

Abstract
Background:
This study aimed to analyze the scientific outputs of diabetic kidney disease (DKD) research and explore its hotspots and frontiers from 2000 to 2017, using bibliometric methods.
Methods:
Articles in DKD research between 2000 and 2017 were retrieved from the Web of Science Core Collection (WoSCC). We used the VOSviewer 1.6.8 and CiteSpace 5.2 to analyze publication years, journals, countries, institutions, authors, references, and keywords. Keywords with citation bursts were used to analyze the research hotspots and emerging trends.
Results:
We identified 27,577 publications in DKD research from 2000 to 2017. The annual publication number increased with time. Nephrology Dialysis Transplantation published the highest number of articles. The United States was the most influential country with most publications and collaborations with other countries. Harvard University was the leading institute. Parving had the most cited publications. Keywords analysis indicated that the renin–angiotensin system inhibition used to be the most prevalent research topic, while recent research hotspots were podocyte, inflammation, and biomarker. The biomarkers for DKD screening, diagnosis, and prognosis could be a research frontier.
Conclusions:
The number of DKD related publications rapidly increased over the past 2 decades. Our study revealed the structure, hotspots, and evolution trends of DKD research. Further studies and more collaborations are needed.
Keywords: bibliometric analysis, CiteSpace, diabetic kidney disease, VOSviewer
1. Introduction
The 21st century has the most diabetogenic environment in human history, with the number of patients with diabetes mellitus (DM) worldwide increasing to 380 million by 2025.[1] Diabetic kidney disease (DKD) is a major complication of DM, approximately 20% to 40% of DM patients develop DKD. DKD is not only one of most common causes of end-stage renal disease (ESRD), but also an independent risk factor for the development of cardiovascular disease (CVD) and mortality, has brought heavy economic burden to the healthcare system all over the world.[2,3]
The research on DKD has increased dramatically in recent years, and many academic journals have published articles in DKD research. Nevertheless, few attempts have been made to analyze the evolution of scientific outputs in this field systematically. Bibliometric analysis has been widely used in various areas to estimate previous research activity, track evolution process and predict emerging trends in specific fields.[4,5] This paper provided an overview of recent studies in DKD using bibliometrics methods through VOSviewer and CiteSpace. Our aims were to obtain the quantitative and visual information in the global scientific outputs of DKD research, identify its hotspots and emerging trends.
2. Materials and methods
The literature data used in this study were downloaded from the Web of Science Core Collection (WoSCC), consisting of the Science Citation Index Expanded, Social Sciences Citation Index, Arts & Humanities Citation Index, Conference Proceedings Citation Index-Science, Conference Proceedings Citation Index-Social Science & Humanities, Book Citation Index-Science, Book Citation Index-Social Sciences &Humanities, Emerging Sources Citation Index, Current Chemical Reactions—Expanded and Index Chemicus. Online retrieval was performed using keywords “diabetic kidney disease” OR “diabetic nephropathy.” The time span was set to between 2000 and 2017. The publication type was not limited. The following information was downloaded for each publication: authors, keywords, institution, and cited references. The data were aggregated as secondary data without personal information, thus informed consent was not required. This study was reviewed by the biomedical research ethics committee of Xuzhou Central Hospital, College of Southeast University; the review board concluded that the utilization of data from published articles did not require oversight by an ethics committee.
VOSviewer is effective in constructing and viewing bibliometric maps, has a powerful function in an easy-to-interpret way of co-citation and co-authorship analysis.[6] CiteSpace is another computer program for information visualization, can visualize emerging trends and abrupt changes in specific fields within a designated period of time.[7] VOSviewer 1.6.8 was used to analyze the country co-authorship, institute co-authorship, journal co-citation, authors co-citation and reference co-citation. CiteSpace 5.2 was used to make the timeline picture for co-citation keywords. GraphPad Prism 7 (San Diego, CA) was used to make histograms and line charts.
3. Results and discussion
From 2000 to 2017, 9 document types were found in 27,596 publications. Excluding the retracted publication (17), early access (1) and retraction (1), there were a total of 27,577 publications left. Among which, most were research articles (74.3%), followed by review article (12.5%), meeting abstract (8.9%), editorial material (2.4%), letter (1.1%), and a book chapter (0.8%).
