

Abstract
There are few studies on the correlation between red blood cell distribution width (RDW) and cardiovascular events in the patients receiving peritoneal dialysis (PD). We explored the correlation between RDW and cardiovascular events in PD patients and possible mechanism.
A total of 138 PD patients were divided into RDW < 15% group (n = 104) and RDW ≥ 15% group (n = 34).
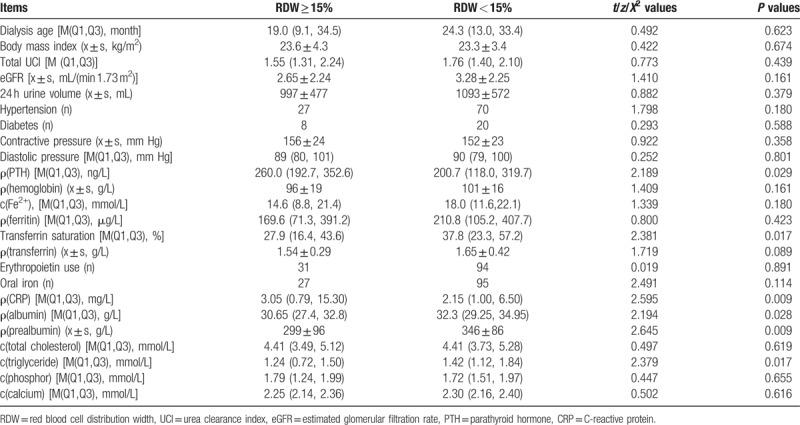
The levels of serum C-reactive protein (CRP) [3.05 (0.79, 15.30) mg/L vs 2.15 (1.00, 6.50) mg/L] and parathyroid hormone (PTH) [260.0 (192.7, 352.6) ng/L vs 200.7 (118.0, 319.7) ng/L] were significantly higher, but the levels of serum albumin [30.65 (27.4,32.8) g/L vs 32.3 (29.25,34.95) g/L], prealbumin [(299 ± 96) g/L vs (346 ± 86) g/L], triglyceride [1.24 (0.72, 1.50) mmol/L vs 1.42 (1.12,1.84) mmol/L], and transferrin saturation [27.9 (16.4, 43.6)% vs 37.8 (23.3, 57.2)%] were significantly lower in the RDW ≥ 15% group than in the RDW < 15% group (all P < 0.05). The RDW was negatively correlated with albumin (r = − 0.258, P = 0.002), prealbumin (r = −0.236, P = 0.005), and triglyceride (r = −0.194, P = 0.023), but was positively correlated with CRP level (r = 0.174, P = 0.041). The incidence of cardiovascular events was significantly higher in the RDW ≥ 15% group (6 patients, 17.6%) than in the RDW < 15% group (6.7%) (7 patients, P < 0.01). Cox proportional hazard model showed that elevated RDW level was an independent risk factor for cardiovascular events in PD patients (HR = 1.622, 95% CI: 1.063–2.475, P = 0.025).
The elevated RDW may be served as a risk factor to predict the cardiovascular events in PD patients.
Keywords: Cardiovascular events, peritoneal dialysis, red blood cell distribution width
1. Introduction
Red blood cell distribution width (RDW), a parameter associated with the heterogeneity of red blood cell volume,[1] is often used for the differential diagnosis of anemia together with mean corpuscular volume (MCV). Cardiovascular diseases (CVD) are a major complication of peritoneal dialysis (PD) in the patients with end-stage renal disease (ESRD).[2] Prevention as well as early diagnosis and treatment of CVD are very important for the patients receiving PD. Elevated RDW may be an independent predictive factor for the severity of coronary artery disease,[3,4] and for the death caused by septic shock,[5] pulmonary hypertension[6] or pulmonary embolism.[7] There are few studies on the correlation between RDW and cardiovascular events in the patients receiving PD. In this study, we explored the correlation between the elevated RDW and the occurrence of cardiovascular events in the patients receiving PD and possible mechanism.
2. Subjects and methods
All study methods were approved by the Ethics Committee of Henan Provincial Peoples Hospital. All the subjects enrolled into the study gave written informed consent to participate.
