

ABSTRACT
Background: Despite numerous calls for a more evidence-based provision of post-disaster psychosocial support, systematic analyses of post-disaster service delivery are scarce.
Objective: The aim of this review was to evaluate the organization of post-disaster psychosocial support in different disaster settings and to identify determinants.
Methods: We conducted a meta-synthesis of scientific literature and evaluations of post-disaster psychosocial support after 12 Dutch disasters and major crises between 1992 and 2014. We applied systematic search and snowballing methods and included 80 evaluations, as well as grey and scientific documents.
Results: Many documents focus on the prevalence of mental health problems. Only a few documents primarily assess the organization of post-disaster psychosocial support and its determinants. The material illustrates how, over the course of two decades, the organizational context of post-disaster psychosocial support in the Netherlands has been influenced by changes in legislation, policy frameworks, evidence-based guidelines, and the instalment of formal expertise structures to support national and local governments and public services. Recurring organizational issues in response to events are linked to interrelated evaluation themes such as planning, training, registration, provision of information and social acknowledgement. For each evaluation theme, we identify factors helping or hindering the psychosocial support organization during the preparedness, acute and recovery phases.
Conclusions: The meta-synthesis illustrates that psychosocial service delivery has grown from a monodisciplinary to a multidisciplinary field over time. Suboptimal interprofessional collaboration poses a recurring threat to service quality. Despite the development of the knowledge base, post-disaster psychosocial support in the Netherlands lacks a systematic and critical appraisal of its functioning. Further professionalization is coupled with the strengthening of evaluation and learning routines.
KEYWORDS: Disasters, recovery, psychosocial support, organizational factors, interprofessional collaboration
HIGHLIGHTS
• Little academic and practical attention has been paid to the organization of post-disaster psychosocial support (PSS).
• Awareness of the need for post-disaster PSS, event type, collaboration and (social) media influence the organization of post-disaster PSS.
• Recurring evaluation themes are planning and training, registration, information and social acknowledgement.
• Suboptimal interprofessional collaboration poses a recurring threat to service quality.
Abstract
Antecedentes: A pesar de las numerosas solicitudes de más prestaciones de apoyo psicosocial posterior al desastre basadas en evidencia, los análisis sistemáticos de éstas son escasos.
Objetivo: Evaluar la organización del apoyo psicosocial posterior al desastre en diferentes entornos de desastre e identificar los determinantes.
Métodos: Realizamos una meta-síntesis de la literatura científica y evaluaciones de apoyo psicosocial posterior al desastre después de 12 desastres holandeses y crisis mayores entre 1992 y 2014. Aplicamos métodos de búsqueda sistemática y de ‘bola de nieve’ e incluimos 80 evaluaciones, así como documentos científicos y ‘grises’ (no publicados oficialmente).
Resultados: Muchos documentos se centran en la prevalencia de problemas de salud mental. Sólo unos pocos evalúan primariamente la organización del apoyo psicosocial posterior al desastre y sus determinantes. El material ilustra cómo, en el transcurso de dos décadas, el contexto organizacional del apoyo psicosocial posterior al desastre en los Países Bajos se encuentra influenciado por los cambios en la legislación, los marcos políticos, directrices basadas en la evidencia y la instalación de estructuras formales de expertos para apoyar a gobiernos locales y servicios públicos. Los problemas organizativos recurrentes en respuesta a los eventos están vinculados con aspectos de evaluación interrelacionados, tales como planificación, capacitación, registro, suministro de información y reconocimiento social. Para cada aspecto de evaluación, identificamos los factores que ayudan o dificultan la organización de apoyo psicosocial durante las fases de preparación, aguda y de recuperación.
Discusión: La meta-síntesis ilustra que la prestación de servicios psicosociales ha crecido a lo largo del tiempo de un campo mono-disciplinario a uno multidisciplinario. Las colaboraciones inter-profesionales que no son óptimas representan una amenaza recurrente para la calidad del servicio. A pesar de la base de conocimientos desarrollados, el apoyo psicosocial posterior al desastre en los Países Bajos carece de una evaluación sistemática y crítica de su funcionamiento. La profesionalización avanzada lleva aparejado el fortalecimiento de las rutinas de evaluación y aprendizaje.
PALABRAS CLAVES: Desastres, recuperación, apoyo psicosocial, evaluación, factores organizacionales, colaboración inter-profesional
Abstract
背景:尽管已有多次呼吁更多循证的灾后心理社会支持,但关于灾后服务的系统分析仍然很少。
目标:评估不同灾害环境中灾后心理社会支持的组织情况,并识别其决定因素。
方法:我们对1992年-2014年间发生的12次荷兰灾难和重大危机之后的科学文献和灾后心理社会支持进行了综合分析。我们采用了系统搜索和滚雪球方法,最后纳入了80项评估以及灰色和科学文献。
结果:许多文献都关注精神健康问题的发生率。只有少数文件主要评估了灾后心理社会支持的组织及其决定因素。该材料说明了在20年的过程中,荷兰灾后社会心理支持的组织背景如何受到立法、政策框架、循证指南的变化以及支持国家和地方政府和公共服务的正式专业结构的影响。反复出现的组织问题与一些相互关联的评估主题有关,例如规划、培训、注册、信息提供和社会认可。对于每个评估主题,我们识别了准备、急性和恢复阶段可以帮助或阻碍心理社会支持组织的因素。
讨论:综合分析表明,随着时间的发展,提供心理社会服务已经从单一学科发展到多学科领域。次优的跨专业协作对服务质量构成了反复威胁。尽管知识库已有所发展,但荷兰的灾后心理社会支持缺乏对其运作的系统和批判性评估。进一步的专业化应与加强评估和学习规划相结合。
关键词: 灾害, 恢复, 心理社会支持, 评估, 组织因素, 跨专业合作
1. Introduction
Disasters can have enormous impacts on communities and individuals, often entailing negative consequences (Boin, ‘t Hart, Stern, & Sundelius, 2016; Bonanno, Brewin, Kaniasty, & La Greca, 2010; Dyb et al., 2014; Norris et al., 2002; Yzermans et al., 2005). The delivery of effective and organized post-disaster psychosocial support (PSS) can aid affected communities and individuals in dealing with the negative consequences of disasters (Bisson et al., 2010; Pfefferbaum & North, 2016; Reifels et al., 2013; Suzuki, Fukasawa, Nakajima, Narisawa, & Kim, 2012; Te Brake & Dückers, 2013; Vymetal et al., 2011). However, the delivery of services during and after disasters is often met with conditions of collective stress and uncertainty (Boin & Bynander, 2015; Comfort, 2007; Reifels et al., 2013; Rosenthal, Charles & ‘t Hart, 1989; Scholtens, 2008). Hence, in addition to research on effective post-disaster PSS interventions for the health and well-being of affected persons (Dieltjens, Moonens, van Praet, de Buck, & Vandekerckhove, 2014; Gouweloos, Dückers, Te Brake, Kleber, & Drogendijk, 2014), some authors have recommended further study of the organizational dimension of post-disaster PSS (Bisson et al., 2010; Dückers, Yzermans, Jong, & Boin, 2017; Reifels et al., 2013; Te Brake & Dückers, 2013).
Various problems have been addressed and solutions proposed to increase the professionalization of post-disaster PSS. Several studies contributed to the development of expert and evidence-informed guidelines and to systems of planning and delivery of post-disaster PSS (Bisson et al., 2010; Dückers, Witteveen, Bisson, & Olff, 2017; Suzuki et al., 2012; Te Brake & Dückers, 2013; Witteveen et al., 2012). In general, a gap exists between norms as prescribed in post-disaster PSS guidelines and actual service delivery (Te Brake & Dückers, 2013). Studies show variations between geographical regions and post-disaster PSS programmes (Dückers et al., 2018; Witteveen et al., 2012). Planning and coordination are considered to be critical elements in disaster preparedness and management (Boin & ‘t Hart, 2003; Boin & Bynander, 2015) and are increasingly emphasized in post-disaster PSS. Collaboration and cooperation between professionals and organizations remain challenging as many different organizations and professionals are involved. As the delivery of psychosocial services in a post-disaster setting remains difficult (Goldman & Galea, 2014), increased knowledge of the effective organization of post-disaster PSS and factors that help or hinder that organization is required.
1.1. Objective
The objective of this study is to evaluate the organization of post-disaster PSS in different disaster settings and to identify factors that help or hinder this. A meta-synthesis of the available documents on Dutch disasters is conducted. This methodology is appropriate because the growing body of academic writings and grey literature on post-disaster PSS has not been examined systematically with the objective of drawing organizational lessons.
This research seeks to contribute to the knowledge base on post-disaster PSS by applying a less traditional research focus. So far, the post-disaster PSS literature has been dominated primarily by psychological, clinical and epidemiological research. In general, little attention has been paid to the organization of service delivery in a post-disaster setting. This study adds to the literature by identifying factors that help or hinder the organization of post-disaster PSS. We analyse the post-disaster PSS organization from a multidisciplinary perspective, including public administration, organization studies and psychology. The outline of this paper is as follows. First, we will describe the methodology, including our selection of disaster cases, the systematic search strategy and the inclusion criteria. Then, we will present the results of our analysis, followed by a discussion of the findings and a general conclusion.
2. Methodology
We conducted a meta-synthesis (Mays, Pope, & Popay, 2005), which is a qualitative systematic review method, to compare, integrate and aggregate the findings of scientific research and evaluations of the organization of post-disaster PSS in the Netherlands. A qualitative synthesis is a process of extracting and interpreting data into a collective form (Campbell et al., 2012), giving room for new insights and a better understanding of the research topic, especially in cases of multiple events (Walsh & Downe, 2005). The meta-synthesis method can be used ‘to explore barriers and facilitators to the delivery and uptake of services’ (Grant & Booth, 2009, p. 26). Although most qualitative review methods only include scientific research based on primary qualitative data (e.g. interviews or observations) (Britten et al., 2002), our meta-synthesis includes evaluations of the organization of post-disaster PSS as well. Research in health and policy disciplines increasingly argues for the inclusion of high-quality evidence based on non-scientific research, such as high-quality evaluation reports, to support decision making by policy makers and managers (Kuipers, Wirz, & Hartley, 2008; Mays et al., 2005). It is therefore important to notice that a meta-synthesis is essentially different from other types of qualitative reviews, for example, critical literature reviews (Thorne, Jensen, Kearney, Noblit, & Sandelowski, 2004). In our meta-synthesis, we include scientific literature based on primary data, as well as grey and formal evaluation reports.
Noblit and Hare (1988) suggest a seven-step approach for conducting a meta-ethnography. These steps are also applicable to a meta-synthesis (Britten et al., 2002). We highlight the important steps of narrowing the scope of the research (step 1), defining inclusion (step 2), analysis (steps 3–6) and writing down (step 7). Step 1 of the methodology involves defining the area of interest, the goal of the research and the research question. Hence, the remainder of this paragraph will address the inclusion of disasters and documents and the selection criteria applied. Moreover, a comprehensive search strategy was used to identify relevant articles and grey literature on the selected disasters, utilizing systematic search methods and snowballing methodology (Greenhalgh & Peacock, 2005). Inclusion and exclusion criteria were predefined, and documents were assessed by multiple reviewers. The review team included social scientists with a background in psychology, epidemiology and public administration, some of whom had previous experience in conducting systematic reviews. Finally, included articles were coded and partially double-checked by a second researcher. Based on the coding, several evaluation themes emerged and were reorganized into a scheme.
2.1. Selection of Dutch disasters
To identify relevant Dutch disasters, five selection criteria were used. First, a time frame between 1990 and 2014 was adopted in which events could be identified. Based on expert opinions, we decided that this time span reflects a relevant period for investigating the organization of post-disaster PSS, as the relevant history of PSS in the Netherlands is considered to have begun in 1990.1 Secondly, the event must have inflicted harm to such an extent that it would lead to Dutch casualties, either on Dutch or on foreign soil. Thirdly, the event must have endangered communities’ social and physical safety. Fourthly, the event must have endangered vital interests, such as economic values. Fifthly, the event should have led to the involvement of public administration in more than the emergency response. No databases exist that include all disasters; hence, expert opinions were used to come up with a non-exclusive list of Dutch disasters. In total, 12 disasters were included, comprising technological, transportation, human-made and natural disasters (Table 1).
Table 1.
List of included Dutch disasters.
| No. | Disaster | Date | Casualties | Injured |
|---|---|---|---|---|
| 1 | Bijlmer aeroplane disaster | 04-10-1992 | 43 (including crew) | Unknown |
| 2 | Faro air crash | 21-12-1992 | 56 | 106 |
| 3 | Legionella outbreak Bovenkarspel | 25-02-1999 | 32 | 206 |
| 4 | Fireworks explosion Enschede | 13-05-2000 | 22 or 23 | 947 |
| 5 | Bar fire Volendam | 01-01-2001 | 14 | 339 (63 severe) |
| 6 | Bird flu epidemic | 2003 | 1 | At least 1000 |
| 7 | Tsunami Indian Ocean | 26-12-2004 | 229,866 (36 Dutch) | Unknown (53 Dutch) |
| 8 | Q-fever outbreak | 2007–2010 | At least 14 | 3522 |
| 9 | Poldercrash Haarlemmermeer | 25-02-2009 | 9 (no Dutch) | 120 |
| 10 | Tripoli air crash | 12-05-2010 | 103 (70 Dutch) | 1 |
| 11 | Alphen aan den Rijn shooting | 09-04-2011 | 7 (including perpetrator) | 17 |
| 12 | MH17 aeroplane crash | 17-07-2014 | 298 (193 Dutch) | 0 |
2.2. Search strategy and selection criteria
A multidimensional search was conducted to find both grey and scientific documents (Figure 1). The search included the following steps. First, a systematic search was conducted in several scientific databases. The Cochrane, MEDLINE, PsycINFO and PILOTS databases between 1990 and 2014 were searched. Keywords for the search included terms associated with the specific disasters, such as ‘q fever’ or ‘flood’; terms associated with psychosocial service delivery, such as ‘psycho-social’; terms associated with the nature of the work, such as ‘rescue’ and ‘emergency’; and terms associated with document types, such as ‘assessment’ or ‘evaluation’. Secondly, personal archives of two Dutch disaster experts involved in the aftermaths of several of the events included were searched to find documents related to the 12 Dutch disasters. All documents eligible for full reading from the systematic search and documents from the personal collections were snowballed to further complete the list of documents associated with the disasters. Inclusion criteria for documents were: (1) their connection to one of the 12 Dutch disasters; (2) addressing post-disaster PSS for Dutch citizens; (3) reference to the organization of post-disaster PSS; and (4) being a form of informal or formal evaluation. Articles and documents were read by two independent readers. Disagreements in the reviewing process were resolved through discussion. An expert was consulted when there was disagreement.
Figure 1.
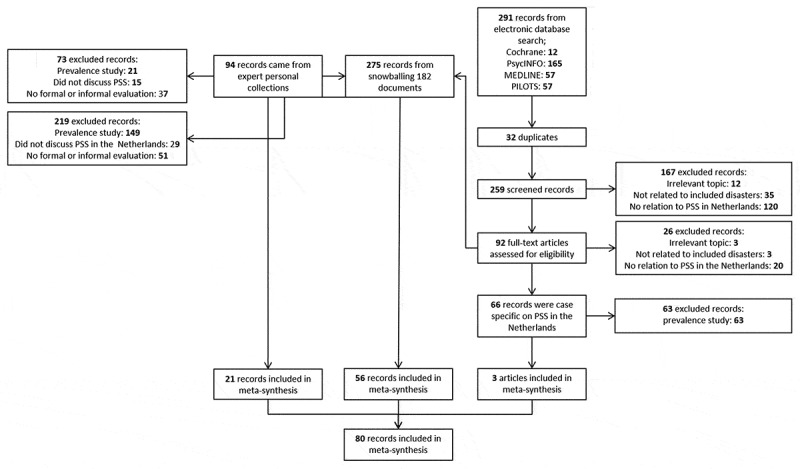
Inclusion scheme. PSS, psychosocial support.
2.3. Analysis
For the document analysis, a distinction in disaster phases was used, i.e. preparedness, acute and recovery (which is a simplification of other models that use a similar division but consider, for instance, prevention, mitigation and evaluation as distinct phases, e.g. Alexander, 2003; Lettieri, Masella, & Radaelli, 2009; Quarantelli, 1988). Coding was centred on central themes, reflecting the five main service categories as distinguished within the Dutch post-disaster PSS guidelines (Impact, 2014), within these phases:
Basic relief: this refers to emergency and rescue work in the direct aftermath of a disaster and to the emergency support that is offered directly afterwards, such as safety, medical assistance, food and water, medication and shelter.
Information provision is considered to be an essential element in post-disaster PSS service delivery (Ammerlaan, 2009; Te Brake & Dückers, 2013), and can refer both to aspects of psycho-education and to aspects of the event itself, the people affected (including next of kin) and expected developments in the aftermath.
Emotional and social support: a supportive context and social acknowledgement should be offered (Bonanno et al., 2010; Hobfoll et al., 2007; Kaniasty & Norris, 2004; Te Brake & Dückers, 2013). Indications exist that lack of social support leads to a higher prevalence of trauma-related mental health problems, such as post-traumatic stress disorder (PTSD) (e.g. Bonanno et al., 2010; Brewin, Andrews, & Valentine, 2000; Ozer, Best, Lipsey, & Weiss, 2003).
Practical support is aimed at assisting those affected with, for example, administrative tasks, household tasks, legal advice and financial support. Disasters often cause affected individuals to be confronted with tasks they normally could easily fulfil, or with tasks that had been unknown to them. Legal advice, for example, belongs to the latter category (Dückers & Thormar, 2015; Impact, 2014).
Medical assistance and health care, such as prevention, screening, diagnosis and treatment, should be provided, especially when affected groups have an increased risk of health complaints (Bisson et al., 2010; Te Brake & Dückers, 2013).
All included articles were coded by at least one researcher using MAXQDA, a software package for qualitative and mixed methods data analysis. Forty-three per cent of the data was coded by two researchers. The coding framework followed the five themes mentioned above against the background of the quality model in the Dutch post-disaster PSS guidelines and can be found in Appendix 1 (Impact, 2014). Based on the framework, key concepts that emerged from the coding were noted. The PSS-related findings from the evaluations per event were structured chronologically in an overview that illustrates which problems were identified, together with lessons and recommendations for the provision of PSS formulated by the evaluators (see Appendix 3). In the next section, the findings per coding theme and disaster phase are described. The findings are structured according to a set of overarching ‘evaluation themes’, reflecting omnipresent issues in PSS delivery since the early 1990s. Besides a description of issues according to each evaluation theme, we looked for specific factors evaluators recognized as determinants helping or hindering the organization of post-disaster PSS.
