

Abstract
Motor neuron diseases (MNDs) are a group of devastating neurologic disorders that cause specific damage to the motor neuron cells. The current diagnosis of MND is based on results of the clinical examination and neurophysiologic studies. The length of time of referral to a neuromuscular neurologist and the lack of validated diagnostic criteria can delay diagnosis. Although the role of imaging is currently most useful in excluding other conditions, several attempts to incorporate neuroimaging in the diagnosis of the disease and assessment of progression have shown promising results.
We conducted a literature review via searches in PubMed and The Cochrane Database using multiple relevant terms to the topic. Two cases with a challenging diagnosis of MND are described, with a thorough discussion of how the diagnosis was suggested on the basis of magnetic resonance imaging evidence in each case. Advanced magnetic resonance imaging findings can be useful tools that add to the diagnostic criteria of MNDs, especially in cases where reaching a definitive diagnosis is difficult. Such findings might enable clinicians to reach an early diagnosis that can improve the patient’s quality of life and prolong survival.
Keywords: corticospinal tract hyperintensities, CST hyperintensities, MND, motor neuron disease, possible MND, possible motor neuron disease, quantitative and functional MRI, ribbon like hypointensities
INTRODUCTION
Motor neuron diseases (MNDs) are a group of progressive degenerative neurologic disorders involving both the upper motor neurons (UMN) and/or the lower motor neurons (LMN). Major forms of MND include 1) amyotrophic lateral sclerosis (ALS), which involves both UMN and LMN; 2) primary lateral sclerosis involving mostly UMN; 3) progressive muscular atrophy involving mostly LMN; 4) progressive bulbar palsy involving both bulbar UMN and LMN only; and 5) pseudobulbar palsy.1,2 The most common disorder in the group is ALS. The diagnosis of ALS and other forms of MND is usually delayed.3 Currently, conventional and quantitative magnetic resonance imaging (MRI) are not included in the diagnostic criteria for MND and are used only to exclude MND mimics.
In this article, we review the literature and present 2 illustrative cases of possible MND that were supported by conventional and advanced MRI findings.
LITERATURE REVIEW
Etiology and Pathogenesis
The etiology and pathogenesis of MNDs are not yet well understood, and it is unclear whether the degeneration starts from the neuron cell and descends to the axons or vice versa.4 Nonetheless, extramotor cerebral pathology with certain genetic linkage is now recognized in 5% to 10% of the cases, and the rest are sporadic cases with no identified genetic component.3,5,6
Diagnostic Challenges
Early diagnosis of MNDs can have a major positive impact on quality of life and survival given the benefit of highly specialized palliative care and pharmacologic therapy. It is now well known that early, noninvasive positive-pressure ventilation and placement of a gastrostomy tube improves the quality of life and prolongs survival in patients with ALS.7–12 However, the subtle onset, different disease presentations, and overlapping symptoms with other neurologic disorders make early diagnosis sometimes difficult to achieve.
Several studies reported that the time from onset to diagnosis of ALS ranges from 5 months to 15 months.13 Initial misdiagnoses by general practitioners and inappropriate referrals are major reasons for the late diagnoses.14 The low incidence of ALS (median incidence rate, 2.08/100,000 population) and other forms of MNDs makes general practitioners and general neurologists unfamiliar with the variety of disease presentations.15 Multiple studies have shown that MNDs are misdiagnosed by 26% to 42% of neurologists.16–18 Even if MND is suspected, it is difficult for any clinician to tell a patient with progressive weakness or disability, or both, that their diagnosis is only probable or possible. Furthermore, with the recent approval of the intravenous medication, edaravone for the early treatment of ALS in the US19 the validation of diagnostic criteria becomes more important.
Diagnostic Criteria
El Escorial criteria and the modified version20 were developed for the diagnosis of ALS. However, the sensitivity of the criteria in the diagnosis of definite ALS is very low. It is categorized according to the presence of both UMN and LMN signs in 4 body regions: Brain stem (bulbar), cervical (neck and upper extremities), thoracic (trunk and abdominal wall), and lumbosacral (lower back and lower extremities).21 A diagnosis of definitive ALS requires 3 regions of combined UMN and LMN pathology, probable ALS requires 2 regions of combined pathology, and possible ALS requires 1 region of combined pathology or 2 UMN signs in 2 regions.
In 2006, Awaji-shima (also called Awaji) criteria integrated electromyographic (EMG) data into the clinical diagnosis.22 These criteria require evidence of both acute and chronic denervation in the absence of sensory nerve conduction abnormalities and the presence of severe motor nerve conduction abnormalities. Evidence of acute denervation includes the presence of fasciculation potentials, fibrillations, and complex repetitive discharges in the weak or wasted muscle. Chronic denervation signs on EMG include increased numbers, duration, and amplitude of the motor unit potentials. A normal sensory nerve conduction study includes normal sensory nerve action potential amplitude and conduction velocities. Severe motor nerve conduction abnormalities include conduction velocity less than 75% of normal, prolonged distal compound muscle action potential latency greater than 150% of normal, and presence of more than 50% distal to proximal compound muscle action potential conduction block. Awaji-shima criteria recommended that EMG abnormalities should be considered equivalent to LMN abnormalities that increase the sensitivity for disease detection.22–24 Both El Escorial and Awaji-shima criteria are used for research purposes but are not used widely in clinical practice.
According to Traynor el al,25 56% of 388 patients given a clinical diagnosis of ALS met the definitive or probable diagnosis of ALS using the El Escorial criteria. Another 10% of the patients, who died, did not reach a level of diagnostic certainty greater than possible ALS.25 According to a meta-analysis, there was a 23% increase in the proportion of patients with a definitive or probable ALS diagnosis after using the Awaji-shima criteria that incorporated EMG findings.26 Nonetheless, there remains insensitivity in detecting the UMN pathology in MNDs, which makes their diagnosis challenging at times.27
Magnetic Resonance Imaging for Diagnosis of Motor Neuron Disease
Few studies have evaluated MRI as an additive technique that can be used for the diagnosis of MND. Findings in conventional MRI include mainly hyperintensities on the T2-weighted sequences, proton density, and fluid-attenuated inversion recovery (FLAIR) sequences along the corticospinal tract and hypointensities in the precentral gyrus, called the motor dark line, on T2-weighted images (susceptibility images).28,29 Recently, quantitative MRI techniques such as diffusion tensor imaging (DTI) have been tested and compared with conventional MRI. DTI has the potential for early detection of the micropathology of the disease before the macropathology shows up on conventional MRI.30 Although more abnormal test measures in DTI were detected in patients with ALS pathology on conventional MRI compared with patients with an ALS diagnosis without conventional MRI pathology, the studies showed variable statistical significance compared with control groups. The DTI measures did not correlate with the duration of the disease, probably because of the different disease pathologies, locations, and durations. Probably the most statistically significant DTI measures were the fractional anisotropy (FA), mean diffusivity (calculated at the motor cortex and the posterior limb of the internal capsule), and the reconstructed tractography of the cerebrospinal tract at the centrum semiovale extending to the motor cortex.31,32
Methods
We conducted an evidence-based search for relevant studies of MND using PubMed from the National Library of Medicine and The Cochrane Database of Systematic Reviews. The following search term combinations were used to find and review relevant articles in the literature: Motor neuron disease, amyotrophic lateral sclerosis, primary lateral sclerosis, progressive muscular atrophy, pseudobulbar palsy, progressive bulbar palsy, MRI, cerebral MRI, brain MRI, cervical MRI, advanced MRI, conventional MRI, diffusion tensor imaging, susceptibility weighted imaging, three-dimensional T1 imaging, T2 imaging, FLAIR, fluid attenuated inversion recovery imaging, tractography, functional MRI, Awaji criteria, El Escorial criteria, and early diagnosis. We did not apply a filter for date of publication. We reviewed all articles that discussed the role of MRI in MNDs.
