

Abstract
Children born preterm (PT) have a higher risk of language delays than children born full-term (FT). Expressive vocabulary plays a central role in language development, as later grammar ability can be predicted from earlier vocabulary size.
To determine the effects of preterm birth on expressive vocabulary at the age of 36 to 41 months.
Cross-sectional study of 27 PT (children with a gestational age of ≤ 32 + 0 weeks and/or a birth weight ≤ 1500 g) and 26 FT children (from several kindergartens in Vienna, Austria). The groups were matched regarding age, sex, and monolingual Austrian German speech. They were all examined using the active vocabulary test (AWST-R) and the development test, Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III).
The AWST-R revealed significantly lower scores (46% vs 52%, P = .027) for PT children. The Bayley-III revealed significantly lower scores in language development (mean 96.3 ± 11.81 vs 105.1 ± 6.24, P = .002) and the expressive communication subscale (8.78 ± 2.01 vs 10.69 ± 1.49, P < .001) for PT children, but no differences in cognitive development (98.5 ± 11.08 vs 100.8 ± 6.43, P = .369) or on the receptive communication subscale (10.15 ± 2.23 vs 11.08 ± 1.09, P = .060).
Preterm children tested had less expressive vocabulary (AWST-R and Bayley-III) than those born full-term, while test results in their cognitive development and receptive communication (Bayley-III) did not differ.
Keywords: AWST-R - expressive vocabulary test, Bayley scales of infant and toddler development, children born preterm, cognitive development, cross-sectional study, expressive vocabulary, monolingual Austrian German speech, third edition (Bayley-III)
1. Introduction
The survival rate of preterm infants has increased dramatically over the last decades, especially among infants with extremely low birth weight,[1] which has led to an increase in the number of children at developmental risk.[1,2] Children born preterm are prone to delays in cognitive[3] and language development compared to children born full-term.[4–11] Cognitive development is known to influence language skills.[12–14]
When children produce their first words, typically at the end of the first year of life,[15] they already understand 50 words on average.[16] This discrepancy between receptive and expressive vocabulary persists throughout language development.[17] The development of early expressive vocabulary varies from child to child.[16,18] Children's expressive vocabulary greatly increases during the second year of life,[19,20] reaching up to 2000 words at the age of 3.[21,22]
The evaluation of the expressive vocabulary of children aged 3 years or under is usually based on parental report forms. In the early period of language acquisition, parental reports are considered representative based on the assumption that parents are in constant contact with their child. Moreover, a parent questionnaire does not require active cooperation on the part of the child. In this regard, the MacArthur-Bates Communicative Development Inventories (CDIs)[23] have proved to be a valid test instrument. The equivalent instrument for Austrian German-speaking children is the Austrian Communicative Development Inventories, Level 2 (ACDI-2).[24,25] At the age of 3 years, when children already have acquired a large vocabulary, parental reports can no longer adequately assess the children's whole expressive vocabulary. Furthermore, children at the age of 3 years are able or even more able to participate actively in a test battery. Therefore, the use of expressive vocabulary tests such as the German picture-naming test, Aktiver Wortschatztest - Revision (AWST-R) (Expressive Vocabulary Test - Revised),[26] for the purposes of assessing 3-year-olds’ expressive vocabulary appears to be appropriate and effective.
While even children born full-term with a history of hospitalization in a neonatal intensive care unit (NICU) or with low Apgar scores are at higher risk of delays regarding word production,[25] this risk might more likely affect children born preterm with more or less long stays at a NICU. Several additional risk factors have been found that affect the language development of children born preterm: low Apgar scores,[27,28] low gestational age,[5,6,11,29] birth weight,[29,32] male sex,[10,11,30,31] medical complications,[33–36] and poor cognitive development.[9,36,37] The educational level of the mother has an influence on language development as well.[36–38] Unlike other language categories, expressive vocabulary can be promoted by parents in the home environment if support is provided by trained staff.
The aim of our study was to investigate the expressive vocabulary of Austrian German-speaking children born preterm at the age of 36 to 41 months (uncorrected for gestational age at birth) in comparison to children born full-term by using the expressive vocabulary test AWST-R and the Bayley-III developmental test. We hypothesized that Austrian German-speaking children born preterm have a 15% smaller expressive vocabulary compared to children born full-term.
2. Materials and methods
2.1. Participants
This cross-sectional study assessed 53 German-speaking children (27 born preterm and 26 full-term) at the age of 36 to 41 months. The PT (children born preterm) and FT (children born full-term) groups were matched regarding age, sex, and monolingual German speech in Austria.
2.2. Study group
Twenty-seven monolingual German-speaking children born preterm were recruited from 2 pediatric hospitals in Vienna, Austria: the Wilhelminenspital and the Vienna General Hospital (AKH Wien). Dates of birth ranged from November 2012 to November 2013. The inclusion criteria were as follows:
-
1.
gestational age (GA) ≤ 32 + 0 and/or birth weight (BW) ≤ 1500 g,
-
2.
medical care in Vienna at the Pediatric Department of the Wilhelminenspital or the Vienna General Hospital,
-
3.
growing up in a monolingual Austrian German-speaking family,
-
4.
assessment age of 36 to 41 months not corrected for gestational age at birth, and
-
5.
written consent of the parents.
The exclusion criteria were:
-
1.
syndromal disorders,
-
2.
growing up in a multilingual family,
-
3.
asphyxia (intra-uterine or during birth),
-
4.
other diseases, including cystic fibrosis, cleft lip and palate, tumor diseases, mental illness, and
-
5.
intraventricular hemorrhage > grade II.