3.1. The annual trends of publications
A total of 27,577 publications in DKD research were identified from 2000 to 2017. Figure 1 showed the annual number of DKD related publications. The annual number of publications continually increased over time. More and more scholars started to research in this field especially after 2007, which led to a faster growth in the number of publications.
Figure 1.
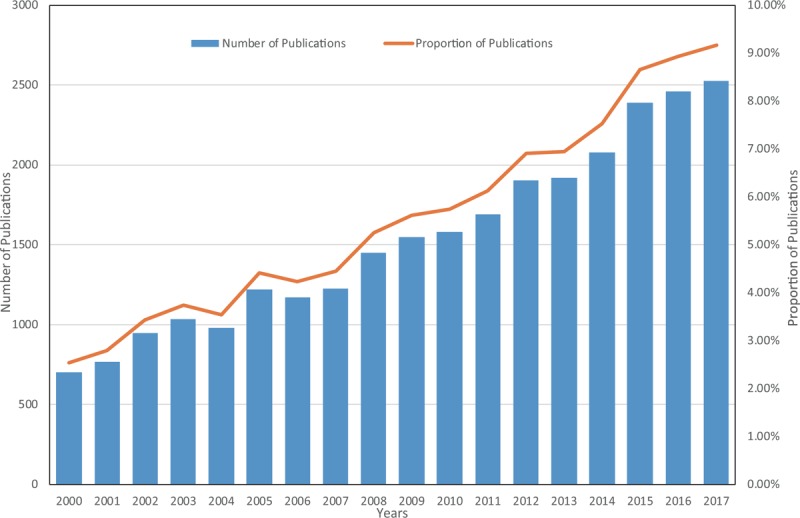
Annual trends in the number of academic DKD related publications from 2000 to 2017. DKD = diabetic kidney disease.
There are several reasons for the rapid growth. First, the prevalence of DM rapidly increased worldwide in decades, mainly due to the changes in dietary and physical activity patterns. For example, the prevalence of DM in Chinese adults was reported to be 0.67% in 1980, then gradually increased to be 10.9% in 2013, and that for prediabetes was 35.7%.[8,9] Second, the DKD research did have new breakthroughs in some fields, such as histopathological diagnosis,[10–13] therapeutic agents,[14–17] and biomarkers for early screening.[2,18–21] Third, with the development of internet technology, massive medical data were easier to be obtained and shared.
3.2. Journal analysis
The 27,577 articles in DKD research were published in more than 2000 academic journals. The 15 most active journals were presented in Table 1. Nephrology Dialysis Transplantation [impact factor (IF) 2017, 4.600] published the highest number of articles (1066 articles, 3.863%), followed by Kidney International (IF 2017, 8.429; 964 articles, 3.493%), Diabetes (IF 2017, 7.273; 857 articles, 3.171%), Journal of the American Society of Nephrology (IF 2017, 8.655; 820 articles, 2.971%) and Diabetologia (IF 2017, 6.023; 781 articles, 2.830%). Compared with other journals, articles in DKD research were more likely to be accepted by these active journals.
Table 1.
Top active 15 journals that published DKD related articles from 2000 to 2017.
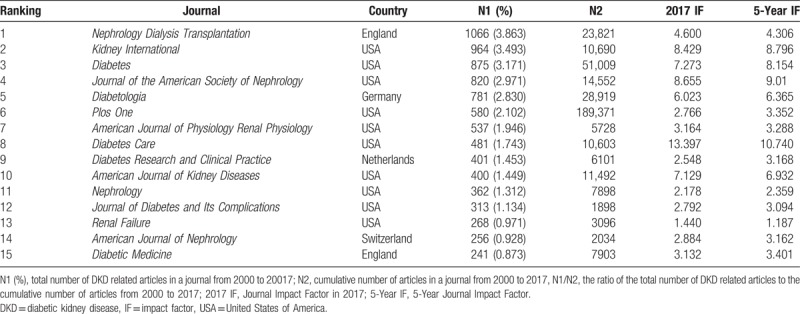
The IF of an academic journal reflects the yearly average number of citations to recent articles published in that journal. It is frequently used as a measure of journal influence within its field. Of the top active 15 journals, 10 journals had an IF > 3.0 with 6566 published articles, which accounted for 23.8% of the total number of DKD related articles. Additionally, 4 of these 10 journals were the top 10 high-IF journals in the field of nephrology. Comparing the rate of high-IF journals to that of all journals (rate of journals with IF > 3.000, 20%; and IF < 3.000, 80%),[22] DKD related articles were relatively published in high-IF journals.