This review of the literature includes 2 challenging cases for illustration. No institutional review board approval was obtained because the reported cases do not meet the criteria for human research. Both patients gave informed consent for publication without disclosure of personal information. Conventional MRI sequences included T2-weighted imaging, FLAIR imaging, and susceptibility-weighted imaging. Advanced MRI sequences were 3-dimensional T1-weighted imaging, DTI, and tractography.
CASE PRESENTATIONS
Case 1
A 63-year-old woman with a history of hypertension and adequately treated hypothyroidism presented with 6 months of progressive bilateral lower extremity weakness and difficulty swallowing. Her physical examination revealed diffuse muscle weakness in all extremities without atrophy or fasciculations. Although an upgoing plantar reflex was noted on the right side, there were no clear UMN findings otherwise (normal upper extremity reflexes and absent lower extremity reflexes).
Results of the nerve conduction study demonstrated a moderate diffuse axonal polyneuropathy. The EMG study findings revealed chronic and active motor denervation out of proportion to the polyneuropathy suggestive of MND, but some diagnostic uncertainty remained because of the presence of less than 70% motor nerve conduction velocities on the nerve conduction study and the lack of any clinical history that explained such neuropathy. Because of the presence of confusing results of nerve conduction studies alongside the abnormal EMG results, the treating neurology team raised a concern of missing a treatable diagnosis such as autoimmune neuropathy.
Conventional MRI with T2-weighted susceptibility images showed a hypointense rim in the right precentral gyrus (Figure 1). The DTI results showed decreased FA in the left Brodmann area 4 (motor) and in the body of corpus callosum bilaterally with bilateral motor cortical thinning on T1-weighted 3-dimensional reconstruction (Figures 2 and 3; Table 1). When combined with EMG, the DTI findings confirmed LMN lesions. A diagnosis of MND (ie, ALS) became more likely because of the presence of both UMN and LMN lesions. A diagnosis of polyneuropathy was then extremely unlikely or irrelevant.
Figure 1.
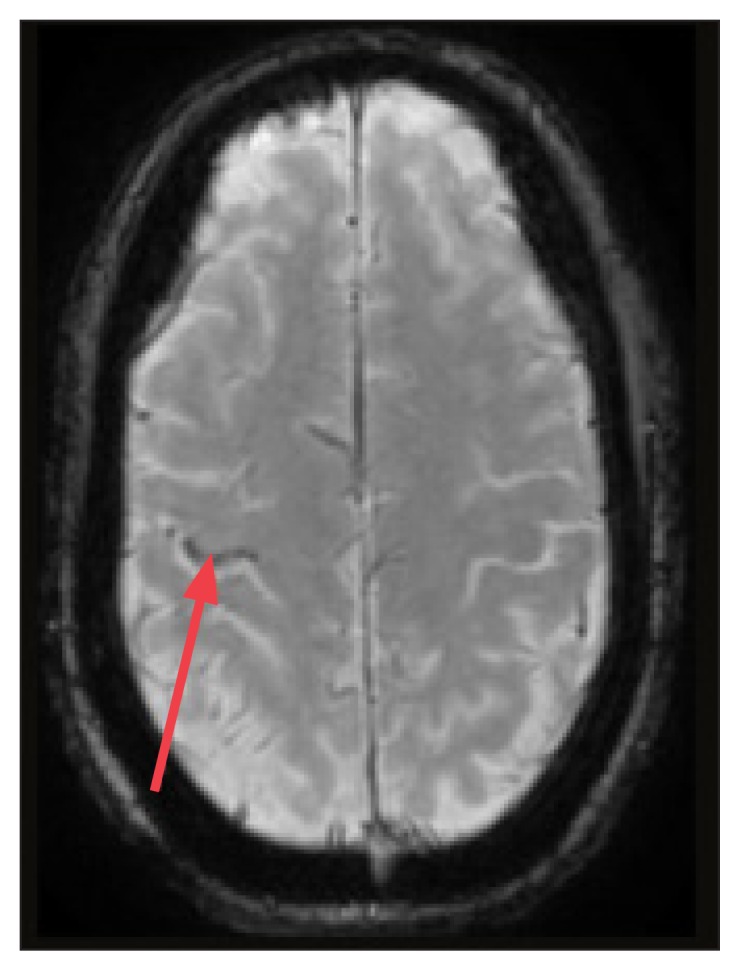
Conventional magnetic resonance T2-weighted susceptibility image from Case 1 showing right-sided, ribbon-like hypointensities in the precentral cortex (red arrow).
Figure 2.
