitis with stenting in patients with PSC is that compared to patients without PSC, the papilla in PSC is often small and retracted. Therefore, in addition to potentially more difficult cannulation, placement of a stent across such a small papilla may have a much higher chance of blocking off the pancreatic duct, thereby leading to pancreatitis. This hypothesis is supported by the fact that studies suggest that a prior sphincterotomy is protective against the development of post-ERC pancreatitis in patients with PSC[59,60]. Similarly, stenting carries an increased risk of blocking off the cystic duct or intrahepatic ducts, which can lead to cholecystitis or acute cholangitis, respectively. This is of particular concern in patients with PSC compared to those without PSC because of the several strictures laden throughout the biliary tree that already result in impaired biliary drainage[61].
SYNOPSIS AND FUTURE DIRECTIONS
In this review article, we have discussed how the role of endoscopy has shifted over the past 4 decades and also highlighted important questions that still are yet to be addressed.
Originally, ERC was the premier diagnostic modality available for PSC and was central to our recognition of PSC and developing an understanding of the various PSC phenotypes. As non-invasive methods of imaging of biliary anatomy emerged, the role of endoscopy has changed, but endoscopy still remains a pillar of PSC management. We now rely on ERC for the diagnosis of PSC when a patient cannot undergo MRCP, for the surveillance of extrabiliary manifestations of, and for the management and surveillance of biliary complications of PSC.
New research continues to provide gastroenterologists guidance with how to best use endoscopic techniques to manage patients with PSC. Specifically, and for example, just within the last year a randomized controlled trial has provided us with important new data regarding how we manage dominant strictures in PSC.
Clinical questions that remain to be answered and that could change the role of endoscopy in the future management of PSC are several: (1) Is there a benefit to chromoendoscopy compared to high-definition white light colonoscopy for dysplasia surveillance in patients with PSC-IBD? (2) Do patients with PSC without cirrhosis require variceal screening? (3) What is the role of cholangioscopy in CCA surveillance? (4) In light of the increased risk of complications, when should endoscopists perform short-term stenting of dominant strictures instead of or in addition to balloon dilation? (5) Would fully-covered self-expanding metallic stents fare better in PSC, though at what (monetary) cost? And (6) What is the role of CLE and other novel techniques in the diagnostic approach to dominant strictures?
We anticipate and encourage that these questions and others be addressed collaboratively in the coming years as we continue to improve how we use endoscopy to best manage and care for patients with PSC.
Footnotes
Conflict-of-interest statement: The authors have no financial disclosures or conflicts of interest.
Manuscript source: Invited manuscript
Peer-review started: December 7, 2018
First decision: December 17, 2018
Article in press: January 30, 2019
Specialty type: Gastroenterology and hepatology
Country of origin: United States
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): B, B
Grade C (Good): C, C
Grade D (Fair): 0
Grade E (Poor): 0
P- Reviewer: Ding SZ, Gkekas I, Kalaitzakis E, Maleki I S- Editor: Ji FF L- Editor: A E- Editor: Tan WW
Contributor Information
Neil Bharat Marya, Vatche and Tamar Manoukian Division of Digestive Diseases, UCLA Gastroenterology Fellowship Training Program, Los Angeles, CA 90095, United States.
James H Tabibian, Division of Gastroenterology, Department of Medicine, Olive View-UCLA Medical Center, Sylmar, CA 91342, United States. jtabibian@dhs.lacounty.gov.