Furthermore, we used VOSviewer to plot the journal co-citation network. Co-citation means that 2 items (e.g., journals, authors, and references) are cited when they are listed in a citing item's reference list. The basic assumption of co-citation analysis is that the more frequently 2 items are co-cited, the more closely they are linked together.[23] Journal co-citation analysis could study overall the structure and characteristics of academic journals network.[24]
Figure 2 showed the journal co-citation network with 300 nodes. The size of nodes represented the activity of journal, which was the number of citations of papers published in this journal. The distance between 2 nodes reflected the link strength between 2 nodes. A shorter distance revealed a stronger relation and a higher citation frequency. The nodes with the same color belonged to a cluster. The clustering technique is a weighted and parameterized variant of modularity-based clustering.[25] Here, the journals were divided into four clusters. The blue cluster contains Nephrology Dialysis Transplantation, Kidney International, Journal of the American Society of Nephrology, American Journal of Kidney Diseases and Transplantation, representing journals in kidney disease and transplantation. The green cluster contains Diabetologia, Diabetes Care, New England Journal of Medicine and Lancet, representing journals in diabetes and general medicine. The yellow cluster contains American Journal of Physiology-Renal Physiology and Hypertension representing journals in hypertension and cardiovascular disease. The red cluster contains PLoS One, Journal of Biological Chemistry, Nature, and Science represents journals in science and technology. Although Diabetes was in the red cluster, it was also located in the center of this map and had connections with the journals in four clusters. Most of the top active 15 journals in Table 1 were also shown in Figure 2, the higher IF, the bigger node, suggesting that publications in higher IF journals had more citations and greater influence in DKD research.
Figure 2.
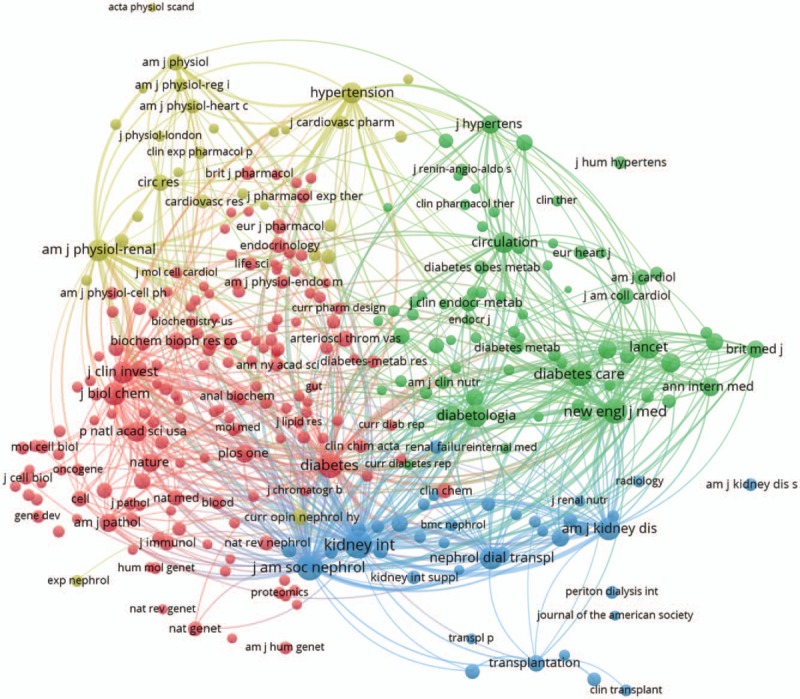
The journal co-citation network of DKD related publications from 2000 to 2017. DKD = diabetic kidney disease.
3.3. Country analysis
The 27,577 articles on DKD research were contributed by 138 countries/territories. The top 10 countries (4 European countries, 3 Asian countries, 2 American countries, and Australia) published 22,430 articles, accounting for 81.3% of the total number of publications (Table 2). The United States of America had the largest number of publications (7100), followed by China (3659), Japan (3206), Germany (1733), and Italy (1486). China was the only developing country in these 10 countries, indicating its great effort and progress in medicine and life sciences during the past 2 decades.
Table 2.
Ranking of countries and institutions that published DKD related articles from 2000 to 2017.