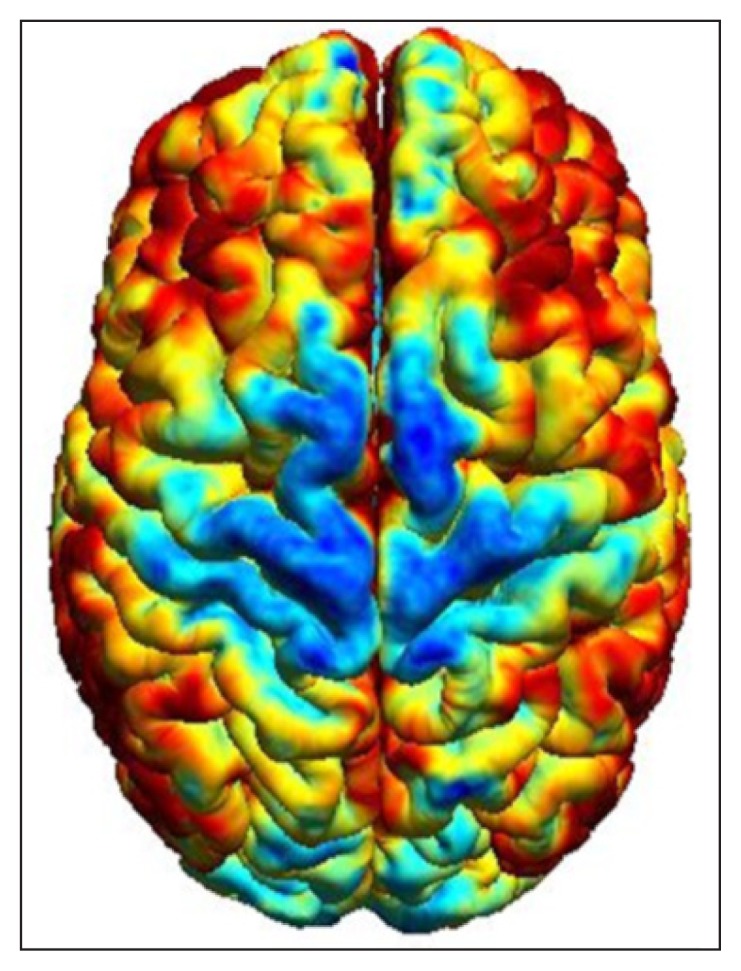
Three-dimensional T1-weighted reconstructed magnetic resonance image from Case 1 showing cortical thinning in the primary motor cortex (blue areas).
Figure 3.
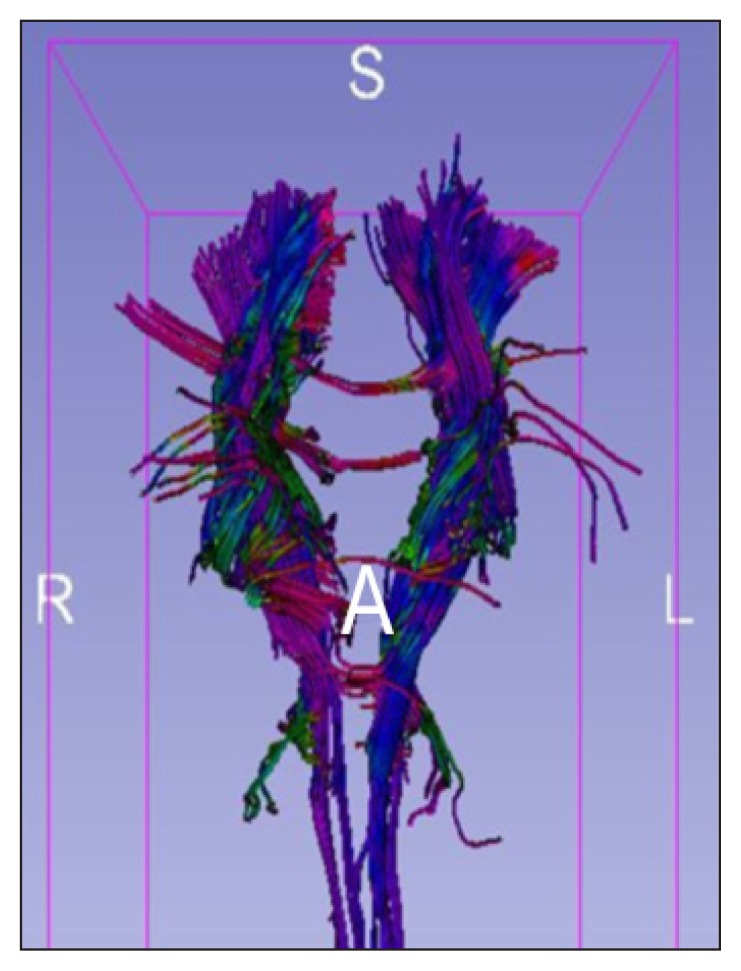
Tractography of the corticospinal tract from Case 1 showing decreased fiber thickness on the right side of the brainstem from the cortex to the cervical spine.
A = anterior; L = left; R = right; S = superior.
Table 1.
Comparative fractional anisotropy across different sites of corticospinal tract from cortex to medullaa
| Site | Patient 1 | Patient 2 | Reference value32,33 | Standard deviation | ||
|---|---|---|---|---|---|---|
| Right | Left | Right | Left | |||
| BA 4 (motor) | 0.54 | 0.27b | 0.39 | 0.48 | 0.39 | 0.02 |
| BA 3, 2, 1 (sensory) | 0.49 | 0.51 | 0.44 | 0.39 | 0.38 | 0.03 |
| Posterior limb of internal capsule | 0.65 | 0.64 | 0.62c | 0.69 | 0.68 | 0.04 |
| Midbrain | 0.72 | 0.70 | 0.62 | 0.60c | 0.64 | 0.03 |
| Pons | 0.76 | 0.65 | 0.55c | 0.47b | 0.59 | 0.03 |
| Medulla | 0.69 | 0.77 | 0.29b | 0.35 | 0.47 | 0.08 |
| Thalamus | 0.27 | 0.35 | 0.25c | 0.28 | 0.29 | 0.03 |
| Splenium of corpus callosum | 0.80 | — | 0.79 | — | 0.78 | 0.03 |
| Body of corpus callosum | 0.47b | 0.30b | 0.72 | 0.83 | 0.70 | 0.05 |
In Patient 1, there is a decrease of the FA in the left motor cortex and the body of the corpus callosum bilaterally. In Patient 2, there is a significant decrease of the FA in the brain stem bilaterally
Boldface values indicate significant decreases in fractional anisotropy (FA).
Italic values indicate mild decreases in FA.
BA = Broadmann area.
Case 2
A 52-year-old woman presented with recurrence of bilateral lower extremity weakness 6 months after thoracic spine evacuation of syringomeningocele that had caused lower extremity myelopathy but had resolved postoperatively. She also complained of hoarseness of voice, slurred speech, difficulty swallowing, intermittent ptosis and diplopia, urinary retention, and fecal incontinence. Her physical examination revealed she had UMN findings, such as a brisk jaw jerk, hyperreflexia, and bilateral arm spasticity not explained by the conventional MRI results.
The EMG findings did not reveal new or evolving LMN changes. The possibility of primary lateral sclerosis superimposed on her other medical conditions was raised clinically but was difficult to tease out given the confounding variables of the case. She had no evidence of other autonomic findings or orthostatic hypotension. Test results for other causes, such as myasthenia gravis, were normal.