The study group's clinical data included maternal age in years, gestational age in weeks, birth weight, Apgar scores at 1, 5, and 10 minutes, educational level of the parents, and family status. Presence of the following comorbidities was documented: Respiratory distress syndrome, mechanical ventilation, atrial septal defect, bronchopulmonary dysplasia (oxygen dependency at the corrected age of 36 weeks), intraventricular hemorrhage grad 1–4, necrotizing enterocolitis, persisting ductus arteriosus Botalli, retinopathy of prematurity, periventricular leucomalacia, and sepsis.
2.3. Control group
Twenty-six children born full-term were recruited from several kindergartens in Vienna, Austria. The dates of birth of the control group ranged from September 2012 to May 2013. The inclusion criteria were as follows:
-
1.
growing up in a monolingual Austrian German-speaking family,
-
2.
assessment age of 36 to 41 months, and
-
3.
written consent of the parents.
The exclusion criteria were:
-
1.
syndromal disorders,
-
2.
growing up in a multilingual family,
-
3.
asphyxia (intra-uterine or during birth),
-
4.
other diseases, including cystic fibrosis, cleft lip and palate, tumor diseases, mental illness, and
-
5.
intraventricular hemorrhage > grade II.
The control group's clinical data included maternal age in years, gestational age in weeks, birth weight, Apgar scores at 1, 5, and 10 minutes, educational level of the parents, and family status. The controls being healthy subjects, no other data were evident.
2.4. Assessments at 36 to 41 months of age
All children were subjected to 2 standardized tests during their regular follow-up:
-
1.
the Expressive Vocabulary Test (AWST-R) [26] and
-
2.
the Bayley Scales of Infant and Toddler Development III (Bayley-III).[39]
The AWST-R is a standardized expressive vocabulary test instrument developed for German-speaking children between 3;0 and 5;5 years of age,[26] requiring them to verbalize one-word responses to pictures presented to them. Picture naming is a complex achievement based on numerous factors. In order to be able to name pictures, the child must have stored phonological and syntactic knowledge, as the word name is associated with existing word-meaning knowledge (semantic-conceptual knowledge).[26] The test consists of 51 nouns and 24 verbs presented graphically. For example, the investigator-in-charge asks “What's he/she doing?” for verbs like “sleep” or “What's that?” for nouns like “tree.” The child's word expression is assessed by means of a quantitative score. Results are given as percentages and raw values. Furthermore, the 75 AWST-R pictures can be sub-classified into 13 item categories: Draußen/Natur (outdoors/nature), Wohnung/Haus/Gebäude (apartment/house/building), Spiel-/Sport-/Freizeitobjekte (games-/sports-/recreational facilities/objects), Verben: Spiel/Sport/Freizeit (games/sports/leisure verbs), Verben: häusliches Umfeld (home environment verbs), Verben: nonverbale Ausdrucksfähigkeit (nonverbal expressiveness verbs), Verben: verbale Ausdruckfähigkeit (verbal expressiveness verbs), Gebrauchsgegenstände/Haushalt (everyday objects/household), Körperpflege/Gesundheit/Körper/Krankheit (personal/hygiene/health/body/ illness), Tiere (animals), Nahrung (food), Kleidung (clothing), and Symbole (symbols). The individual strengths in the various categories depend greatly on the language input to which the child is exposed. The 13 categories help in the analysis of the results of the AWST-R, allowing speech therapists and parents to focus on the categories in which the child still has some delay.
The Bayley-III provides separate assessments for cognitive, language, and motor development.[39] As motor development was not the focus of the current study, it is not discussed here. The cognitive scale examines sensorimotor development, exploration and manipulation, object relatedness, concept formation, memory, and other aspects of cognitive processing.[39] The significant revision of the Bayley-III compared to the previous versions enables the language scale to be differentiated into expressive and receptive communication subscales for the first time. The receptive communication subscale tests vocabulary development aspects such as identifying referenced objects and pictures, vocabulary related to morphological development (pronouns and prepositions), and the understanding of morphological markers (plural, tense, and possessive).[39] The expressive communication subscale tests vocabulary development aspects, for example, naming objects, pictures, and attributes, as well as morphosyntactic development aspects such as using 2-word utterances, plurals, and verb tense.[39] Both the cognitive and the language development scale have a standard score of 100 ± 15 (mean ± 1 SD). Scores < 70 (> 2 SD below the mean) are considered to be “low,” indicating delay, while scores between 70 and 84 (> 1 SD below the mean) are considered “low average,” indicating mild to moderate delay. Scores > 85 are related to normal development. The language development subscales have a standard raw score ranging from 1 to 19, with a mean of 10 and a standard deviation of 3.
The study was approved by the Vienna City Council's Ethics Committee (EK-15–281-VK, dated April 4, 2016) and the Ethics Committee of the Medical University of Vienna (159/2016, dated September 21, 2016).
3. Statistical analyses
Given that children born full-term at the age of 36 to 41 months are able to correctly name 25 words in average from the AWST-R and assuming that children born preterm have a 15% reduced expressive vocabulary, assuming a power (1-ß) of 0.80 at a significance level α of 0.05 resulted in 25 children per group, to detect this noticeable effect (d ≥ 0.80) according to the Cohen classification.[40]
Statistical analyses were performed using IBM SPSS 20 for Windows for descriptive and inferential statistics. The significance level α was set at 5%. Welch t tests were used for comparisons between groups.[41] Welch t test restricts the nominal risk of alpha error and proves robustness at 20%. The assessment of the difference in vocabulary performance as a function of both age at birth and sex was performed by means of 2-way univariate ANOVAs. Contingency tables for nominally scaled variables (with 2 or more steps) were examined using the chi-squared (χ2) test. Pearson correlation coefficient r was used to express the strength of the relationship between 2 parameters.[42] Fisher z-transformation was used to examine the difference in the correlation between 2 independent groups.