3. Results
The systematic search of scientific databases yielded 259 records. After screening of titles and abstracts, 92 records were retained and fully read. Three records addressed the organization of post-disaster PSS in the Netherlands. The search of experts’ personal collections resulted in 94 records. Snowballing of scientific literature and grey documents resulted in 275 records. After exclusions, the expert collections and snowballing yielded 77 results. Finally, a total of 80 records was included for analysis. See Figure 1 for a detailed overview of the inclusion process.
Figure 2.

Psychosocial support (PSS) evaluation themes and explanatory factors identified. The PSS delivery problems described in the included works centre on five distinct evaluation themes. In the preparedness phase, shortcomings are linked to training and planning. A recurring issue in the acute phase is the registration of affected individuals, which is linked to the immediate planning of services. In the recovery phase, evaluators repeatedly describe problems connected to information and social acknowledgement. The one-way arrows represent causal relations across stages, implied in the material studied. The two-way arrows represent associations where the direction is difficult to ascertain. The line of reasoning reflected in the documents points at sequential interdependencies across the crisis life cycle. Deficiencies in training and planning in the preparedness phase influence registration and planning in the acute phase. Registration and planning in the acute phase influence information and social acknowledgement. All PSS evaluation themes are influenced by four generic explanatory factors: awareness, event type, collaboration and (social) media.
3.1. Description of included documents
The included documents were divided into four categories. Formal evaluation reports are reports that have formal mandates to evaluate or investigate a disaster, given by governments or government institutions, for example. ‘Grey documents’ refer to documents that address some form of evaluation of psychosocial care after disasters but that do not have a formal mandate. Scientific research refers to documents that follow scientific methods, yet are not published in peer-reviewed journals. Examples are doctoral dissertations or research reports. The last category is scientific publications in a peer-reviewed journal (Table 2). Three peer-reviewed scientific publications were found to address the organization or evaluation of post-disaster PSS. Document analysis shows that evaluation of post-disaster PSS is often included as a small part of general crisis response evaluations. Stand-alone evaluations of post-disaster PSS services are amply done.
Table 2.
List of included Dutch disasters and documents.
| Disaster | Year | Total number of documents | Formal evaluation reports | Grey documents | Scientific research | Scientific publications in peer-reviewed journals |
|---|---|---|---|---|---|---|
| Bijlmer aeroplane disaster | 1992 | 23 | 5 | 12 | 4 | 2 |
| Faro air crash | 1992 | 4 | 3 | 1 | 0 | 0 |
| Legionella outbreak Bovenkarspel | 1999 | 2 | 1 | 1 | 0 | 0 |
| Fireworks explosion Enschede | 2000 | 18 | 4 | 10 | 4 | 0 |
| Bar fire Volendam | 2001 | 5 | 3 | 1 | 1 | 0 |
| Bird flu epidemic | 2003 | 3 | 1 | 2 | 0 | 0 |
| Tsunami Indian Ocean | 2004 | 0 | 0 | 0 | 0 | 0 |
| Q-fever outbreak | 2006–2009 | 4 | 3 | 1 | 0 | 0 |
| Poldercrash Haarlemmermeer | 2009 | 4 | 2 | 1 | 1 | 0 |
| Tripoli air crash | 2010 | 2 | 1 | 1 | 0 | 0 |
| Alphen aan den Rijn shooting | 2011 | 4 | 2 | 2 | 0 | 0 |
| MH17 aeroplane crash | 2014 | 9 | 3 | 4 | 1 | 1 |
| Multiple disasters | 2 | 0 | 2 | 0 | 0 | |
| Total | 80 | 28 | 38 | 11 | 3 |
3.2. Synthesis
A total of 80 documents was coded using the heuristic framework in Appendix 1. See Appendix 2 for the coding tree and Appendix 3 for a detailed overview of the analysed documents, including details on author, methods and main findings. Only three peer-reviewed scientific publications focused on the organization of post-disaster PSS (Boin, van Duin, & Heyse, 2001; Jong, Dückers, & van der Velden, 2016) or drew a conclusion on the organization of post-disaster PSS (Carlier & Gersons, 1997). The changes in the breadth of post-disaster PSS that we identified in the collected material, as well as the recurring evaluation themes considered by different authors across events, and the general factors helping or hindering the organization of post-disaster PSS will be considered in the following subsections.
3.2.1. Changes in the breadth of post-disaster PSS over time
The document analysis points to changes due to problems and deficiencies in the provision of services for people affected by the Bijlmermeer disaster in 1992 – across most of the coding themes – that resulted in recommendations and lessons that were implemented in the PSS approach in later disasters and major events. In addition, the scope of post-disaster PSS evaluations broadened from a rather medical, mainly psychological orientation on professional health care to an explicit assessment of social and emotional support, practical support and the provision of information. The observations and conclusions by evaluators are indicative of the broadening of post-disaster PSS over time, which is reflected in two ways in the documents.
First, since 1992, there has been a growing awareness of the long-term psychosocial consequences of disasters and crises (Witteveen, 2006) and the need for post-disaster PSS in the form of coordinated care provision (Carlier, van Uchelen, & Gersons, 1995; van Hemert & Smeets, 2004). This has resulted in a wider range of suitable interventions, such as a ‘one-stop shop’ (Carlier et al., 1995; Meijer, Oudkerk, van den Doel, Augusteijn-Esser, & Oedayraj Singh Varma, 1999), digital information and referral centres (Impact, 2012; Te Brake & Schaap, 2017) and specialized on-site reception (Inspectie Openbare Orde en Veiligheid, 2009). Secondly, there is a clear shift of emphasis from complaints and clinical interventions based on psychology and psychiatry (Carlier & Gersons, 1997; Carlier, Gersons, & Uchelen, 1993; Verschuur et al., 2004b) to general post-disaster health research. Moreover, authors apply a broader perspective on well-being and support, with an increased focus on needs and problems and particular risk groups (de Jong & van Schaik, 1994; Drogendijk, van der Velden, Kleber, & Gersons, 2004; Jong et al., 2016; Impact, 2004b; van der Bijl, van der Velden, Govers, & van Dorst, 2012; van Duin, Tops, Wijkhuijs, Adang, & Kop, 2012). The coding scheme (Appendix 1) (Impact, 2014) that we used covers this broadened range in PSS themes. No additional themes were identified during the analysis.
3.2.2. Recurring organizational evaluation themes
In light of developments in the organization of post-disaster PSS, it is possible to identify a series of omnipresent overarching evaluation themes in the reflections and conclusions by different authors, all related to (shortcomings in) the organization of post-disaster PSS. Figure 2 gives an overview of the evaluation themes and their causal relationships as implied in the documents. Conceptually, the themes could be linked to three phases. In the preparedness phase, the documents elaborate on post-disaster PSS problems that have to do with ‘planning’ and ‘training’. Besides ‘planning’ of recovery in the acute phase, another issue that remains problematic over the study period is the ‘registration’ of affected individuals and other post-disaster PSS target groups. Finally, two evaluation themes play roles in the recovery phase. Authors repeatedly describe problems concerning ‘information’ and ‘social acknowledgement’.
Figure 2 visualizes several associations and causal relations across phases assumed by different authors in the material studied (shown as dotted arrows; double arrows where the direction can go two ways). The evaluation themes are influenced by four generic factors: event type, awareness, collaboration and (social) media, which we will discuss in Section 3.2.3. In the remainder of this section, we will describe why these themes are seen as important and why they are recurring.
3.2.2.1. Planning
Planning aims at identifying and developing processes to effectively respond to disasters before the event takes place. Examples of such processes are the registration of affected individuals, quick response or post-disaster PSS at the event scene or in shelter locations. Over time, planning has gained an important role in pre-disaster preparation and has grown from being nearly absent (Carlier et al., 1993; Kroon & Overdijk, 1993) to being universal in preparation and even a legal responsibility (Alders, Belonje, van Den Berg, Ten Duis, & Doelen, 2001). The importance of planning is recognized by several authors (not only before but also for the recovery phase and the acute phase) (Veiligheidsregio Kennemerland, 2009a) because plans can assist in structuring behaviour during and after disasters (Kroon & Overdijk, 1993), promote making sense of a situation, and address responsibilities and tasks of individual stakeholders (Alders et al., 2001; Inspectie Openbare Orde en Veiligheid (IOOV), 2009; Inspectie voor de Gezondheidszorg, 2001a).
Although planning has an added value, several recurring issues are associated with planning. First, plans need to stay up to date (Alders et al., 2001; Inspectie Openbare Orde en Veiligheid, 2009; Jeeninga, de Vos, Wijkmans, & Bon-Martens, 2010), incorporating the changing local, organizational and governmental contexts and societal demands. Secondly, plans can never fully integrate the flexible nature of disasters. For example, it is difficult to take into consideration the scale of the disaster (Torenvlied et al., 2015; van Deursen, Prins, Kelderman, & Priester, 1993) and the length of the aftermath (Bosman et al., 2004; Impact, 2004a). As a result, plans must primarily be aimed at ‘guiding’ organizations and professionals through the uniqueness of each new disaster (van Duin et al., 2012).
Thirdly, authors note that plans should be embedded within organizations and the networks in which they function, and that more attention for implementation is preferred (Inspectie Openbare Orde en Veiligheid (IOOV), 2009; van der Meijden, Roorda, IJzermans, van der Velden, & Grievink, 2006). Fourthly, the use of plans requires that the parties implementing them constantly practise their plans and update their knowledge of those plans; yet, this aspect is often overlooked (Alders et al., 2001; Inspectie Openbare Orde en Veiligheid, 2011; Oosting et al., 2001).
3.2.2.2. Training
Training is the second recurring theme in the preparation phase. Evaluations or discussions on almost every disaster emphasize the need for adequate, even structural, training of professionals in assessing and delivering PSS. Even the most recent evaluations still focus on improved training for adequate response in PSS (Laurier, Ten Brink, de Gouw, & Corvers-Debers, 2013; Te Brake & Schaap, 2017). Authors state that training can help to secure plans within organizations (Inspectie Openbare Orde en Veiligheid (IOOV), 2009; Kroon & Overdijk, 1993), that it makes people familiar with their tasks (Alders et al., 2001; Inspectie Openbare Orde en Veiligheid (IOOV), 2009) and that it is helpful in creating a thorough understanding of the field (Laurier et al., 2013).
Difficulties lie in the connectedness of the quality of training with the presence and quality of plans (Alders et al., 2001; Oosting et al., 2001). Moreover, training design influences effectiveness. The need for realistic training based on existing plans is emphasized (Veiligheidsregio Kennemerland, 2009b). Some authors recommend incorporating a culturally sensitive approach in training to create awareness of cultural differences (Drogendijk et al., 2004; Netten, 2005).
3.2.2.3. Registration
Registration of victims and affected persons emerged as an important theme and seems to serve several goals. First, registration serves as an indicator of the scale of the disaster for first-response organizations and to facilitate identification of victims and their next of kin (Inspectie Openbare Orde en Veiligheid (IOOV), 2009b, 2011). Insufficient information about the fate of loved ones can lead to feelings of uncertainty and disquiet (Alders et al., 2001; de Boer & van der Heide, 2010; Noordegraaf et al., 1993). When affected persons are not registered at all, this generates dissatisfaction (Soeteman, 2009), especially when errors in registration occur (Alders et al., 2001) or when, during registration, a distinction is made that does not do justice to the actual course of events (Laurier et al., 2013).
Secondly, registration provides important information for the organization of the recovery phase (Laurier et al., 2013). Authors state that registration is important to guarantee continuity of care (Kroon & Overdijk, 1993) and to enable an adequate flow of information and practical assistance to those in need (Nuijen, 2006; Oosting et al., 2001). Existing registration (e.g. primary care databases) can be used to monitor (health) problems over time and consequently to direct care (Dorn, ten Veen, & IJzermans, 2007; Yzermans & Gersons, 2002).
Registration of victims and affected persons has remained a constant challenge over the years (Alders et al., 2001; Groen, Koekkoek, & Slump, 2001; Informatieen Adviescentrum, 2001; Inspectie Openbare Orde en Veiligheid (IOOV), 2009; Oosting et al., 2001; Veiligheidsregio Kennemerland, 2009b). For example, registration to monitor affected persons requires specific knowledge (Yzermans, Dirkzwager, Kerssen, Cohen-Bendahan, & Ten Veen, 2006), and a uniform registration format does not exist (Informatie en Adviescentrum, 2001, 2003b). It is difficult to organize training to prepare for registration and to do justice to the complexity of registration during the acute phase (Inspectie Openbare Orde en Veiligheid (IOOV), 2009; Veiligheidsregio Kennemerland, 2009b), yet it is necessary to clarify roles and responsibilities (Inspectie Openbare Orde en Veiligheid (IOOV), 2011).
3.2.2.4. Information
Information delivery during the recovery phase deals with sending information about the nature and range of the disaster, the settlement of claims, legal procedures, commemoration ceremonies, etc. Quick and adequate information is seen as a minimal requirement for post-disaster PSS (e.g. Alders et al., 2001; Meijer et al., 1999; Oosting et al., 2001). It helps to reduce uncertainty among affected persons (Meijer et al., 1999) and helps them to get a grip on the situation again (Oosting et al., 2001). The lack of adequate information can have far-reaching consequences, significantly complicating the recovery in terms of length of time and content of the recovery (Boin et al., 2001; Witteveen, 2006; Yzermans & Gersons, 2002).
Focal points in evaluations are transparency in information processes and debunking of rumours (Meijer et al., 1999; van der Bijl et al., 2012), the creation of a (digital) one-stop shop (Bosman et al., 2004; Carlier et al., 1995; Yzermans & Gersons, 2002; Impact, 2004a; Meijer et al., 1999), the alignment of different information flows (Carlier, 1996) and the creation of accessible and understandable information, especially in dealing with technical information (Bosman et al., 2004) or with different cultural groups (Groen et al., 2001; Netten, 2005). A timely delivery of information is important, yet many disasters are characterized by a late and cautious response by authorities in addressing the event (van Dijk et al., 2010; Gersons, Carlier, & IJzermans, 2000; Yzermans & Gersons, 2002; Klerx van Mierlo, 2009; van der Bijl, van der Velden, Govers, & van Dorst, 2012; van Duin et al., 2012b; Verschuur et al., 2004b). Solutions can be found in early impact assessments on health communication (Grievink, van der Velden, de Vries, Mulder & Smilde - van den Doel, 2006), frequent communication (Oosting et al., 2001) and early meetings with affected persons (de Boer & van der Heide, 2010).
3.2.2.5. Social acknowledgement
Many documents point to the importance of social acknowledgement, simultaneously addressing the multifaceted nature of social acknowledgement as a concept (Jong et al., 2016; Laurier et al., 2013; van der Bijl et al., 2012). On the one hand, social acknowledgement is seen as a goal in itself, something that should actively be delivered through, for example, house visits by mayors (Jong et al., 2016; Laurier et al., 2013) or (health-care) professionals (Gouweloos & Den Brinke, 2013; van der Velden & Kleber, 2000).
On the other hand, social acknowledgement is seen as a by-product of post-disaster activities, such as information delivery (Laurier et al., 2013; van der Bijl et al., 2012), the organization of a one-stop shop serving the needs of those affected (Impact, 2012, te Brake & Schaap, 2017), a particular case management approach (Laurier et al., 2013) and the simplification of bureaucratic structures resulting in, for example, easier access to (semi-)governmental institutions and health-care organizations (Alwart, Macnack, Pengel-Forst, & Sarucco, 1993; Laurier et al., 2013; van der Bijl et al., 2012; Yzermans & Gersons, 2002). Several documents address the effect of correct registration of affected persons on their perceived experience of social acknowledgement (Laurier et al., 2013; Oosting et al., 2001).
3.2.3. Recurring explanatory factors
The analysis of the included documents points to several generic and recurring explanatory factors in the organization of post-disaster PSS. We will describe them below.
3.2.3.1. Awareness
Political and governmental actors need to be aware of the need for post-disaster PSS. This awareness has increased over time (Coebergh, 1999; Crisis Onderzoeksteam, 1999; Inspectie voor de Gezondheidszorg, 2001b; van Deursen et al., 1993), resulting in, for example, planning templates (Bosman et al., 2004; Inspectie Openbare Orde en Veiligheid (IOOV), 2009). However, many challenges remain. For example, investments in preparation for long-term recovery after disasters are amply done (Alders et al., 2001), and the embedment of post-disaster PSS structures in local governments remains problematic (Crisis Onderzoeksteam, 1999).
Costs of training can be high (Te Brake & Schaap, 2017), while at the same time professionals have little time to participate (Oosting et al., 2001). As a result, the organization of training for post-disaster PSS is highly dependent on the political priority that is given to post-disaster PSS preparation (Alders et al., 2001; Laurier et al., 2013). A lack of political priority (Klerx van Mierlo, 2009; Meijer, Oudkerk, van Den Doel, Augusteijn-Esser & Oedayraj Singh Varma, 1999; van Duin, Overdijk, & Wijkhuijs, 1998a) or insufficient knowledge of psychosocial needs (Laurier et al., 2013; Nuijen, 2006; Oosting et al., 2001) can result in a lack of awareness for giving or organizing social acknowledgement.
3.2.3.2. Disaster type
The different events analysed in this research can be categorized differently. There are sudden-onset disasters with either a short or a lingering aftermath and slow-onset disasters; in this study, mostly infectious diseases. Slow-onset events are difficult to detect, and involved parties have difficulties setting priorities for the recovery (Bosman et al., 2004; Crisis Oonderzoeksteam, 1999; van der Bijl et al., 2012). Slow-onset disasters lack a position in planning and training (Bosman et al., 2004; Impact, 2004a). It is difficult to oversee the scale of the disaster (van Deursen et al., 1993) and the length of the aftermath (Bosman et al., 2004; Impact, 2004b). Registration of affected persons is a constant factor that requires attention (Bosman et al., 2004).
3.2.3.3. Collaboration
Many documents emphasize the importance of collaboration for the organization of post-disaster PSS. Collaboration is problematic across several of the recurring evaluation themes. For example, dissemination of plans and templates among different partners was sometimes lacking (Alders et al., 2001; Oosting et al., 2001), there was a lack of agreement about the contents of the plans (Inspectie voor de Gezondheidszorg, 2001b), and information exchange between different partners remains problematic (Kroon & Overdijk, 1993; van Duin et al., 1998b).