References
- 1.Hurlburt KJ, McMahon BJ, Deubner H, Hsu-Trawinski B, Williams JL, Kowdley KV. Prevalence of autoimmune liver disease in Alaska Natives. Am J Gastroenterol. 2002;97:2402–2407. doi: 10.1111/j.1572-0241.2002.06019.x. [DOI] [PubMed] [Google Scholar]
- 2.Bambha K, Kim WR, Talwalkar J, Torgerson H, Benson JT, Therneau TM, Loftus EV, Jr, Yawn BP, Dickson ER, Melton LJ., 3rd Incidence, clinical spectrum, and outcomes of primary sclerosing cholangitis in a United States community. Gastroenterology. 2003;125:1364–1369. doi: 10.1016/j.gastro.2003.07.011. [DOI] [PubMed] [Google Scholar]
- 3.Toy E, Balasubramanian S, Selmi C, Li CS, Bowlus CL. The prevalence, incidence and natural history of primary sclerosing cholangitis in an ethnically diverse population. BMC Gastroenterol. 2011;11:83. doi: 10.1186/1471-230X-11-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Palmela C, Peerani F, Castaneda D, Torres J, Itzkowitz SH. Inflammatory Bowel Disease and Primary Sclerosing Cholangitis: A Review of the Phenotype and Associated Specific Features. Gut Liver. 2018;12:17–29. doi: 10.5009/gnl16510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Takakura WR, Tabibian JH, Bowlus CL. The evolution of natural history of primary sclerosing cholangitis. Curr Opin Gastroenterol. 2017;33:71–77. doi: 10.1097/MOG.0000000000000333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gossard AA, Gores GJ. Primary Sclerosing Cholangitis: What the Gastroenterologist and Hepatologist Needs to Know. Clin Liver Dis. 2017;21:725–737. doi: 10.1016/j.cld.2017.06.004. [DOI] [PubMed] [Google Scholar]
- 7.Cotton PB. Cannulation of the papilla of Vater by endoscopy and retrograde cholangiopancreatography (ERCP) Gut. 1972;13:1014–1025. doi: 10.1136/gut.13.12.1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Halefoglu AM. Magnetic resonance cholangiopancreatography: a useful tool in the evaluation of pancreatic and biliary disorders. World J Gastroenterol. 2007;13:2529–2534. doi: 10.3748/wjg.v13.i18.2529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Eaton JE, Talwalkar JA, Lazaridis KN, Gores GJ, Lindor KD. Pathogenesis of primary sclerosing cholangitis and advances in diagnosis and management. Gastroenterology. 2013;145:521–536. doi: 10.1053/j.gastro.2013.06.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dave M, Elmunzer BJ, Dwamena BA, Higgins PD. Primary sclerosing cholangitis: meta-analysis of diagnostic performance of MR cholangiopancreatography. Radiology. 2010;256:387–396. doi: 10.1148/radiol.10091953. [DOI] [PubMed] [Google Scholar]
- 11.Meagher S, Yusoff I, Kennedy W, Martel M, Adam V, Barkun A. The roles of magnetic resonance and endoscopic retrograde cholangiopancreatography (MRCP and ERCP) in the diagnosis of patients with suspected sclerosing cholangitis: a cost-effectiveness analysis. Endoscopy. 2007;39:222–228. doi: 10.1055/s-2007-966253. [DOI] [PubMed] [Google Scholar]
- 12.Claessen MM, Vleggaar FP, Tytgat KM, Siersema PD, van Buuren HR. High lifetime risk of cancer in primary sclerosing cholangitis. J Hepatol. 2009;50:158–164. doi: 10.1016/j.jhep.2008.08.013. [DOI] [PubMed] [Google Scholar]
- 13.Fevery J, Henckaerts L, Van Oirbeek R, Vermeire S, Rutgeerts P, Nevens F, Van Steenbergen W. Malignancies and mortality in 200 patients with primary sclerosering cholangitis: a long-term single-centre study. Liver Int. 2012;32:214–222. doi: 10.1111/j.1478-3231.2011.02575.x. [DOI] [PubMed] [Google Scholar]