Conventional MRI did not show any abnormality (Figure 4), but T1-weighted 3-dimensional reconstruction images displayed bilateral motor cortical thinning (Figure 5). Tractography showed asymmetric truncation of motor fibers with low FA along the corticospinal tract (Figure 6; Table 1). These findings were located in the motor cortex and extended down the corticospinal tract, indicating a selective UMN lesion. Advanced MRI results helped confirm the clinical finding of UMN pathology in 3 different anatomical regions. This abnormality was confined to the motor cortex and the corticospinal tract as illustrated in Figures 5 and 6. Absence of any lesion on the repeat conventional MRI made the correlation of her new symptoms to the old pathology (syringomeningocele) extremely unlikely. On the basis of the advanced MRI findings, the diagnosis of primary lateral sclerosis became more likely.
Figure 4.
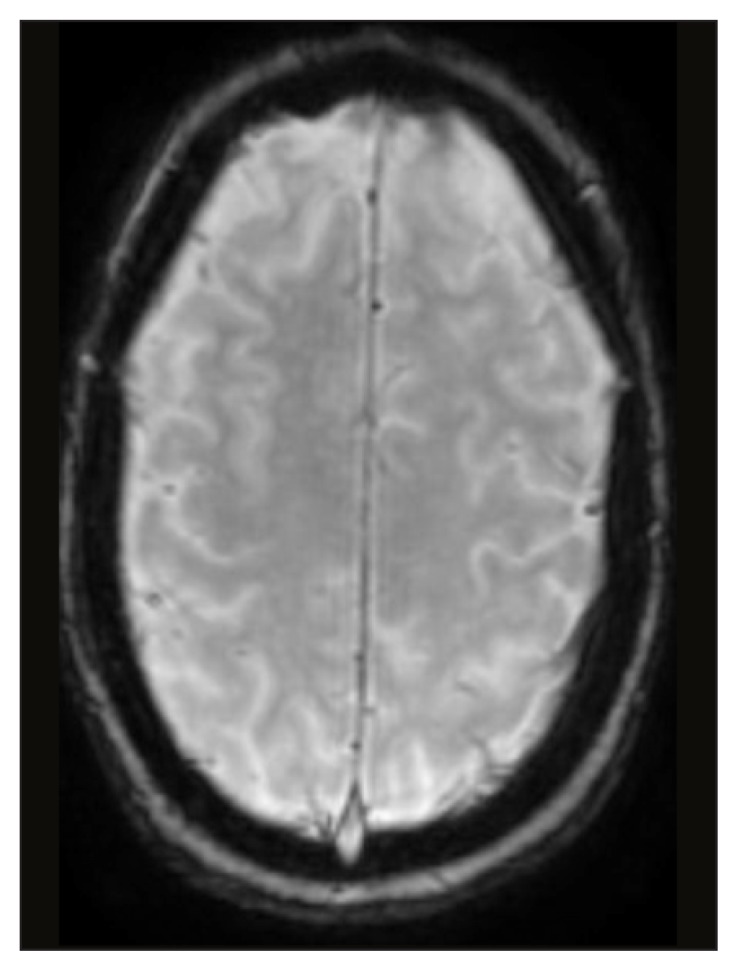
Normal conventional magnetic resonance T2-weighted susceptibility image from Case 2.
Figure 5.
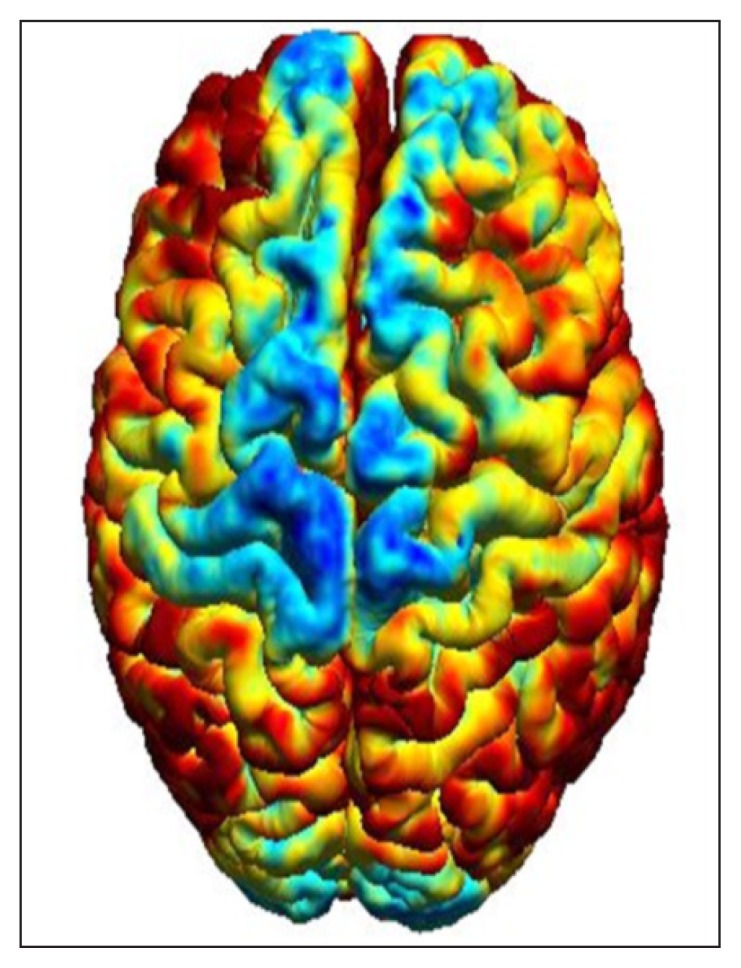
Three-dimensional T1-weighted reconstructed magnetic resonance image from Case 2 showing cortical thinning in the primary motor cortex (blue areas).
Figure 6.