Research projects need collaborative strengths to complete. Co-authorship research is an index to assess the current status of research in a specific field.[26] Country co-authorship analysis reflects the degree of communication between countries as well as the influential countries in this field. The country co-authorship network with 98 nodes was showed in Figure 3. Different colors represented the diversification of research directions. The bigger nodes represented the more influential countries in this field. The links between nodes represented the cooperative relationships among institutes. The distance and thickness of links represented the degree of cooperation among countries. Figure 3 showed that the United States was not only the research center but also closely cooperated with many countries in DKD research, such as Canada, Germany, England, Japan, and China. This map indicated that developed countries in America and Europe had close cooperative relationships, and the geographical advantage was not the primary influencing factor. More cooperation could bring more advanced achievements in scientific research.
Figure 3.

The country co-authorship network of DKD related publications from 2000 to 2017. DKD = diabetic kidney disease.
3.4. Institution analysis
More than 1000 institutions contributed to the publications on DKD research. The top 10 institutions (3 institutions in the United States, 3 in Australia, 1 in Denmark, Canada, Netherlands, and Finland) published 3082 articles, accounting for 11.2% of the total number of publications. Harvard University ranked first place, followed by Steno Diabetes Center and University of Melbourne (Table 2).
Institution co-authorship analysis reflects the degree of communication between institutions as well as the influential institutions in this field.[26] Here, we ranked institutions by a number of citations of their published articles. Figure 4 showed the institute co-authorship network with 100 nodes (top 100 influential institutions). The Harvard University from the United States, the Steno Diabetes Center from Denmark, and the University of Pennsylvania from the USA were the top 3 influential institutes with the largest number of citations in DKD related publications. The rank of an institution in a number of published articles could be different from the number of citations. For example, the number of publications in DKD research from the University of Helsinki ranked ninth, while the total of citations of these articles only ranked 34th. Although China contributed a large number of publications and ranked in the second place in countries (Table 2), only 1 institution could be found in the top 100 nodes, that was the Chinese University of Hong Kong, which ranked 33rd. These results suggested that the quality of some academic articles should be improved.
Figure 4.
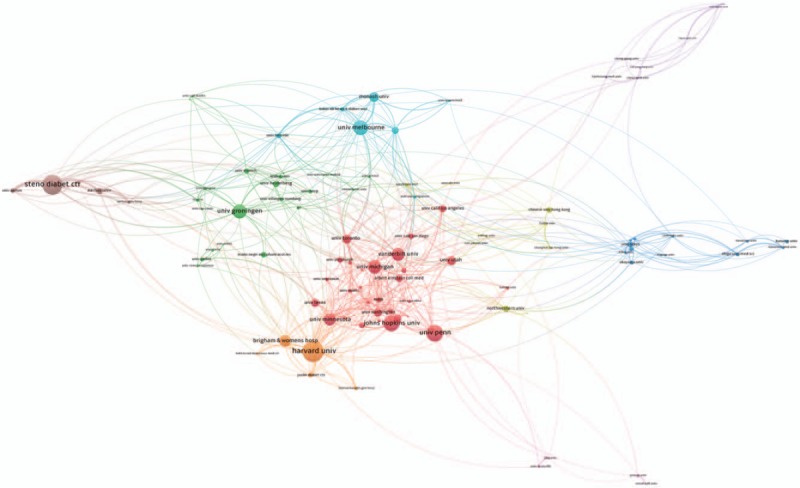
The institution co-authorship network of DKD related publications from 2000 to 2017. DKD = diabetic kidney disease.
3.5. Author and reference co-citation analyses
These 27,577 articles were drafted by more than 20,000 authors. These authors were ranked by a number of citations of their published articles. The top 500 authors were presented in the co-citation cited author network (Fig. 5). The largest node was Parving et al[27,28] (3945 citations), indicating that his important role in DKD research. Parving et al[29] had reported the renal and cardiovascular protective effects of blockade of the renin–angiotensin–aldosterone system in DM patients, such as the New England Journal of Medicine and Kidney International. There were 5 clusters with different colors, authors in the same cluster usually suggested that they studied in a similar field and had close cooperation with each other.
Figure 5.