- 14.Terg R, Sambuelli A, Coronel E, Mazzuco J, Cartier M, Negreira S, Muñoz A, Gil A, Miguez C, Huernos S, Romero G, Goncalvez S, Levi D, Abecasis R. Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis and the risk of developing malignancies. A large prospective study. Acta Gastroenterol Latinoam. 2008;38:26–33. [PubMed] [Google Scholar]
- 15.Lindström L, Lapidus A, Ost A, Bergquist A. Increased risk of colorectal cancer and dysplasia in patients with Crohn's colitis and primary sclerosing cholangitis. Dis Colon Rectum. 2011;54:1392–1397. doi: 10.1097/DCR.0b013e31822bbcc1. [DOI] [PubMed] [Google Scholar]
- 16.Wang R, Leong RW. Primary sclerosing cholangitis as an independent risk factor for colorectal cancer in the context of inflammatory bowel disease: a review of the literature. World J Gastroenterol. 2014;20:8783–8789. doi: 10.3748/wjg.v20.i27.8783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Farraye FA, Odze RD, Eaden J, Itzkowitz SH. AGA technical review on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology. 2010;138:746–774, 774.e1-4; quiz e12-13. doi: 10.1053/j.gastro.2009.12.035. [DOI] [PubMed] [Google Scholar]
- 18.Naymagon S, Ullman TA. Chromoendoscopy and Dysplasia Surveillance in Inflammatory Bowel Disease: Past, Present, and Future. Gastroenterol Hepatol (NY) 2015;11:304–311. [PMC free article] [PubMed] [Google Scholar]
- 19.Azizi S, Al-Rubaye H, Turki MAA, Siddiqui MRS, Shanmuganandan AP, Ehsanullah B, Brar R, Abulafi AM. Detecting dysplasia using white light endoscopy or chromoendoscopy in ulcerative colitis patients without primary sclerosing cholangitis: A systematic review and meta-analysis. Int J Surg. 2018;52:180–188. doi: 10.1016/j.ijsu.2018.02.028. [DOI] [PubMed] [Google Scholar]
- 20.Zein CO, Lindor KD, Angulo P. Prevalence and predictors of esophageal varices in patients with primary sclerosing cholangitis. Hepatology. 2004;39:204–210. doi: 10.1002/hep.20029. [DOI] [PubMed] [Google Scholar]
- 21.Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W Practice Guidelines Committee of the American Association for the Study of Liver Diseases; Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46:922–938. doi: 10.1002/hep.21907. [DOI] [PubMed] [Google Scholar]
- 22.Sainte-Marie G. The lymph node revisited: development, morphology, functioning, and role in triggering primary immune responses. Anat Rec (Hoboken) 2010;293:320–337. doi: 10.1002/ar.21051. [DOI] [PubMed] [Google Scholar]
- 23.Lindor KD, Kowdley KV, Harrison ME American College of Gastroenterology. ACG Clinical Guideline: Primary Sclerosing Cholangitis. Am J Gastroenterol. 2015;110:646–659; quiz 660. doi: 10.1038/ajg.2015.112. [DOI] [PubMed] [Google Scholar]
- 24.Björnsson E, Lindqvist-Ottosson J, Asztely M, Olsson R. Dominant strictures in patients with primary sclerosing cholangitis. Am J Gastroenterol. 2004;99:502–508. doi: 10.1111/j.1572-0241.2004.04106.x. [DOI] [PubMed] [Google Scholar]
- 25.Stiehl A, Rudolph G, Klöters-Plachky P, Sauer P, Walker S. Development of dominant bile duct stenoses in patients with primary sclerosing cholangitis treated with ursodeoxycholic acid: outcome after endoscopic treatment. J Hepatol. 2002;36:151–156. doi: 10.1016/s0168-8278(01)00251-3. [DOI] [PubMed] [Google Scholar]