Several causes of collaboration issues are mentioned. First, problems are rooted in a lack of knowledge of the existing and required network (Alders et al., 2001; Inspectie Openbare Orde en Veiligheid (IOOV), 2009; Laurier et al., 2013; Oosting et al., 2001) and associated roles and responsibilities (Inspectie Openbare Orde en Veiligheid (IOOV), 2009). Secondly, international boundaries cause the international exchange of information to remain problematic even today (Torenvlied et al., 2016; van Duin, Overdijk, & Wijkhuijs, 1998b). Thirdly, interests may be difficult to align – for example, economic interests versus health interests (van der Bijl et al., 2012) – between different organizations and stakeholders, such as governmental departments, semi-governmental organizations and hospitals (Crisis Onderzoeksteam, 1999; Jeeninga et al., 2010; Oosting et al., 2001; van der Bijl et al., 2012; van Duin et al., 2012). Fourthly, a monodisciplinary focus on the organization of the crisis response and its associated recovery phase may result in, for example, an inadequate and delayed dissemination of information (Impact, 2004a; Inspectie Openbare Orde en Veiligheid (IOOV), 2011). A monodisciplinary focus also prevents organizations from adequately learning from each other (Nuijen, 2006).
3.2.3.4. (Social) media
The role of the media – and later on social media – is mentioned as an important factor in the organization of post-disaster PSS. Repeatedly, media are found to give confusing and ambiguous information about disasters (KLM Arbo Services, 2004; van Duin et al., 1998a; Witteveen, 2006). Recently, social media has become influential in information delivery and retrieval (van Duin et al., 2012; Veiligheidsregio Kennemerland, 2009b), enabling a quick spread of information and rumours and causing organizations to experience less control over information flows. Social media watching can be considered a crucial part of crisis response and communication (Veiligheidsregio Kennemerland, 2009b).
4. Discussion
In this research, we systematically investigated the organization of post-disaster PSS in the Netherlands over time and identified several determinants. To increase our understanding of the organization of post-disaster PSS, we followed an interpretative approach, using a meta-synthesis to aggregate information on 12 different Dutch disasters. To our knowledge, this is the first synthesis in the field of post-disaster PSS to use this approach and include such a large number of disasters. Our review included scientific documents and evaluation reports. In this section, we will reflect on our findings, make suggestions for further research and discuss the limitations of this research.
4.1. Changes in organizational context of post-disaster PSS over time
The body of knowledge captured in the documents that we analysed points to a growing and developing field of post-disaster PSS in which policies and interventions are embedded within national, regional and local governments, as well as semi-governmental and private partners. This is reflected in several main topics. First, the plea for coordinated provision of care after the Bijlmer aeroplane crash (Carlier et al., 1995; Meijer, 1992; van Hemert & Smeets, 2004) has been realized over the years (Informatie en Adviescentrum, 2003a; 2003b; Laurier et al., 2013; Oosting et al., 2001; Te Brake & Schaap 2017), reflected in, for example, the forms of working agreements and partnerships. Secondly, in the Netherlands – particularly in reaction to the negative post-disaster PSS evaluation after the Bijlmer aeroplane disaster in 1992 and the generally more positive evaluation of the Enschede fireworks disaster in 2000 – a national PSS knowledge centre was established by three ministries in 2002, and a health research and monitoring expert committee was installed in 2004 to support local and national governments during crises with a public health dimension (Behbod et al., 2017).
Since the early 2000s, post-disaster PSS has been incorporated as a public health and public safety responsibility in legislation and strategy documents (e.g. Bruinooge et al., 2012; Dückers, 2012; Wet Publieke gezondheid, 2012; Wet Veiligheidsregio, 2010). National evidence-based post-disaster PSS guidelines for the general population and uniformed services were developed for governments and service providers (e.g. Impact, 2010, Impact, 2014; also see te Brake et al., 2009). In addition, since the Enschede fireworks disaster, coordinated service structures for affected populations have become standard post-disaster PSS instruments (Behbod et al., 2017; Dückers, Witteveen, et al., 2017; Te Brake & Schaap, 2017; Vereniging voor Nederlandse Gemeenten, 2004; Yzermans & Gersons, 2002).
These developments and structures are reflected in the documents that we analysed. They gradually affected the planning and evaluation of the later events over the course of our time frame, influencing the background against which the authors described and reviewed post-disaster PSS delivery in the context of the 12 events. The changes in organizational context follow from the broader exchange and cooperation between governments, professional service providers and academics, and resulted in quality improvement instruments at the local, regional and national levels in the Netherlands. As such, we can conclude that many of the lessons and recommendations listed in Appendix 3 were actually implemented. Nevertheless, the fact that the quality management system of post-disaster PSS has been enriched does not take away the need for continued investment in preparation for PSS by responsible governments and agencies, nationally and locally (de Bas, Helsloot, & Dückers, 2017).
4.2. Further research
The changes and innovations highlighted so far give rise to new challenges in addition to the old ones that still need to be maintained. First, our findings show that although post-disaster PSS in the selected time frame was amply evaluated, a systematic approach was lacking. This seriously reduces the possibility of learning from major events, limits possibilities for quality improvement and makes estimates on (cost-)effectiveness and other quality criteria in relation to the health of affected individuals and groups problematic.
The inclusion of only three relevant peer-reviewed scientific articles analysing organizational aspects of PSS leads us to believe that there is still little academic and practical attention being paid to this topic in the Netherlands. The majority of the scientific publications on post-disaster PSS is aimed at understanding health effects resulting from disasters, while little attention is given to the organization of post-disaster PSS during each phase of the disaster. This can be seen as surprising, given the implications of suboptimal post-disaster PSS for affected persons, and also given the risks involving suboptimal PSS for public leaders in terms of accountability (Dückers, Yzermans, et al., 2017). Developing coherent evaluation models for post-disaster PSS focusing on unravelling contexts, mechanisms and outcomes is a promising next step in improving the organization of post-disaster PSS.
Secondly, as a result of the broadening of the scope of post-disaster PSS, the multidisciplinary nature of post-disaster PSS requires researchers to adopt new theoretical perspectives, such as interorganizational and network theory, to better understand the organizational dynamics of post-disaster PSS. In terms of training and planning, this requires organizations and professionals to develop new skills and integrate knowledge about psychosocial principles and new ways of working into their crisis management activities and normal routines (Dückers, Yzermans, et al., 2017). Interprofessional collaboration could be enhanced by training PSS actors to become more familiar with their and each other’s roles (Boin & Bynander, 2015; D’Amour, Ferrada-Videla, Rodriguez & Beaulieu, 2005) and with viewing the organization of planning more as a process than as a product (Perry & Lindell, 2003). Training may also enhance managers’ knowledge of contextual and organizational factors and their improvisational skills (Perry & Lindell, 2003).
Thirdly, the evaluation themes in this article seem to have sequential interdependence. Shortcomings in the preparedness phase affect other themes in successive phases. For example, information retrieved from registration of affected persons is essential for the layout of the recovery phase, yet registration – despite national initiatives to formulate solutions – remains difficult to organize and the suboptimal transfer of information is likely to hinder the provision of PSS to people with needs and problems in future events.
Our findings corroborate earlier findings on the interconnectedness of these phases (e.g. Kapucu & van Wart, 2006; Neal, 1997; Quarantelli, 1988, Quarantelli, 2005). Moreover, this research shows that post-disaster PSS has a distinct role during every phase of the disaster management cycle and not only during the recovery phase. Based on the collected material, we conclude that the success or failure of PSS in the recovery phase is highly dependent on activities in the preparedness and acute phases. Hence, the organization of post-disaster PSS deserves an important and visible place during every step of disaster and emergency management.
We can conclude that coordinated collaboration across the borders of disciplines and professions remains at the heart of the organization of post-disaster PSS. This is in line with earlier research on post-disaster PSS (e.g. Bisson et al., 2010; Dückers et al., 2018; Reifels et al., 2013; Witteveen et al., 2012) and findings in the general crisis management literature (Alexander, 2003; Boin & Bynander, 2015; Neal, 1997; Quarantelli, 1988). General issues associated with coordination are a lack of an exclusive definition of coordination (Boin & Bynander, 2015), preparedness that is insufficient for dealing with the flexible nature of disasters (Ansell, Boin, & Keller, 2010), and interagency and intergovernmental alignment (‘t Hart, Rosenthal, & Kouzmin, 1993). Similar problems are found in this research: implementation of expert-informed or evidence-based knowledge into practice is difficult, and alignment of interprofessional, interorganizational and intergovernmental interests remains problematic, especially during creeping crises like the examples mentioned and infectious diseases or zoonosis, owing to conflicting interests of involved ministries and the ministry of health (e.g. Haalboom, 2017; van der Bijl et al., 2012).
Initiatives to address the issues found in our study locally and nationally will potentially be affected by the decentralization and decoupling of semi-governmental institutions, an international trend in Western European countries (e.g. Bannink & Ossewaarde, 2012; Pollitt & Bouckaert, 2011). Coordinative processes for interprofessional and interorganizational practice require continuous attention. We described how coordination roles were legally allocated to regional public health and public safety actors who need to align and connect their respective networks on behalf of PSS. Moreover, post-disaster PSS opened up a broad spectrum of organizations and professionals, expanding the diversity of the domain rapidly. To optimize coordination, Boin and Bynander (2015) suggest a combination of top–down and bottom–up coordination consisting of professional reliance (competent and skilled professionals in a working context with a management that supports timely and adequate action in different time stages). However, it is the role of the professional that remains largely underexposed in the literature (including the meta-synthesis described in this article). Improvement of interprofessional collaboration requires knowledge of how collaboration is and can be organized in uncertain and pressured settings and which professional skills are required.
Finally, the focus of the meta-synthesis has been entirely on the Netherlands since the beginning of the 1990s. It would be very valuable to compare the findings to the development of post-disaster PSS in other countries and to compare the issues encountered, lessons formulated, solutions tested and factors that helped or hindered the provision of services to people affected by disasters and major incidents. In earlier studies, notable differences were described in six European regions in their adherence to evidence-based guidelines (Witteveen et al., 2012) and the developmental statuses of the local PSS planning and delivery systems; these developmental statuses were confirmed to be associated with country characteristics such as good governance, access to general practitioners and hospitals, and public and private health expenditure (Dückers, Witteveen, et al., 2017). Since the adherence to guidelines and the organization of PSS are not similar across regions, reflecting differences in tradition, culture and other conditions, it is not likely that our results are universally applicable to, for instance, the southern, south-east and eastern regions of Europe, given the differences in professional health-care capacity and lower developmental scores of PSS planning and delivery systems. We expect that the organization of services in countries in northern, western and central Europe, with similar guidelines, professional standards, institutions and cultural values, will experience similar challenges.
4.3. Limitations
In this study, a substantial number of publications was assessed on the organization of PSS during different events. However, several limitations should be discussed. First, this meta-synthesis included academic literature, systematic evaluation and grey literature. We should note that the evaluations reflect the prevailing ideas of that time and other interests. For example, topics for evaluation differ per time and per disaster as a result of political attention to specific subjects. In other words, the objectivity of the evaluations should be considered with caution. Secondly, the quality of the evaluations depends on the methodology used. Only a few evaluations explicitly mentioned methodological considerations, and overall, no systematic evaluation approach was used. Nevertheless, in our opinion, the included documents contain indispensable information.
Thirdly, although we have included a large number of documents using systematic search methods, some proportion of evaluations and grey documents might not show up in databases or through snowballing. We feel confident that with our systematic search through scientific databases, snowballing and the use of expert input, we have included the most important documents. Fourthly, a meta-synthesis aims at aggregating information on specific phenomena, but as the basis of this method is interpretative research, and the research itself is also interpretative, generalizability of the findings should be considered with caution. We recommend replication of our study in other countries. In this light and more broadly, we recommend international cooperation and investment in the development of comprehensive PSS evaluation frameworks and instruments. The availability of high-quality evaluations is a crucial precondition for an informative meta-analysis.
5. Conclusion
In this study, we systematically examined available evaluations of the organization of post-disaster PSS in the Netherlands over time and identified several continual evaluation themes and explanatory factors. Based on our collected data, we can draw several important conclusions. Despite the implications of suboptimal post-disaster PSS, there is still little academic and practical attention being paid to the organization of post-disaster PSS. Post-disaster PSS has become professionalized over the years, yet we identified recurring challenges in the multidisciplinary landscape where post-disaster PSS is shaped and implemented. These challenges have to do with a lack of awareness and coordination and collaboration between network partners. We have shown the interconnectedness of different disaster phases and activities within those phases. Several important factors hindering or helping the organization of post-disaster PSS were found. The coordination of interprofessional and interorganizational processes requires continuous attention. Further professionalization is coupled with the strengthening of evaluation and learning routines.
Acknowledgements
The authors wish to thank Jonna Lind for her assistance with the literature search, and Berthold Gersons and Joris Yzermans for giving the researchers access to their personal archives with evaluations, articles, books, reports and correspondence on many of the disasters and crises analysed in this study.
Appendix 1.
Coding scheme based on Dutch psychosocial support guidelines flowchart
Background
The Dutch post-disaster psychosocial support (PSS) guidelines (Impact, 2014) contain several flowcharts for different target user groups of the guidelines. Each flowchart is made up of similar process and thematic content branches, which will be elaborated upon below. In this study, the themes in the sections A–D of the ‘collective PSS’ flowchart were used as a coding scheme for the included PSS evaluations. The themes are shown in red in Figure A1.
Figure A1.

Flowchart of collective psychosocial support (PSS).
Process
The planning and delivery of PSS ideally follow a series of sequential steps and repetitive loops. On the left-hand side of the flowchart, the process stem runs down vertically and stimulates parties to involve available expertise from earlier events and to look at needs, problems, and risk and protective factors of affected people at the group and individual levels. The content branches include different themes to consider when developing the PSS plan; a plan that needs to be updated as time evolves and the needs and problems of affected people are likely to change. Whether a particular theme in sections A–D (see below) is relevant depends upon the circumstances. During the coordinated implementation, the strategy and its outcomes can be assessed. Monitoring allows for the detection of bottlenecks. To what extent do expected and actual measures, conditions and results differ from each other? To be able to assess this, it is necessary to speak to affected people, service providers and other people involved. Follow-up actions in case of problems and bottlenecks encountered are needed to safeguard the quality of the PSS approach.
Section A. Themes Relevant Regardless of Phase
The first section covers themes that are not linked to a particular phase.
Provision of information
The first four themes concern the provision of information via a variety of sources and channels, e.g. appointed contact persons for those affected, press conferences, residents’ meetings, closed meetings for survivors and relatives, mass media, mailing, pamphlets and websites, and open or private forums. Contact persons, gatherings and forums can also be used to gather information about the needs and wishes of those affected, as well as existing bottlenecks in the aid offered. Whereas themes A1 and A4 can be worked out in a public communication approach, in themes A2 and A3 service provision enters the personal realm of those affected.
A1. During a disaster or major crisis, the first and foremost thing to do is to supply reliable information about the event and its consequences. The information needs to be given in the language and format that the affected person will be able to understand. It will be partially supplied by the authorities, but an individual relief worker can also explain what he or she knows, as long as the information is indeed verified and released. After the event, affected people will want to know what exactly happened, what caused it and what will happen next. What will the government and other parties involved do? What have they consciously chosen not to do? Are there (health) risks involved and if so, how are people expected to react to those? Are there rumours that need be denied or rectified?
A2. Some information requires a personal conversation, especially about the fate of loved ones. This is where personal contact between the bearer and receiver of good or bad news is very important.
A3. The same applies to reunification of people missing and their families, the confrontation with those deceased, and handing over personal possessions; these are all emotional matters which in practice will involve compassionate involvement of family detectives, victim support or employees from the Ministry of Defence.
A4. What are non-alarming reactions (such as sadness, anger), what tips are given about the things that people can do themselves (do not watch the images on screen for too long, play with your children, visit a general practitioner if complaints last longer, etc.)?
Social acknowledgement/recognition
In the second place, section A relates to the expressed acknowledgement/recognition that those affected have been confronted with danger and great loss.
A5. PSS is, in itself, an expression of engagement on behalf of government and society. PSS by public leaders and service providers can play an important role in showing engagement towards affected people including relief works and other service providers. This can be done during the channels used for A1–A4, and particularly by involving people as much as possible in choices and initiatives that can be relevant for them. Expressing concern and listening to an affected person’s story is something that can be done by any service provider or government or organization representative; from paramedic to mayor. Engagement is reflected in a compassionate and respectful attitude, regardless of the occasion, whether it is a ministerial visit to the location of the disaster, a gathering of survivors, relatives and members of the royal family, a home visit by the mayor, a local or national memorial service, or unveiling a monument.
A6. Make apologies where this is suitable. However, liability and compensation issues might have a negative effect on the perceived sincerity of social recognition expressed by governments or organizations, at least from the perspective of the affected.
A7. In all cases, it is important that realistic expectations are raised and that promises are fulfilled, otherwise disappointment and disillusion of those affected will be fostered.
Section B. Themes Relevant During and Directly After the Event
Section B comprises the PSS themes in the immediate response. Especially in this phase, there will be a need for basic help and practical support.
B1. People affected by a disaster or major event will need basic help. In the acute phase, emergency services and rescue workers are tasked with bringing people into safety and transporting the wounded as quickly as possible to a place where they can receive medical care.
B2. The affected person may want to contact loved ones or others, and may need transport to go home or to another (temporary) place of residence.
B3. If conditions enable it, the relief worker can provide those affected with food, drink and medication, or mediate for those things.
B4. If everyday surroundings are completely destroyed, those who are affected will have to be provided with shelter or temporary living arrangements (e.g. family, a hotel, a sufficiently large public space, tents).
B5. As soon as people are out of danger, for example at a shelter or simply at a safe distance, the relief worker can focus on fostering peace and quiet, and intervene in the rare cases that someone affected constitutes a threat to himself or others (conflict, psychological decompensation).
Section C. Themes Relevant in the Recovery Phase
The recovery phase can take a long period of time, up to many years. People need to find a way to deal with their material and immaterial losses. Support from governments and relief workers will have to complement the capacity to recover and the resources available to affected people. In addition to that, support needs to be aimed at minimizing disappointment and disillusion, as soon as mobilized social support and other aid diminishes.
C1. Basic help is needed in areas where homes have been destroyed, or food supplies have broken down due to disrupted infrastructure.