4. Results
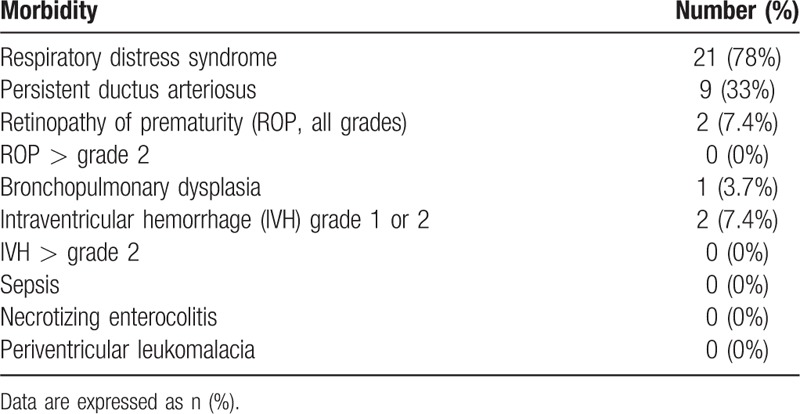
The participants’ demographic data are given in Table 1. The comparison of the variables of gestational age and birth weight showed significant differences between the study group and the control group, confirming correct use of the inclusion criteria. The Apgar scores at 1–5–10 minutes also differed significantly. Sex was distributed homogeneously in each group. There was a small but significant difference in both maternal (P = .045) and paternal (P = .046) education levels. The details are given in Table 2. There was no difference (P = .194) in terms of the family status of the parents. The PT group represented low rates of major morbidities, details of which are given in Table 3.
Table 1.
Demographic data of the study and control group.
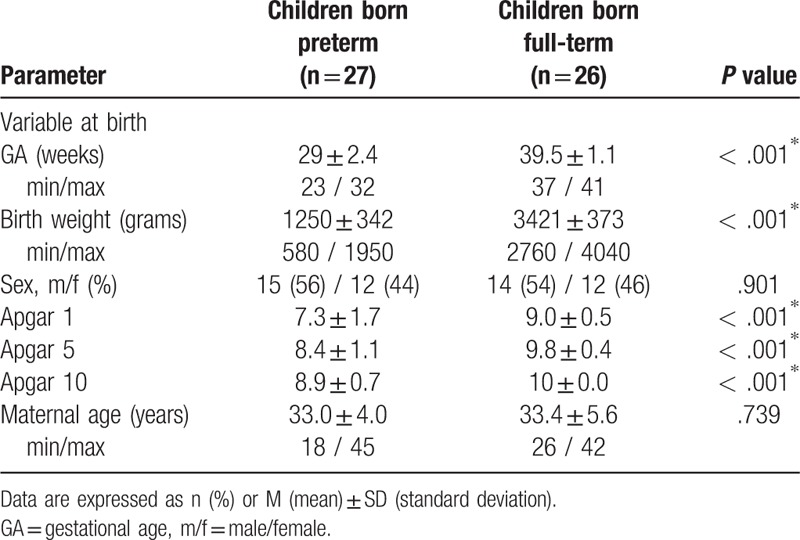
Table 2.
Parental level of education.
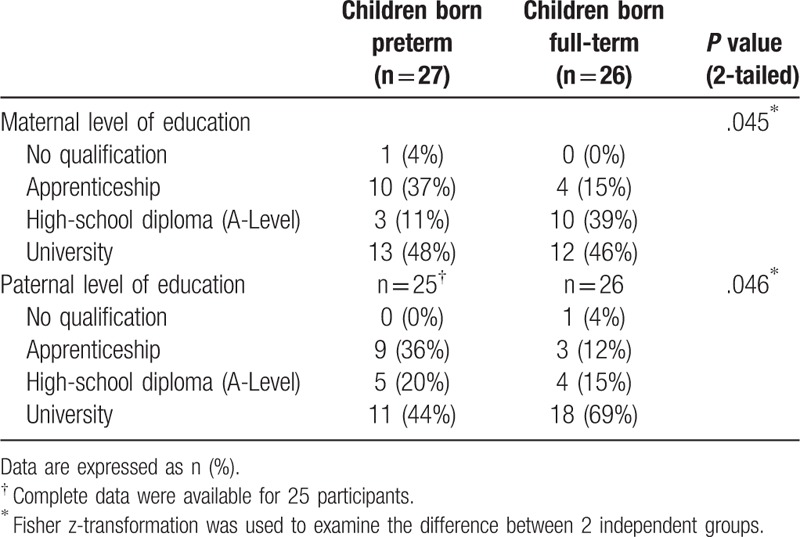
Table 3.
Major morbidities of the preterm infant (n = 27) group.
4.1. AWST-R results
Significant differences were found in both the study and control groups’ expressive vocabulary rates (46.4% ± 10.8 vs 52.2% ± 7.5, P = .027) (Fig.3). Details are given in Table 4. The evaluation of the 75 AWST-R pictures sub-classified into 13 item categories showed significant differences in 3 categories: outdoors/nature (mean 15.23 ± 10.74 vs mean 25.21 ± 17.37, P = .016), verbal verb expressiveness (mean 25.93 ± 28.99 vs mean 53.85 ± 34.42, P = 0002) and clothing (mean 40.74 ± 31.12 vs mean 55.13 ± 18.72, P = .047). Details are given in Table 5.