2.1. Subjects
A total of 138 patients receiving maintenance PD by catheterization and regular follow-up between July 2012 and June 2016 were enrolled in this study. Of the 138 patients, 98 were male and 40 female, with a mean age of (46.9 ± 16.2) years. All these patients received continuous ambulant PD with dialysate solutions of 6000 to 10,000 mL/day. The inclusion criteria were that (1) the patients were 18 years old or over when they received PD; (2) the patients received PD catheterization in the Department of Nephrology, Henan Provincial People's Hospital and (3) the maintenance PD lasted 3 months or more. The exclusion criteria were that (1) the patients were younger than 18 years old when they received PD; (2) the patients received PD catheterization in other PD centers; (3) the patients had malignant tumor and/or hematological diseases; (4) the patients received PD due to the failures in hemodialysis and/or renal transplantation; (5) PD lasted less than 3 months; and (6) the patients had no data of RDW. According to the toplimit of normal range of RDW, the 138 patients were divided into RDW < 15% group (n = 104) and RDW≥15% group (n = 34). In the RDW < 15% group, 73 patients were male and 31 female, with a mean age of (46.13 ± 16.44) years. In the RDW ≥ 15% group, 25 patients were male and 9 female, with a mean age of (49.1 ± 15.4) years. There were no statistical differences in sex and age between the two groups (all P > 0.05).
2.2. Collection of general data
General data of patients were collected when they received PD for one month, including age, sex, body mass index, blood pressure, past medical history, and proportions of erythropoietin use and oral iron supplementation.
2.3. Dialysis-related data and laboratory data
Dialysis-related data and laboratory data were collected when they received PD for one month. Dialysis-related data included 24 h urine volume, estimated glomerular filtration rate (eGFR), and total urea clearance index. Laboratory data included hemoglobin, RDW, serum iron, ferritin, transferrin, transferrin saturation, serum C-reactive protein (CRP), serum albumin, prealbumin, serum creatinine, urea nitrogen, parathyroid hormone (PTH), total cholesterol, triglyceride, and electrolytes.
2.4. The predefined end point of this study and follow-up
The predefined end point of this study was cardiovascular events including acute heart failure, angina pectoris, acute myocardial infarction, arrhythmia requiring drug intervention, cerebral infarction or cerebral hemorrhage, and cardiac sudden death. Follow-up was from July 1, 2012 to the occurrences of endpoint events or death. For the patients who had no any endpoint event and survived, the follow-up was from July 1, 2012 to June 30, 2016. For the patients whose PD was changed into hemodialysis and/or renal transplantation during the follow-up, the follow-up's deadline was the last PD. The time and name of the cardiovascular events as well as the cause of death were recorded during the follow-up. In the patients with repeated cardiovascular events, the first event was used in survival analysis.
2.5. Research methods
The general data, dialysis-related data, laboratory data, and the incidence of cardiovascular events were compared between the two groups. The correlation between RDW and each item was analyzed. The influence of RDW on the occurrence of cardiovascular events was observed.
2.6. Statistical analysis
Statistical analysis was performed using SPSS 18.0 software. Measurement data were tested by normality and homogeneity of variance. The measurement data with normal distribution were expressed as (x ± s), and were compared between the two groups using t test. The measurement data with non-normal distribution were expressed as median (quartile) [M(Q1, Q3)], and were compared between the two groups using Wilcoxon rank sum test. Chi-square test was used in the comparison of count data. The correlation between RDW and each item was analyzed using Pearson bivariate correlation analysis or Spearman bivariate rank correlation analysis. The incidence of cardiovascular events was analyzed by Kaplan–Meier method, and was compared between the two groups using Log-Rank test. Cox proportional risk regression model was used to analyze the influence of RDW on cardiovascular events. Statistical significance was established at P < 0.05.
3. Results
3.1. Comparison of general data
There were no significant differences in body mass index, dialysis age, 24 h urine volume, total urea clearance index, eGFR, blood pressure, proportion of diabetes history, proportion of hypertension history, and drug use rate for treatment of anemia between the two groups (all P > 0.05). The levels of CRP and PTH were significantly higher, but the levels of serum albumin, prealbumin, triglyceride, and transferrin saturation were significantly lower in the RDW ≥ 15% group than in the RDW < 15% group (all P < 0.05) (Table 1).