C2. Practical help around the house and administration can be needed if affected persons are incapable of providing for themselves, and the personal circle is unable to offer sufficient help.
C3. When events involve larger numbers of affected people – exact numbers are hard to name; it also depends upon the complexity of their needs and problems – it is helpful to bring supportive services together in a one-stop shop, e.g. a physical information and advice centre or a digital information and referral centre. In case the geographical spacing of affected people is limited, setting up a physical centre is the most obvious. In those cases where people are distributed over a wider geographical area, an online environment is recommended. Both types of one-stop shops allow visitors to receive answers and connect to the right service providers. Various types of service and information can be made accessible via one point. A one-stop shop is a fixed starting point for contact with affected people, helps in monitoring aid and problems, can further contact with fellow sufferers (peer support) and can support legal completion of the event for those affected, without stigmatizing people in the outside world.
C4. Other support which fits the needs of affected people in the recovery phase includes facilitating self-organizations (giving them a voice to stimulate the promotion of interests, creating a contact point that can speak on behalf of those affected) and peer support (gatherings, closed forums).
C5. Memorial services or monuments are essential elements of public meaning-making and collective mourning within an affected community. It is important that those affected are included in both decision-making and implementation processes.
Section D. Themes Relevant for People with Health Problems
The fourth section covers the care for people with health problems or health risks.
D1. This theme is linked to the earlier steps in the process tree, yet now explicitly linked to the health of the affected population. Health research is a means to understand the (potential) need for support and care; it also can help to prevent or reduce social commotion when people are afraid of harmful consequences to their health due to exposure to the disaster or related hazards.
D2. The themes in section D are about health care and the road leading up to it. If a disaster severely disrupts the regular care system, or makes a larger appeal to its capacity than is available, emergency measures will have to be put in place. In other cases the regular, stepwise health-care system will be used to offer care to affected people.
D3. Everyone affected is responsible for their own health. People suffering from lasting symptoms can consult their general practitioner or company doctor, whether or not urged to by the circles surrounding them. Health-care providers can assess whether care is needed. In the first month, the general advice is to exercise restraint. In addition, some psychological problems can only be diagnosed adequately after one month. Consultation with an affected person may result in the decision to wait a bit longer, or treatment may be prescribed, but the general practitioner or company doctor may also refer to specialized care providers. For children, the policy is not to wait too long, because symptoms may interfere with development and can lead to emotional, social and cognitive stagnation.
D4. For various diagnoses and treatments, evidence-based guidelines have been developed for care professionals.
Appendix 2.
Coding tree.
| Code | No. of codes |
|---|---|
| Process | 0 |
| P1. Involve experts of other disasters and crises | 27 |
| P2. Register those affected, identify risk groups and (social) risk factors | 160 |
| Risk groups | 6 |
| P3. Gain insight into needs and problems of affected people | 158 |
| P4. Develop/plan the PSS approach | 135 |
| P5. Coordinate and support the implementation of the PSS approach | 189 |
| P6. Evaluate the implementation and results of the PSS approach | 89 |
| P7. Adjust the PSS approach if it does not suffice any more | 16 |
| Recommendations | 299 |
| Section A: relevant regardless of phase | 0 |
| A1. Provide reliable information about the event (facts, progress, interpretation) and rectify rumours | 271 |
| A2. Provide reliable information about the situation of loved ones | 88 |
| A3. Facilitate reunion/confrontation with loved ones | 44 |
| A4. Inform people about possible reactions, complaints and reassure when appropriate | 39 |
| A5. Show engagement to affected people on behalf of government and society | 62 |
| A6. Government: react humanly and reasonably to compensation requests and apologize | 54 |
| A7. Raise realistic expectations, live up to promises made | 23 |
| Section B: relevant during and directly after the event | 29 |
| B1. Bring those in need into safety and ensure medical help | 80 |
| B2. Offer practical support (communication, transport, money) | 32 |
| B3. Provide for primary necessities of life (food, drink, medication, sanitary options) | 6 |
| B4. Take care of temporary relief or shelter for those who have nowhere to go | 41 |
| B5. Keep professionals close during collective risk moments (e.g. escalation or psychological decompensation) | 12 |
| Section C: relevant in the recovery phase | 21 |
| C1. Provide basic help where needed (safety, transport, food, drink, medication, shelter) | 30 |
| C2. Provide practical help where needed (administration, household, legal advice, financial support) | 160 |
| C3. Set up a one-stop shop for coordinated provision of information or services | 135 |
| C4. Facilitate self-organization and exchange of experiences between affected people where needed | 80 |
| C5. Organize/facilitate a memorial service/monument (a collective moment of commemoration or mourning) | 51 |
| Section D: relevant for people with health problems | 0 |
| D1. Carry out health research for actual or perceived health risks | 177 |
| Prevalence/incidence | 184 |
| Psychosocial issues/complaints | 82 |
| D2. Refer people with lasting symptoms to regular health care, organize, if necessary, extra capacity | 161 |
| D3. Enable GPs and company doctors to detect, treat and refer people with symptoms | 43 |
| D4. Stimulate that individual care providers and other service providers adhere to these and other relevant guidelines | 1 |
PSS, psychosocial support; GP, general practitioner.
Appendix 3.
Included documents per disaster.
| Reference (Document type, method: techniquea) |
Publisher/journal | Main findings |
|---|---|---|
| Bijlmer Aeroplane disaster (event type: aeroplane crash) | ||
| Meijer (1992). Een vliegtuigramp in een huisartspraktijk; posttraumatische reacties in de eerste vier weken na de ramp in de Bijlmermeer. (Scientific publication, C) |
Nederlands Tijdschrift voor de Geneeskunde | ● Proper coordination of care in collaboration with a GP is required ● There was little collaboration between GPs and other medical disciplines |
| Carlier et al. (1993). De Bijlmermeer-vliegramp: een onderzoek naar de psychische gevolgen bij getroffenen en hun commentaar op de geboden nazorg. (Research report, A:3) |
Academic Medical Center Amsterdam | ● Preparation for post-disaster PSS in the Netherlands hardly exists ● 72% of the affected population was psychologically disrupted ● No formalized coordination of post-disaster PSS and specialist mental health care ● Organize a one-stop shop ● Disasters require significant flexibility from organizations involved in the direct and long-term provision of PSS |
| Gersons and Carlier (1993b). De Bijlmer-ramp: crisisinterventie en consultatie. (Scientific publication, C) |
Maandblad Geestelijke Volksgezondheid | ● Crisis intervention was the main methodology in the direct aftermath |
| Kroon and Overdijk (1993). Psychosocial care and shelter following the Bijlmermeer air disaster. (Scientific publication, B:5,7). |
Crisis | ● Difficulties exist in interagency coordination ● There is a need for ample planning and training ● Interventions should be tailored to survivors’ specific needs ● Registration is of utmost importance for the continuity of care ● A two-edged strategy for dealing with the media should be developed |
| Gersons and Carlier (1993a). Plane crash crisis intervention: A preliminary report from the Bijlmermeer, Amsterdam. (Scientific publication, C) |
Journal of Crisis Intervention and Suicide Prevention | ● Better interaction between intervention and research is required |
| Alwart et al. (1993). Rouw en rituelen na de vliegtuigramp. (Scientific publication, C) |
Maandblad Geestelijke Volksgezondheid | ● Respect local culture and rituals ● Allow for support other than solely professional health care |
| van Deursen et al. (1993). Kinderen na de ramp. Hulpverlening aan jeugdige slachtoffers van de Bijlmer-vliegramp. (Scientific publication, C) |
Maandblad Geestelijke Volksgezondheid | ● There were difficulties in organizing specialized care for large groups of children ● Collaboration with different stakeholders required logistic skills |
| de Jong and van Schaik (1994). Culturele en religieuze aspecten van rouw- en traumaverwerking naar aanleiding van de Bijlmerramp. (Scientific publication, B:8) |
Tijdschrift voor Psychiatrie | ● Rituals in foreign cultures can be different and should be integrated in normal support routines |
| Carlier et al. (1995). De Bijlmermeervliegramp: Een vervolgonderzoek naar de lange termijn psychische gevolgen en de nazorg bij getroffenen. (Research report, A:1) |
Academic Medical Center Amsterdam | ● Information dissemination towards affected persons is insufficient ● Organize a central information hub ● Organize long-term monitoring of the recovery ● Facilitate continuity of care for specialized psychosocial services ● Facilitate group gatherings with bereaved |
| Carlier (1996). Studiedag Hulp bij rampen en calamiteiten; je kan er beter op voorbereid zijn! Aanbevelingen naar aanleiding van de Bijlmerramp. (Presentation, A:3,4) |
Amsterdam Medical Center Amsterdam | ● 1.5 years after disaster, much psychological disturbance has faded away ● Significant number of people require specialized mental health care ● Specialized mental health care is offered for too short a period of time ● Create a one-stop shop ● Organize quality check for acute support ● Organize information alignment between caregivers |
| Carlier and Gersons (1997). Stress reactions in disaster victims following the Bijlmermeer plane crash. (Peer-reviewed scientific publication, A:4) |
Journal of Traumatic Stress | ● A proportion of the people affected recover from (acute) PTSD within 6 months without professional help |
| Meijer et al. (1999). Een beladen vlucht. (Evaluation report, B:5,7) |
Parlementaire Enquêtecommissie Bijlmerramp | ● Organize a central information hub ● Organization of the government during the long-term recovery is fragmented and compartmentalized ● Discard rumours and give correct information ● Delegate responsibilities for the recovery |
| Coebergh (1999). Zorg voor de volksgezondheid na de vliegtuigramp in de Bijlmermeer; de beladen nasleep. (Scientific publication, C) |
Nederlands Tijdschrift voor de Geneeskunde | ● Long-term follow-up of affected persons is required |
| KLM Arbo Services (1999). Protocol 1. Individueel medisch onderzoek. Medisch onderzoek Vliegramp Bijlmermeer. (Research report, A:3) |
KLM Arbo Services | ● Internal and external alignment of parties involved in health research is required |
| Gersons et al. (2000). ‘In de Spiegel der emoties’. Onvoorziene langetermijngevolgen van de Bijlmervliegramp. (Scientific publication, B:8) |
Maandblad Geestelijke Volksgezondheid | ● A one-stop shop should be organized ● Financial aid is required for affected persons ● Protocoled treatment for affected persons with psychological complaints is required |
| Boin et al. (2001). Toxic fear: the management of uncertainty in the wake of the Amsterdam air crash. (Peer-reviewed scientific publication, B:7) |
Journal of Hazardous Materials | ● Certain human-made or technological disasters have different, some say more severe, consequences for the various categories of affected people than natural disasters may have. The fear of the unknown and the possible toxic substances that are (probably) involved form the basis for these severe consequences ● Long-term psychosocial impacts of a disaster are affected not only by victim characteristics but also by patterns of aid distribution and access to that aid ● After a disastrous situation has occurred, authorities should initiate a well-staffed information unit that can function for quite some time (years on end if necessary). This unit can be the intermediary organization, the link between different groups of victims and the many organizations working on all aspects of material and immaterial aftercare ● Authorities should stimulate, if not facilitate, the forming of self-help organizations ● Crisis managers should keep the longer term in mind while dealing with immediate and pressing problems. Only if crisis managers become aware of the potential problems that may arise during the aftermath can the disaster after the disaster be averted |
| Carlier, Sijbrandij, Meijer, and Gersons (2001). De late hulpverlening voor posttraumatische stressklachten bij getroffenen van de bijlmermeer vliegramp. (Evaluation report, A:4) |
AMC/De Meren | ● Treatment of psychological problems in the aftermath of disasters should be offered in a broad spectrum of health-care interventions ● Lessons learned should be used in dealing with future disasters |
| Yzermans and Gersons (2002). The chaotic aftermath of an air plane crash in Amsterdam. A second disaster. (Book chapter, C) |
Kluwer Academic | ● It is important to inform the affected about all available services (victim and peer support), e.g. in a leaflet ● It is very important to have a central advice and information point that should be operational for several years ● Long-term monitoring of aftercare provision is essential ● It is also important to monitor (developments in) health problems, preferably using existing registration systems and databases ● Treatment has been too brief and too discontinuous to achieve a satisfactory outcome ● Ineffective and/or disconnected responses by authorities lead to chronic stress-related health problems |
| van Hemert and Smeets (2004). Evaluatie van de nazorg na het Individueel Medisch Onderzoek Vliegramp Bijlmermeer – Evaluatieverslag. (Evaluation report, A:1) |
Academic Medical Center Leiden | ● Organize coordination of accessible care ● Support should be continued long after the disaster ● Facilitate group gatherings with bereaved |
| Verschuur et al. (2004a). Medisch onderzoek Vliegramp Bijlmermeer. (Summary, A:3) |
Academic Medical Center Leiden | ● Health research and post-disaster PSS should be integrated ● MUPS (Medically Unexplained Physical Symptoms) play an extensive role during post-disaster PSS |
| Verschuur et al. (2004b). Het effect van het Medisch Onderzoek Vliegramp Bijlmermeer op de gezondheidsbeleving van bewoners en hulpverleners ruim acht jaar na de Vliegramp Bijlmermeer. (Research report, A:3) |
Academic Medical Center Leiden | ● Health research after disasters is delicate and should only be implemented if there is a direct need |
| Witteveen (2006). The long-term aftermath of the Amsterdam air disaster: psychological wellbeing of professionally involved rescue workers. (Dissertation, A:3) |
Free University Amsterdam | ● Organizations of fire-fighters and police officers should be aware of potential long-term adverse effects of disaster exposure on psychological well-being and its risk factors ● Provide access to adequate aftercare even many years after occupational involvement in such a unique event as an air disaster ● It is important for organizations to be aware of additional chronic job stressors and negative life events |
| Verschuur (2009). Effects of the medical investigation Bijlmermeer aviation disaster on health perception of residents and rescue workers. (Dissertation, A:3) |
Leiden University | ● Participation in post-disaster health research has a negative effect on health ● Stepped care models, which start with monitoring of health and increasingly offer more intense care and support according to the severity and progression of complaints, seem appropriate |
| Faro aeroplane crash (event type: aeroplane crash) | ||
| Noordegraaf et al. (1993). De opvang en behandeling van 14 slachtoffers van het vliegtuigongeval in Faro, Portugal, in het calamiteitenhospitaal Utrecht van 23 tot en met 29 december 1992. (Evaluation report, C) |
Rijksinstituut voor Volksgezondheid en Milieu | ● Reunification with family should be handled with great care |
| van Duin, Overdijk, and Wijkhuijs (1998a). Faro gevolgen enquête 1. (Research report, A:1) |
Crisis Onderzoek Team Leiden | ● Organizational problems increased the impact of the disaster ● Media contributed to wrong meaning-making ● Government played little to no role in the recovery |
| van Duin, Overdijk, and Wijkhuijs (1998b). Faro gevolgen enquête 2. (Research report, A:1) |
Crisis Onderzoek Team Leiden | ● Long financial and legal procedures give way to feelings of anger |
| Klerx van Mierlo (2009). Faro gevolgen enquête 3. (Research report, A:1) |
Intervict | ● Organizations showed little recognition of the problems of affected persons ● Financial procedures are experienced very negatively |
| Legionella outbreak Bovenkarspel (event type: infectious disease) | ||
| Crisis Onderzoeksteam (1999). De uitbraak van de veteranenziekte te Bovenkarspel: Een evaluatie van de epidemiebestrijding. (Evaluation report, B:7) |
Crisis Onderzoek Team Leiden | ● Organization of recovery was not embedded in governmental organization ● Contents of recovery were influenced by the Bijlmer aeroplane disaster ● Government has a facilitating and monitoring role during recovery, complementary to existing structures |
| van der Velden and Kleber (2000). Gezondheid en nazorg getroffenen legionella epidemie. (Research report, A:2) |
Instituut voor Psychotrauma | ● Greater access to care improved affected persons’ opinions of quality of care |
| Fireworks explosion Enschede (event type: explosion) | ||
| Broekman (2000). Na de vuurwerkramp: Peiling werkdruk en ondersteuningsbehoefte Huisartsen Enschede. (Research report, A:1) |
Coördinatie Commissie Vuurwerkramp | ● Disasters put pressure on existing capacities ● Organize support for local GPs to work with disaster-specific problems |
| Slis (2000). Gebruik van communicatiemiddelen in relatie tot de vuurwerkramp. Stadspeiling najaar 2000. (Research report, A:1) |
I&O Research | ● Only a small percentage of the inhabitants of Enschede used the one-stop shop |
| Inspectie voor de Gezondheidszorg (2001a). Onderzoek vuurwerkramp Enschede. Rapportage geneeskundige hulpverlening getroffenen vuurwerkramp Enschede. (Evaluation report, C) |
Inspectie voor de Gezondheidszorg | ● The Health Council of the Netherlands should issue an advisory report on the content of psychosocial aftercare in the event of accidents and disasters ● The policy of the mental health care institution, social work institutions and GPs after a disaster like this should be clear to everyone, especially concerning the accessibility of specialized professional mental health care assistance ● All mental health care institutions that can be involved in the aftercare of a disaster must have guidelines for mental health care staff for supporting affected people and debriefing of emergency service providers ● The content of these guidelines must be regularly updated in line with latest insights |
| Groen et al. (2001). Sociale wederopbouw na de vuurwerkramp. Eerste peiling voortgang maatregelen. (Evaluation report, B:5,6) |
DSP | ● Shortly after the disaster, residents and affected people were insufficiently informed, including about victims and property, which led to a great deal of uncertainty ● The registration of missing persons took a very long time, and it was not clear why ● In many cases, affected people assess their own circumstances and prospects before and after the disaster differently from, for example, an insurance agent, an alderman or a social worker, and may feel short-changed by them ● The times when the (legal) responsibilities of authorities and service providers begin and end are seldom laid down unequivocally and can remain unclear for the people affected |
| van Kamp and van der Velden (2001). Vuurwerkramp Enschede: Lichamelijke en geestelijke gezondheid en ervaringen met de ramp: rapportage van het gezondheidsonderzoek. (Research report, A:2) |
Rijksinstituut voor Volksgezondheid en Milieu | ● The current study was a result of recommendations from the Bijlmer evaluations ● 2–3 weeks after the disaster, a significant part of the population showed severe mental health problems |
| Informatieen Adviescentrum (2001). Jaarverslag 2000. (Year report, D) |
IAC Enschede | ● The one-stop shop was the result of Bijlmer advice ● Registration of affected persons and their needs was a challenge ● Primary phase of the one-stop shop was characterized by chaos and pragmatism ● Needs of affected persons differed over time |
| Oosting et al. (2001). De vuurwerkramp. Eindrapport. (Evaluation report, B:5,7). |