Table 4.
Developmental results and results for expressive vocabulary.
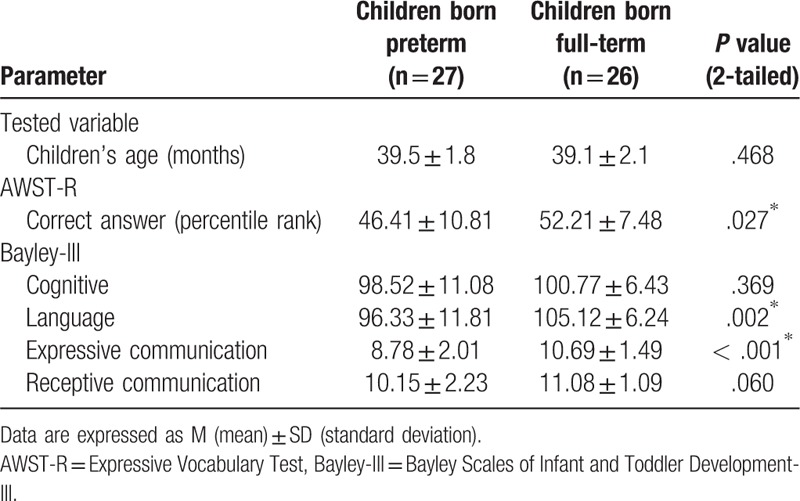
Table 5.
AWST-R item categories.
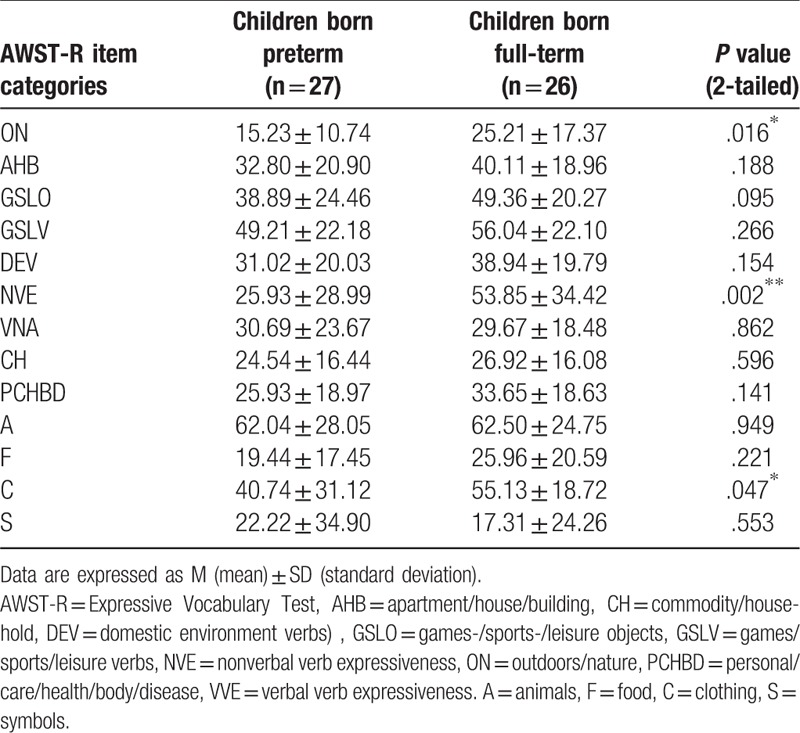
Figure 3.
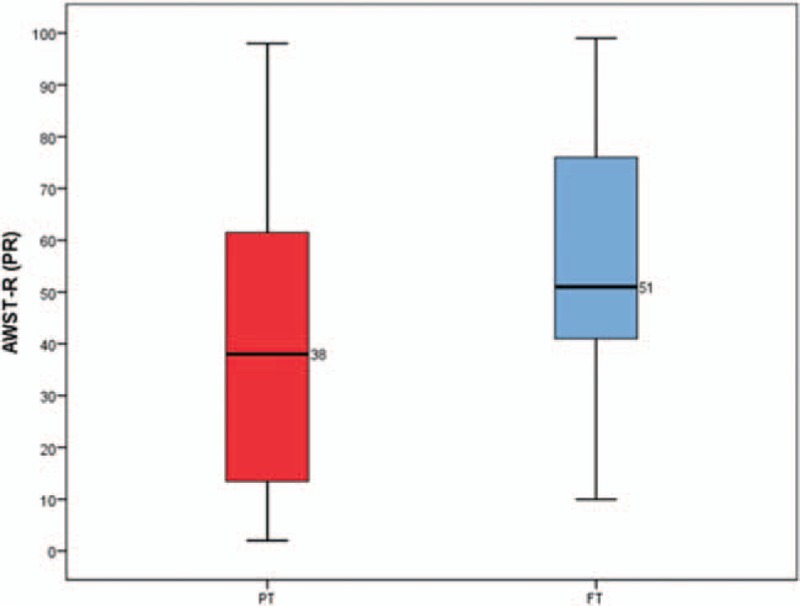
AWST-R results comparing 27 children born preterm with 26 children born full-term at the age of 36 to 41 months. AWST-R = active vocabulary test.