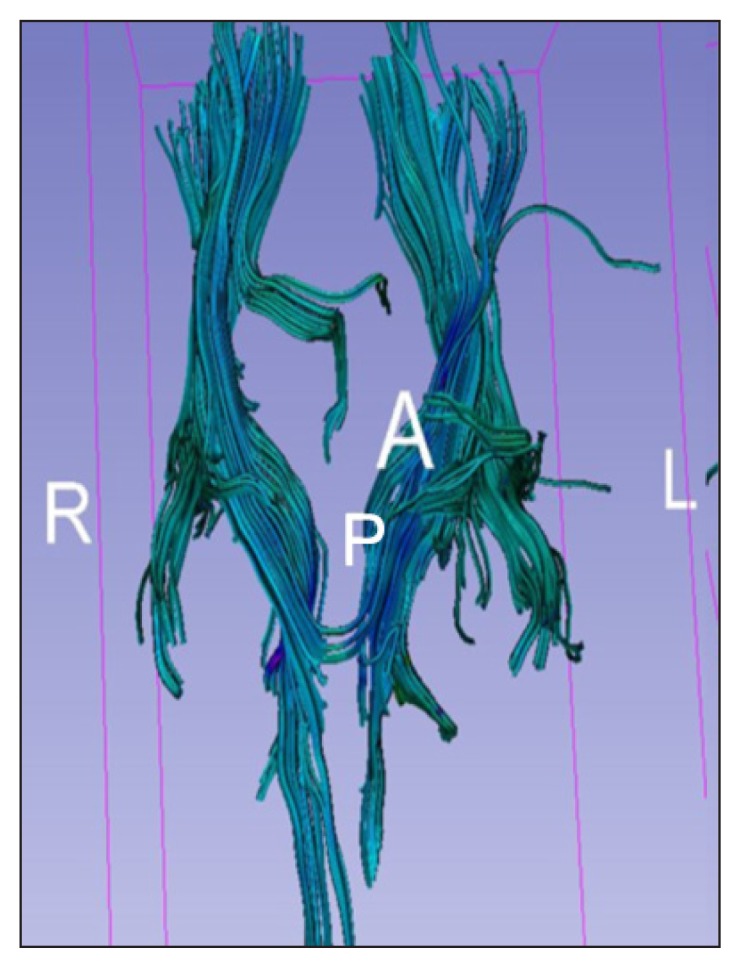
Tractography of the corticospinal tract from Case 2 showing truncated motor fibers on the left side of the brainstem and corpus callosum and decreased density in the left subcortical fibers.
A = anterior; L = left; P = posterior; R = right.
DISCUSSION
The results of the conventional and advanced MRI imaging in our 2 patients were variable but overall were consistent with dispersed UMN pathology not explained by other diseases. In Case 1, because of the presence of confusing results of nerve conduction studies (< 70% motor nerve conduction velocities) with the abnormal EMG results, the treating neurology team considered the possibility of missing a treatable diagnosis such as autoimmune neuropathy. Eventually, the MRI results confirmed degeneration along the fibers of the corticospinal tract and the motor cortex, thus increasing the possibility of an ALS diagnosis.
In Case 2, because this was a challenging case, the neurology team suggested using other advanced modalities to try to narrow the differential diagnosis. Although the patient’s symptoms were anatomically overlapping, a chronologic understanding of her symptoms was crucial. Initially, the patient had lower extremity myelopathic manifestations with EMG degenerative changes. This condition resolved after surgery. The patient came back describing new progressive myelopathic manifestations involving the lumbar, cervical, and bulbar regions without LMN signs that started 6 months after resolution of her initial symptoms. A subsequent spine MRI revealed no new lesions. A repeat EMG showed resolution of the denervation signs. Findings on advanced MRI sequences suggested that a diagnosis of primary lateral sclerosis was more likely.
Although a retrograde atrophy of the corticospinal tract secondary to a thoracic syrinx was a possibility, it was rather unlikely given the long period of resolution of the lower extremity symptoms and resolution of signs of denervation on the EMG after surgery, with no evidence of new lesion on the most recent MRI. Nonetheless, it was even less probable that the developmental abnormalities that caused the thoracic syrinx initially might be causing her new symptoms because the patient was asymptomatic in the bulbar and cervical region before the development of the thoracic syrinx and because the new MRI did not show any lesion progression.
A similar diagnostic approach was followed by Matsunaga et al32 before they diagnosed ALS in a patient with new-onset myelopathic weakness in the upper extremities. In their case, it was accompanied by C4 to C7 spinal foraminal narrowing.
Primary lateral sclerosis presents early with only UMN signs; LMN signs appear several years later. For this reason, diagnosis in the early stages depends on the absence of LMN signs. The disease is slowly progressive. Such challenges make the diagnosis difficult for many clinicians, which might contribute to the reported rarity of the disease. The diagnosis of primary lateral sclerosis is thus mainly clinical so far, making it likely a diagnosis of exclusion.
Other diagnoses that need to be excluded in patients with primary lateral sclerosis are diffuse neurodegenerative diseases, including multiple system atrophy and spinocerebellar ataxia. These possibilities further stress the importance of MRI, which in our Case 2 did not show diffuse cerebral or cerebellar atrophy. Clinically, multiple system atrophy was less likely in our case because of the absence of orthostatic hypotension that indicates autonomic instability, and spinocerebellar ataxia was less likely because of the absence of ataxia.
Although MNDs involve pathologies in both the UMN and LMN with variable degrees of involvement, it is unknown which pathology occurs first. Is it an anterograde process starting as neuronopathy and spreading downstream, or is it a retrograde process starting as axonopathy and then extending upstream to the motor neuron? It is possible that both hypotheses are true and that different or combined forms of the disease occur. Also, the anatomical location where the disease begins is still unknown.31 Nevertheless, other motor areas such as the corpus callosum, especially the middle and posterior parts, are involved in the pathology and are now well recognized.33 A new hypothesis in the pathogenesis of the disease has been proposed, which suggests an imbalance between the excitatory-inhibitory signals in the interneuron on the basis of some magnetic resonance spectroscopy studies.3,34,35
DTI is a promising quantitative MRI technique for the diagnosis of MND. This technique detects the diffusion of proton particles freely within the tissues in multiple plains while intact myelin provides the maximum restriction of such diffusion, leading to a higher FA and lower mean diffusivity.36–38 Decreased FA and increased mean diffusivity in the cerebrospinal tract in primary lateral sclerosis, ALS, and progressive muscular atrophy could potentially be used as a marker for early and clinically silent UMN involvement. Inconsistent mean diffusivity values in some studies might be attributed to coexisting gliosis along with myelin/axonal degeneration that also can limit proton diffusivity. If this is true, normal mean diffusivity and decreased FA might indicate longer duration of the disease because of restrictive gliosis.39–41 Decreased FA also has been described in the corpus callosum, premotor white matter, prefrontal white matter, temporal white matter, and cervical cord. Nevertheless, a significant direct correlation between the amount of decrease in FA and disease progression has been noticed in small studies. The amount of corpus callosum involvement was independent of the degree of UMN involvement clinically in these small studies,42–44 and other studies showed truncated subcortical motor fibers on tractography.45
Changes on magnetic resonance spectroscopy such as decreased N-acetylaspartate (NAA), NAA/creatinine, NAA/choline, NAA/creatine + choline, and NAA/myoinositol along the cerebrospinal tract from the cortex to the cerebral peduncle have been described with variable sensitivity and specificity. These changes also correlated with the disease severity. The NAA/myoinositol marker is the most sensitive and specific.46,47
Three-dimensional T1-weighted reconstructed MRI images have shown cortical thinning in the primary motor cortex with or without clinical cognitive impairment. Also, temporal and parietal thinning has been described in patients with associated dementia and possible genetic linkage. Results using a surface-based rather than voxel-based technique were more statistically consistent with these findings.48,49 A small, controlled study in 2016 showed no difference in cortical thickness or DTI metrics between patients with LMN-predominant MND and healthy controls.50 Cervical spinal cord MRI showed evidence of thinning of the cord diameter compared with controls.50 Also, a decrease in the FA on DTI was noticed, especially in the distal cervical cord.50 Assessment of the cervical cord requires more sophisticated MRI machines and is technically challenging to assess in most medical centers.51
Regarding functional MRI, a few studies have shown decreased connectivity in the sensorimotor areas, but other study results showed increased connectivity. This is probably because it depends on the type of neuron affected and the timing along the disease course when the functional MRI was done. The increased connectivity might be caused by a compensatory process for the associated structural damage or because of direct loss of the inhibitory interneurons.52
It is important to note that the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of advanced MRI findings have not been studied on a large scale. Nonetheless, incorporating such findings with the current diagnostic criteria and studying its effect on shortening the time needed to reach a diagnosis of MND and on outcomes must be studied as well. Because adding the electrophysiologic results to the LMN clinical criteria for MND diagnosis has improved the sensitivity of the criteria, it is possible that neuroimaging might add to the sensitivity of detecting UMN pathology.