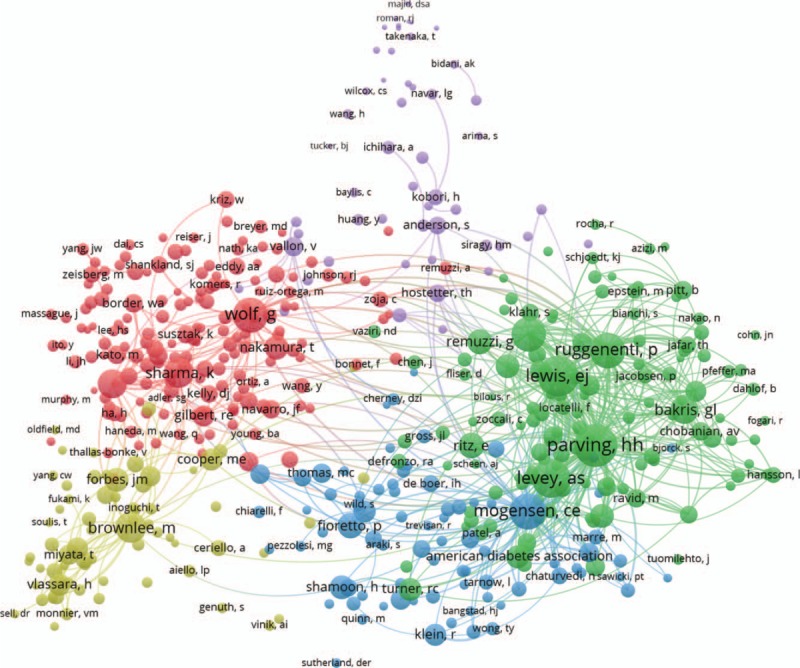
The co-citation cited author network of DKD related publications from 2000 to 2017. DKD = diabetic kidney disease.
When 2 papers are cited simultaneously in a third paper, it is considered that these 2 papers establish a co-citation relationship.[23] Here, references were ranked by the number of their citations, then we constructed a co-cited reference map with 500 nodes (top 500 cited references) and 81,450 links (Fig. 6). In the reference co-citation network, the size of the nodes not only revealed the number of its citations but also illustrated their association with DKD research. For example, in Figure 6, the biggest node was the article by Brenner et al[30] BM, titled “Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy,” which was published in New England Journal of Medicine 2001. This paper was cited 1850 times altogether in these 27,577 DKD related publications and was cited more than 4200 times in the WoSCC. Parving, the author with most citations of publications in DKD research (Fig. 5), was also one of the co-authors of this article.
Figure 6.

The reference co-citation network of DKD related publications from 2000 to 2017. DKD = diabetic kidney disease.
3.6. Emerging trends and research frontiers of DKD
The topics involved in DKD research can be delineated in the keywords assigned to each article. Keywords provide a reasonable description of research hotspots, thus burst keywords represent research frontiers and predict emerging trends.[4,7] Here, CiteSpace 5.2 was used to capture the keywords with the strongest citation bursts that identified as research frontiers during 2000 to 2017. The time intervals were plotted on the green lines, while the periods of burst keywords were highlighted in red, indicating the beginning and end of the time interval of each burst.[31] The top 25 research frontiers of DKD research were listed in Figure 7.
Figure 7.

The keywords with the strongest citation bursts of DKD related publications from 2000 to 2017. DKD = diabetic kidney disease.
From 2000 to 2008, the keywords “renin–angiotensin system (RAS) inhibition” and “Angiotensin II” suggested that RAS inhibitors [e.g., angiotension converting enzyme inhibitor (ACEI) and angiotensin receptor blocker (ARB)] were the research hotspots in patients with DM and DKD. Hypertension is a part of the natural history of DKD and could accelerate its progression. Long-term blood pressure control is associated with a reduction in the incidence of DKD in DM patients with hypertension.[32] The renoprotective effects of ACEI or ARB have been confirmed in DKD patients, and RAS inhibitors have been recommended to titrate up to the maximum approved dose in the absence of side effects or adverse events.[15] The keywords “extracellular matrix,” “protein kinase C,” “transforming growth factor-beta” and “messenger RNA” reflected the main research areas in pathology and etiology of DKD. During this period, chronic complications of DM, such as “diabetic nephropathy” and “retinopathy” were the most concerned topics. Since 2003, the term “diabetic nephropathy” was gradually replaced by the term “diabetic kidney disease.”