- 26.Hilscher MB, Tabibian JH, Carey EJ, Gostout CJ, Lindor KD. Dominant strictures in primary sclerosing cholangitis: A multicenter survey of clinical definitions and practices. Hepatol Commun. 2018;2:836–844. doi: 10.1002/hep4.1194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chapman MH, Webster GJ, Bannoo S, Johnson GJ, Wittmann J, Pereira SP. Cholangiocarcinoma and dominant strictures in patients with primary sclerosing cholangitis: a 25-year single-centre experience. Eur J Gastroenterol Hepatol. 2012;24:1051–1058. doi: 10.1097/MEG.0b013e3283554bbf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Janse M, Lamberts LE, Verdonk RC, Weersma RK. IBD is associated with an increase in carcinoma in PSC irrespective of the presence of dominant bile duct stenosis. J Hepatol. 2012;57:473–474; author reply 475. doi: 10.1016/j.jhep.2012.02.034. [DOI] [PubMed] [Google Scholar]
- 29.Rudolph G, Gotthardt D, Klöters-Plachky P, Kulaksiz H, Rost D, Stiehl A. Influence of dominant bile duct stenoses and biliary infections on outcome in primary sclerosing cholangitis. J Hepatol. 2009;51:149–155. doi: 10.1016/j.jhep.2009.01.023. [DOI] [PubMed] [Google Scholar]
- 30.Ali AH, Tabibian JH, Nasser-Ghodsi N, Lennon RJ, DeLeon T, Borad MJ, Hilscher M, Silveira MG, Carey EJ, Lindor KD. Surveillance for hepatobiliary cancers in patients with primary sclerosing cholangitis. Hepatology. 2018;67:2338–2351. doi: 10.1002/hep.29730. [DOI] [PubMed] [Google Scholar]
- 31.Tabibian JH, Ali AH, Lindor KD. Primary Sclerosing Cholangitis, Part 2: Cancer Risk, Prevention, and Surveillance. Gastroenterol Hepatol (NY) 2018;14:427–432. [PMC free article] [PubMed] [Google Scholar]
- 32.Lindberg B, Arnelo U, Bergquist A, Thörne A, Hjerpe A, Granqvist S, Hansson LO, Tribukait B, Persson B, Broomé U. Diagnosis of biliary strictures in conjunction with endoscopic retrograde cholangiopancreaticography, with special reference to patients with primary sclerosing cholangitis. Endoscopy. 2002;34:909–916. doi: 10.1055/s-2002-35298. [DOI] [PubMed] [Google Scholar]
- 33.Chen YK, Parsi MA, Binmoeller KF, Hawes RH, Pleskow DK, Slivka A, Haluszka O, Petersen BT, Sherman S, Devière J, Meisner S, Stevens PD, Costamagna G, Ponchon T, Peetermans JA, Neuhaus H. Single-operator cholangioscopy in patients requiring evaluation of bile duct disease or therapy of biliary stones (with videos) Gastrointest Endosc. 2011;74:805–814. doi: 10.1016/j.gie.2011.04.016. [DOI] [PubMed] [Google Scholar]
- 34.Chen YK, Pleskow DK. SpyGlass single-operator peroral cholangiopancreatoscopy system for the diagnosis and therapy of bile-duct disorders: a clinical feasibility study (with video) Gastrointest Endosc. 2007;65:832–841. doi: 10.1016/j.gie.2007.01.025. [DOI] [PubMed] [Google Scholar]
- 35.Draganov PV, Chauhan S, Wagh MS, Gupte AR, Lin T, Hou W, Forsmark CE. Diagnostic accuracy of conventional and cholangioscopy-guided sampling of indeterminate biliary lesions at the time of ERCP: a prospective, long-term follow-up study. Gastrointest Endosc. 2012;75:347–353. doi: 10.1016/j.gie.2011.09.020. [DOI] [PubMed] [Google Scholar]
- 36.Dumonceau JM. Sampling at ERCP for cyto- and histopathologicical examination. Gastrointest Endosc Clin N Am. 2012;22:461–477. doi: 10.1016/j.giec.2012.05.006. [DOI] [PubMed] [Google Scholar]
- 37.Hartman DJ, Slivka A, Giusto DA, Krasinskas AM. Tissue yield and diagnostic efficacy of fluoroscopic and cholangioscopic techniques to assess indeterminate biliary strictures. Clin Gastroenterol Hepatol. 2012;10:1042–1046. doi: 10.1016/j.cgh.2012.05.025. [DOI] [PubMed] [Google Scholar]