According to the revised criteria of the World Federation of Neurology Research Group on Motor Neuron Diseases,53 conventional MRI studies are not required in patients with clinically definite disease with bulbar or pseudobulbar onset. However, in those with probable or possible ALS, routine brain and/or spinal cord MRI can be useful in excluding several ALS mimics.53
According to the European guidelines,53 and although cerebrospinal tract hyperintensities or a T2-weighted hypointense rim in the precentral gyrus can support a preexisting suspicion of MND, the specific search of these abnormalities for the purpose of making a firm diagnosis is not recommended. We encourage the establishment of new clinical trials using the different MRI measures to gain additional insight into disease pathophysiology and into the value of these techniques in a longitudinal assessment of the diagnosis and progression of MNDs.
CONCLUSION
As illustrated in our 2 challenging cases, findings on the conventional MRI sequences (T2-weighted imaging, FLAIR imaging, and susceptibility-weighted imaging) and advanced MRI sequences (3-dimensional T1-weighted imaging, DTI, and tractography) solidified the MND diagnosis. The intent of this review is to raise the awareness of these advanced MRI findings to serve as a backup tool when a diagnosis of MND is in doubt. By having these tools available, the time to reach a definitive or more affirmative diagnosis can be shortened in doubtful cases. Although it is not the intent of this article to change the guidelines or amend the diagnostic criteria, our results point toward the need for more advanced criteria for the diagnosis of MNDs.
Applying early supportive measures and pharmacologic therapies will improve the quality of life and survival in patients with MNDs, and thus early diagnosis is preferable. Primary care practitioners and general neurologists may have limited experience with MNDs, and a delay in diagnosis may lead to worse outcomes. Recent studies and reviews have shown that a combined approach between all imaging techniques (especially DTI and functional MRI) might have stronger sensitivity and specificity. Nevertheless, we recommend the development of standardized criteria that include clinical findings, EMG findings, and MRI findings to increase the sensitivity of disease detection.
Acknowledgment
Kathleen Louden, ELS, of Louden Health Communications provided editorial assistance.
Footnotes
Disclosure Statement
The author(s) have no conflicts of interest to disclose.
References
- 1.Zarei S, Carr K, Reiley L, et al. A comprehensive review of amyotrophic lateral sclerosis. Surg Neurol Int. 2015 Nov 16;6:171. doi: 10.4103/2152-7806.169561. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Leigh PN, Ray-Chaudhuri K. Motor neuron disease. J Neurol Neurosurg Psychiatry. 1994 Aug;57(8):886–96. doi: 10.1136/jnnp.57.8.886. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brown RH, Al-Chalabi A. Amyotrophic lateral sclerosis. New Engl J Med. 2017 Jul 13;377(2):162–72. doi: 10.1056/NEJMra1603471. . [DOI] [PubMed] [Google Scholar]
- 4.Rajagopalan V, Allexandre D, Yue GH, Pioro EP. Diffusion tensor imaging evaluation of corticospinal tract hyperintensity in upper motor neuron-predominant ALS patients. J Aging Res. 2011;2011 doi: 10.4061/2011/481745. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abhinav K, Stanton B, Johnston C, et al. Amyotrophic lateral sclerosis in South-East England: A population-based study. The South-East England register for amyotrophic lateral sclerosis (SEALS Registry) Neuroepidemiology. 2007;29(1–2):44–8. doi: 10.1159/000108917. . [DOI] [PubMed] [Google Scholar]
- 6.Ticozzi N, Vance C, Leclerc AL, et al. Mutational analysis reveals the FUS homolog TAF15 as a candidate gene for familial amyotrophic lateral sclerosis. Am J Med Genet B Neuropsychiatr Genet. 2011 Apr;156B(3):285–90. doi: 10.1002/ajmg.b.31158. . [DOI] [PubMed] [Google Scholar]
- 7.Orrell RW. Motor neuron disease: Systematic reviews of treatment for ALS and SMA. Br Med Bull. 2010;93(1):145–59. doi: 10.1093/bmb/ldp049. . [DOI] [PubMed] [Google Scholar]
- 8.Miller RG, Jackson CE, Kasarskis EJ, et al. Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter update: The care of the patient with amyotrophic lateral sclerosis: Multidisciplinary care, symptom management, and cognitive/behavioral impairment (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2009 Oct 13;73(15):1227–33. doi: 10.1212/WNL.0b013e3181bc01a4. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tsai MJ, Hsu CY, Sheu CC. Amyotrophic lateral sclerosis. N Engl J Med. 2017 Oct 19;377(16):1602. doi: 10.1056/NEJMc1710379. . [DOI] [PubMed] [Google Scholar]
- 10.Traynor BJ, Alexander M, Corr B, Frost E, Hardiman O. Effect of a multidisciplinary amyotrophic lateral sclerosis (ALS) clinic on ALS survival: A population based study, 1996–2000. J Neurol Neurosurg Psychiatry. 2003 Sep;74(9):1258–61. doi: 10.1136/jnnp.74.9.1258. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Burkhardt C, Neuwirth C, Sommacal A, Andersen PM, Weber M. Is survival improved by the use of NIV and PEG in amyotrophic lateral sclerosis (ALS)? A post-mortem study of 80 ALS patients. PLoS One. 2017 May 23;12(5):e0177555. doi: 10.1371/journal.pone.0177555. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.ProGas Study Group. Gastrostomy in patients with amyotrophic lateral sclerosis (ProGas): A prospective cohort study. Lancet Neurol. 2015 Jul;14(7):702–9. doi: 10.1016/s1474-4422(15)00104-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cellura E, Spataro R, Taiello AC, La Bella V. Factors affecting the diagnostic delay in amyotrophic lateral sclerosis. Clin Neurol Neurosurg. 2012 Jul;114(6):550–4. doi: 10.1016/j.clineuro.2011.11.026. . [DOI] [PubMed] [Google Scholar]