Commissie Onderzoek Vuurwerkramp | ● Although a draft PSS plan for disasters and major events is available locally at the time of the disaster, it is not known to organizations. This contributed to the inadequate coordination of aftercare in the reception halls and aftercare during the first days ● The coordination of the response needs to be improved. It is important to make a proper division of tasks between municipal health services, mental health services and social work, and to specify the roles and positions of the professionals involved ● The stratified organization of services resulted in a situation where heavily traumatized people were assessed by volunteers and care providers with little or no experience. A stronger representation of specialized care providers in reception halls could have prevented these problems ● The Ministry of Health provides funding for the implementation of a coordinated care plan with a follow-up period of 5 years. The Commission finds the initiative to achieve coordinated aftercare particularly valuable and is positive about the rapid support provided by the ministry. The implementation can be improved, which can be traced back partly to the concept stage of the psychosocial planning and local unfamiliarity. The extra human resources and specific knowledge brought in have had a positive effect on the organization of the aftercare ● In general, participants in the evaluation survey were very satisfied about psychosocial services provided. However, a number of affected people with a Turkish background expressed a need for psychosocial care providers with whom they can communicate in their own language: according to them, treatment through interpreters leads to significant problems ● The Commission considers it important that sufficient service capacity is available in the longer term to perform the extra work as a result of the fireworks disaster ● Concerning the schools, the Commission has great appreciation for the well-planned assistance to affected pupils, parents, teachers and the school leaders involved, shaped in cooperation with the municipality ● The municipality was successful on many fronts from the start in offering affected people adequate help; given the circumstances in which the municipality had to operate, the Commission considers this an extraordinary achievement ● The municipal administration has also indicated its openness to criticism of its performance with respect to practical assistance; in the first place, this may occur when the cause of the disaster is (partly) ascribed to the government, which the people might have expected could have fully guaranteed the safety of the citizens. In a situation such as this, assistance from the government will partly have the character of repair of affected trust; it is absolutely essential for citizens to trust the accuracy of the information issued to them by the municipality ● The ‘caring government’ objective is ambitious, not in the least because it will have to be maintained over a long period of time, even when a return to the order of the day has long been accomplished ● Making arrangements alone is not sufficient: their implementation must be guaranteed ● The great importance of proper information, available on time to anyone whom it concerns, has already become apparent from both other parts of the investigation; this is no different for the provision of practical assistance: on this point, the registration of affected people was clearly problematic |
| Informatie en Adviescentrum (2002). Jaarverslag 2001. (Year report, D) |
IAC Enschede | ● Full and adequate reimbursement is a prerequisite for recovery ● The function of a one-stop shop is highly dependent on an external network |
| Informatie en Adviescentrum (2003a). Jaarverslag 2002. (Year report, D) |
IAC Enschede | ● It is difficult to gather, save and disseminate disaster-related information ● The one-stop shop experienced difficulties in taking a governing (directing) role |
| Informatie en Adviescentrum (2003c). Informatie – en adviescentrum – Vuurwerkramp Enschede mei 2000 – juni 2003 – Eindevaluatie. (Evaluation report, C) |
IAC Enschede | ● The one-stop shop should have a formal governing role in post-disaster PSS ● A national registration format for the registration of affected persons should be developed ● Prepare for financial reimbursement after disasters ● Combine all lessons learned in one manual and develop national policy on recovery |
| Informatie en Adviescentrum (2003b). Informatie en adviescentrum Vuurwerkramp Enschede mei 2000 – juni 2003 – Eindrapportage. (Final report, D) |
IAC Enschede | ● The one-stop shop played an important role in organizing PSS ● A national knowledge centre for PSS after disasters was created ● A manual one-stop shop was created |
| Drogendijk et al. (2004). Leidende en misleidende verwachtingen. Een kwalitatief onderzoek onder Turkse getroffenen van de vuurwerkramp Enschede omtrent de psychosociale nazorg. (Research report, B:5) |
Instituut voor Psychotrauma | ● Immigrants affected by the disaster had a high level of complaints, yet made little use of specialist mental health care ● Turkish immigrants request help when mental health problems become a burden for the social environment ● Lack of knowledge about health care prevents access to care |
| Gersons, Huijsman-Rubingh, and Olff (2004). De psychosociale zorg na de vuurwerkramp in Enschede; lessen van de Bijlmer-vliegramp. (Scientific publication, C) |
Nederlands Tijdschrift voor Geneeskunde | ● In the design and implementation of the psychosocial care for those affected by the fireworks disaster in Enschede (2000), lessons were learned from the Bijlmer air disaster (1992) |
| Drogendijk, van der Velden, Boeije, Gersons, and Kleber (2005). De ramp heeft ons leven verwoest. De psychosociale weerslag van de vuurwerkramp Enschede op Turkse getroffenen. (Scientific publication, B:5) |
Medische Antropologie | ● Mental problems were often mentioned first by Turkish immigrants, as opposed to somatic complaints ● Care relationships in families of Turkish migrants complicate their demand for care |
| van der Meijden et al. (2006) Gezondheidsmonitoring Getroffenen Vuurwerkramp Enschede (Research report, A:2) |
GGD regio Twente | ● Disaster health research should be prepared for ● Earlier disasters showed a need for long-term PSS ● Alignment between partners facilitating and executing health research is a requirement ● It is necessary to reflect on the positions of all involved parties and political sensitivities, preferably before disaster strikes ● Political reality and substantive reasoning can divert from what is needed |
| IJzermans, Dirkzwager, Kerssens, Cohen-Bendahan, and Ten Veen (). Gevolgen van de vuurwerkramp in Enschede voor de gezondheid. Eindrapport vande monitoring in de huisartspraktijken. (Research report, A:2) |
NIVEL | ● Quickly start with monitoring ● Monitoring of health problems should be a responsibility of GPs ● A facility should exist to harness knowledge on monitoring and registration |
| Soeteman (2009). Health problems of Enschede residents in the aftermath of the Fireworks Disaster. A longitudinal study with a pre-disaster assessment in general practice. (Dissertation, A:3) |
Radboud Universiteit Nijmegen | ● Disaster can have a great impact on second-line workers, such as GPs ● Affected people who had to relocate and who had a history of psychological problems were at risk of presenting post-disaster psychological and physical health problems ● Researchers and public health workers have to focus on interventions for some specific risk groups which can be easily traced in the medical records |
| Drogendijk (2012). Long-term psychosocial consequences for disaster affected persons belonging to ethnic minorities. (Dissertation, A,B:2,5) |
Arq Psychotrauma Expert Group | ● Results clearly indicate that differences in support between immigrants and Dutch natives are not so much a consequence of the disaster but were largely present before the disaster ● With regard to the more collectivist cultures with a very high degree of interdependence, information should be brought out in the collective arena |
| Bar fire Volendam (event type: fire) | ||
| Inspectie voor de Gezondheidszorg (2001b). Rapport evaluatie geneeskundige hulpverlening cafébrand nieuwjaarsnacht 2001. (Evaluation report, B:5,7) |
Inspectie voor de Gezondheidszorg | ● The emergency health (GHOR) policy section on reception and (psychosocial) care for people affected should be worked out in more detail (in terms of both procedure and content) ● The desirability and possibilities of (better) linking the Red Cross’s reception and care task to the GHOR assistance process should be explored ● The Volendam disaster showed that the relief chain is larger than the disaster site; the reception in hospitals as well as the reception of the population and the (psychosocial) aftercare are essential parts of the chain, and chain management (by the municipal health authorities) must also be aimed at ensuring this coherence ● Contingency plans should address the psychosocial reception of affected people, relatives and staff |
| Alders et al. (2001). Cafébrand Nieuwjaarsnacht – Publieksversie. (Evaluation report, B:5,7) |
Commissie Onderzoek Cafébrand Nieuwjaarsnacht | ● In the Commission’s opinion, municipalities of a similar size to Edam-Volendam do not have the necessary knowledge and expertise to adequately shape their preparations for disaster relief, making it equally predictable that, in an actual disaster situation, the demand for help will be greater than the supply ● The Commission therefore concludes that preparing for population care in disaster situations requires a consistent regional approach, especially for the benefit of smaller municipalities; for specific aspects, such as the preparation of an information number or support in the verification of lists of missing persons, well-prepared national support is desirable ● The Commission notes that the municipality did not play any role in the population, except for the deployment of a few individual civil servants during the first night ● The Commission concludes that the municipal emergency plan should have been deployed; then there could have been coordination of matters such as reception and care, registration of the affected and funeral services ● People involved were focused to such an extent on removal of wounded people that they started developing activities only when the need came to light ● The contingency plan, which was in force on 1 January 2001, was outdated and not elaborated in subplans and plans: tasks and responsibilities were not clearly defined ● The Commission concludes that the contingency plan did not meet the legal requirements and that the officials responsible for disasters were not trained, instructed or practised in the field |
| Inspectie voor de Gezondheidszorg (2003). Waakzaamheid blijft geboden. Een oriënterend onderzoek naar de hulpverlening bij psychische problemen na de cafébrand in Volendam. (Research report, B:5,7) |
Inspectie voor de Gezondheidszorg | ● The involvement of clients/beneficiaries in the provision of care should be improved ● A discussion must start between the care providers and institutions involved in the psychosocial and psychiatric assistance regarding the future organization of assistance, with an emphasis on the relationship between regular health services and specific disaster-related assistance ● Two years after the disaster, specialist research and the treatment of disaster-related psychological problems should be implemented in regular mental health care |
| Nuijen (2006). Nieuwjaarsbrand Volendam 2001. Lessen voor Later. (Evaluation report, C) |
CRN Het Anker | ● Organize national or provincial expertise for the organization of the first recovery ● Immediately after a disaster, bring together important actors ● Place an expert with disaster experience in a coordinator role above the group ● Health research should be planned and conducted from a central point in order to avoid overlap and to promote effectiveness and efficiency ● Start health screening and monitoring activities immediately after a disaster, calamity or other serious event ● Do not sideline the municipality during the recovery: it is the continuous factor; it is important that the municipal organization and the local administration are broadly involved ● Disaster exercises remain necessary, including administrative ones ● Stepped care is an important condition for efficient recovery ● Ensure transparency, integrity and coordination in the psychosocial field ● The development of a ‘gold standard’ for psychosocial aftercare in the event of disasters is indispensable: every disaster is different, and such a standard can therefore never be more than an intermediate product, always leaving room for adaptation to the specific disaster situation |
| Dorn et al. (2007). Gevolgen van de nieuwjaarsbrand in Volendam voor de gezondheid. Eindrapport van de monitoring in huisartsenpraktijken en apotheken. (Research report, A:3) |
NIVEL | ● After disasters, particularly those in which a community is affected, research using existing registrations (GPs and pharmacies, and possibly also company doctors, psychotherapists and social workers) is necessary ● In addition to studies utilizing existing registrations, studies should be conducted with (parts of) the affected population; shortly after the disaster, a limited questionnaire was used to record the exposure per individual; however, only after several months were those affected asked about self-reported health problems ● When conducting primary health research after a subsequent disaster, there should be a possibility of registering referrals and letters returning from specialists and other first-line care providers ● It is of great importance that monitoring in general practice be implemented soon after a disaster ● Those affected (and their families) should be registered as soon as possible ● It is sensible to carry out further research into the desired length of both monitoring and questionnaire research ‘in peacetime’; this work should include a meta-analysis of studies carried out, both cross-sectional and longitudinal, considering different types of research in different populations |
| Bird flu epidemic (event type: infectious disease) | ||
| Impact (2004a). Monitor organisatie psychosociale zorg n.a.v. Aviaire Influenza onder pluimvee. (Evaluation report, B:5,7) |
Impact | ● The organization of PSS at the onset of AI is diffuse; a large number of parties involved suffered from insufficient coordination and communication ● There is hardly any mention of the chain of psychosocial care for animal diseases ● By clearly allocating control, effectiveness and efficiency can increase; agreements on control, coordination and the role of regular care providers must be made in order to promote cooperation, effectiveness and efficiency ● Roadmaps and protocols are monodisciplinary in nature, while AI is a creeping crisis with a multidisciplinary character, involving humans and animals; the monodisciplinary manuals do not sufficiently reflect the multidisciplinary nature of animal diseases ● Previous animal diseases (classical swine fever and FMD) resulted in discussions about psychosocial care for farmers that led to several local initiatives and adjustments of procedures within the Ministry of Agriculture, Nature and Food Quality (LNV); the disasters in the Bijlmer, Enschede and Volendam contributed to a change in the PSS vision and approach ● The government has been given an emphatic role ● Ensure coordination between the local (LNV-related) networks on the one hand and the regular care providers on the other ● Use local networks to provide psychosocial care to farmers; strengthen them, map them out from the ministry, so that the connection between central management and local networks is properly established ● Ensure that the ministries of the LNV, health and the interiors develop a joint vision of psychosocial care in the event of animal diseases ● Clarify roles and responsibilities for aftercare in case of animal diseases (without disaster status) |
| Bosman et al. (2004). Vogelpest Epidemie 2003: gevolgen voor de volksgezondheid. (Research report, A,B:1,5,7,9) |
Rijksinstituut voor Volksgezondheid en Milieu | ● Earlier research among livestock farmers affected by the FMD crisis showed a great deal of dissatisfaction with the way in which they were treated during the culls; in the case of the bird flu epidemic, various authorities have therefore explicitly devoted a great deal of attention to this subject ● The improvement of communication and information provision compared to FMD, and improved contact with those involved in the depopulation operations, was achieved by setting up a regional information centre, an office of the Ministry of Agriculture and a telephone assistance service for farmers, among other things ● In general, the provision of information went well; there is, however, still room for improvement in the provision of correct information on depopulation |
| Impact (2004b). Samenvattingen rapporten en monitor Aviaire influenza. (Conference report, D) |
Impact | ● The model used for the supervision of affected poultry farmers, communication and treatment during depopulation is a starting point for future crises ● Mutual coordination between the various emergency services is a subject for attention ● The Ministry of Agriculture must consider socio-emotional and psychosocial problems that can arise as a result of the outbreak of an animal disease crisis and must assume its responsibility in this respect; the extent to which this responsibility for providing guidance and assistance extends, during and after the crisis, is not yet clearly visible, particularly in the area of aftercare, and no policy has yet been formulated in this respect ● In order to offer appropriate socio-emotional counselling and PSS, the desired support chain needs to be thought through: What does it look like? Who sets the chain in motion? What is appropriate for the farmer, his/her family and for the Ministry of Agriculture? ● In order to fill gaps and shortcomings, guidance can be provided with a chapter on PSS, policy-making and administrative processes can be improved, and it is recommended to adapt implementation plans in relevant areas with concrete actions ● The plans for FMD and AI are very different in structure and nature, with the FMD roadmap offering better starting points for PSS ● Be open and communicate intentions and changes/adaptations by government ● Structural attention should be given to psychosocial aspects ● Recognize, support and use existing local and regional networks of assistance, expertise and services ● Restore trust in the government by recognizing/acknowledging problems and ‘mistakes made’; by such gestures from the government, those involved are taken seriously |
| Q-fever outbreak (event type: infectious disease) | ||
| van Dijk et al. (2010). Van verwerping tot verheffing. Q-koorts beleid in Nederland 2005–2010. (Evaluation report, B:5,7) |
Evaluatiecommissie Q-koorts | ● On several occasions relevant information, e.g. about the occurrence of human Q-fever cases in association with dairy goats in 2005 and 2006, appeared to have been insufficiently communicated, both between and within the organizations involved; consequently, the Q-fever outbreak in 2007 was considered a one-off event, apart from the occurrence of Q-fever outbreaks in dairy goats already in 2005 and 2006, and as a result, the urgency of the situation in 2007 was not sufficiently recognized |
| Jeeninga et al. (2010). Q-koortsbestrijding door de GGD; evalueren en leren. (B:5,6,7) |
Infectieziekten Bulletin | ● In anticipation of the next outbreak, the municipal health services will draw up a proactive, strategic communication plan based on advancing insight and changing measures ● Politically sensitive questions and topics should preferably be dealt with by one and the same spokesperson on behalf of the municipal health services |
| van der Velden, Dusseldorp, Drogendijk, and van Overveld (2011). Q-koorts – ruimingen van besmette bedrijven. Evaluatieonderzoek onder geitenhouders. (Research report, A:1) |
Rijksinstituut voor Volksgezondheid en Milieu | ● The financial situation is a (continuous) source of stress in the event of this animal disease crisis. This is also evident in the question of what is of most concern to those affected ● Almost one in five of those affected indicated that he or she needed professional help in the past 12 months because of psychological problems, tensions or the use of alcohol or drugs, but that he or she did not go to a doctor or other counsellor ● It should be noted that the effect of psychological help may be limited if concerns about the financial situation remain |
| van der Bijl et al. (2012). Het spijt mij. Over Q-koorts en de menselijke maat. (Evaluation report, B:5,7) |
De Nationale Ombudsman | ● The National Ombudsman is of the opinion that the government has not been sufficiently open and clear in actively providing information to the citizens, and by not doing so, it has even contributed to tensions in society; the National Ombudsman does not consider this to be adequate ● The government did not pay enough attention to the citizens during the Q-fever epidemic; it has not studied the needs of citizens during the epidemic ● The government and the citizens did not join forces to tackle the issue of the uncertainty associated with Q fever. The National Ombudsman is of the opinion that the government has not acted responsibly towards its citizens because it did not actively involve them in its actions ● The National Ombudsman is of the opinion that the government is insufficiently involved and acted in a solution-oriented manner by focusing for too long on certainty and obvious evidence of transferability of the bacterium; in doing so, the government failed to act expeditiously and the National Ombudsman does not consider this to be adequate ● The National Ombudsman recommends that the Minister of Health, Welfare and Sport and the State Secretary for Agriculture create a support centre where Q-fever patients and other parties involved can obtain information, advice and support with regard to social, care-related and financial problems in relation to Q fever ● The National Ombudsman asked the Minister and State Secretary to coordinate the practical implementation and possibilities of the support centre together with Foundation “Q-uestion” |