4.2. Bayley-III results
There was no difference between the 2 groups (mean 98.5 ± 11.1 vs mean 100.8 ± 6.4, P = .369) in cognitive development, while significant differences were found in language development (96.3 ± 11.8 vs 105.1 ± 6.2, P = .002) (Fig. 1). The evaluation of the 2 language development subscales showed a significant difference in expressive communication (8.78 ± 2.01 vs 10.69 ± 1.49, P < .001) (Fig. 2) but no difference in receptive communication (10.15 ± 2.23 vs 11.08 ± 1.09, P = .060). Details are given in Table 4.
Figure 1.
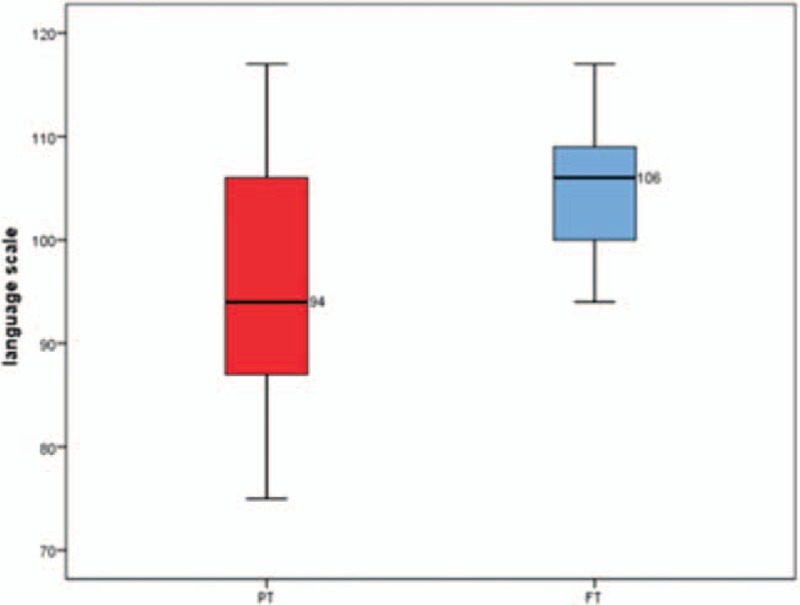
Bayley-III scores for the language scale comparing 27 children born preterm with 26 children born full-term at the age of 36 to 41 months. Bayley-III = Bayley scales of infant and toddler development, Third Edition.
Figure 2.
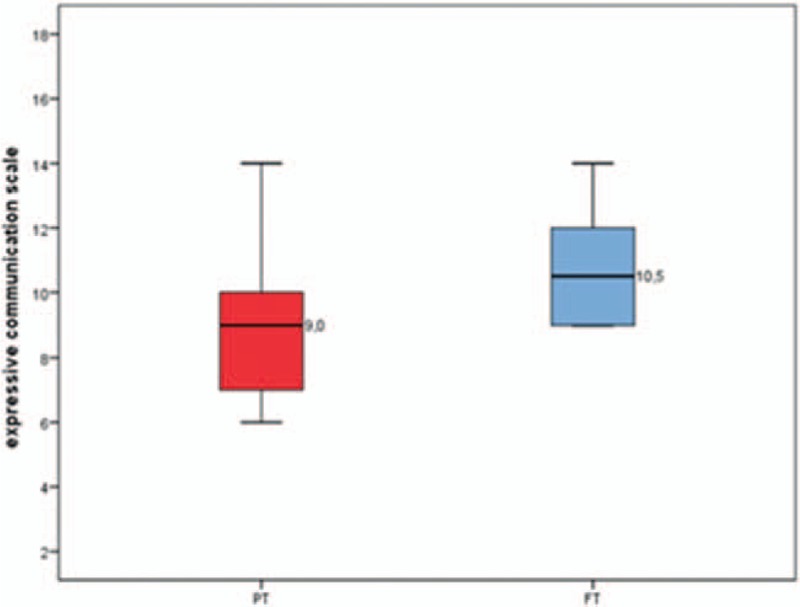
Bayley-III scores for the expressive communication subscale comparing 27 children born preterm with 26 children born full-term at the age of 36 to 41 months. Bayley-III = Bayley scales of infant and toddler development, Third Edition.
5. Discussion
The present cross-sectional study examined the expressive vocabulary of Austrian German-speaking PT compared to FT at the age of 36 to 41 months, using the AWST-R expressive vocabulary test. We found that the PT group had a smaller expressive vocabulary than the FT group. The Bayley-III also showed significant differences in language development. Subscale analysis of the Bayley-III regarding expressive communication revealed significantly lower scores in the PT group. Interestingly, the “cognitive development” and subscale “receptive communication” scores did not differ between the 2 groups.
Our results are similar to the findings of recent studies,[43–46] which examined children at the comparable age of 36 months.[43,44,46] Furthermore, the results of other studies[5,6,47,48,49–53] and 2 meta-analyses [54,55] at different ages led to the same conclusion that children born preterm have a smaller expressive vocabulary than children born full-term.
Poor cognitive, motor and sensory development, either in isolation or combination, is known to contribute to poor language development.[41] The isolated difference regarding expressive language scores is of interest. It might correlate with a low rate of severe comorbidities in our study group.
A detailed analysis of the 13 semantic fields in the AWST-R showed that significant differences could be found in 3 categories: outdoors/nature, verbal verb expressiveness and clothing. In this context, the significant differences in these 3 areas appear to be interesting, since clothing, for instance, represents an important aspect of daily life. Poor language performance in this field might be easily remedied by parents.