- 38.Kalaitzakis E, Webster GJ, Oppong KW, Kallis Y, Vlavianos P, Huggett M, Dawwas MF, Lekharaju V, Hatfield A, Westaby D, Sturgess R. Diagnostic and therapeutic utility of single-operator peroral cholangioscopy for indeterminate biliary lesions and bile duct stones. Eur J Gastroenterol Hepatol. 2012;24:656–664. doi: 10.1097/MEG.0b013e3283526fa1. [DOI] [PubMed] [Google Scholar]
- 39.Manta R, Frazzoni M, Conigliaro R, Maccio L, Melotti G, Dabizzi E, Bertani H, Manno M, Castellani D, Villanacci V, Bassotti G. SpyGlass single-operator peroral cholangioscopy in the evaluation of indeterminate biliary lesions: a single-center, prospective, cohort study. Surg Endosc. 2013;27:1569–1572. doi: 10.1007/s00464-012-2628-2. [DOI] [PubMed] [Google Scholar]
- 40.Ramchandani M, Reddy DN, Gupta R, Lakhtakia S, Tandan M, Darisetty S, Sekaran A, Rao GV. Role of single-operator peroral cholangioscopy in the diagnosis of indeterminate biliary lesions: a single-center, prospective study. Gastrointest Endosc. 2011;74:511–519. doi: 10.1016/j.gie.2011.04.034. [DOI] [PubMed] [Google Scholar]
- 41.Azeem N, Gostout CJ, Knipschield M, Baron TH. Cholangioscopy with narrow-band imaging in patients with primary sclerosing cholangitis undergoing ERCP. Gastrointest Endosc. 2014;79:773–779.e2. doi: 10.1016/j.gie.2013.09.017. [DOI] [PubMed] [Google Scholar]
- 42.Heimbach JK, Sanchez W, Rosen CB, Gores GJ. Trans-peritoneal fine needle aspiration biopsy of hilar cholangiocarcinoma is associated with disease dissemination. HPB (Oxford) 2011;13:356–360. doi: 10.1111/j.1477-2574.2011.00298.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gleeson FC, Lee JH, Dewitt JM. Tumor Seeding Associated With Selected Gastrointestinal Endoscopic Interventions. Clin Gastroenterol Hepatol. 2018;16:1385–1388. doi: 10.1016/j.cgh.2018.05.014. [DOI] [PubMed] [Google Scholar]
- 44.Wani S, Shah RJ. Probe-based confocal laser endomicroscopy for the diagnosis of indeterminate biliary strictures. Curr Opin Gastroenterol. 2013;29:319–323. doi: 10.1097/MOG.0b013e32835fee9f. [DOI] [PubMed] [Google Scholar]
- 45.Meining A, Chen YK, Pleskow D, Stevens P, Shah RJ, Chuttani R, Michalek J, Slivka A. Direct visualization of indeterminate pancreaticobiliary strictures with probe-based confocal laser endomicroscopy: a multicenter experience. Gastrointest Endosc. 2011;74:961–968. doi: 10.1016/j.gie.2011.05.009. [DOI] [PubMed] [Google Scholar]
- 46.Heif M, Yen RD, Shah RJ. ERCP with probe-based confocal laser endomicroscopy for the evaluation of dominant biliary stenoses in primary sclerosing cholangitis patients. Dig Dis Sci. 2013;58:2068–2074. doi: 10.1007/s10620-013-2608-y. [DOI] [PubMed] [Google Scholar]
- 47.Gotthardt DN, Rudolph G, Klöters-Plachky P, Kulaksiz H, Stiehl A. Endoscopic dilation of dominant stenoses in primary sclerosing cholangitis: outcome after long-term treatment. Gastrointest Endosc. 2010;71:527–534. doi: 10.1016/j.gie.2009.10.041. [DOI] [PubMed] [Google Scholar]
- 48.Ponsioen CY, Arnelo U, Bergquist A, Rauws EA, Paulsen V, Cantú P, Parzanese I, De Vries EM, van Munster KN, Said K, Chazouillères O, Desaint B, Kemgang A, Färkkilä M, Van der Merwe S, Van Steenbergen W, Marschall HU, Stotzer PO, Thorburn D, Pereira SP, Aabakken L. No Superiority of Stents vs Balloon Dilatation for Dominant Strictures in Patients With Primary Sclerosing Cholangitis. Gastroenterology. 2018;155:752–759.e5. doi: 10.1053/j.gastro.2018.05.034. [DOI] [PubMed] [Google Scholar]