- 14.Nzwalo H, de Abreu D, Swash M, Pinto S, de Carvalho M. Delayed diagnosis in ALS: The problem continues. J Neurol Sci. 2014 Aug 15;343(1–2):173–5. doi: 10.1016/j.jns.2014.06.003. . [DOI] [PubMed] [Google Scholar]
- 15.Chiò A, Logroscino G, Traynor BJ, et al. Global epidemiology of amyotrophic lateral sclerosis: A systematic review of the published literature. Neuroepidemiology. 2013;41(2):118–30. doi: 10.1159/000351153. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Belsh JM, Schiffman PL. Misdiagnosis in patients with amyotrophic lateral sclerosis. Arch Intern Med. 1990;150(11):2301–5. doi: 10.1001/archinte.1990.00390220055011. [DOI] [PubMed] [Google Scholar]
- 17.Belsh JM, Schiffman PL. The amyotrophic lateral sclerosis (ALS) patient perspective on misdiagnosis and its repercussions. J Neurol Sci. 1996 Aug;139(Suppl):110–6. doi: 10.1016/0022-510X(96)00088-3. [DOI] [PubMed] [Google Scholar]
- 18.Chiò A. ISIS survey: An international study on the diagnostic process and its implications in amyotrophic lateral sclerosis. J Neurol. 1999 Nov;246(3):III1–5. doi: 10.1007/bf03161081. [DOI] [PubMed] [Google Scholar]
- 19.Sawada H. Clinical efficacy of edaravone for the treatment of amyotrophic lateral sclerosis. Expert Opin Pharmacother. 2017 May;18(7):735–8. doi: 10.1080/14656566.2017.1319937. . [DOI] [PubMed] [Google Scholar]
- 20.Brooks BR, Miller RG, Swash M, Munsat TL World Federation of Neurology Research Group on Motor Neuron Diseases. El Escorial revisited: Revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord. 2000 Dec;1(5):293–9. doi: 10.1080/146608200300079536. . [DOI] [PubMed] [Google Scholar]
- 21.Nodera H, Izumi Y, Kaji R. New diagnostic criteria of ALS (Awaji criteria). [Article in Japanese] Brain Nerve. 2007 Oct;59(10):1023–9. [PubMed] [Google Scholar]
- 22.Carvalho MD, Swash M. Awaji diagnostic algorithm increases sensitivity of El Escorial criteria for ALS diagnosis. Amyotroph Lateral Scler. 2009 Feb;10(1):53–7. doi: 10.1080/17482960802521126. . [DOI] [PubMed] [Google Scholar]
- 23.Li DW, Liu M, Cui B, et al. The Awaji criteria increases the diagnostic sensitivity of the revised El Escorial criteria for amyotrophic lateral sclerosis diagnosis in a Chinese population. PLoS One. 2017 Mar 1;12(3):e0171522. doi: 10.1371/journal.pone.0171522. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Geevasinga N, Loy CT, Menon P, et al. Awaji criteria improves the diagnostic sensitivity in amyotrophic lateral sclerosis: A systematic review using individual patient data. Clin Neurophysiol. 2016 Jul;127(7):2684–91. doi: 10.1016/j.clinph.2016.04.005. . [DOI] [PubMed] [Google Scholar]
- 25.Traynor BJ, Codd MB, Corr B, Forde C, Frost E, Hardiman OM. Clinical features of amyotrophic lateral sclerosis according to the El Escorial and Airlie House diagnostic criteria: A population-based study. Arch Neurol. 2000 Aug;57(8):1171–6. doi: 10.1001/archneur.57.8.1171. . [DOI] [PubMed] [Google Scholar]
- 26.Costa J, Swash M, de Carvalho M. Awaji criteria for the diagnosis of amyotrophic lateral sclerosis: A systematic review. Arch Neurol. 2012 Nov;69(11):1410–16. doi: 10.1001/archneurol.2012.254. . [DOI] [PubMed] [Google Scholar]
- 27.Swash M. Why are upper motor neuron signs difficult to elicit in amyotrophic lateral sclerosis? J Neurol Neurosurg Psychiatry. 2012 Jun;83(6):659–62. doi: 10.1136/jnnp-2012-302315. . [DOI] [PubMed] [Google Scholar]
- 28.Kassubek J, Ludolph AC, Müller HP. Neuroimaging of motor neuron diseases. Ther Adv Neurol Disord. 2012 Mar;5(2):119–27. doi: 10.1177/1756285612437562. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Grosskreutz J, Peschel T, Unrath A, Dengler R, Ludolph AC, Kassubek J. Whole brain-based computerized neuroimaging in ALS and other motor neuron disorders. Amyotroph Lateral Scler. 2008 Aug;9(4):238–48. doi: 10.1080/17482960802163622. . [DOI] [PubMed] [Google Scholar]
- 30.Verstraete E, van den Heuvel MP, Veldink JH, et al. Motor network degeneration in amyotrophic lateral sclerosis: A structural and functional connectivity study. PLoS One. 2010 Oct 27;5(10):e13664. doi: 10.1371/journal.pone.0013664. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chiò A, Pagani M, Agosta F, Calvo A, Cistaro A, Filippi M. Neuroimaging in amyotrophic lateral sclerosis: Insights into structural and functional changes. Lancet Neurol. 2014 Dec;13(12):1228–40. doi: 10.1016/S1474-4422(14)70167-X. [DOI] [PubMed] [Google Scholar]
- 32.Matsunaga K, Iwamoto M, Tsuji S, Hashimoto T, Murai Y. [The diagnosis of amyotrophic lateral sclerosis supported by motor evoked potential and brain MRI studies]. Rinsho Shinkeigaku. 1997 Mar;37(3):233–8. [Article in Japanese] [PubMed] [Google Scholar]