From 2008 to 2015, the “microvascular complication” of DM and the association between DKD and “metabolic syndrome” became the research hotspots. The investigators started to use “urinary albumin excretion” to evaluate the degree of proteinuria in DKD patients. The study of cardiovascular diseases (CVDs) and vascular function in DKD patients gradually attracted attention with burst keywords “blood pressure,” “atherosclerosis,” “glycation end product,” “nitric oxide” and “smooth muscle cell.” DKD is one of the most common microvascular complications of DM, and also predominantly account for the increased risk of CVDs in DM patients.[33] Since CVDs are the leading causes of morbidity and mortality in DM patients, multiple risk factor control for CVDs has been discussed widely. For example, the classical CVD risk factors include hyperglycemia, hypertension, dyslipidemia, smoking, as well as overweight or obese,[34] therefore, Hamada and Gulliford[35] reported that multiple risk factor control, consisting of four components: HbA1c <53 mmol/mol (<7.0%), BP <140/90 mm Hg, total cholesterol <5 mmol/L and no smoking, which could achieve lower relative hazards for CVDs and its related mortality in DKD patients. More studies on the management of complications of DKD and CVDs are still needed.
In recent years, research hotspots in pathology and etiology of DKD switched to “podocyte,” “apoptosis,” “fibrosis,” “inflammation,” and “nuclear factor kappa B.” With new technologies developing, identifying novel “biomarker” for DKD screening, diagnosis and prognosis had made great progress, such as the genome sequencing, epigenetics, and omics technologies.[2,18,19] For example, the CKD273 classifier, based on 273 urinary peptides, was well suited for early detection of DKD in patients with type 2 DM, who had no sign of DKD with normal estimated glomerular filtration rate (eGFR) and normo-albuminuria.[20,21] Some other biomarkers, such as α1-microglobulin (α1-MG), β2-microglobulin (β2-MG), inflammatory markers (e.g., C-reactive protein, interleukin-6, and tumor necrosis factor-α), as well as several angiogenic and anti-angiogenic factors (e.g., vascular endothelial growth factor (VEGF), VEGF receptors, angiopoietins and endostatin) were reported to play important roles in early detection, therapeutic prevention and implementation of DKD.[36–38] Plasma tumor necrosis factor receptor-1 (TNFR-1), TNFR-2, and kidney injury molecule-1 (KIM-1) were independently associated with higher risk of eGFR decline in patients with early or advanced DKD.[39,40] The research in “biomarker” should still be a direction in the future. Personalized screening and intervention will be provided to DKD patients, according to the individual clinical phenotypes, such as “omics”-based biomarkers, the rate of progression, the degree of comorbidities, and response to interventions.
There are limitations in our study. These results are based on statistical analysis of academic publications in the WoSCC, which is a large and comprehensive database with a collection of high-quality literature, but it does not index all scientific journals, therefore, some articles in DKD could be missed. The WoSCC might also bring some bias by over-representing journals in English.
4. Conclusions
This study investigated the global scientific outputs of DKD research, analyzed its structure, hotspots, and evolution trends from 2000 to 2017. During this period, the number of DKD related publications increased. Nephrology Dialysis Transplantation published the highest number of articles on DKD research, followed by Kidney International, Diabetes and Journal of the American Society of Nephrology. The United States was the most influential country, not only contributed the highest number of articles but also closely cooperated with many other countries. The Harvard University from the United States was the most influential institution with the largest number of publications and citations. Parving had the most cited publications. RAS inhibition used to be the most prevalent research topic, while recent research hotspots were podocyte, inflammation, and biomarker.
Overall, our findings could be important supplements to the traditional research and provide valuable information to identify new perspectives and shape future research directions. DKD is still a research hotspot, and biomarker for DKD screening, diagnosis and prognosis could be a research frontier in the future. Further studies and more collaborations are needed in DKD study worldwide.
Author contributions
Conceptualization: Lu-Xi Zou, Ling Sun.
Data curation: Lu-Xi Zou, Ling Sun.
Formal analysis: Lu-Xi Zou, Ling Sun.
Funding acquisition: Ling Sun.
Investigation: Lu-Xi Zou, Ling Sun.
Methodology: Lu-Xi Zou, Ling Sun.
Project administration: Lu-Xi Zou, Ling Sun.
Resources: Lu-Xi Zou, Ling Sun.
Software: Lu-Xi Zou, Ling Sun.
Supervision: Ling Sun.
Validation: Ling Sun.
Visualization: Ling Sun.