- 49.Rosen CB, Nagorney DM, Wiesner RH, Coffey RJ, Jr, LaRusso NF. Cholangiocarcinoma complicating primary sclerosing cholangitis. Ann Surg. 1991;213:21–25. doi: 10.1097/00000658-199101000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Charatcharoenwitthaya P, Enders FB, Halling KC, Lindor KD. Utility of serum tumor markers, imaging, and biliary cytology for detecting cholangiocarcinoma in primary sclerosing cholangitis. Hepatology. 2008;48:1106–1117. doi: 10.1002/hep.22441. [DOI] [PubMed] [Google Scholar]
- 51.Nehls O, Gregor M, Klump B. Serum and bile markers for cholangiocarcinoma. Semin Liver Dis. 2004;24:139–154. doi: 10.1055/s-2004-828891. [DOI] [PubMed] [Google Scholar]
- 52.Sinakos E, Saenger AK, Keach J, Kim WR, Lindor KD. Many patients with primary sclerosing cholangitis and increased serum levels of carbohydrate antigen 19-9 do not have cholangiocarcinoma. Clin Gastroenterol Hepatol. 2011;9:434–439.e1. doi: 10.1016/j.cgh.2011.02.007. [DOI] [PubMed] [Google Scholar]
- 53.Nanda A, Brown JM, Berger SH, Lewis MM, Barr Fritcher EG, Gores GJ, Keilin SA, Woods KE, Cai Q, Willingham FF. Triple modality testing by endoscopic retrograde cholangiopancreatography for the diagnosis of cholangiocarcinoma. Therap Adv Gastroenterol. 2015;8:56–65. doi: 10.1177/1756283X14564674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Nishikawa T, Tsuyuguchi T, Sakai Y, Sugiyama H, Miyazaki M, Yokosuka O. Comparison of the diagnostic accuracy of peroral video-cholangioscopic visual findings and cholangioscopy-guided forceps biopsy findings for indeterminate biliary lesions: a prospective study. Gastrointest Endosc. 2013;77:219–226. doi: 10.1016/j.gie.2012.10.011. [DOI] [PubMed] [Google Scholar]
- 55.Siiki A, Rinta-Kiikka I, Koivisto T, Vasama K, Sand J, Laukkarinen J. Spyglass single-operator peroral cholangioscopy seems promising in the evaluation of primary sclerosing cholangitis-related biliary strictures. Scand J Gastroenterol. 2014;49:1385–1390. doi: 10.3109/00365521.2014.940376. [DOI] [PubMed] [Google Scholar]
- 56.Arnelo U, von Seth E, Bergquist A. Prospective evaluation of the clinical utility of single-operator peroral cholangioscopy in patients with primary sclerosing cholangitis. Endoscopy. 2015;47:696–702. doi: 10.1055/s-0034-1391845. [DOI] [PubMed] [Google Scholar]
- 57.Khaderi SA, Sussman NL. Screening for malignancy in primary sclerosing cholangitis (PSC) Curr Gastroenterol Rep. 2015;17:17. doi: 10.1007/s11894-015-0438-0. [DOI] [PubMed] [Google Scholar]
- 58.Bangarulingam SY, Gossard AA, Petersen BT, Ott BJ, Lindor KD. Complications of endoscopic retrograde cholangiopancreatography in primary sclerosing cholangitis. Am J Gastroenterol. 2009;104:855–860. doi: 10.1038/ajg.2008.161. [DOI] [PubMed] [Google Scholar]
- 59.Ismail S, Kylänpää L, Mustonen H, Halttunen J, Lindström O, Jokelainen K, Udd M, Färkkilä M. Risk factors for complications of ERCP in primary sclerosing cholangitis. Endoscopy. 2012;44:1133–1138. doi: 10.1055/s-0032-1325677. [DOI] [PubMed] [Google Scholar]
- 60.Simmons DT, Petersen BT, Gostout CJ, Levy MJ, Topazian MD, Baron TH. Risk of pancreatitis following endoscopically placed large-bore plastic biliary stents with and without biliary sphincterotomy for management of postoperative bile leaks. Surg Endosc. 2008;22:1459–1463. doi: 10.1007/s00464-007-9643-8. [DOI] [PubMed] [Google Scholar]
- 61.Navaneethan U, Jegadeesan R, Nayak S, Lourdusamy V, Sanaka MR, Vargo JJ, Parsi MA. ERCP-related adverse events in patients with primary sclerosing cholangitis. Gastrointest Endosc. 2015;81:410–419. doi: 10.1016/j.gie.2014.06.030. [DOI] [PubMed] [Google Scholar]