| Poldercrash Haarlemmermeer (event type: aeroplane crash) | ||
| Inspectie Openbare Orde en Veiligheid (2009). Poldercrash 25 februari 2009. Een onderzoek door de Inspectie van Openbare Orde en Veiligheid, in samenwerking met de Inspectie voor de Gezondheidszorg. (Evaluation report, B:5,7) |
Inspectie Openbare Orde en Veiligheid | ● In the roadmap of the registration and information process (CRIB), the roles, tasks and responsibilities of everyone who contributes to CRIB need to be specified ● Include not only the municipality but also the (military) police and emergency health, and secure the plan within the organizations by means of multidisciplinary training and practice ● Coordinate all activities linked to the registration of the affected and relatives (injury cards, people at the reception location, family registration, passenger lists, etc.) ● The tasks of the disaster relief organization in a mass casualty incident also include the reception of relatives; during the planning, how this reception will be organized and which parties have a role to play in this must be described (also pay attention to the provision of information to relatives of fatalities and ensure that those who are given this responsibility are adequately trained) ● An early sketch of a ‘broad’ plan of action for the recovery phase has proved its worth for the Poldercrash; the safety inspection considers the way in which the municipality of Haarlemmermeer has performed in the aftermath as a ‘good practice’ that deserves to be embedded in municipal planning |
| Veiligheidsregio Kennemerland (2009a). Vaststellen Plan van Aanpak Nafase verongelukte vliegtuig Turkish Airlines (TK1951). (Action plan, D) |
Veiligheidsregio Kennemerland | ● Already during the acute phase, the municipality identified the likely character of the aftercare phase ● On the day of the crash, work was carried out to draft a first plan of action for the aftercare phase, and frameworks were worked out on the second day in a subgroup of the ‘Recovery project group’, serving as input for subsequent decision making |
| Veiligheidsregio Kennemerland (2009b). Reactie rapportageonderzoek vliegtuigongeval d.d. 25 februari 2009 |
Veiligheidsregio Kennemerland | ● The crisis organization in the Netherlands is not properly geared to the role and impact of new media (SMS, YouTube, Twitter, Internet, etc.) ● The names of the deceased were published within 48 hours; nevertheless, we see a tension in the extremely careful working method, based on international agreements, between forensics and the need of potential surviving relatives to obtain clarity as soon as possible ● In practice, registering, locating and following up on people affected after the aircraft accident turned out to be more complex than exercises had shown; at first glance, this seems to have been caused, among other things, by an incorrect passenger list and a high degree of self-reliance on the part of the affected, supported by civilian emergency services, and cooperation between the services concerned has proven to be complex in practice |
| Gouweloos and Den Brinke (2013). Bevindingen getroffenen Poldercrash. Resultaten van drie belrondes onder getroffenen van het vliegtuigongeluk met de TK 1951 op 25 februari 2009. (Research report, A:4) |
Impact | ● This does not alter the fact that 3.5 years after the Poldercrash, a considerable number of those affected still have complaints, and there is also a need for additional assistance ● 35 of the 56 people affected who were interviewed during the third round were advised to seek help, based on their level of complaints and their own needs ● The telephone rounds offer a way to identify a need for additional assistance and to provide immediate information and advice ● In general, this method of working is also well appreciated by those affected |
| Tripoli air crash (event type: aeroplane crash) | ||
| de Boer and van der Heide (2010). Landelijke aanpak nazorg vliegramp Tripoli. (Popular publication, C) |
Magazine Nationale Veiligheid en Crisisbeheersing | ● Identification and registration of the people aboard the plane is challenging, resulting in high levels of insecurity in the next of kin |
| Impact (2012). Eindrapportage IVC Vliegramp Tripoli. (Evaluation report, A:1) |
Impact | ● Based on the user analysis, the opinions of the respondents to the survey, experts from the field and the participating organizations in the online one-stop shop website (IVC Vliegramp Tripoli or IVC), it can be concluded that the IVC mainly had a function for the next of kin of the aircraft accident in Tripoli ● When it comes to these various parties involved, it seems likely that, especially in the first weeks after the aircraft accident, there is a need to know more about the practical, material, mental and legal aspects of the aircraft accident; this need does not seem to be as great in the period that follows ● For those affected, it can be of great (symbolic) significance that the (national) government attaches itself to such an IVC as an instrument for recovery because it indicates that the government recognizes the next of kin in their roles as disaster victims ● By doing so, the (national) government is also sending out a signal that it considers it important for those affected to receive adequate support in the adjustment process for a longer period of time ● Also, by doing so, the (national) government communicates to those affected that the information available on the site is reliable, preventing those affected from being sucked along in a rumour stream that often occurs after disasters ● From the process evaluation, it can be concluded that the initiative and elaboration were seen as positive but that improvements can still be made in the areas of cooperation and communication ● The most important recommendation is to actively use the IVC with an open area, and especially a closed area, as a fully fledged policy instrument for aftercare for groups of people affected after a subsequent emergency ● In the future, it will be important to have an interactive format for such an IVC available that can be put online quickly, considers the nature and particularities of a disaster and can respond to ‘couleur locale’ ● Broad support from the organizations directly involved and the (national) government is required for an effective joint approach so that a dynamic and interactive IVC can be brought to the air quickly after a disaster or calamity ● In order to improve communication and the division of tasks between the various parties involved, and to streamline the process, it is necessary to make clear agreements in advance ● Clear job descriptions, management and transparent financial accountability create clarity and professionalism |
| Alphen aan den Rijn shooting (event type: shooting) | ||
| Inspectie Openbare Orde en Veiligheid (2011). Schietincident in ‘De Ridderhof’ Alphen a/d Rijn. (Evaluation report, B:5,7) |
Inspectie Openbare Orde en Veiligheid | ● Complete the implementation of the municipal crisis processes as soon as possible ● Pay special attention to the citizen support (bevolkingszorg) team, the organization of crisis communication and the supporting processes ● In the very near future, make effective agreements on the circumstances in which information about affected people can be shared, with due observance of the law and regulations ● In carrying out this process, several organizations are involved that each operate on the basis of a more or less independent role, which appears to be a bottleneck in the reception of the affected, forcing the police, the municipality and third parties to take on this specialized form of assistance and do so to the best of their ability in a hectic situation ● After the response organization has become operational, an intensive collaboration with the municipality is established in which PSS plays an important role during aftercare ● Within the crisis management organization, there is a differentiation in tasks, responsibilities and powers between authorities responsible for registration of the affected; agreements made in this respect do not appear to be known within the entire organization, creating misunderstanding in addressing problems during the verification of deceased and injured citizens |
| Laurier et al. (2013). Over napijn en nazorg. Eindverslag van de onafhankelijke adviescommissie nazorg schietincident Alphen aan den Rijn. (Evaluation report, B:5,7) |
Onafhankelijke adviescommissie nazorg schietincident Alpen aan den Rijn | ● Organize the aftercare on the basis of the recovery formats and manuals, and deal with this in a systematic and structured manner until the end of the aftercare ● The appreciation of those involved with regard to the aftercare depends on the end result ● Make it clear as a municipality how the project organization and the regular line organization relate to each other ● Ensure good documentation and archiving, and keep them in place until the ‘end’ ● Realize the integrated, mutual influence of the medical, psychosocial and material (practical/legal) problems of those involved, and apply case management to the most vulnerable among those affected ● Work with a broad definition of affected people (also, people who are indirectly involved can suffer serious consequences of a disaster or incident over many years) ● As a municipality, be outreaching in the contacts with those directly involved ● Consider the context and history, at both individual and aggregated levels (shopping centre, district, municipality, specific target groups) ● Assume that the effects of a disaster or incident can last for years and are current for those involved at all times ● Do not leave any possibility for interpretation with regard to the role, responsibilities and tasks of the municipality ● Provide education and training within the organization in the area of aftercare after disasters and incidents |
| van Duin et al. (2012). Lessen in crisisbeheersing. Dilemma’s uit het schietdrama in Alphen aan den Rijn. (Book, B:5,7) |
Boom Lemma Uitgevers | ● More needs to be done to communicate the time that is thought to be needed for the identification and recovery of fatalities, both to those responsible for the administration and to the outside world; choices made in this respect should be made more explicit ● The interests of the next of kin must be considered explicitly ● The fact that there is a covenant between safety regions and hospitals does not guarantee that those who become involved in a specific situation are aware of the agreements in question, or that they follow them: making people known does not automatically mean that they are becoming known ● Business care for special situations, in which many times more people are involved than after more regular situations, should be based on the strength and patterns of more normal situations but also deserves special attention ● The scale and intensity of a crisis such as the shooting in Alphen aan den Rijn (or the riots in Hoek van Holland) require extra capacity, support and organization, and in particular, a person who maintains an overview of roles and tasks |
| Tielen, van de Laar, and van Dijk (2012). Schietincident 9 april 2011 Alphen aan den Rijn. Onderzoek naar de gevolgen voor de gezondheid van de getroffenen en betrokkenen. (Research report, A:1) |
GGD Hollands Midden | ● The majority of the meetings organized by the municipality made a positive contribution to the handling of the incident ● Respondents’ health-care utilization after the shooting is relatively high compared to the general population ● The respondents with ‘less good’ experiences had contact with a care provider after the event: the majority have been in contact with victim support, but half of them also visited the GP and the psychologist or psychiatrist ● The respondents ‘going well’ have (much) less contact with each other or with a care provider but more contact with victim support |
| MH17 air crash (event type: aeroplane crash) | ||
| Joustra, Muller, and van Asselt (2015). MH17. Passagiersinformatie. (Evaluation report, B:5,7) |
Onderzoeksraad voor de Veiligheid | ● The surviving relatives of the Dutch victims of the MH17 disaster had to wait unnecessarily long for clarity about the presence of their relatives on the aircraft because the passenger information available immediately after the disaster did not offer sufficient guidance to enable the next of kin to confirm that their relatives were on the aircraft ● The Dutch crisis organization was insufficiently prepared for such a situation and there was a lack of direction and coordination in the information process ● The fact that the Ministry of Security and Justice (in particular the National Coordinator for Counterterrorism and Security) did not take control and that the Ministry of Foreign Affairs did not seek sufficient coordination with other parties involved meant that information gathered by various parties about the people on the plane and their surviving relatives was not brought together; as a result, it took a long time before the correct information was available to inform the next of kin |
| Saan, Bollen, and Kunst (2015). Het werk van de familierechercheur: een bron van stress of een bron van persoonlijke groei? (Scientific publication, B:5) |
Process | ● The results also show that the function of the family liaison officer is still in development ● Major differences can be seen in both the presence and the interpretation of basic tasks ● At the moment, there is no uniform national method of working |
| Torenvlied et al. (2015). Rapport evaluatie nationale crisisbeheersingsorganisatie vlucht MH17. (Evaluation report, B:5,7) |
Universiteit Twente | ● Because there was too little focus on cooperation and coordination between the national crisis management organization and other organizations, activities for the provision of information and aftercare to relatives were not properly coordinated; as a result, the next of kin were negative about their initial contacts with the central government ● The next of kin were generally satisfied with the aftercare provided by central governmental organizations, in cooperation with crisis partners; ● The actions of the family liaison officers, as a link with the crisis management organization, have been experienced by all the next of kin as essential and extremely valuable for aftercare in the broadest sense of the word ● The national organization of police liaison officers and the forensic detectives were not properly embedded in the national crisis management organization ● In the provision of aftercare to the next of kin, there was sometimes a lack of coordination between the activities of organizations: tasks of family liaison officers, victim support and municipal services ● Aftercare for employees involved in crisis management varied and was not always adequately organized ● Remarkably enough, aftercare for governmental staff is not regulated |
| Te Brake and Schaap (2017). Eindrapportage Informatie- en Verwijscentrum Vliegramp Oekraïne. Evaluatie onder gebruikers en betrokken partijen. (Evaluation report, A,B:1,5,6,10) |
Impact | ● After a disaster or large-scale crisis, an information and advice centre (one-stop shop) should be set up, in this case a website ● Maintain the digital centre, the IVC, as a reliable source of information and archive for at least 2 years ● Provide for a house style that expresses the fact that the IVC is an independent concept, intended for next of kin, not linked to a single organization ● Facilitate contact with fellow bereaved, but meet the needs of those affected ● Practise in peacetime: develop a ‘basic IVC’ for various scenarios; keep contacts between involved partners warm, and discuss the division of roles between them |
| Te Brake (2016). Informatie- en Verwijscentrum Vliegramp Oekraïne. (Popular publication, A,B:1,5,6,10) |
Cogiscope | ● Contacts should preferably be established within and outside the IVC’s own circle, and the IVC can facilitate this ● The next of kin know how to find the IVC well and still visit it regularly one-and-a-half years after the start ● There is room for improvement in the communication about the functionalities; a great deal of information on the open area of the IVC, for example, is also available to people without a login code ● Most surviving relatives indicate that the IVC must remain available for about 2 years ● Parties involved see the IVC as a platform complementary to existing multidisciplinary services and as a portal for information and contact ● The division of roles between different parties in the IVC, with regard to the functioning of the IVC, should be clear as early as possible ● A roadmap and the possibility of ‘practising in peacetime’ would be a solution |
| Jong et al. (2016). Crisis leadership by mayors: a qualitative content analysis of newspapers and social media on the MH17 disaster. (Peer-reviewed scientific publication, B:7) |
Journal of Contingencies and Crisis Management | ● Mayors appear to have functioned on both public and private stages as the facilitators whose task is not only to manage the crisis but also to support the healing process from disaster to restoration ● Where ‘meaning-making’ and ‘remembering’ depart from a public dimension, the ‘listening ear’ and ‘support regarding practical issues’ are far more private, although interviews with family members elevate the private to the public sphere again |
| Torenvlied et al. (2016). Evaluatie nationale crisisbeheersingsorganisatie vlucht MH17. (Popular publication, B:5,7) |
Magazine Nationale Veiligheid en Crisisbeheersing | ● Surviving relatives are dissatisfied with initial reception and information; often they received no formal confirmation that loved ones were on board ● Positive turnaround of opinions of affected persons on governmental support after day of national mourning ● Family investigators are a great support, as are the royal family, ministers and mayors ● Sometimes problems were encountered during identification and transfer of the deceased |
| Giebels (2016). Communicatie met en nazorg aan nabestaanden. (Popular publication, B:5,7) |
Magazine Nationale Veiligheid en Crisisbeheersing | ● In general, the public response has been reviewed as positive ● It has also become clear that there are large individual differences in experience and appreciation among the next of kin ● On a number of points the next of kin are predominantly in agreement: they are predominantly very satisfied with the national ceremonies and the efforts and working methods of the family investigators, and the great personal involvement of ministers, members of the royal family and mayors has also been experienced as a great help by many surviving relatives ● On the other hand, there is collective dissatisfaction with the first reception; despite understanding of the response time required after a disaster, the next of kin interviewed experienced the first reception by the government as bad: not easily accessible, not very professional and unpleasant, and the lack of formal confirmation of the death of their loved ones is also frequently mentioned, which they would have liked to have |
| Gutteling and Torenvlied (2016). Informatievoorziening naar Tweede Kamer, media en samenleving. (Popular publication, B:5,7) |
Magazine Nationale Veiligheid en Crisisbeheersing | ● There was a high peak in the intensity of media and social media attention after the crash, decreasing after 3 weeks ● Later peaks correspond to important events ● A public survey showed that a large proportion of the Dutch citizens considered the day of national mourning impressive ● Despite the developing critical tone in the Lower House of Parliament and (social) media, 1 year after the MH17 disaster, a majority of the Dutch population was retrospectively satisfied to very satisfied with the information provided by the central government |
| Multiple disasters | ||
| Netten (2005). Cultuur sensitieve psychosociale zorg na rampen. Lessons learned and good practices. Psychosociale zorg aan getroffenen uit etnische groepen bij de Bijlmer vliegramp en Enschede vuurwerkramp. (Research report, B:5,7) |
Impact | ● The central theme of the lessons to draw concerning PSS for those affected originating from cultural groups can be summarized under the umbrella of communication problems ● These communication problems originate from differences in language and cultural backgrounds between those affected and social workers in professional institutions providing PSS |
| de Vries and Rooze (2008). Gezondheidsonderzoek na rampen in Nederland. Overzicht van resultaten en aanbevelingen van afgerond onderzoek. (Summary of research reports, D) |
Impact | ● It is desirable for close cooperation to be established between different services, such as addiction care, social services and somatic health care ● Ideally, this should take place within a single body so that integrated psychosocial care can be provided ● A supportive policy, not discriminating between psychological and physical health complaints, must be developed, attentive to the material and financial issues which can cause a lot of stress and tension ● Some authors recommend setting up a special interdisciplinary emergency team consisting of local emergency services and care providers ● Specialist post-disaster care needs to be available for a longer period of time, up to a number of years |
a A, quantitative; B, qualitative; C, unknown; D, irrelevant; 1, survey research; 2, cross-sectional; 3, longitudinal; 4, clinical/diagnostic interviews; 5, interviews; 6, focus groups; 7, document analysis; 8, observation; 9, biological data; 10, user data website.
GP, general practitioner; PSS, psychosocial support; PTSD, post-traumatic stress disorder; AI, avian influenza; FMD, foot-and-mouth disease.