Table 1.
Comparisons of general data, dialysis-related data, and laboratory data between the two groups.
3.2. Correlation between RDW and each item
The RDW was positively correlated with CRP level (r = 0.174, P = 0.041), but was negatively correlated with albumin (r = −0.258, P = 0.002), prealbumin (r = −0.236, P = 0.005), and triglyceride (r= - 0.194, P=0.023).
3.3. Comparison of the incidence of cardiovascular events between the two groups
During the follow-up period, the treatment was changed from PD into hemodialysis or renal transplantation in 7 patients (5%) and 3 patients (2%), respectively; 3 patients (2%) lost their follow-up visits; one patient (0.7%) died of severe infection; and 13 patients (9.4%) had cardiovascular events. In the 13 patients with cardiovascular events, 7 had heart failure, 2 acute coronary syndrome, 3 acute stroke, and one sudden cardiac death. Of the 13 patients with cardiovascular events, 6 (17.6%) were from the RDW ≥ 15% group and 7 (6.7%) from the RDW < 15% group. The Kaplan–Meier curve showed that the incidence of cardiovascular events was significantly higher in the RDW ≥ 15% group than in the RDW < 15% group (X2 = 7.267, P = 0.007) (Fig. 1).
Figure 1.
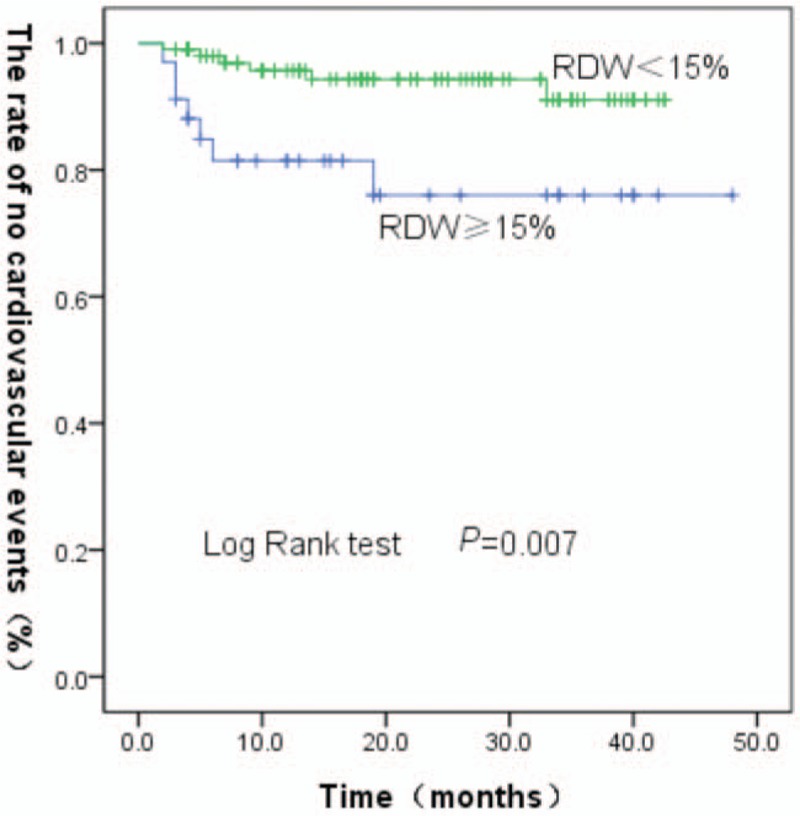
Kaplan–Meier curve showing RDW and cardiovascular events. RDW = red blood cell distribution width.