The PT and FT in our study were also tested with the Bayley-III. The Bayley-III showed significant differences on the subscale “expressive communication” too. Interestingly, the “cognitive development” scale and “receptive communication” subscale scores did not differ between the 2 groups. Most of the PT studies also used the Bayley-II or Bayley-III as an additional developmental test.[6,44,47,49,52,53,56] The findings indicated significant differences in cognitive development between PT and FT at a younger test age [6,44,49,52] but these findings were also noted in children at age 48 months.[57] Our results differ regarding the “receptive communication” subscale compared to the literature.[50,52,54,55,57,58] As receptive vocabulary contributes to expressive language development,[17] our findings may indicate a chance of catch-up growth as far as expressive language is concerned.
In this study, the PT and FT were homogeneous in terms of “children's age at testing”, “maternal age at delivery” and “gender distribution”. These characteristics could therefore not have influenced the significant differences in expressive vocabulary between the 2 groups.
According to the inclusion criteria applied, there were significant differences between PT and FT in the variables “Apgar Score 1–5–10”, “gestational age”, and “birth weight”. The study can thus substantiate that these variables might have an effect on the expressive vocabulary of preterm infants at birth. The important influence of low Apgar scores, GA, and BW on language development is well known.[5,6,11,27–32]
Apart from these variables, the level of parental education differed significantly between the 2 groups. Parents of PT had lower maternal and paternal educational levels than parents of FT. This might additionally impact negatively on the expressive vocabulary of the PT group and corresponds to earlier published results. Those studies found that the educational level of the mother has an impact on language development.[36–38]
The main limitation of the study was the difficulty recruiting the study participants, which proved to be very costly and time-consuming due to the narrow inclusion criteria. The factor “monolingual German” required undreamt-of efforts, as a large number of the PT at the City of Vienna's Wilhelminenspital have a migration background and are therefore bi- or trilingual. In the course of the survey, it became clear that sufficient study participants could not be obtained at the Wilhelminenspital alone, so we recruited participants from the Vienna General Hospital (AKH) as well.
The main characteristics and strengths of the study are the particular age group (36–41 months) and the active assessment of expressive vocabulary using the AWST-R. In addition, a control group was recruited for the study, which was matched with the PT group in age, gender and monolingual German speech. All children included in the study were also tested with Bayley-III in addition to AWST-R. This made it possible to obtain an overall picture of the children in terms of cognition and language skills.
In conclusion, using the AWST-R and the “expressive communication” subscale of the Bayley-III in children aged 36 to 41 months, we found that PT had a less expressive vocabulary than FT, while the “cognitive development” scale and the “receptive communication” subscale results did not differ between the 2 groups. Providing parental or carer (e.g., grandparents, uncles, aunties, babysitters) support for PT might help them to catch up on their expressive vocabulary acquisition.
Acknowledgments
We would like to thank all the children and their parents for their participation in the study.
Author contributions
Conceptualization: Nina Brósch-Fohraheim.
Data curation: Nina Brósch-Fohraheim, Renate Fuiko.
Formal analysis: Nina Brósch-Fohraheim.
Funding acquisition: Nina Brósch-Fohraheim.
Investigation: Nina Brósch-Fohraheim.
Methodology: Nina Brósch-Fohraheim.
Project administration: Nina Brósch-Fohraheim.
Resources: Nina Brósch-Fohraheim.
Software: Nina Brósch-Fohraheim.
Supervision: Nina Brósch-Fohraheim, Bernhard Resch.
Validation: Nina Brósch-Fohraheim.
Visualization: Nina Brósch-Fohraheim.
Writing – original draft: Nina Brósch-Fohraheim.
Writing – review & editing: Nina Brósch-Fohraheim, Peter B. Marschik, Bernhard Resch.
Nina Brósch-Fohraheim orcid: 0000-0002-2964-7882.
Footnotes
Abbreviations: AKH = Vienna general hospital, AWST-R = active vocabulary test, Bayley-III = Bayley scales of infant and toddler development, Third Edition, BW = birth weight, FT = full-term born children, GA = gestational age, NICU = neonatal intensive care unit, PT = preterm born children.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- [1].Philip AG. The evolution of neonatology. Pediatr Res 2005;58:799–815. [DOI] [PubMed] [Google Scholar]
- [2].Singer D. Die Langzeitprognose von Frühgeborenen: Was sich hinter den Statistiken verbirgt. Zeitschrift für Geburtshilfe und Neonatologie 2006;210:50–9. [DOI] [PubMed] [Google Scholar]
- [3].Bhutta AT, Cleves MA, Casey PH, et al. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis. JAMA 2002;288:728–37. [DOI] [PubMed] [Google Scholar]
- [4].Magill-Evans J, Harrison MJ. Parent-child interactions and development of toddlers born preterm. West J Nurs Res 1999;21:292–307. [DOI] [PubMed] [Google Scholar]