Writing – original draft: Lu-Xi Zou, Ling Sun.
Writing – review & editing: Ling Sun.
Ling Sun orcid: 0000-0002-5276-1309.
Footnotes
Abbreviations: ACEI = angiotension converting enzyme inhibitor, ARB = angiotensin receptor blocker, CVD = cardiovascular disease, DKD = diabetic kidney disease, DM = diabetes mellitus, ESRD = end-stage renal disease, IF = impact factor, RAS = renin–angiotensin system, USA = United States of America, WoSCC = Web of Science Core Collection.
LXZ and LS contributed equally to this work.
This study was supported by the National Natural Science Foundation of China (grant number 81600540); Natural Science Foundation of Jiangsu Province (grant number BK20150224); Science and Technology Foundation of Xuzhou City (grant number KC16SL119), Jiangsu Entrepreneurial Innovation Program, Jiangsu Six Talent Peaks Project, Jiangsu Health International (regional) exchange support program, and Xuzhou Entrepreneurial Innovation Program.
The authors have no conflicts of interest to disclose.
References
- [1].Atkins RC, Zimmet PZ. Int Soc N, Int Fed Kidney Fdn World Kidney D, Int Diabet F. Diabetic kidney disease: act now or pay later. Med J Aust 2010;192:272–4. [DOI] [PubMed] [Google Scholar]
- [2].Persson F, Rossing P. Diagnosis of diabetic kidney disease: state of the art and future perspective. Kidney Int Suppl 2018;8:2–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Rocha NA, McCullough PA. Cardiovascular outcomes in diabetic kidney disease: insights from recent clinical trials. Kidney Int Suppl 2018;8:8–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Zhou H, Tan W, Qiu Z, et al. A bibliometric analysis in gene research of myocardial infarction from 2001 to 2015. Peer J 2018;6:e4354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Liao HC, Tang M, Luo L, et al. A bibliometric analysis and visualization of medical big data research. Sustainability 2018;10:166. [Google Scholar]
- [6].van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010;84:523–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Chen CM. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol 2006;57:359–77. [Google Scholar]
- [8].Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in china in 2013. JAMA 2017;317:2515–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Li MZ, Su L, Liang BY, et al. Trends in prevalence, awareness, treatment, and control of diabetes mellitus in mainland china from 1979 to 2012. Int J Endocrinol 2013;2013:753150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Mogensen CE, Christensen CK, Vittinghus E. The stages in diabetic renal disease. With emphasis on the stage of incipient diabetic nephropathy. Diabetes 1983;32suppl 2:64–78. [DOI] [PubMed] [Google Scholar]
- [11].Bermejo S, Pascual J, Soler MJ. The current role of renal biopsy in diabetic patients. Minerva Med 2018;109:116–25. [DOI] [PubMed] [Google Scholar]
- [12].Hoshino J, Mise K, Ueno T, et al. A pathological scoring system to predict renal outcome in diabetic nephropathy. Am J Nephrol 2015;41:337–44. [DOI] [PubMed] [Google Scholar]
- [13].Hoshino J, Furuichi K, Yamanouchi M, et al. A new pathological scoring system by the Japanese classification to predict renal outcome in diabetic nephropathy. PLoS One 2018;13:e0190923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Cherney DZI, Bakris GL. Novel therapies for diabetic kidney disease. Kidney Int Suppl 2018;8:18–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Anders HJ, Davis JM, Thurau K. Nephron protection in diabetic kidney disease. N Engl J Med 2016;375:2096–8. [DOI] [PubMed] [Google Scholar]
- [16].Agrawal V, Giri C, Solomon RJ. The effects of glucose-lowering therapies on diabetic kidney disease. Curr Diabetes Rev 2015;11:191–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Dekkers CCJ, Gansevoort RT, Heerspink HJL. New diabetes therapies and diabetic kidney disease progression: the role of SGLT-2 inhibitors. Curr Diab Rep 2018;18:27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Sun L, Zou LX, Chen MJ. Make precision medicine work for chronic kidney disease. Med Princ Pract 2017;26:101–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Iyengar SK, Sedor JR, Freedman BI, et al. Genome-wide association and trans-ethnic meta-analysis for advanced diabetic kidney disease: family investigation of nephropathy and diabetes (FIND). PLoS Genet 