3.4. COX analysis of cardiovascular events and RDW in the patients receiving PD
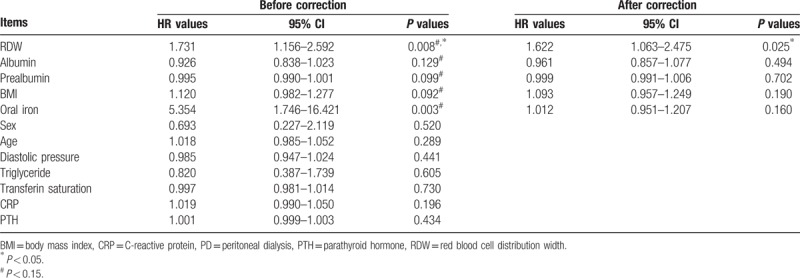
The items including RDW, age, sex, BMI, albumin, prealbumin, triglyceride, CRP, transferin saturation, PTH, oral iron, and contractive pressure were first underwent univariate analysis. The univariate analysis indicated that increased RDW was a risk factor for cardiovascular events in the patients receiving PD (HR = 1.731, 95% CI: 1.156–2.592, P = 0.008). The items with P < 0.15 indicated by COX univariate analysis including BMI, albumin, prealbumin, oral iron, and RDW underwent multivariate COX analysis. The multivariate analysis also indicated that the increased RDW was a risk factor for cardiovascular events in the patients receiving PD (HR = 1.622, 95% CI: 1.063–2.475, P = 0.025) (Table 2).
Table 2.
Risk analysis for cardiovascular events in the patients receiving PD.
4. Discussion
PD technique is a main replacement therapy for the patients with ESRD. PD has many advantages such as simple equipment, convenient operation, small chance of cross-infection, safety and effectiveness, little interference with hemodynamics, and better protective effect on residual renal function, so it has been gradually accepted by more and more patients with ESRD and has become the treatment of the top choice in the renal replacement therapy.[8] The common complications occurring in the patients receiving PD include cardiovascular diseases, infection, and malnutrition; and the cardiovascular diseases are the main cause of death.[9] Timely correction of the cardiovascular disease-related risk factors is conductive to improving the prognosis of PD patients.
In the RDW ≥ 15% group of this study, the incidence of cardiovascular events was 16.7%. It has been reported that in the hemodialysis patients with elevated RDW, the incidence of cardiovascular events was 48%.[10] This may be that PD has better cardiovascular protection than hemodialysis in the patients with ESRD. In this study, the Kaplan–Meier curve showed that the incidence of cardiovascular events was significantly higher in the RDW ≥ 15% group than in the RDW < 15% group, and multivariate COX analysis indicated that the increased RDW was a risk factor of cardiovascular events after corrections of BMI, albumin, prealbumin, and oral iron.
RDW is associated with the extent of anisocytosis. Some conditions including ineffective erythropoiesis (such as iron deficiency, folic acid deficiency, vitamin B12 deficiency, hemoglobin disease, etc.), increased erythrocyte destruction, and blood transfusion all can cause elevated RDW. The mechanism that elevated RDW raises the incidence of cardiovascular events has been unclear. This study indicated that RDW was positively correlated with CRP, and CRP level was significantly higher in the RDW ≥ 15% group than in the RDW < 15% group. These suggest that the elevated RDW affecting the occurrence of cardiovascular events may be caused by inflammation in the patients receiving PD. In the patients receiving PD, micro-inflammation condition is common, and these elevated inflammatory factors such as tumor necrosis factor-α, interleukin-1, and interleukin-6 inhibit erythropoietin production, leading to erythrocyte heterogeneity and elevated RDW.[11,12] Förhécz et al[13] have reported that RDW is closely related to malnutrition because the deficiencies of erythropoiesis-related substances such as folic acid, vitamin B12, and serum iron can cause varying degrees of anemia, leading to elevated RDW. Our results displayed that the elevated RDW was negatively correlated with the levels of albumin and prealbumin (all P < 0.05), the levels of albumin and prealbumin were significantly lower in the RDW ≥ 15% group than in the RDW < 15% group. Our results suggest that malnutrition may be associated with the risk of cardiovascular events in the patients receiving PD. Zhang Yan et al[14] found that PTH was closely associated with left ventricular hypertrophy in the patients receiving PD. Our results showed that PTH level was significantly higher in the RDW ≥ 15% group than in the RDW < 15% group, suggesting that PTH was involved in the occurrence and development of cardiovascular disease in the patients receiving PD. Therefore, controlling inflammation, improving nutritional status, and regulating parathyroid function will be conducive to reduction of cardiovascular events in the patients receiving PD.
In summary, elevated RDW may be served as an independent risk factor for cardiovascular events and can be used to predict the cardiovascular events in PD patients. It is important for improving patients’ survival rate to prevent the occurrence of cardiovascular events according to RDW combined with other clinical data.