- [5].Kern S, Gayraud F. Influence of preterm birth on early lexical and grammatical acquisition. First Lang 2007;27:159–73. [Google Scholar]
- [6].Foster-Cohen S, Edgin JO, Champion PR, et al. Early delayed language development in very preterm infants: evidence from the MacArthur-Bates CDI. J Child Lang 2007;34:655–75. [DOI] [PubMed] [Google Scholar]
- [7].Stolt S, Lehtonen L, Haataja L, et al. The language used in early mother-child interaction by very-low-birth-weight children, with a focus on the emergence of grammar. Rev Logop Fon Audiol 2011;31:115–24. [Google Scholar]
- [8].Stolt S, Lehtonen L, Haataja L, et al. The development and predictive value of early vocalizations in prematurely born very-low-birth-weight children: a longitudinal study. Clin Linguist Phon 2012;26:414–27. [DOI] [PubMed] [Google Scholar]
- [9].Sansavini A, Savini S, Guarini A, et al. The effect of gestational age on developmental outcomes: a longitudinal study in the first two years of life. Child: Care, Health Dev 2010;37:26–36. [DOI] [PubMed] [Google Scholar]
- [10].Sansavini A, Guarini A, Savini S. Linguistic and cognitive delays in very preterm infants at 2 years: general or specific delays? Rev Logop Fon Audiol 2011;31:133–47. [Google Scholar]
- [11].Schults A, Tulviste T, Haan E. Early vocabulary in full term and preterm Estonian children. Early Hum Dev 2013;89:721–6. [DOI] [PubMed] [Google Scholar]
- [12].Bloom L, Tinker E, Margulis C. The words children learn: evidence against a noun bias in early vocabularies. Cog Dev 1993;8:431–50. [Google Scholar]
- [13].Weinert S. Wortschatzerwerb und kognitive Entwicklung. Sprache-Stimme-Gehör 2004;28:20–8. [Google Scholar]
- [14].Hollich G, Hirsh-Pasek K, Golinkoff R, et al. Breaking the language barrier: An emergentist coalition model for the origins of word learning. Monogr Soc Res Child Dev 2000;65:1–23. [PubMed] [Google Scholar]
- [15].Kauschke C. Der Erwerb des frühkindlichen Lexikons - eine empirische Studie zur Entwicklung des Wortschatzes im Deutschen. Tübingen. Narr 2000. 8–36. [Google Scholar]
- [16].Fenson L, Dale P, Reznick J, et al. Variability in early communicative development. Monogr Soc Res Child Dev 1994;59:1–73. [PubMed] [Google Scholar]
- [17].Bates E, Dale P, Thal D. Individual differences and their implications for theories of language development. In: Fletcher, P. & Mac Whinney, B. (Eds.), Handbook of Child Language. Oxford, Basil Blackwell; 1995:96–151. [Google Scholar]
- [18].Bates E, Goodman J. On the emergence of language from the lexicon. In: B. MacWhinney (Ed.): The Emergence of Language. Mahwah,N.J., Lawrence Erlbaum; 1999:29–79. [Google Scholar]
- [19].Kauschke C. Kindlicher Spracherwerb im Deutschen: Verläufe, Forschungsmethoden, Erklärungsansätze. Berlin. De Gruyter 2012. 42–68. [Google Scholar]
- [20].Dapretto M, Bjork E. The development of word retrieval abilities in the second year and its relation to early vocabulary growth. Child Dev 2000;71:635–48. [DOI] [PubMed] [Google Scholar]
- [21].Dittmann J. Der Spracherwerb des Kindes. Verlauf und Störungen. 3. Auflage. München. Verlag C H Beck 2010. 36–45. [Google Scholar]
- [22].Kannengieser S. Sprachentwicklungsstörungen. Grundlagen, Diagnostik und Therapie. München: Urban & Fischer/Elsevier; 2009. [Google Scholar]
- [23].Fenson L, Dale PS, Reznick JS, et al. The MacArthur Communicative Development Inventories: User's Guide and Technical Manual. San Diego: Singular Publishing Group; 1993. [Google Scholar]
- [24].Marschik PB, Vollmann R, Einspieler C. Austrian Communicative Development Inventories, Level 2. 2nd EditionGraz: Medizinische Universität Graz; 2004. [Google Scholar]
- [25].Marschik PB, Einspieler C, Garzarolli B, et al. Events at early development: are they associated with early word production and neurodevelopmental abilities at the preschool age? Early Hum Dev 2007;83:107–14. [DOI] [PubMed] [Google Scholar]
- [26].Kiese-Himmel C. AWST-R. Aktiver Wortschatztestfür 3- bis 5-jährige Kinder - Revision. Göttingen: Beltz; 2005. [Google Scholar]
- [27].Pérez-Pereira M, Fernández P, Resches M, et al. Determinants of early language and communication in preterm and fullterm infants: a comparative study. Enfance 2013;1:59–76. [Google Scholar]
- [28].Cusson RM. Factors influencing language development in preterm infants. J Obstet Gynecol Neonatal Nurs 2003;32:402–9. [DOI] [PubMed] [Google Scholar]
- [29].Largo RH, Molinari L, Comenale Pinto L, et al. Language development of term and preterm children during the first five years of life. Dev Med Child Neurol 1986;28:333–50. [DOI] [PubMed] [Google Scholar]
- [30].Bosch L, Ramon Casas M, Solé J, et al. Desarrollo léxico en el prematuro: medidas del vocabulario expresivo en el segundo año de vida. Rev Logop Fon Audiol 2011;31:169–79. [Google Scholar]
- [31].Sansavini A, Guarini A, Alessandroni R, et al. Early relations between lexical and grammatical development in very immature Italian preterms. J Child Lang 2006;33:199–216. [DOI] [PubMed] [Google Scholar]
- [32].Islam UA, Poole KL, Schmidt LA, et al. Childhood language skills and adolescent self-esteem in preterm survivors. J Child Health Care 2018;22:34–45. [DOI] [PubMed] [Google Scholar]