- 33.Filippi M, Agosta F, Grosskreutz J, et al. Neuroimaging Society in ALS (NiSALS). Progress towards a neuroimaging biomarker for amyotrophic lateral sclerosis. Lancet Neurol. 2015 Aug;14(8):786–8. doi: 10.1016/s1474-4422(15)00134-9. [DOI] [PubMed] [Google Scholar]
- 34.Foerster BR, Pomper MG, Callaghan BC, et al. An imbalance between excitatory and inhibitory neurotransmitters in amyotrophic lateral sclerosis revealed by use of 3-T proton magnetic resonance spectroscopy. JAMA Neurol. 2013 Aug;70(8):1009–16. doi: 10.1001/jamaneurol.2013.234. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Turner MR, Kiernan MC. Does interneuronal dysfunction contribute to neurodegeneration in amyotrophic lateral sclerosis? Amyotroph Lateral Scler. 2012 May;13(3):245–50. doi: 10.3109/17482968.2011.636050. . [DOI] [PubMed] [Google Scholar]
- 36.Mori S, editor. Introduction to diffusion tensor imaging. Amsterdam, The Netherlands: Elsevier Science; 2008. Subject index: A2 - Mori, Susumu; pp. 175–6. [Google Scholar]
- 37.Sach M, Winkler G, Glauche V, et al. Diffusion tensor MRI of early upper motor neuron involvement in amyotrophic lateral sclerosis. Brain. 2004 Feb;127(Pt 2):340–50. doi: 10.1093/brain/awh041. . [DOI] [PubMed] [Google Scholar]
- 38.Abe O, Yamada H, Masutani Y, et al. Amyotrophic lateral sclerosis: Diffusion tensor tractography and voxel-based analysis. NMR Biomed. 2004 Oct;17(6):411–6. doi: 10.1002/nbm.907. . [DOI] [PubMed] [Google Scholar]
- 39.Ellis CM, Simmons A, Jones DK, et al. Diffusion tensor MRI assesses corticospinal tract damage in ALS. Neurology. 1999 Sep 22;53(5):1051–8. doi: 10.1212/wnl.53.5.1051. . [DOI] [PubMed] [Google Scholar]
- 40.Takahata N, Yamanouchi T, Fukatsu R, Katagiri M. Brain stem gliosis in a case with clinical manifestations of amyotrophic lateral sclerosis. Psychiatry Clin Neurosci. 1976 Mar;30(1):41–8. doi: 10.1111/j.1440-1819.1976.tb00109.x. . [DOI] [PubMed] [Google Scholar]
- 41.Iwata NK, Aoki S, Okabe S, et al. Evaluation of corticospinal tracts in ALS with diffusion tensor MRI and brainstem stimulation. Neurology. 2008 Feb 12;70(7):528–32. doi: 10.1212/01.wnl.0000299186.72374.19. . [DOI] [PubMed] [Google Scholar]
- 42.Foerster BR, Dwamena BA, Petrou M, et al. Diagnostic accuracy of diffusion tensor imaging in amyotrophic lateral sclerosis: A systematic review and individual patient data meta-analysis. Acad Radiol. 2013 Sep;20(9):1099–106. doi: 10.1016/j.acra.2013.03.017. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Schweitzer AD, Liu T, Gupta A, et al. Quantitative susceptibility mapping of the motor cortex in amyotrophic lateral sclerosis and primary lateral sclerosis. AJR Am J Roentgenol. 2015 May;204(5):1086–92. doi: 10.2214/ajr.14.13459. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lee JY, Lee YJ, Park DW, et al. Quantitative susceptibility mapping of the motor cortex: A comparison of susceptibility among patients with amyotrophic lateral sclerosis, cerebrovascular disease, and healthy controls. Neuroradiol. 2017 Dec;59(12):1213–22. doi: 10.1007/s00234-017-1933-9. . [DOI] [PubMed] [Google Scholar]
- 45.Iwata NK, Kwan JY, Danielian LE, et al. White matter alterations differ in primary lateral sclerosis and amyotrophic lateral sclerosis. Brain. 2011 Sep;134(Pt 9):2642–55. doi: 10.1093/brain/awr178. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Han J, Ma L. Study of the features of proton MR spectroscopy ((1)H-MRS) on amyotrophic lateral sclerosis. J Magn Reson Imaging. 2010 Feb;31(2):305–8. doi: 10.1002/jmri.22053. . [DOI] [PubMed] [Google Scholar]
- 47.Govind V, Sharma KR, Maudsley AA, Arheart KL, Saigal G, Sheriff S. Comprehensive evaluation of corticospinal tract metabolites in amyotrophic lateral sclerosis using whole-brain 1H MR spectroscopy. PLoS One. 2012;7(4):e35607. doi: 10.1371/journal.pone.0035607. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Verstraete E, Veldink JH, Hendrikse J, Schelhaas HJ, van den Heuvel MP, van den Berg LH. Structural MRI reveals cortical thinning in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2012 Apr;83(4):383–8. doi: 10.1136/jnnp-2011-300909. . [DOI] [PubMed] [Google Scholar]
- 49.Oba H, Araki T, Ohtomo K, et al. Amyotrophic lateral sclerosis: T2 shortening in motor cortex at MR imaging. Radiology. 1993 Dec;189(3):843–6. doi: 10.1148/radiology.189.3.8234713. . [DOI] [PubMed] [Google Scholar]
- 50.Spinelli EG, Agosta F, Ferraro PM, et al. Brain MR imaging in patients with lower motor neuron-predominant disease. Radiol. 2016 Aug;280(2):545–56. doi: 10.1148/radiol.2016151846. . [DOI] [PubMed] [Google Scholar]
- 51.Stroman PW, Wheeler-Kingshott C, Bacon M, et al. The current state-of-the-art of spinal cord imaging: Methods. Neuroimage. 2014 Jan 1;84:1070–81. doi: 10.1016/j.neuroimage.2013.04.124. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Mohammadi B, Kollewe K, Samii A, Krampfl K, Dengler R, Münte TF. Changes of resting state brain networks in amyotrophic lateral sclerosis. Exp Neurol. 2009 May;217(1):147–53. doi: 10.1016/j.expneurol.2009.01.025. . [DOI] [PubMed] [Google Scholar]
- 53.Filippi M, Agosta F, Abrahams S, et al. European Federation of Neurological Societies. EFNS guidelines on the use of neuroimaging in the management of motor neuron diseases. Eur J Neurol. 2010 Apr;17(4):526–e20. doi: 10.1111/j.1468-1331.2010.02951.x. . [DOI] [PMC free article] [PubMed] [Google Scholar]