Acknowledgment
None.
Author contributions
Conceptualization: Feng-min Shao.
Data curation: Xin-di Zhao, Lei Yan.
Formal analysis: Xiao-guang Fan.
Writing – original draft: Hui-xia Cao.
Footnotes
Abbreviations: CRP = C-reactive protein, CVD = cardiovascular diseases, eGFR = estimated glomerular filtration rate, ESRD = end-stage renal disease, MCV = mean corpuscular volume, PD = peritoneal dialysis, RDW = red blood cell distribution width, RTH = parathyroid hormone.
Funding: None.
Conflict of interest: Nothing to disclose.
References
- [1].Ephrem G, Kanei Y. Elevated red blood cell distribution width is associated with higher recourse to coronary artery bypass graft. Cardiology 2012;123:135–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Zeng J-y, Li H, Luo Z-m, et al. Correlation between red blood cell distribution width and cardiovascular-related mortality in maintenance dialysis patients. J New Med 2015;46:728–31. [Google Scholar]
- [3].Tao B, Jian X-j, Fang Z, et al. Changes of red blood cell distribution width in patients with acute myocardial infarction and its significance. J Chin Pract Diagnosis Therapy 2016;30:666–8. [Google Scholar]
- [4].Zhang D, Wang H-y, Qu P. Relation of RDW with the severity of coronary artery disease and long-term prognosis in ACS. J Clin Cardiol 2015;31:37–41. [Google Scholar]
- [5].Balta S, Demirkol S, Hatipoglu M, et al. Red cell distribution width is a predictor of mortality in patients with severe sepsis and septic shock. Am J Emerg Med 2013;31:989–90. [DOI] [PubMed] [Google Scholar]
- [6].Hampole CV, Mehrotra AK, Thenappan T, et al. Usefulness of red cell distribution width as a prognostic marker in pulmonary hypertension. Am J Cardiol 2009;104:868–72. [DOI] [PubMed] [Google Scholar]
- [7].Zorlu A, Bektasoglu G, Guven FM, et al. Usefulness of admission red cell distribution width as a predictor of early mortality in patients with acute pulmonary embolism. Am J Cardiol 2012;109:128–34. [DOI] [PubMed] [Google Scholar]
- [8].Yu X-k, Zhang L, Bi C-s. Effects of peritoneal dialysis on chronic renal failure with liver cirrhosis and ascites. Chin J Gen Pract 2012;10:1223–4. [Google Scholar]
- [9].Dong J, Wang T, Han Q-f, et al. Impact of nutritional status, inflammation and cardiovascular disease on the mortality of 90 Chinese peritoneal dialysis patients. J Peking Univ (Health Sci) 2003;35:5–9. [PubMed] [Google Scholar]
- [10].Mo L-y, Li Z-l, Xu L-x, et al. Higher red blood cell distribution width is the independent risk factor for cardiovascular mortality in hemodialysis patients. Chin J Blood Purific 2016;15:5–9. [Google Scholar]
- [11].Monteiro CM, Pinheiro LF, Izar MC, et al. Highly sensitive C-reactive protein and male gender are independently related to the severity of coronary disease in patients with metabolic syndrome and an acute coronary event. Braz J Med Biol Res 2010;43:297–302. [DOI] [PubMed] [Google Scholar]
- [12].Ma FL, Li S, Li XL, et al. Correlation of red cell distribution width with the severity of coronary artery disease: a large Chinese cohort study from a single center. Chin Med J (Engl) 2013;126:1053–7. [PubMed] [Google Scholar]
- [13].Förhécz Z, Gombos T, Borgulya G, et al. Red cell distribution width in heart failure: prediction of clinical events and relationship with markers of ineffective erythropoiesis, inflammation, renal function, and nutritional state. Am Heart J 2009;158:659–66. [DOI] [PubMed] [Google Scholar]
- [14].Zhang Y, Zhao X, Renazuoli N, et al. Relationship of the level of intact parathyroid hormone and cytokines with left ventricular hypertrophy in continuous ambulatory peritoneal dialysis patients. J Chin Pract Diagnosis Therapy 2016;30:805–7. [Google Scholar]