Note
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- *Alders J. G. M., Belonje M. M., van den Berg A., ten Duis H. J., & Doelen A. (2001). Cafébrand Nieuwjaarsnacht – Publieksversie. Rotterdam: Phoenix & den Oudsten; Retrieved from http://nationaalbrandweerdocumentatiecentrum.nl/wp-content/uploads/2015/01/Publieksversie.pdf [Google Scholar]
- Alexander D. (2003). Towards the development of standards in emergency management training and education. Disaster Prevention and Management: an International Journal, 12(2), 113–39. [Google Scholar]
- *Alwart I., Macnack U., Pengel-Forst C., & Sarucco M. (1993). Rouw en rituelen na de vliegtuigramp. Maandblad Geestelijke Volksgezondheid, 48, 1056–1066. [Google Scholar]
- Ammerlaan K. (2009). Na de ramp: De rol van de overheid bij de (schade) afwikkeling van rampen vanuit een belangenperspectief van de slachtoffers (Doctoral dissertation). Universiteit van Tilburg, Tilburg: Retrieved from https://pure.uvt.nl/portal/en/publications/na-de-ramp(6f95b5b6-b3f7-4088-a29b-033ae651e058).html [Google Scholar]
- Ansell C., Boin A., & Keller A. (2010). Managing transboundary crises: Identifying the building blocks of an effective response system. Journal of Contingencies and Crisis Management, 18(4), 195–207. [Google Scholar]
- Arbo Service KLM. (1999). Protocol 1 Amsterdam: Author. [Google Scholar]
- Bannink D., & Ossewaarde R. (2012). Decentralization: New modes of governance and administrative responsibility. Administration & Society, 44(5), 595–624. [Google Scholar]
- Behbod B., Leonardi G., Motreff Y., Beck C. R., Yzermans J., Lebret E., … Close R. (2017). An international comparison of the instigation and design of health registers in the epidemiological response to major environmental health incidents. Journal of Public Health Management and Practice, 23(1), 20–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bisson J. I., Tavakoly B., Witteveen A. B., Ajdukovic D., Jehel L., Johansen V. J., & Olff M. (2010). TENTS guidelines: Development of post-disaster psychosocial care guidelines through a Delphi process. The British Journal of Psychiatry, 196(1), 69–74. [DOI] [PubMed] [Google Scholar]
- Boin A., & ‘t Hart P. (2003). Public leadership in times of crisis: Mission impossible? Public Administration Review, 63(5), 544–553. [Google Scholar]
- Boin A., ‘t Hart P., Stern E., & Sundelius B. (2016). The politics of crisis management: Public leadership under pressure. Cambridge: Cambridge University Press; Retrieved from http://www.cambridge.org/gb/academic/subjects/politics-international-relations/comparative-politics/politics-crisis-management-public-leadership-under-pressure-2nd-edition?format=PB&isbn=9781107544253 [Google Scholar]
- Boin A., & Bynander F. (2015). Explaining success and failure in crisis coordination. Geografiska Annaler: Series A, Physical Geography, 97(1), 123–135. [Google Scholar]
- *Boin A., van Duin M., & Heyse L. (2001). Toxic fear: The management of uncertainty in the wake of the Amsterdam air crash. Journal of Hazardous Materials, 88(2–3), 213–234. [DOI] [PubMed] [Google Scholar]
- Bonanno G. A., Brewin C. R., Kaniasty K., & La Greca A. M. L. (2010). Weighing the costs of disaster: Consequences, risks, and resilience in individuals, families, and communities. Psychological Science in the Public Interest, 11(1), 1–49. [DOI] [PubMed] [Google Scholar]
- *Bosman A., Mulder Y. M., de Leeuw J. R. J., Meijer A., Du Ry van Beest Holle M., Kamst R. A., & Ruijten M. W. M. M. (2004). Vogelpest Epidemie 2003: Gevolgen voor de volksgezondheid. Onderzoek naar risicofactoren, gezondheid, welbevinden, zorgbehoefte en preventieve maatregelen ten aanzien van pluimveehouders en personen betrokken bij de bestrijding van AI H7N7 epidemie in Nederland. Bilthoven: Rijksinstituut voor Volksgezondheid en Milieu; Retrieved from https://www.rivm.nl/bibliotheek/rapporten/630940001.pdf [Google Scholar]
- Brewin C. R., Andrews B., & Valentine J. D. (2000). Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology, 68(5), 748–766. [DOI] [PubMed] [Google Scholar]
- Britten N., Campbell R., Pope C., Donovan J., Morgan M., & Pill R. (2002). Using meta ethnography to synthesise qualitative research: A worked example. Journal of Health Services Research & Policy, 7(4), 209–215. [DOI] [PubMed] [Google Scholar]
- *Broekman H. (2000). Na de vuurwerkramp: Peiling werkdruk en ondersteuningsbehoefte Huisartsen Enschede. Enschede: Coördinatie Commissie Vuurwerkramp. [Google Scholar]
- Bruinooge P., Bitter R., Helsloot I., Dekker K., Stierhout J., & Langelaar J. (2012). Bevolkingszorg op orde 2.0: Eigentijdse bevolkingszorg, volgens afspraak. Den Haag: Veiligheidsberaad. [Google Scholar]
- Campbell R., Pound P., Morgan M., Daker-White G., Britten N., Pill R., … Donovan J. (2012). Evaluating meta ethnography: Systematic analysis and synthesis of qualitative research. Health Technology Assessment, 15(43). doi: 10.3310/hta15430 [DOI] [PubMed] [Google Scholar]
- *Carlier I. V. E., Gersons B. P. R., & Uchelen J. J. (1993). De Bijlmermeer-vliegramp. Een onderzoek naar de psychische gevolgen bij getroffenen en hun commentaar op de geboden nazorg. Amsterdam: Academisch Medisch Centrum Amsterdam. [Google Scholar]
- *Carlier I. V. E., van Uchelen J. J., & Gersons B. P. R. (1995). De bijlmermeer-vliegramp. Een vervolgonderzoek naar de lange termijn psychische gevolgen en de nazorg bij getroffenen. Amsterdam: Academisch Medisch Centrum Amsterdam. [Google Scholar]
- *Carlier I. V. E. (1996). Studiedag hulp bij rampen en calamiteiten; je kan er beter op voorbereid zijn! Aanbevelingen naar aanleiding van de Bijlmerramp. Amsterdam: Academisch Medisch Centrum Amsterdam. [Google Scholar]
- *Carlier I. V. E., & Gersons B. P. R. (1997). Stress reactions in disaster victims following the Bijlmermeer plane crash. Journal of Traumatic Stress, 10(2), 329–335. [DOI] [PubMed] [Google Scholar]
- *Coebergh J. W. W. (1999). Zorg voor de volksgezondheid na de vliegtuigramp in de Bijlmermeer; de beladen nasleep. Nederlands Tijdschrift voor de Geneeskunde, 143(46), 2301–2305. [PubMed] [Google Scholar]
- *Carlier I. V. E., Sijbrandij E. M., Meijer J. E. M., & Gersons B. P. R. (2001). De late hulpverlening voor posttraumatische stressklachten bij getroffenen van de Bijlmermeer vliegramp. Amsterdam: AMC. [Google Scholar]
- Comfort L. K. (2007). Crisis management in hindsight: Cognition, communication, coordination, and control. Public Administration Review, 67(1), 189–197. [Google Scholar]
- *Crisis Onderzoeksteam (1999). De uitbraak van de veteranenziekte te Bovenkarspel: Een evaluatie van de epidemiebestrijding. Leiden: Author. [Google Scholar]
- D’Amour D., Ferrada-Videla M., San Martin Rodriguez L., & Beaulieu M. D. (2005). The conceptual basis for interprofessional collaboration: Core concepts and theoretical frameworks. Journal of Interprofessional Care, 19(1), 116–131. [DOI] [PubMed] [Google Scholar]
- de Bas M., Helsloot I., & Dückers M. L. A. (2017). De preparatie op de nafase binnen veiligheidsregio’s: Een verkennend onderzoek. Tijdschrift voor Veiligheid, 17, 3–16. Retrieved from http://postprint.nivel.nl/PPpp6607.pdf [Google Scholar]
- *de Jong J. T. V. M., & van Schaik M. M. (1994). Culturele en religieuze aspecten van rouw- en traumaverwerking naar aanleiding van de Bijlmerramp. Tijdschrift voor Psychiatrie, 4,293–303. [Google Scholar]
- *de Vries M., & Rooze M. W. (2008). Gezondheidsonderzoek na rampen in Nederland. Diemen: Impact. [Google Scholar]
- *de Boer W., & van der Heide A. (2010). Landelijke aanpak nazorg vliegramp Tripoli. Magazine Nationale Veiligheid en Crisisbeheersing, 8(3), 26–30. Retrieved from https://www.ifv.nl/kennisplein/wet-veiligheidsregios-wvr/nieuws/magazine-nationale-veiligheid-en-crisisbeheersing-mei-juni-2010-artikel-rampen-kennen-geen-grenzen [Google Scholar]
- Dieltjens T., Moonens I., van Praet K., de Buck E., & Vandekerckhove P. (2014). A systematic literature search on psychological first aid: Lack of evidence to develop guidelines. PloS one, 9(12), e114714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Drogendijk A. N., van der Velden P. G., Kleber R. J., & *Gersons B. P. R. (2004). Leidende en misleidende verwachtingen. Een kwalitatief onderzoek onder Turkse getroffenen van de vuurwerkramp Enschede omtrent de psychosociale nazorg. Zaltbommel: Instituut voor Psychotrauma (IVP). [Google Scholar]
- *Drogendijk A. N., van der Velden P. G., Boeije H. R., Gersons B. P. R., & Kleber R. J. (2005). De ramp heeft ons leven verwoest. De psychosociale weerslag van de vuurwerkramp Enschede op Turkse getroffenen. Medische Antropologie, 17(2), 217–232. [Google Scholar]
- *Dorn T., ten Veen P. M. H., & IJzermans C. J. (2007). Gevolgen van de nieuwjaarsbrand in Volendam voor de gezondheid. Eindrapport van de monitoring in huisartsenpraktijken en apotheken. Utrecht: NIVEL; Retrieved from https://www.nivel.nl/sites/all/modules/custom/wwwopac/adlib/publicationDetails.php?database=ChoicePublicat&priref=1001477&width=650&height=500&iframe=true [Google Scholar]
- *Drogendijk A. N. (2012). Long term psychosocial consequences for disaster affected persons belonging to ethnic minorities (Doctoral dissertation). Stichting Arq, Diemen. [Google Scholar]
- Dückers M. (2012). Richting geven aan de laatste schakel: De nafase. Rijksbrede versterking van herstel en nazorg bij rampen en crises. Den Haag: Ministerie van Veiligheid en Justitie. [Google Scholar]
- Dückers M. (2013). Lessen uit twintig jaar rampenhulpverlening: Berthold Gersons over zijn ervaringen bij de grootste rampen in Nederland. Cogiscope, 10(3), 20–25. [Google Scholar]
- Dückers M. (2015). In de werkkamer. In gesprek met René Stumpel, arts en directeur publieke gezondheid bij de GGD GHOR. Cogiscope, 12(4), 44–47. [Google Scholar]
- Dückers M. L. A., & Thormar S. B. (2015). Post-disaster psychosocial support and quality improvement: A conceptual framework for understanding and improving the quality of psychosocial support programs. Nursing & Health Sciences, 17(2), 159–165. [DOI] [PubMed] [Google Scholar]
- Dückers M. L. A., Thormar S. B., Juen B., Ajdukovic D., Newlove L., & Olff M. (2018). Measuring and modelling the quality of 40 post-disaster psychosocial support programmes. PLOS ONE, 13(2), e0193285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dückers M. L. A., Witteveen A. B., Bisson J. I., & Olff M. (2017). The association between disaster vulnerability and post-disaster psychosocial service delivery across Europe. Administration and Policy in Mental Health and Mental Health Services Research, 44(4), 470–479. [DOI] [PubMed] [Google Scholar]
- Dückers M. L. A., Yzermans C. J., Jong W., & Boin A. (2017). Psychosocial crisis management: the unexplored intersection of crisis leadership and psychosocial support. Risk, Hazards & Crisis in Public Policy, 8(2), 94–112. [Google Scholar]
- Dyb G., Jensen T. K., Nygaard E., Ekeberg Ø., Diseth T. H., Wentzel-Larsen T., & Thoresen S. (2014). Post-traumatic stress reactions in survivors of the 2011 massacre on Utøya Island, Norway. The British Journal of Psychiatry, 204(5), 361–367. [DOI] [PubMed] [Google Scholar]
- *Gersons B. P. R., & Carlier I. V. E. (1993a). Plane crash crisis intervention: A preliminary report from the Bijlmermeer, Amsterdam. Journal of Crisis Intervention and Suicide Prevention, 14, 109–116. [PubMed] [Google Scholar]
- *Gersons B. P. R., & Carlier I. V. E. (1993b). De Bijlmer-ramp: Crisisinterventie en consultatie. Maandblad Geestelijke Volksgezondheid, 10, 1043–1055. [Google Scholar]
- *Gersons B. P. R., Carlier I. V. E., & IJzermans C. J. J. M. (2000). “In de Spiegel der emoties”. Onvoorziene langetermijngevolgen van de Bijlmervliegramp. Maandblad Geestelijke Volksgezondheid, 55, 876–889. [Google Scholar]
- *Gersons B. P. R., Huijsman-Rubingh R. R. R., & Olff M. (2004). De psychosociale zorg na de vuurwerkramp in Enschede; lessen van de Bijlmer-vliegramp. Nederlands Tijdschrift voor Geneeskunde, 148(29), 1426–1430. [PubMed] [Google Scholar]
- *Giebels E. (2016). Communicatie met en nazorg aan nabestaanden. Magazine Nationale Veiligheid en Crisisbeheersing, 2, 10–11. [Google Scholar]
- Giel R. (1989). De psychosociale kant van rampen. Tijdschrift voor Psychiatrie, 3, 223–239. [Google Scholar]
- Goldman E., & Galea S. (2014). Mental health consequences of disaster. Annual Review of Public Health, 35, 169–183. [DOI] [PubMed] [Google Scholar]
- *Gouweloos J., & den Brinke T. (2013). Bevindingen getroffenen Poldercrash. Resultaten van drie belrondes onder getroffenen van het vliegtuigongeluk met de TK 1951 op 25 februari 2009. Diemen: Stichting Impact; Retrieved from https://www.ifv.nl/kennisplein/ghor-algemeen/publicaties/bevindingen-getroffenen-poldercrash-resultaten-van-drie-bellrondes [Google Scholar]
- Gouweloos J., Dückers M., Te Brake H., Kleber R., & Drogendijk A. (2014). Psychosocial care to affected citizens and communities in case of CBRN incidents: A systematic review. Environment International, 72, 46–65. [DOI] [PubMed] [Google Scholar]
- Grant M. J., & Booth A. (2009). A typology of reviews: An analysis of 14 review types and associated methodologies. Health Information & Libraries Journal, 26(2), 91–108. [DOI] [PubMed] [Google Scholar]
- Greenhalgh T., & Peacock R. (2005). Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. British Medical Journal, 331(7524), 1064–1065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Groen H., Koekkoek M., & Slump G. J. (2001). Sociale wederopbouw na de vuurwerkramp. Eerste peiling voortgang maatregelen. Amsterdam: DSP; Retrieved from https://publicaties.dsp-groep.nl/getFile.cfm?file=01_02_Sociale%20wederopbouw%20na%20de%20vuurwerkramp%20Eerste%20peiling%20voortgang%20maatregelen_02-20012.pdf&dir=rapport [Google Scholar]
- *Gutteling J., & Torenvlied R. (2016). Informatievoorziening naar de Tweede Kamer, media en samenleving. Magazine Nationale Veiligheid en Crisisbeheersing, 2, 12–13. [Google Scholar]
- Grievink L., van der Velden P. G., de Vries M., Mulder Y.M., & den Doel Smilde-van, D.A. (2006). Gezondheidsonderzoek na rampen: een inventarisatie van wensen en verwachtingen Bilthoven: RIVM. [Google Scholar]
- Haalboom A. F. (2017). Was de uitbraak van Q-koorts een verassing? Nederlands Tijdschrift voor Geneeskunde, 161(33), D1786. [PubMed] [Google Scholar]
- ‘t Hart P., Rosenthal U., & Kouzmin A. (1993). Crisis decision making: The centralization thesis revisited. Administration & Society, 25(1), 12–45. [Google Scholar]
- Hobfoll S. E., Watson P., Bell C. C., Bryant R. A., Brymer M. J., Friedman M. J., … Ursano R. J. (2007). Five essential elements of immediate and mid-term mass trauma intervention: Empirical evidence. Psychiatry, 70, 283–315. [DOI] [PubMed] [Google Scholar]
- *Informatieen Adviescentrum (2001). Jaarverslag 2000. Enschede: Informatie en adviescentrum. [Google Scholar]
- *Inspectie voor de Gezondheidszorg (IGZ) (2001a). Onderzoek vuurwerkramp Enschede Rapportage geneeskundige hulpverlening getroffenen vuurwerkramp Enschede. Utrecht: IGZ. [Google Scholar]
- *Inspectie voor de Gezondheidszorg (IGZ) (2001b). Rapport evaluatie geneeskundige hulpverlening cafébrand nieuwsjaarsnacht 2001. Utrecht: IGZ; Retrieved from http://www.algemeneehbodenbosch.nl/bibliotheek_info/cafebrand_vollendam_hulpverlening.pdf [Google Scholar]
- *Informatieen Adviescentrum (2002). Jaarverslag 2001. Enschede: Informatie en adviescentrum. [Google Scholar]
- *Inspectie voor de Gezondheidszorg (IGZ) (2003). Waakzaamheid blijft geboden. Een oriënterend onderzoek naar de hulpverlening bij psychische problemen na de cafébrand in Volendam. Den Haag: IGZ; Retrieved from http://www.nazorgvolendam.nl/pdf/Waakzaamheid%20blijft%20geboden.pdf [Google Scholar]
- *Informatieen Adviescentrum (2003a). Jaarverslag 2002. Enschede: Informatie en adviescentrum. [Google Scholar]
- *Informatieen Adviescentrum (2003b). Eindrapportage. Enschede: Informatie en adviescentrum. [Google Scholar]
- *Informatieen Adviescentrum (2003c). Eindevaluatie. Enschede: Informatie en adviescentrum. [Google Scholar]
- *Impact (2004a). Monitor organisatie psychosociale zorg n.a.v. Aviaire Influenze onder pluimvee. Eindrapportage. Amsterdam: Author. [Google Scholar]
- *Impact (2004b). Samenvattingen rapporten en monitor Aviaire Influenza. Amsterdam: Author. [Google Scholar]
- Impact (2010). Richtlijn psychosociale ondersteuning geüniformeerden. Diemen: Author. [Google Scholar]
- *Impact (2012). Eindrapportage IVC Vliegramp Tripoli. Diemen: Author. [Google Scholar]
- Impact (2014). Multidisciplinary guideline for post-disaster psychosocial support. Diemen: Author. [Google Scholar]