- [33].Singer LT, Siegel AC, Lewis B, et al. Preschool language outcomes of children with history of bronchopulmonary dysplasia and very low birth weight. J Dev Behav Pediatr 2001;22:19–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Lewis BA, Singer LT, Fulton S, et al. Speech and language outcomes of children with bronchopulmonary dysplasia. J Commun Disord 2002;35:393–406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Baron IS, Ahronovich MD, Erickson K, et al. Age-appropriate early school age neurobehavioral outcomes of extremely preterm birth without severe intraventricular hemorrhage: a single center experience. Early Hum Dev 2009;85:191–6. [DOI] [PubMed] [Google Scholar]
- [36].Sansavini A, Guarini A, Savini S, et al. Longitudinal trajectories of gestural and linguistic abilities in very preterm infants in the second year of life. Neuropsychologia 2011;49:3677–88. [DOI] [PubMed] [Google Scholar]
- [37].Stolt S, Klippi A, Launonen K, et al. Size and composition of the lexicon in prematurely born very-low-birth-weight and full-term Finnish children at two years of age. J Child Lang 2007;34:283–310. [DOI] [PubMed] [Google Scholar]
- [38].Sansavini A, Guarini A, Alessandroni R, et al. Are early grammatical and phonological working memory abilities affected by preterm birth? J Commun Disord 2007;40:239–56. [DOI] [PubMed] [Google Scholar]
- [39].Reuner G, Rosenkranz J. Bayley-Scales of Infant and Toddler Development, Third Edition - Deutsche Version. Frankfurt/M: Pearson Assessment; 2014. [Google Scholar]
- [40].Cohen J. Statistical power analysis for the behavioral sciences. Second EditionHillsdale/NJ: Lawrence Erlbaum; 1988. [Google Scholar]
- [41].Kubinger K, Rasch D, Moder K. Zur legende der Voraussetzungen des t- Tests für unabhängige Stichproben. Psychologische Rundschau 2009;60:26–7. [Google Scholar]
- [42].Field A. Discovering Statistics Using SPSS. 3rd EditionLondon: Sage Publications Ltd; 2009. [Google Scholar]
- [43].Ribeiro C, Lamônica D. Communicative Abilities in Premature and extreme premature Infants. Rev CEFAC 2014;16:830–9. [Google Scholar]
- [44].Fasolo M, D’Odorico L, Constantini A, et al. The influence of biological, social, and developmental factors on language acquisition in pre-term born children. Int J Speech Lang Pathol 2010;12:461–71. [DOI] [PubMed] [Google Scholar]
- [45].Soraya M, Mahmoodi-Bakhtiari B, Badiee Z, et al. The size of expressive lexicon in prematurely born children low-birth-weight with full-term 18 to 36 month's children: a comparative study. J Neurosci Behav Health 2012;4: Available at: http://aud.tums.ac.ir/article-1-58-en.pdf (Accessed 12 February 2018). [Google Scholar]
- [46].Costantini A, Coppola G, Fasolo M, et al. Preterm birth enhances the contribution of mothers’ mind-mindedness to infants’ expressive language development: a longitudinal investigation. Infant Behav Dev 2017;49:322–9. [DOI] [PubMed] [Google Scholar]
- [47].D’Odorico L, Majorano M, Fasolo M, et al. Characteristics of phonological development as risk factor for language development in Italian-speaking preterm children: a longitudinal study. Clin Linguist Phon 2010;25:53–65. [DOI] [PubMed] [Google Scholar]
- [48].Isotani SM, Frasson de Azevedo MF, Chiari BM, et al. Expressive language of two-year-old pre-term and full-term children. Pro Fono 2009;21:155–9. [DOI] [PubMed] [Google Scholar]
- [49].Stolt S, Matomäki J, Haataja L, et al. The emergence of grammar in very-low-birth-weight Finnish children at two years of age. J Child Lang 2013;40:336–57. [DOI] [PubMed] [Google Scholar]
- [50].Jansson-Verkasalo E, Valkama M, Vainionpää L, et al. Language development in very low birth weight preterm children: a follow-up study. Folia Phoniatr Logop 2004;56:108–19. [DOI] [PubMed] [Google Scholar]
- [51].Guarini A, Sansavini A, Fabbri C, et al. Reconsidering the impact of preterm birth on language outcome. Early Hum Dev 2009;85:639–45. [DOI] [PubMed] [Google Scholar]
- [52].Adams-Chapman I, Bann C, Carter SL, et al. Language outcomes among ELBW infants in early childhood. Early Hum Dev 2015;91:373–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [53].Marchman VA, Loi EC, Adams KA, et al. Speed of language comprehension at 18 months old predicts school-relevant outcomes at 54 months old in children born Preterm. J Dev Behav Pediatr 2018;39:246–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Barre N, Morgan A, Doyle LW, et al. Language abilities in children who were very preterm and/or very low birth weight: a meta-analysis. J Pediatr 2011;158:766–74. [DOI] [PubMed] [Google Scholar]
- [55].Zimmerman E. Do infants born very premature and who have very low birth weight catch up with their full term peers in their language abilities by early school age? J Speech Lang Hear Res 2018;61:53–65. [DOI] [PubMed] [Google Scholar]
- [56].Sansavini A, Pentimonti J, Justice LM, et al. Language, motor and cognitive development of extremely preterm children: Modeling individual growth trajectories over the first three years of life. J Commun Disord 2014;49:55–68. [DOI] [PubMed] [Google Scholar]
- [57].Woodward LJ, Moor S, Hood KM, et al. Very preterm children show impairments across multiple neurodevelopmental domains by age 4 years. Arch Dis Child Fetal Neonatal 2009;94:339–44. [DOI] [PubMed] [Google Scholar]
- [58].Foster-Cohen SH, Friesen MD, Champion PR, et al. High prevalence/low severity language delay in preschool children born very preterm. J Dev Behav Pediatr 2010;31:658–67. [DOI] [PubMed] [Google Scholar]