2015;11:e1005352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Argiles A, Siwy J, Duranton F, et al. CKD273, a new proteomics classifier assessing CKD and its prognosis. PLoS One 2013;8:e62837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Siwy J, Schanstra JP, Argiles A, et al. Multicentre prospective validation of a urinary peptidome-based classifier for the diagnosis of type 2 diabetic nephropathy. Nephrol Dial Transplant 2014;29:1563–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Yin ZY, Chen DY, Li BF. Global regulatory T-cell research from 2000 to 2015: a bibliometric analysis. PLoS One 2016;11:e0162099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Boyack KW, Klavans R. Co-citation analysis, bibliographic coupling, and direct citation: which citation approach represents the research front most accurately? J Am Soc Inf Sci Technol 2010;61:2389–404. [Google Scholar]
- [24].Hu CP, Hu JM, Gao Y, et al. A journal co-citation analysis of library and information science in China. Scientometrics 2011;86:657–70. [Google Scholar]
- [25].Waltman L, van Eck NJ, Noyons ECM. A unified approach to mapping and clustering of bibliometric networks. J Informetr 2010;4:629–35. [Google Scholar]
- [26].Reyes-Gonzalez L, Gonzalez-Brambila CN, Veloso F. Using co-authorship and citation analysis to identify research groups: a new way to assess performance. Scientometrics 2016;108:1171–91. [Google Scholar]
- [27].Parving HH, Lehnert H, Brochner-Mortensen J, et al. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med 2001;345:870–8. [DOI] [PubMed] [Google Scholar]
- [28].Parving HH, Persson F, Lewis JB, et al. Aliskiren combined with losartan in type 2 diabetes and nephropathy. N Engl J Med 2008;358:2433–46. [DOI] [PubMed] [Google Scholar]
- [29].Parving HH, Lewis JB, Ravid M, et al. Prevalence and risk factors for microalbuminuria in a referred cohort of type II diabetic patients: a global perspective. Kidney Int 2006;69:2057–63. [DOI] [PubMed] [Google Scholar]
- [30].Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001;345:861–9. [DOI] [PubMed] [Google Scholar]
- [31].Miao Y, Xu SY, Chen LS, et al. Trends of long noncoding RNA research from 2007 to 2016: a bibliometric analysis. Oncotarget 2017;8:83114–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].De Cosmo S, Viazzi F, Piscitelli P, et al. Blood pressure status and the incidence of diabetic kidney disease in patients with hypertension and type 2 diabetes. J Hypertens 2016;34:2090–8. [DOI] [PubMed] [Google Scholar]
- [33].Nikolsky E, Mehran R, Turcot D, et al. Impact of chronic kidney disease on prognosis of patients with diabetes mellitus treated with percutaneous coronary intervention. Am J Cardiol 2004;94:300–5. [DOI] [PubMed] [Google Scholar]
- [34].Yang ZJ, Liu J, Ge JP, et al. Prevalence of cardiovascular disease risk factor in the Chinese population: the 2007–2008 China National Diabetes and Metabolic Disorders Study. Eur Heart J 2012;33:213–20. [DOI] [PubMed] [Google Scholar]
- [35].Hamada S, Gulliford MC. Multiple risk factor control, mortality and cardiovascular events in type 2 diabetes and chronic kidney disease: a population-based cohort study. BMJ Open 2018;8:e019950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Winter L, Wong LA, Jerums G, et al. Use of readily accessible inflammatory markers to predict diabetic kidney disease. Front Endocrinol (Lausanne) 2018;9:225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Futrakul N, Futrakul P. Biomarker for early renal microvascular and diabetic kidney diseases. Ren Fail 2017;39:505–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Jiang X, Zhang Q, Wang HB, et al. Associations of urinary, glomerular, and tubular markers with the development of diabetic kidney disease in type 2 diabetes patients. J Clin Lab Anal 2018;32:e22191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Barr ELM, Barzi F, Hughes JT, et al. High baseline levels of tumor necrosis factor receptor 1 are associated with progression of kidney disease in indigenous australians with diabetes: the eGFR follow-up study. Diabetes Care 2018;41:739–47. [DOI] [PubMed] [Google Scholar]
- [40].Coca SG, Nadkarni GN, Huang Y, et al. Plasma biomarkers and kidney function decline in early and established diabetic kidney disease. J Am Soc Nephrol 2017;28:2786–93. [DOI] [PMC free article] [PubMed] [Google Scholar]