- *Inspectie Openbare Orde en Veiligheid (IOOV) (2009). Poldercrash 25 februari 2009. Een onderzoek door de Inspectie Openbare Orde en Veiligheid, in samenwerking met de Inspectie voor de Gezondheidszorg. Den Haag: IOOV; Retrieved from https://www.inspectie-jenv.nl/Publicaties/rapporten/2009/06/22/poldercrash-25-februari-2009 [Google Scholar]
- *Jeeninga W., de Vos E. H. M., Wijkmans C. J., & Bon-Martens M. J. H. (2010). Q-koortsbestrijding door de GGD; evalueren en leren. Infectieziekten Bulletin, 21(9), 342–345. Retrieved from https://www.rivm.nl/Documenten_en_publicaties/Algemeen_Actueel/Uitgaven/Infectieziekten_Bulletin/Archief_jaargangen/Jaargang_21_2010/Nummers_jaargang_21/November_2010/Inhoud_November_2010/Q_koortsbestrijding_door_de_GGD_evalueren_en_leren/Download/Q_koortsbestrijding_door_de_GGD_evalueren_en_leren [Google Scholar]
- *Inspectie Openbare Orde en Veiligheid (IOOV) (2011). Schietincident in ‘De Ridderhof’ Alphen aan den Rijn. Den Haag: IOOV; Retrieved from https://www.inspectie-jenv.nl/Publicaties/rapporten/2011/11/25/rapportage-schietincident-in-%E2%80%98de-ridderhof%E2%80%99-alphen-aan-den-rijn [Google Scholar]
- *Joustra T. H. J., Muller E. R., & van Asselt M. B. A. (2015). MH17. Passagiersinformatie. Den Haag: Onderzoeksraad voor de Veiligheid. [Google Scholar]
- *Jong W., Dückers M. L. A., & van der Velden P. (2016). Crisis leadership by mayors: A qualitative content analysis of newspapers and social media on the MH17 disaster. Journal of Contingencies and Crisis Management, 24(4), 286–295. [Google Scholar]
- Kaniasty K., & Norris F. H. (2004). Social support in the aftermath of disasters, catastrophes, and acts of terrorism: Altruistic, overwhelmed, uncertain, antagonistic, and patriotic communities In Ursano R. J., Norwoord A. E., & Fullerton C. S. (Eds.), Bioterrorism: Psychological and public health interventions (pp. 200–229). Cambridge: Cambridge University Press. [Google Scholar]
- Kapucu N., & van Wart M. (2006). The evolving role of the public sector in managing catastrophic disasters: Lessons learned. Administration & Society, 38(3), 279–308. [Google Scholar]
- *Kroon M. B., & Overdijk W. I. (1993). Psychosocial care and shelter following the Bijlmermeer air disaster. Crisis, 14, 117–125. [PubMed] [Google Scholar]
- *KLM Arbo Services (2004). Medisch Onderzoek Vliegramp Bijlmermeer. Schiphol: Author. [Google Scholar]
- *Klerx van Mierlo F. (2009). Faro gevolgen enquête 3. Tilburg: Intervict; Retrieved from https://www.vliegrampfaro.nl/publicaties/faro-gevolgen-enquetes/ [Google Scholar]
- Kuipers P., Wirz S., & Hartley S. (2008). Systematic synthesis of community-based rehabilitation (CBR) project evaluation reports for evidence-based policy: A proof-of-concept study. BMC International Health and Human Rights, 8(1), 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Laurier J. P., Ten Brink C. E., de Gouw J. M. M., & Corvers-Debers E. M. R. (2013). Over napijn en nazorg. Eindverslag van de onafhankelijke adviescommissie nazorg schietincident Alphen aan den Rijn. Alphen aan den Rijn: Onderzoekscommissie Nazorg schietincident; Retrieved from https://www.ifv.nl/kennisplein/nazorg-en-nafase/publicaties/over-napijn-en-nazorg-eindverslag-van-de-onafhankelijke-adviescommissie-nazorg-schietincident-alphen-aan-den-rijn [Google Scholar]
- Lettieri E., Masella C., & Radaelli G. (2009). Disaster management: Findings from a systematic review. Disaster Prevention and Management: an International Journal, 18(2), 117–136. [Google Scholar]
- Mays N., Pope C., & Popay J. (2005). Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. Journal of Health Services Research & Policy, 10, 6–20. [DOI] [PubMed] [Google Scholar]
- *Meijer J. S. (1992). Een vliegtuigramp in een huisartspraktijk; posttraumatische reacties in de eerste vier weken na de ramp in de Bijlmermeer. Nederlands Tijdschrift voor de Geneeskunde, 136(52), 2553–2558. [PubMed] [Google Scholar]
- *Meijer T. A. M., Oudkerk R. H., van Den Doel M., Augusteijn-Esser M. J., & Oedayraj Singh Varma T. (1999). Een beladen vlucht. Eindrapport Bijlmer Enquête. Den Haag: Sdu Uitgevers. [Google Scholar]
- Neal D. M. (1997). Reconsidering the phases of disasters. International Journal of Mass Emergencies and Disasters, 15(2), 239–264. [Google Scholar]
- *Netten J. C. M. (2005). Cultuur sensitieve psychosociale zorg na rampen. Lessons learned and good practices. Psychosociale zorg aan getroffenen uit etnische groepen bij de Bijlmer vliegramp en Enschede vuurwerkramp. Diemen: Impact. [Google Scholar]
- Noblit G. W., & Hare R. D. (1988). Meta-ethnography: Synthesizing qualitative studies (Vol. 11). Thousand Oaks: Sage. [Google Scholar]
- *Noordegraaf G. J., Savelkoul T. J. F., Van der Werken C., Kon M., Vandenbroucke C. M. J. E., & Meulenbelt J. (1993). De opvang en behandeling van 14 slachtoffers van het vliegtuigongeval in Faro, Portugal, in het calamiteitenhospitaal Utrecht van 23 tot en met 29 december 1992. De Bilt: Rijksinstituut voor Volksgezondheid en Milieu. [Google Scholar]
- Norris F. H., Friedman M. J., Watson P. J., Byrne C. M., Diaz E., & Kaniasty K. (2002). 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry: Interpersonal and Biological Processes, 65(3), 207–239. [DOI] [PubMed] [Google Scholar]
- *Oosting M., Beckers-de Bruijn M. B. C., Enthoven M. E. E., de Ruiter J., Savelkoul T. J. F., & Tümer Y. I. (2001). De vuurwerkramp. Eindrapport. Rotterdam: Phoenix & den Oudsten; Retrieved from https://dloket.enschede.nl/loket/sites/default/files/DOC/Eindrapport%20Commissie%20Oosting%20compleet.pdf [Google Scholar]
- *Nuijen M. (2006). Nieuwjaarsbrand Volendam 2001. Lessen voor later. Volendam: CRN Het Anker; Retrieved from http://www.nazorgvolendam.nl/pdf/Cat0106boek%20Volendaminternet.pdf [Google Scholar]
- Ozer E. J., Best S. R., Lipsey T. L., & Weiss D. S. (2003). Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin, 129(1), 52–73. [DOI] [PubMed] [Google Scholar]
- Perry R. W., & Lindell M. K. (2003). Preparedness for emergency response: Guidelines for the emergency planning process. Disasters, 27(4), 336–350. [DOI] [PubMed] [Google Scholar]
- Pfefferbaum B., & North C. S. (2016). Child disaster mental health services: A review of the system of care, assessment approaches, and evidence base for intervention. Current Psychiatry Reports, 18(1), 5. [DOI] [PubMed] [Google Scholar]
- Pollitt C., & Bouckaert G. (2011). Continuity and change in public policy and management. Cheltenham: Edward Elgar Publishing. [Google Scholar]
- Quarantelli E. L. (1988). Disaster crisis management: A summary of research findings. Journal of Management Studies, 25(4), 373–385. [Google Scholar]
- Quarantelli E. L. (ed.). (2005). What is a disaster?: A dozen perspectives on the question. London: Routledge. [Google Scholar]
- Reifels L., Pietrantoni L., Prati G., Kim Y., Kilpatrick D. G., Dyb G., & O’Donnel M. (2013). Lessons learned about psychosocial responses to disaster and mass trauma: An international perspective. European Journal of Psychotraumatology, 4(1), 22897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenthal U., Charles M. T., & Hart P. T. (1989). Coping with crises: The management of disasters, riots, and terrorism. Springfield: Charles C. Thomas. [Google Scholar]
- *Saan M., Bollen L., & Kunst M. (2015). Het werk van de familierechercheur: Een bron van stress of een bron van persoonlijke groei? Process, 94, 192–207. [Google Scholar]
- Scholtens A. (2008). Controlled collaboration in disaster and crisis management in the Netherlands, history and practice of an overestimated and underestimated concept. Journal of Contingencies and Crisis Management, 16(4), 195–207. [Google Scholar]
- *Slis E. (2000). Gebruik van communicatiemiddelen in relatie tot de vuurwerkramp. Stadspeiling najaar 2000. Enschede: I&O Research. [Google Scholar]
- *Soeteman J. H. (2009). Health problems of Enschede residents in the aftermath of the Fireworks Disaster. A longitudinal study with a pre-disaster assessment in general practice (Doctoral dissertation). NIVEL, Utrecht. [Google Scholar]
- Suzuki Y., Fukasawa M., Nakajima S., Narisawa T., & Kim Y. (2012). Development of disaster mental health guidelines through the Delphi process in Japan. International Journal of Mental Health Systems, 6(1), 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Te Brake H. (2016). Informatie- en Verwijscentrum Vliegramp Oekraïne. Wat kunnen we leren van nabestaanden en betrokkenen? Cogiscope, 16(4), 9–13. [Google Scholar]
- Te Brake H., & Dückers M. (2013). Early psychosocial interventions after disasters, terrorism and other shocking events: Is there a gap between norms and practice in Europe? European Journal of Psychotraumatology, 4. doi: 10.3402/ejpt.v4i0.19093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Te Brake H., Dückers M., De Vries M., van Duin D., Rooze M., & Spreeuwenberg C. (2009). Early psychosocial interventions after disasters, terrorism, and other shocking events: Guideline development. Nursing & Health Sciences, 11(4), 336–343. [DOI] [PubMed] [Google Scholar]
- *Te Brake H., & Schaap R. (2017). Eindrapportage Informatie- en Verwijscentrum Vliegramp Oekraïne. Diemen: Stichting Impact; Retrieved from https://www.rijksoverheid.nl/documenten/rapporten/2017/08/23/tk-bijlage-eindrapportage-van-de-evaluatie-onder-gebruikers-en-betrokken-partijenmpact-eindrapportage-evaluatie-ivc-vliegramp-oekraine [Google Scholar]
- Thorne S., Jensen L., Kearney M. H., Noblit G., & Sandelowski M. (2004). Qualitative metasynthesis: Reflections on methodological orientation and ideological agenda. Qualitative Health Research, 14(10), 1342–1365. [DOI] [PubMed] [Google Scholar]
- *Tielen H., van de Laar A., & van Dijk A. (2012). Schietincident 9 april 2011 Alphen aan den Rijn. Onderzoek naar de gevolgen voor de gezondheid van de getroffenen en betrokkenen. Alphen aan den Rijn: GGD Hollands Midden. [Google Scholar]
- *Torenvlied R., Giebels E., Wessel R. A., Gutteling J. M., Moorkamp M., & Broekema W. G. (2015). Rapport evaluatie nationale crisisbeheersingsorganisatie vlucht MH17. Enschede: Universiteit Twente; Retrieved from https://www.ifv.nl/kennisplein/Documents/20150101-WODC-UTwente-Evaluatie-nationale-crisisbeheersingsorganisatie-vlucht-MH17.pdf [Google Scholar]
- *Torenvlied R., Giebels E., Wessel R. A., Gutteling J. M., Moorkamp M., & Broekema W. G. (2016). Evaluatie nationale crisisbeheersingsorganisatie vlucht MH17. Magazine Nationale Veiligheid en Crisisbeheersing, 2, 4–6. [Google Scholar]
- *van der Meijden P. A., Roorda J., IJzermans C. J., van der Velden P. G., & Grievink L. (2006). Gezondheidsmonitoring Getroffenen Vuurwerkramp Enschede. Enschede: GGD Regio Twente; Retrieved from https://www.ifv.nl/kennisplein/ghor-algemeen/publicaties/gezondheidsmonitoring-getroffenen-vuurwerkramp-enschede [Google Scholar]
- *van der Velden P. G., Dusseldorp A., Drogendijk A. N., & van Overveld A. (2011). Q-koorts - ruimingen van besmette bedrijven Evaluatieonderzoek onder geitenhouders. Bilthoven: Rijksinstituut voor Volksgezondheid en Milieu. [Google Scholar]
- *van der Bijl N., van der Velden T. M. H., Govers E. G. E., & van Dorst P. C. (2012). Het spijt mij. Over Q-koorts en de menselijke maat. Den Haag: De Nationale Ombudsman; Retrieved from https://www.nationaleombudsman.nl/uploads/rapport_2012-100_webversie_0.pdf [Google Scholar]
- *van der Velden P. G., & Kleber R. J. (2000). Gezondheid en nazorg getroffenen legionella epidemie. Zaltbommel: Instituut voor Psychotrauma. [Google Scholar]
- *van Deursen S., Prins J., Kelderman F., & Priester R. (1993). Kinderen na de ramp. Hulpverlening aan jeugdige slachtoffers van de Bijlmer-vliegramp. Maandblad Geestelijke Volksgezondheid, 48, 1077–1088. [Google Scholar]
- *van Dijk G., van Dissel J. T., Speelman P., Stegeman J. A., Vanthemsche P., de Vries J., & van Woerkum C. M. J. (2010). Van verwerping tot verheffing. Q-koorts beleid in Nederland 2005-2010. Den Haag: Evaluatiecommissie Q-Koorts; Retrieved from https://www.ifv.nl/kennisplein/informatiebeleid-im/publicaties/onderzoeksrapport-van-verwerping-tot-verheffing [Google Scholar]
- van Duin M., Overdijk W., & Wijkhuijs V. (1998a). Faro gevolgen enquête 1. Leiden: Crisis Onderzoek Team; Retrieved from https://www.vliegrampfaro.nl/publicaties/faro-gevolgen-enquetes/ [Google Scholar]
- *van Duin M., Overdijk W., & Wijkhuijs V. (1998b). Faro gevolgen enquête 2. Leiden: Crisis Onderzoek Team; Retrieved from https://www.vliegrampfaro.nl/publicaties/faro-gevolgen-enquetes/ [Google Scholar]
- van Duin M., Tops P., Wijkhuijs V., Adang O., & Kop N. (2012). Lessen in crisisbeheersing. Dilemma’s uit het schietdrama in Alphen aan den Rijn. Den Haag: Boom Lemma uitgevers; Retrieved from https://www.ifv.nl/advieseninnovatie/Documents/2012-IFV-PA-Lessen-in-crisisbeheersing-dilemmas-Alphen-aan-den-Rijn.pdf [Google Scholar]
- *van Kamp I., & van der Velden P. G. (2001). Vuurwerkramp Enschede: Lichamelijke en geestelijke gezondheid en ervaringen met de ramp: Rapportage van het gezondheidsonderzoek. Bilthoven: Rijksinstituut voor Volksgezondheid en Milieu (RIVM). [Google Scholar]
- Vereniging voor Nederlandse Gemeenten (VNG) (2004). Handreiking opzet informatie en adviescentrum (IAC) na rampen. Den Haag: VNG. [Google Scholar]
- *van Hemert A. M., & Smeets E. C. (2004). Medisch Onderzoek Vliegramp Bijlmermeer – Evaluatieverslag. Amsterdam: Academisch Medisch Centrum Amsterdam. [Google Scholar]
- *Verschuur M. J., Maric M., Cuijpers A. T. F., van Emmerik A. A. P., Rosendaal F. R., & Spinhoven P. (2004a). Medisch onderzoek Vliegramp Bijlmermeer (samenvatting). Leiden: Leids Universitair Medisch Centrum. [Google Scholar]
- *Verschuur M. J., Maric M., Cuijpers A. T. F., van Emmerik A. A. P., Rosendaal F. R., & Spinhoven P. (2004b). Het effect van het Medisch Onderzoek Vliegramp Bijlmermeer op de gezondheidsbeleving van bewoners en hulpverleners ruim acht jaar na de Vliegramp Bijlmermeer. Leiden: Leids Universitair Medisch Centrum. [Google Scholar]
- *Verschuur M. J. (2009). Effects of the medical investigation Bijlmermeer aviation disaster on health perception of residents and rescue workers (Doctoral dissertation). Leiden University Repository (Accession No. 9789081472210). [Google Scholar]
- *Veiligheidsregio Kennemerland (2009a). Vaststellen Plan van Aanpak Nafase verongelukte vliegtuig Turkish Airlines (TK1951). Haarlem: Author. [Google Scholar]
- *Veiligheidsregio Kennemerland (2009b). Reactie rapportage onderzoek vliegtuigongeval d.d. 25 februari 2009. Haarlem: Author. [Google Scholar]
- Vymetal S., Deistler A., Bering R., Schedlich C., Rooze M., Orengo F., … Krtickova M. (2011). European commission project: European guideline for target group-oriented psychosocial aftercare—implementation. Prehospital and Disaster Medicine, 26(3), 234–236. [DOI] [PubMed] [Google Scholar]
- Walsh D., & Downe S. (2005). Meta-synthesis method for qualitative research: A literature review. Journal of Advanced Nursing, 50(2), 204–211. [DOI] [PubMed] [Google Scholar]
- *Witteveen A. B. (2006). The long-term aftermath of the Amsterdam air disaster: Psychological wellbeing of professionally involved rescue workers (Doctoral dissertation). Vrije Universiteit Amsterdam (Accession No. 198867). [Google Scholar]
- Wet Publieke gezondheid (2012). Retrieved from http://wetten.overheid.nl/BWBR0024705
- Wet Veiligheidsregio (2010). Retrieved from http://wetten.overheid.nl/BWBR0027466
- Witteveen A. B., Bisson J. I., Ajdukovic D., Arnberg F. K., Bergh Johannesson K., Bolding H. B., … Olff M. (2012). Post-disaster psychosocial services across Europe: The TENTS project. Social Science & Medicine, 75, 1708–1714. [DOI] [PubMed] [Google Scholar]
- Yzermans C. J., Donker G. A., Kerssens J. J., Dirkzwager A. J., Soeteman R. J., & Ten Veen P. M. (2005). Health problems of victims before and after disaster: A longitudinal study in general practice. International Journal of Epidemiology, 34(4), 820–826. [DOI] [PubMed] [Google Scholar]
- *Yzermans C. J., & Gersons B. P. R. (2002). The chaotic aftermath of an air plane crash in Amsterdam. A second disaster In Havenaar J. M., Cwikel J. G., & Bromet E. J. (Eds.), Toxic turmoil: Psychological and societal consequences of ecological disasters (pp. 85–100). New York: Kluwer Academic/Plenum Publishers. [Google Scholar]
- Yzermans, C.J., Dirkzwager, A.J.E., Kerssens, J.J., Cohen-Bendahan, C.C.C. & ten Veen, P.M.H (2006). Gevolgen van de vuurwerkramp in enschede voor de gezondheid Eindrapport van de monitoring in de huisartspraktijken. Utrecht: NIVEL. [Google Scholar]
- References marked with (*) are included in the meta-synthesis. [Google Scholar]